
Abstract
The demand for an improvement of the biocompatibility and durability of vascular and valvular implants requires translational animal models to study the in vivo fate of cardiovascular grafts. In the present article, a review on the development and application of a microsurgical rat model of infrarenal implantation of aortic grafts and aortic valved conduits is provided. By refinement of surgical techniques and inclusion of hemodynamic considerations, a functional model has been created, which provides a modular platform for the in vivo assessment of biological and tissue-engineered grafts. Through optional addition of procalcific diets, disease-inducing agents, and genetic modifications, complex multimorbidity scenarios mimicking the clinical reality in cardiovascular patients can be simulated. Applying this model, crucial aspects of the biocompatibility, biofunctionality and degeneration of vascular and valvular implants in dependency on graft preparation, and modification as well as systemic antidegenerative treatment of the recipient have been and will be addressed.
Introduction
I
Techniques of tissue engineering have led to a variety of new cardiovascular grafts with excellent performance in experimental as well as first clinical trials.1–5 To examine the in vivo fate of new cardiovascular implant candidates, translational small and large animal models are necessary. The present review article focuses on the evaluation of cardiovascular grafts in a small animal model, which particularly allows for sophisticated research on structural and metabolic processes in the implants as well as on the underlying mechanisms.
Choice of Species for the Implantation Model
At the end of the 1980s, a functional rat model for the chronic in vivo evaluation of vascular grafts anastomosed to the infrarenal aorta has been introduced.
6
Since then, this model has been adapted by several groups worldwide, and a number of modifications have been added in the following. There are multiple good reasons for the ongoing acceptance and the remarkable dissemination of this model: (1) functionality of the grafts, particularly in comparison with other implantation models, such as in subcutaneous tissue, (2) high reproducibility translating into robust experimental results, (3) availability of a broader range of diagnostic tools (such as antibodies and molecular agents for the histological, biomolecular, and imaging assessment), when compared to the choice available for large animal species, (4) availability of genetically modified strains, allowing for dedicated studies focused on functional aspects of specific genes, (5) acceptable stress and operative mortality, particularly in comparison to orthotopic heart valve implantation in small animals, and (6) considerably lower project costs and less ethical concerns as compared with large animal studies (Supplementary Table S1; Supplementary Data are available online at
On the contrary, certain limitations are inherent to rodent animal models with respect to studies on cardiovascular grafts, mainly related to the smaller life span and a lower tendency to spontaneous ectopic calcification when compared to sheep or rabbits. Moreover, hemodynamic aspects of cardiovascular grafts should be examined in adequate large animal models, such as sheep or pigs.
Rats are the smallest animals that have been so far accessible to perform the microsurgical implantation of heart valves effectively and safely, while there exist reports on aortic vascular graft implantation in mice. 7 In addition, rats can be reproduced very fast and can be monitored and followed-up quite easily. 4 Therefore, our research group has chosen the species rat for the infrarenal aortic conduit implantation model, which has been adapted in 2009 and since then used with several modifications to address specific aspects of the in vivo remodeling of cardiovascular implants.8–14 This report presents our own experience as well as a review of the data published by others.
Development of the Microsurgical Rat Model
A short overview on the chronicle of aortic graft implantation techniques in rats is displayed in Table 1.
AG, vascular aortic graft; AI, insufficiency of the recipient aortic valve; AVC, aortic valved conduit; CV, cardiovascular; DC, decellularization; GA, glutaraldehyde.
Early approaches of aortic conduit implantation
In principle, a specific cardiovascular graft can be implanted into the systemic circulation of a recipient animal without the use of extracorporeal circulation and cardioplegic cardiac arrest. For this purpose, the implant is integrated into the infrarenal aorta by sequentially anastomosing the graft in an end-to-end or end-to-side manner. Further variations may be introduced by using implants carrying valvular elements, turning a vascular aortic graft (AG) into an aortic valved conduit (AVC). An alternative technique for the examination of graft materials exposed to the bloodstream is the implantation of vascular patches into the abdominal wall. Several groups have reported on studies on biological as well as artificial patches implanted using this surgical approach.15–17
In terms of the associated technical demand, stress and impairment for the animals as well as involved costs, the patch model does not provide a major advantage over the AG and AVC implantation models. On the contrary, AG and AVC grafts better mimic clinical scenarios compared with aortic patches. Moreover, they provide information on the hemodynamics and hemodynamic-dependent structural and functional changes in circular prosthesis and valved grafts in particular. Therefore, in the following, only AG and AVC implantation models are discussed.
