
Abstract
Objective:
Preclinical evaluation of hernia meshes is commonly performed in porcine models. We recently developed two surgically induced porcine hernia models—an incisional and an excisional model—that formed persistent hernias in the absence of graft repair. Herein, we investigate if these models will continue to form a hernia after graft repair.
Materials and Methods:
Ten pigs were used to create two hernia models—a 10-cm partial-thickness incisional defect (n = 5) and an 8 × 8-cm full-thickness excisional defect (n = 5). The defects were repaired using a 12 × 12-cm human acellular dermis graft placed in a preperitoneal/retrorectus sublay position and fixed using transfascial sutures. Postoperative management included the use of suction drainage for 1 week and an abdominal binder for 4 weeks in the more severe excisional model. Hernia development was assessed clinically, and hernia defect size and volume were measured using postoperative computed tomography (CT) imaging over 12 weeks. Radiographic inflation testing (2 L inflation), biaxial mechanical testing, and histological evaluation were also performed at 12 weeks.
Results:
All pigs with the excisional model, but none with the incisional model, developed a clinically relevant hernia. At the end of 12 weeks, the excisional model had a significantly greater hernia defect size (259 ± 51 cm2 vs. 47 ± 16 cm2) and repair volume (865 ± 414 cm3 vs. 85 ± 52 cm3) compared with the incisional model. The excisional model also showed an order of magnitude greater increase in repair volume (280 cm3 vs. 47 cm3) compared with the incisional model upon 2 L inflation. Furthermore, the excisional model showed a trend of having higher dilatational strain at average biaxial load of 250 N and lower stiffness compared with the incisional model. The excisional model had a thin, hypercellular hernia sac spanning the defect, whereas the incisional model had a thick densely fibrotic scar bridging the defect.
Conclusion:
The 8 × 8-cm excisional defect model, together with appropriate postoperative wound management, in the pig model is recommended for preclinical investigation of different grafts for hernia repair. Novel CT imaging and biomechanical testing methods are recommended to measure functional outcomes of hernia repair in preclinical models.
Introduction
V
To overcome the limitations of currently available grafts, there has been a continued effort to develop newer meshes that further improve the long-term durability of VHRs while simultaneously reducing adverse events, such as mesh infection, following VHR. The effectiveness of new hernia meshes and grafts is commonly evaluated in animal hernia models before being used clinically. Whereas mesh biocompatibility is often assessed in small animal models such as the rat, functional outcomes such as repair integrity, hernia formation, and biomechanical properties are studied in large animal models such as the pig. Indeed, various models of hernia injury and repair in the pig model have been reported in the peer-reviewed literature.13–29 However, in several of these studies, the absence of healing an unrepaired defect and the persistence of a hernia at a postacute time point were never verified.13–29 We have recently shown that robust scar formation in certain porcine hernia models may result in spontaneous healing of the hernia. 30 By avoiding injury to the peritoneum, using elastic abdominal binders to support the hernia defect, and using drains to prevent seroma in the early postoperative period, we were able to avoid robust scar formation and create persistent large hernias in the pig model in the absence of a graft repair. Specifically, in our prior work, we developed a 10-cm partial-thickness incisional defect model wherein the posterior rectus sheath and peritoneum were intact and an 8 × 8-cm full-thickness excisional defect model wherein a portion of the rectus abdominis muscle was excised. 30 Both models formed a persistent hernia in the absence of repair, with the excisional model forming larger hernias during the 5-week study. Both models offer the option to perform repair using grafts that are similar in size to grafts used clinically and allow for the placement of grafts in the onlay, inlay, or sublay positions.
Given that we demonstrated two porcine models of persistent hernia in the absence of surgical repair, our next research question was to determine if one or both of these models would be appropriate for investigating the interventional strategy of graft repair. To be an appropriate model for studying graft repair interventions, we need to demonstrate that repair with a graft that fails clinically (i.e., results in hernia recurrence) also demonstrates failure in the animal model. Hence the aim of this study was to investigate if surgically induced incisional and excisional hernia models that form persistent hernias in the absence of a graft repair will also form a hernia after repair with a dermis graft known to fail clinically in human subjects.
Materials and Methods
We created two surgical models of acute ventral hernia injury in porcine models that have been previously shown to form a persistent hernia. 30 The hernia injury in both models was repaired with an acellular dermal graft and evaluated over a 12-week period.
Preoperative and intraoperative details
Ten female Yorkshire pigs (25–30 kg, 3 months old; Michael Fanning Farms, Howe, IN) were used in the study. The pigs were housed under standard conditions and fed twice daily (Teklad Vegetarian Pig/Sow Grower Diet, 2–4% of body weight) throughout the study. All animal care and operative procedures were approved by the Institutional Animal Care and Use Committee (IACUC) at the Cleveland Clinic.
Animals were acclimated for 1 week and fasted for 12 h before surgery. General anesthesia was induced with intramuscular (IM) ketamine (20 mg/kg) and xylazine (2 mg/kg) and maintained by inhalational isoflurane (1–3%) throughout the procedure. Perioperative medications included intravenous (IV) isotonic saline, IV cefazolin (20 mg/kg, every 2 h), IM famotidine (0.5–1 mg/kg), IM buprenorphine (0.005–0.01 mg/kg), and a fentanyl transdermal patch (50 μg/h). Standard abdominal preparation, with abdominal shaving and 70% alcohol and betadine washes, was performed and sterile drapes were placed.
Surgical models of VHR
All repairs were performed on acutely created hernia defects using a 12 × 12-cm human acellular dermis graft (HADM, DermaMatrix; Musculoskeletal Transplant Foundation, NJ) with transfascial suture fixation. The details of each model follow here.