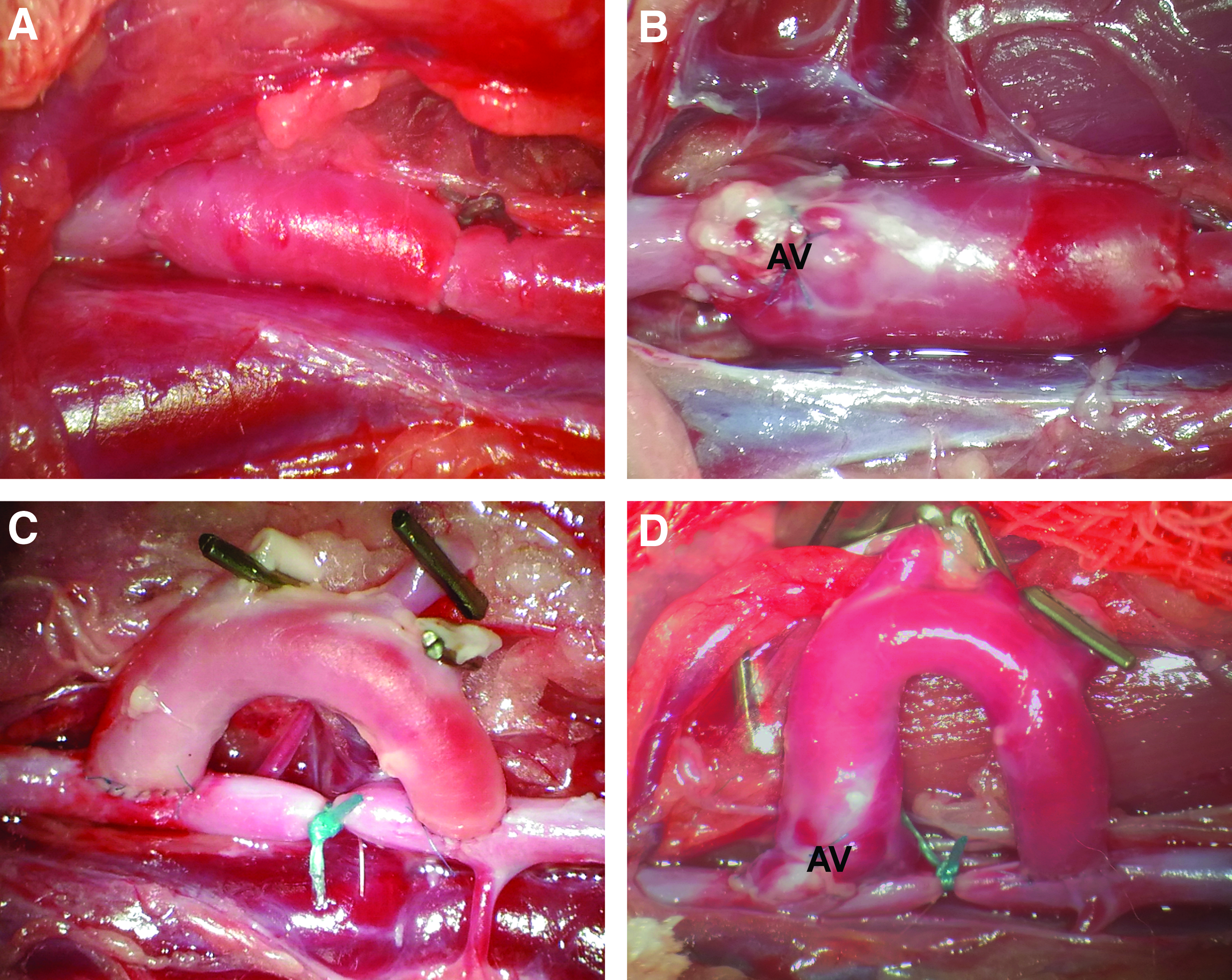
After an early report on the end-to-end implantation model of AG in rats (Fig. 1A), 18 the AVC implantation in a microsurgical rat model was described by Yankah et al., 19 who anastomosed the native AVC in an infrarenal position to the aorta in an end-to-end manner (Fig. 1B). However, this pioneering version of the rat model exhibits several limitations. First of all, there was an anatomical size mismatch, as the AVCs were larger in diameter than the native abdominal aorta in recipient rats. This mismatch caused surgical trauma and flow turbulence, which was probably responsible for early graft fibrosis and calcifying degeneration. Moreover, to avoid a valsalva sinus thrombosis despite the unfavorable hemodynamics, one of the aortic leaflets was excised.
Implantation techniques and graft types. Vascular aortic grafts
To solve the size mismatch issue, Zhou et al. modified the geometry of the AVC in a complex manner as follows 20 : The aortic graft was harvested and divided into two parts, that is, one part including the aortic valve and the ascending aorta up to the brachiocephalic trunk, and another part including the descending aorta with the origin of the left subclavian artery. These two parts were reconnected by anastomosing the aortic valve with the distal part of the descending aorta. Finally, the conduit was infrarenally implanted into the recipient rats, connecting the origins of the supraaortic branches to the recipient aorta in an end-to-end manner. By introducing this modification, the size mismatch issue was resolved. Nevertheless, this method is technically extremely demanding.
Modification toward a U-shaped implantation technique
Oei et al. described for the first time an end-to-side implantation technique with a U-shaped AVC. 21 Allogeneic and syngeneic AVC were implanted in an end-to-side manner, resulting in no fibrosis or intimal thickening of the conduit leaflets 21 days postoperatively. Thus, it has been proved that the U-shape implantation method did not induce any structural changes in the conduits. In another study on U-shaped AVC, Kallenbach et al. investigated the functionality of the implanted conduits by means of echocardiography. Thereby, they could show pulsatile opening and closing movements of the implanted aortic valve leaflets. 22
Our research group has applied the U-shape graft model on AG and AVC implantation in the context of degeneration of native cryopreserved and decellularized prostheses (Fig. 1C, D).8–14 In brief, this approach includes the following surgical steps: after median sternotomy of the donor animal, the thoracic aorta is dissected from the surrounding tissue, and a U-shaped AG or AVC is prepared. For the AVC graft, the coronary arteries are ligated with an 8-0 monofilament, nonabsorbable polypropylene suture. For implantation, a median laparotomy is performed to expose the infrarenal aorta of the recipient animal. Heparin (300 IU [kg bw]−1) is administered via the central venous catheter to achieve effective anticoagulation. Afterward, the infrarenal aorta is clamped. Distal of the clamping, an incision is made to the native aorta to suture the proximal anastomosis of the U-shaped conduit in an end-to-side manner, using a 10-0 monofilament, nonabsorbable polypropylene suture. After a short reperfusion period to prevent paraplegia, the distal side of the graft is anastomosed in a similar manner. To guarantee that the blood flows exclusively through the aortic conduit, the native aorta between the two anastomoses is ligated with 5-0 silk sutures (Fig. 1D). After wound closure, the patency of the graft is controlled by Doppler sonography.
A short checklist with the central procedures of the rat model is displayed in (Supplementary Table S2).
Improvement of aortic valve graft hemodynamics
All previously discussed rat models to some degree exhibit functional limitations. Due to the competent native aortic valve of the recipient rat, the hemodynamic situation for the implanted AVC remains unphysiological with a continuous antegrade blood flow during systole as well as in diastole. This in turn hinders the implanted valve from complete closure at any time.
Aiming to solve this hemodynamic problem, Legare et al. introduced a further modification by generating a catheter-induced aortic valve insufficiency. 23 Via a vasotomy of the right carotid artery, a catheter was inserted toward the level of the aortic valve (Fig. 2A). Afterward, the catheter was utilized to perforate the aortic valve cusps under echocardiographic guidance (Fig. 2B). By creating a native aortic valve insufficiency, a reverse diastolic flow appeared in the whole aorta (Fig. 2C), resulting in diastolic closure of the implanted valve. The diastolic competence of the implanted valve is indicated by a lack of diastolic backflow in the aorta distally to the AVC (Fig. 2D).

Creation of aortic valve insufficiency. A catheter or a guide wire, respectively, is inserted via the right carotid artery
In the above-mentioned study, the authors observed a substantial mortality rate following catheter-induced aortic valve insufficiency (37.5%). The treated rats deteriorated hemodynamically as a consequence of heart failure due to the acute aortic valve insufficiency with consecutive volume overload of the left ventricle. Our experimental research group has improved the method of creating an aortic valve insufficiency. 12 Using dedicated Doppler sonography, it has been demonstrated that the severity of the aortic valve insufficiency is proportional to the ratio of the time–velocity integral of reversed diastolic flow to forward systolic flow in the ascending aorta. In a series of experiments, rats that went on to die presented a significantly higher degree of insufficiency compared with animals surviving the procedure. These data suggest that a moderate grade of aortic valve insufficiency, as defined by the insufficiency jet area per area of the left ventricular outflow tract, not only caused a more adequate hemodynamic situation for the implanted AVC but also improved the survival of the recipient rats.
Due to the improved hemodynamics, resulting in diastolic valve closure, degenerative processes are expected to occur in a similar way as in the orthotopic implant position. On the contrary, heterotopic implantation of AVC in recipients without native aortic valve insufficiency has been reported to result in retrovalvular thrombus formation, which is most probably due to the absence of an early diastolic backflow and thus a lack of complete valvular closure. 24
Another option to control the hemodynamic effects of aortic valve insufficiency generation may be invasive pressure monitoring, or pressure–volume monitoring, whereas in our opinion, invasiveness and high costs of these methods do not seem to be justified in the light of accurate and reliable Doppler sonography assessment.
Besides Doppler sonography assessment, high-resolution magnetic resonance imaging can be applied to examine the patency of implanted grafts. In a previous article on the development of the rat implantation model, we have shown the worth of small animal magnetic resonance imaging for displaying unimpaired perfusion of the implant as well as the downstream parts of the vascular system. 13 In this context, plastination techniques that are based on the injection of colored glues into the vascular system of euthanized rats are worthwhile tools to control the postoperative perfusion particularly of smaller downstream arteries. 13 However, the latter method should be used only for validation studies, since the loss of all tissues is an inherent issue of this method. Thus, no further tissue analyses are possible in these animals.
Preclinical Simulation of Different Clinical Scenarios
Relevance for pediatric patients
Implantation of aortic valve allografts is a routine therapeutic option especially in pediatric cardiovascular surgery. However, due to the long-lasting life span of pediatric patients, a final graft failure is inevitable.25,26 Adaptive immunity is accused of causing accelerated failure of allografts in both animals and humans.27,28 Therefore, it is of major interest to find other solutions especially for pediatric patients. Tissue engineering and decellularization, in particular, are innovative methods which are supposed to resolve current limitations of allogeneic grafts. However, reports on individual pediatric cases with a disastrous outcome following the implantation of a decellularized graft have challenged the reliability of this concept. Very limited post mortem analyses have suggested an insufficient donor cell removal as a possible reason for the adverse outcome of decellularized allografts and xenografts. Therefore, a more rigorous preclinical testing of these implants is necessary.29,30
As a response to this clinical demand, a growing rat model has been developed to mimic the clinical setting of pediatric cardiovascular surgery. In particular, the in vivo observation of AVC in terms of immune and inflammatory response and recellularization may be an advantage of this model, which is designed to study juvenile recipient animals. 13 The model can be described as follows: decellularized AVCs that had been harvested from adult rats (200–250 g) were implanted in the infrarenal position of the abdominal aorta of a juvenile recipient rat (70–80 g) in an end-to-side manner. Eight weeks after implantation, neointimal recellularization by endothelial cells can be found on large proportions of the intimal surface of the implanted conduits. In our study, there were no signs of increased inflammatory activity, which may point to a diminished inflammatory response against decellularized grafts compared with fresh or cryopreserved allografts, containing living cells or cellular remnants, respectively. These findings are in agreement with previously published data by Meyer et al. demonstrating a significantly decreased level of inflammatory infiltration of decellularized aortic conduit implants compared with nondecellularized controls in rats. 31
Unfortunately, microcalcification, an uncontroversial activator of cardiovascular degeneration, was observed in all parts of the decellularized scaffolds. Several studies have reported similar findings, as they revealed signs of moderate calcification for instance in the wall of decellularized sheep pulmonary artery alloimplants, pulmonary homografts or in decellularized porcine heart valve xenografts.29,32,33 Intramural deposition of calcium may be related to extracellular matrix components, cell remnants, or the respective decellularization protocol. Therefore, more detailed and comparative in vivo analyses of these potential causes should be conducted in further studies.
Comorbidity factors associated with accelerated cardiovascular calcification
Several proarteriosclerotic factors such as obesity, arterial hypertension, diabetes mellitus, dyslipidemia, chronic kidney disease (CKD), as well as smoking are known to predispose cardiovascular diseases. 34 Metabolic syndrome describes a clinical condition with a combination of hypertension, diabetes mellitus, dyslipidemia, and obesity, where individual adverse factors promote the progression of each other in a vicious circle, for example, insulin resistance aggravating obesity and arterial hypertension, and so on. A remarkable number of patients undergoing an aortic valve replacement present with characteristics of a metabolic syndrome, with an indisputably elevated risk of accelerated calcifying degeneration of biological graft prostheses. Therefore, it is of high relevance to the validity of preclinical screening system to include metabolic syndrome in an adequate animal model to evaluate the functionality and stability of grafts in vivo.
There are several models related to arteriosclerosis and calcifying degeneration in animals using different diets to induce the above-mentioned characteristics of a metabolic syndrome. Our research team investigated the effect of procalcific diets on the in vivo degeneration of biological and tissue-engineered heart valves and vascular grafts in rats. A systematic evaluation of various dietary concentrations of vitamin D, cholesterol, and phosphate has been reported with the aim of induction of arteriosclerosis. 11 Thereby, it has been demonstrated that diets containing high concentrations of vitamin D (300,000 IU/kg), cholesterol (2%), and phosphate (1.5%) resulted in an extremely increased rate of ectopic calcification, including the native aorta, but most interestingly also involving the native aortic valve. In front of such robust procalcific experimental background, an accelerated deterioration has also been observed in implanted biological AVC.
Another mechanism of degenerative calcification is triggered by diabetes. To induce a diabetic metabolic status, the streptozotocin model has been introduced. 35 Due to cytotoxic mechanisms leading to the extinction of pancreatic β-cells, the administration of streptozotocin results in an experimental type 1 diabetes mellitus. This model has been validated not only in rats but also in mice, therefore allowing a combination of this approach with the various variants of the microsurgical model of AVC implantation. To realize an experimental type 2 diabetes, a further modification has been described, where nicotinamide application partially inhibits the cytotoxicity of streptozotocin.36–38
CKD plays a major role in the etiology and progression of cardiovascular disease. Hence, several studies have evaluated different approaches to achieve a clinically relevant CKD in small rodents. A subtotal (5/6th) nephrectomy in rats is one of the most commonly used kidney failure models. 39 This approach results in significantly reduced creatinine clearance levels and elevated blood pressure. By adding high concentrations of salt water and nitric oxide synthase inhibitor, the cardiac function also declines. 40 However, it is still unknown to what extent this experimental model of kidney failure may contribute to arteriosclerosis. Moreover, the mechanisms involved may significantly differ when the above-mentioned experimental model is compared with the clinically prevailing forms of CKD.
Cigarette smoking remains a global health hazard with associated noxious effects on the cardiovascular system. In a work by Al Hariri et al., the effects of cigarette smoke exposure on the cardiovascular system have been investigated in a rat model. 41 Data presented so far show a significant association between smoke exposure and cardiac hypertrophy, inflammation, profibrotic, and atherogenic markers as well as aortic calcification. Given these significant results on cardiovascular remodeling, it appears most likely that a combination of the herein described AVC model and the inhalative exposure to cigarette smoke may provide new insights in the mechanisms that govern the in vivo remodeling of biological implants, including tissue-engineered cardiovascular grafts.
Most cardiovascular diseases and age-related cardiovascular alterations are accompanied by increases in oxidative stress, mostly due to the enhanced generation and decreased metabolism of reactive oxygen species and reactive nitrogen species. 34 In particular, oxidative stress contributes to atherosclerosis and aortic valve degeneration, while its involvement in the pathophysiological processes of cardiovascular graft deterioration is not clarified yet. 42
To adequately mimic the allogeneic situation of homografts, which present the current gold standard in the clinic practice, different rat strains are necessary as donor and recipient animals, respectively. With only one (inbred) rat strain, a syngeneic or pseudosyngeneic transplantation scenario may be present, which would certainly affect the extent and speed of the degeneration of the implant.
Evaluation of Tissue-Engineered Grafts
Decellularized versus cryopreserved implants
Cryopreservation is the common method to treat allogeneic homografts after harvesting. On the one side, cryopreservation is necessary to store the collected prostheses until implantation. On the other side, cryopreservation has been reported to favor the in vivo deterioration of allogeneic and syngeneic AVC when compared with fresh grafts in a rat implantation model. 43 As cryopreserved homografts undergo progressive in vivo degeneration due to immune and inflammatory processes predominantly against their cellular components, decellularized prostheses consisting of extracellular matrix only have been researched on extensively over the last decade.
Our experimental research group has examined the performance of detergent-decellularized versus cryopreserved allografts in the above presented rat implantation model under procalcific metabolic conditions. 11 The results of this study demonstrate that main pathological processes of graft degeneration, such as myofibroblast-associated intima hyperplasia, inflammatory cell infiltration, and hydroxyapatite deposition, could be significantly inhibited by decellularization of the AVC. These findings confirm previous reports on the superiority of decellularized cardiovascular grafts over fresh or cryopreserved donor implants in small as well as large animal models .24,31,33,44,45
To store decellularized grafts until later clinical usage, allowing for off-the-shelf availability in the operation room, cryopreservation may be an appropriate treatment. However, studies on the overall quality of donor grafts stored by methods of conventional cryopreservation have revealed mixed results, with convincing data suggesting a negative impact on the extracellular matrix preservation with direct implications for the in vivo performance in preclinical (large animal) chronic implantation models. 46 As an alternative, ice-free cryopreservation has been demonstrated to result in superior tissue quality and may therefore prove as the best preservation method. However, clinical evidence regarding this issue is currently lacking.
Decellularization techniques as a foundation for cardiovascular tissue engineering
Several methods for decellularization to obtain a completely acellular graft without losing the structure of the extracellular matrix have been proposed. The methodical repertoire comprises the utilization of detergents, such as sodium dodecyl sulfate and dichloracetate, cell toxins, such as latrunculin B, enzymes, such as trypsin and DNase, osmotic shock by high ionic strength salt solutions, and physical methods, such as freeze-drying or sonication.
Exemplary, Grauss et al. evaluated the following methods to decellularize rat AVC using different combinations of detergents, including triton X-100, sodium dodecyl sulfate, and a combination of trypsin and ethylenediaminetetraacetic acid. According to their histological evaluation, decellularization was ineffective when using only triton X-100, and all protocols based on trypsin caused a severe damage of the extracellular matrix of the conduits. Only sodium dodecyl sulfate administration resulted in an adequate balance of acellularity and matrix preservation. 24 These observations confirm previous data from our group as well as others on the usefulness of detergents for balanced decellularization of valvular and vascular tissues. 47
However, it has also been reported that detergents not only promote cell removal but also remarkably degrade the architecture of the extracellular matrix.48,49 Furthermore, detergent-decellularization approaches may result in incomplete removal of cellular remnants from tissues with dense extracellular matrix structure, such as the aortic wall, leading to an inflammatory response of the recipient against the implant. 50 To eliminate basophilic nuclear residues, the addition of RNase and DNase should be considered, although the aim to obtain improved cellular protein removal has caused the examination of alternative techniques. Based on a decellularization approach for skeletal muscle containing only biological agents, 51 our research group has developed a new protocol applying the cell toxin latrunculin B, high ionic strength salt solutions, and DNase. This detergent-free, nonproteolytic, actin-disassembling regimen has been proven to preserve the mechanical and structural integrity of the extracellular matrix and to provide an adequate elimination of cellular residues in small as well as large diameter valved grafts. 10 After implantation in the herein discussed rat model, biologically decellularized AVC presented significantly accelerated autologous in vivo recellularization compared with grafts treated with detergents, presumably due to lower matrix density, including a diminished glycosaminoglycan content.
The evaluation of decellularization techniques in small animal valves and vessels could be a limitation in so far that the effects of the procedure may differ when being applied in large animal or human tissues, since thickness and extracellular matrix architecture are not homologous between different species. However, predominantly in case of detergent-based decellularization, clinical and large animal studies have confirmed the excellent performance that has been described in other studies using small animals.52–55 Moreover, for the above mentioned biological decellularization protocol, our group has already shown appropriate in vitro performance in terms of histoarchitecture cytotoxicity and mechanics compared with native and detergent-decellularized grafts. 10 Nevertheless, when transferring any decellularization approach from small to large animals or even to humans, protocol adaption has to be considered.
Collectively, these findings demonstrate the value of extracellular matrix generation by means of decellularization as a foundation for successful tissue engineering of cardiovascular grafts.
Significance of autologous in vivo recellularization in tissue-engineered grafts
After implantation, rapid autologous in vivo recellularization is desired for decellularized cardiovascular grafts to improve their biocompatibility in terms of low thrombogenicity, low immunogenicity, and fast integration into the host organism, including growth potential. For the in vivo population of cardiovascular grafts with autologous cells, different routes of cell invasion are discussed: transanastomotic cellular ingrowth from the adjacent recipient tissue, cell recruitment from the blood stream, and cellular ingrowth via the adventitial side of the implant. While transanastomotic ingrowth plays a minor role in humans, it seems to be the major force in most animal models, including rat implantation models. To differentiate between transanastomotic ingrowth and transmural endothelialization or cell recruitment from the blood stream, respectively, a rat model with interposition of a vascular polytetrafluoroethylene loop graft to the infrarenal aorta has been published. 56 This model has shown rapid and progressive cellular population of the perianastomotic regions of the grafts with a peak velocity in the first 2 weeks after implantation, while the other mechanisms of cellular population resulted in confluent endothelial layers not before week 12.
Since neointima formation on cardiovascular prostheses ideally involves predominantly endothelial cells, strategies to improve the recruitment of endothelial progenitor cells (EPC), such as systemic treatment with granulocyte colony-stimulating factor (G-CSF) or surface coating with vascular endothelial growth factor (VEGF) and stromal cell-derived factor 1α (SDF1α), have been investigated. EPC are a mononuclear cell population in the peripheral blood that has a core function in angiogenesis and vascular regeneration. 34 In this context, it has been described that EPC augment collateral vessel growth to ischemic tissues and deliver anti- or proangiogenic agents, thus contributing to tissue remodeling. 57 These factors, such as VEGF, G-CSF, and hepatocyte growth factor, support vasculogenesis by paracrine signaling. 58 Besides effects on intima formation that directly target cells, EPC also take part in active extracellular matrix remodeling by release of matrix metalloproteinases (MMP), especially MMP type 2 and 9. 59
Biointerface modification of tissue-engineered cardiovascular grafts
Since cellular repopulation is a slow process, particularly in graft regions apart from the anastomoses and in regions with dense matrix architecture, different strategies of “guided tissue regeneration” have been examined to accelerate the autologous recellularization. 60 In this context, bioactive proteins and peptides have been used as coating agents to improve the biofunctionality of cardiovascular grafts 61 (Table 2).
BIO, detergent-free, nonproteolytic, actin-disassembling regimen; CCB, calcium channel blocker; EPC, endothelial progenitor cells; FN, fibronectin; G-CSF, granulocyte colony-stimulating factor; HG-VEGF, vascular endothelial growth factor conjugated to a temperature-sensitive aliphatic polyester hydrogel; SDF1α, stromal cell-derived factor 1α.
Fibronectin
Fibronectin (FN) is an extracellular matrix protein that binds to various types of integrins, receptor proteins integrated in cell membranes. Among other functions, FN promotes the adhesion, growth, and migration of different cell types by binding to α4β1 integrin. 62 Therefore, our group has examined the impact of luminal and adventitial FN coating of decellularized AVC on their autologous in vivo recellularization in the rat implantation model described above. 9 This study revealed significantly accelerated neointima formation and especially media repopulation compared with uncoated grafts, whereas the latter effect is predominantly caused when coating is applied to the adventitial side of the implants. Consecutively, a follow-up project revealed that the above-mentioned biological, actin-disassembling decellularization protocol allows for improved biofunctionalization of AVC, particularly in terms of rapid media repopulation by FN coating before implantation. 10
Vascular endothelial growth factor
VEGF is a glycoprotein associated with angiogenesis and vasculogenesis that attracts EPC from the bloodstream. VEGF primarily binds to a cell surface receptor and stimulates cell division, migration, and differentiation. 61 Recently, our research team evaluated the benefit of AVC coating with VEGF conjugated to a temperature-sensitive aliphatic polyester hydrogel. 63 We implanted detergent-decellularized AG luminally coated with VEGF hydrogel in the heterotopic rat graft model. As a result, we found VEGF hydrogel coating to stimulate the autologous endothelialization and medial recellularization, whereas intimal hyperplasia also occurred. Similar findings have been obtained in a murine model of decellularized vascular graft implantation by Tsai et al. 64 In this model, VEGF coating improves endothelialization and also has a favorable impact on intima hyperplasia. However, when considering VEGF as treatment agent, concerns about its oncogenic risk should not be neglected. 65
Stromal cell-derived factor 1α
SDF1α is a chemokine that plays an active role in guiding progenitor cells to target tissues by binding to its selective receptor CXCR4, which is abundantly expressed on EPC. 61 Moreover, SDF1α is involved in tissue repair by differentiating T helper cells into an anti-inflammatory subtype. Zhou et al. implanted decellularized AVC coated with heparin and SDF1α in rats and observed increased endothelialization, including EPC, compared with controls after 4 weeks.66,67 Interestingly, myofibroblast-associated intima hyperplasia could be reduced. Moreover, SDF1α coating significantly reduced the number of platelets attached to the valves of the AVC. The research group of Flameng showed that a combined coating with SDF1α and FN may increase endothelial cell growth on vascular synthetic knitted polyester grafts in an ovine carotid artery interposition model as well as on decellularized AVC in the ovine right ventricular outflow tract.52,68 Furthermore, this combined coating strategy reduced intimal pannus formation, immune response, and calcification of the grafts.
Custom-made synthetic peptides
Since natural bioactive proteins do not allow for selective cell attraction, a recent collaborative work has developed a platform to bind custom-made synthetic peptides onto AG. 8 A proof-of-concept study on different peptides with cell-adhesive sequences suggested a positive effect on graft endothelialization within the first 10 days after heterotopic implantation in the rat aorta.
Summarizing the current evidence for strategies of preimplantation improvement of tissue-engineered cardiovascular implants, it appears feasible to gain significant impact on the in vivo remodeling of grafts based on decellularized donor tissue. However, control over long-term in vivo remodeling is yet an unmet requirement for in vitro modification steps, and early endothelial repopulation has been associated with late neointimal hyperplasia. A more sophisticated approach using dual or multicomponent biofunctionalization appears more appropriate to protect tissue-engineered cardiovascular grafts in vivo in the long term.
Systemic Pharmacotherapy For In Vivo Protection of Tissue-Engineered Grafts
Besides new tissue-engineered biomaterials and various methods of decellularization and supplementary coating strategies, efficient systemic pharmacotherapy can be additionally applied to promote recellularization and to inhibit calcifying degenerative processes (Table 2). Again, the herein presented rat model is well suited to study respective therapeutic approaches in a preclinical setting.
Inhibition of biomineralization and intima hyperplasia
Thompson et al. examined the effect of calcium channel blockers on syngeneically or allogeneically transplanted fresh allografts in rats. 69 It could be demonstrated that the calcium channel blockers verapamil and diltiazem attenuate early calcification, which usually occurs in aortic valves after transplantation. Thus, these agents might influence the durability of aortic valve allografts.
Our research team investigated whether the systemic administration of simvastatin may have an impact on degenerative processes in decellularized AVC transplanted in rats under procalcific diet. 14 Rats were fed with different procalcific diets to induce a hypercalcemia and hyperlipidemia and thereon treated with simvastatin. Rats treated with simvastatin did not show any differences in the extent of calcification compared with controls. Moreover, statin administration neither affected recellularization nor intima hyperplasia.
Another crucial factor causing intima hyperplasia is the platelet-derived growth factor (PDGF) that induces migration and proliferation of smooth muscle cells in the intima of vascular wall. The other way round, PDGF can also be generated by smooth muscle cells, macrophages, and endothelial cells after vascular injury, potentially causing a vicious circle. 70 Deuse et al. showed that intima hyperplasia in balloon-injured human internal mammary arteries exhibited increased PDGF levels. 71 Moreover, pyruvate dehydrogenase kinase isoform 2 was revealed to act as key regulator for new intima hyperplasia. In another rat model, it could be demonstrated that in a balloon-injured aorta, dichloroacetate, a pyruvate dehydrogenase kinase isoform 2-blocker, decreased intima and media hyperplasia and promoted smooth muscle cell apoptosis without inhibiting reendothelialization.
Suppression of immune response
Cyclosporine A is an immunosuppressive drug commonly used to counteract organ transplant rejection, for example, after heart transplantation. Legare et al. examined the impact of cyclosporine A on aortic valve allografts in rats. 72 This study has provided experimental evidence that immune effector cell trafficking to allogeneic valve leaflets after implantation appears to occur via α4 and/or β2 integrin pathways. A continuous cyclosporine treatment of recipients resulted in inhibition of allograft valve infiltration and structural failure. These therapeutic approaches may not indefinitely protect valve leaflets from cellular loss but may reduce the immune infiltration early after implantation. It is possible that attenuating this immune attack may lead to better preservation of the valve and thus prolong the survival of a functional allograft valve.
Recently, it has been demonstrated that pioglitazone, a peroxisome proliferator-activated receptor gamma (PPARγ) agonist, may be a potential candidate to inhibit native heart valve degeneration by downregulating the receptor for advanced glycation endproducts and thereby inhibiting inflammatory cascades. 73 However, up to date, it is unclear whether systemic PPARγ activation may have an impact on the inflammatory and subsequent calcifying processes that occur in biological heart valves and vascular grafts.
So far, the emphasis has been placed on how to promote reendothelialization and to attenuate intima hyperplasia, to decelerate the development of graft insufficiency or even prevent this adverse event. However, another cause of graft failure can be aneurysmal degeneration. In this context, it has been reported that transforming growth factor-β-neutralizing antibodies and selective angiotensin-II type 1 receptor blockers such as losartan may alleviate aneurysmal degeneration.74,75 Using the herein discussed model of infrarenally transplanted abdominal decellularized AG in rats, Lee et al. examined the effectiveness of losartan in vivo. 76 Administration of losartan showed a significantly lower medial elastic fragmentation, a superior medial layer preservation, and relatively more physiological cellular morphology in the intima.
Enhancement of endothelial function
G-CSF is a cytokine that stimulates proliferation and differentiation of hematopoietic progenitor cells and increases the number of neutrophil granulocytes. Zhou et al. hypothesized that G-CSF inhibits intima hyperplasia, and therefore, they examined the impact of G-CSF on decellularized AG in rats. G-CSF stimulated neointima formation 2 weeks after graft implantation and significantly attenuated intima hyperplasia after 6 months. 67 Furthermore, it could be demonstrated that G-CSF stimulated the production of EPC in the peripheral blood and showed better graft patency.
Collecting these findings of pharmacological intervention, modulation of recipient immune response appears to be a potent mechanism of preservation of tissue-engineered cardiovascular grafts. While harsh methods, for example, immune suppression by cyclosporine A, may lead to significant side effects, the challenge in optimal medical therapy will be defined by achieving a balance between favorable effects on the graft versus adverse systemic side effects.
Conclusion
The microsurgical rat model of infrarenal implantation of AG and AVC is a modular platform for the in vivo assessment of biological and tissue-engineered grafts (Fig. 3). By optional addition of procalcific diet, disease-inducing agents such as streptozotocin (STZ) and genetic modifications such as superoxide dismutase (SOD) deficiency, 77 complex multimorbidity scenarios mimicking the clinical reality in many cardiovascular patients can be simulated. Applying this model, crucial aspects of the biocompatibility, biofunctionality, and in vivo degeneration of vascular and valvular implants in dependency on graft preparation and modification as well as systemic antidegenerative treatment of the recipient have been and will be addressed. Considering the current forefront translational challenges in tissue engineering, this model represents an ideal platform for screening and focused research in cardiovascular tissue engineering.

The modular platform for cardiovascular graft evaluation in vivo. AT-II, angiotensin-II type I; CKD, chronic kidney disease; CV, cardiovascular; G-CSF, granulocyte colony-stimulating factor; PPARγ, peroxisome proliferator-activated receptor γ; SDF1α, stromal cell-derived factor 1α; VEGF, vascular endothelial growth factor. Color images available online at
Footnotes
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.