Partial-thickness incisional model with retrorectus repair
A 12-cm midline skin incision was made, and 1-cm-wide skin flaps were raised bilaterally through the avascular prefascial plane. The anterior rectus sheath was exposed and 10-cm incisions were made bilaterally on the anterior rectus sheath along the medial edge of the rectus abdominis muscles to enter the retrorectus space. A 12 × 12-cm retrorectus space was developed by extending the incisions bilaterally to the lateral edge of the rectus muscles and extending medially to connect the two spaces across the midline. The resulting incisional defect was almond shaped and ∼10 × 5 cm in size (Fig. 1A, n = 5 pigs).

Surgical models of ventral hernia defects repaired with a bridging 12 × 12-cm human acellular dermis graft:
The incisional defect was bridged with an HADM placed in the retrorectus sublay location (Fig. 1A). Eight transfascial 2–0 Prolene sutures were used to fix the graft to the overlying musculofascial layer. The sutures were applied using a Reverdin needle 2 cm from the graft edge, spaced about 4 cm apart from each other, and tied in the musculofascial plane through separate buttonhole skin incisions. Each buttonhole skin incision was closed with a single subcutaneous stitch (4–0 PDS).
Full-thickness excisional model with preperitoneal repair
A 10-cm midline incision was made through the skin, subcutaneous fat, and aponeurotic layers, and 5-cm-wide skin flaps were raised bilaterally. An 8 × 8-cm region was marked on the rectus abdominis fascial surface. An 8-cm midline incision was made through the linea alba without violating the parietal peritoneum, and 4 × 8-cm sections of rectus abdominis muscles were resected bilaterally using electrocautery. The resulting excisional defect was rectangular and ∼11 × 10 cm in the craniocaudal and transverse directions, respectively (Fig. 1B, n = 5 pigs).
The excisional defect was bridged with an HADM that was placed in the preperitoneal sublay position with ∼2 cm of edge overlap (Fig. 1B). Sixteen transfascial 2–0 Prolene sutures were used to fix the graft to the overlying musculofascial layer. The sutures were applied using a Reverdin needle 2 cm from the graft edge, spaced about 2 cm apart from each other, and tied.
Radiopaque marker placement
To permit computed tomography (CT)-based monitoring of the hernia defect and repair graft, radiopaque markers were placed around the defect edge as well as on the graft surface (Fig. 1A, B). Eight interrupted radiopaque polypropylene suture tags (USP-0; Viscus Biologics, Cleveland, OH) were used to mark the defect edge. Twenty-one 1.6-mm diameter tantalum beads (Tilly Medical Products, Lund, Sweden) were affixed to the graft surface using 5–0 Prolene suture in a distributed axisymmetric pattern just before implantation.
Incision closure and postoperative management
Closed suction drainage was used to mitigate postoperative seroma formation in pigs with the excisional model only due to the dead space created by the excisional defect and the wide skin flaps. Specifically, a Jackson-Pratt (JP) drain (flat fully perforated drain, SU130-1311, 400 mL reservoir, SU130-1000, Cardinal Health, Dublin, OH) was placed in the subcutaneous space just before skin closure. Subsequently, the midline skin incision in all pigs was closed in layers using subcutaneous interrupted 2–0 PDS/2–0 Vicryl and subcuticular running 4–0 PDS sutures. A long-term postoperative bandage (Aquacel™ Ag; ConvaTec, Skillman, NJ) was applied over the skin incision. In addition, in pigs with the excisional model only, a modified abdominal elastic binder (3-Panel Binder, TruForm®; OTC, Cincinnati, OH) was used during the first 4 weeks postoperatively to support the hernia defect and mitigate seroma formation. The binder was secured with a modified adjustable mesh jacket (Lomir Biomedical, Malone, NY) (Fig. 2B). The binder and jacket were not used in the pigs with the partial-thickness incisional defect model because seromas were not observed in this model in a previous study. 30

Postoperative appearance of pigs with HADM repair over 12 weeks. Pigs with the excisional model were placed in an abdominal elastic binder secured with a mesh jacket for 4 weeks
Postoperatively, the pigs were fed a softened diet for 1 day and their regular diet thereafter. Postoperative analgesia was provided by the Fentanyl transdermal patch (applied preoperatively; Preoperative and intraoperative details section), IM buprenorphine (0.005–0.01 mg/kg, two doses on the day of surgery), and IM meloxicam (5 mg OD on the day of surgery and the day after if required). Oral cephalexin (20–25 mg/kg BID) was administered for 5 days postoperatively. All animals were monitored for postoperative complications and seroma and clinical evidence of hernia (Fig. 2) during the 12-week course of the study.
Postoperative CT imaging and analysis
All pigs were imaged using a Dyna-CT (Axiom Artis system; Siemens Medical Solutions USA, Inc., Malvern, PA) immediately postsurgery (0 week) and at 4, 8, and 12 weeks. For CT imaging, animals were anesthetized as previously described and placed in a prone position on a custom donut-shaped frame such that their ventral abdominal wall remained unsupported during the scan (Fig. 3A). CT image sets from each time point were analyzed using custom software (Hernia Tracker; ImageIQ, Cleveland, OH). Specifically, CT acquired raw 16-bit DICOM images (396 images; 463 μm isotropic voxel resolution) were compiled and thresholded to identify the radiopaque marker arrays. The respective marker arrays—graft surface (21 tantalum beads) and defect perimeter (eight radiopaque suture tags)—were then surface-fitted using a three-dimensional triangular mesh algorithm to calculate the repair volume and defect area (Fig. 3B). 31
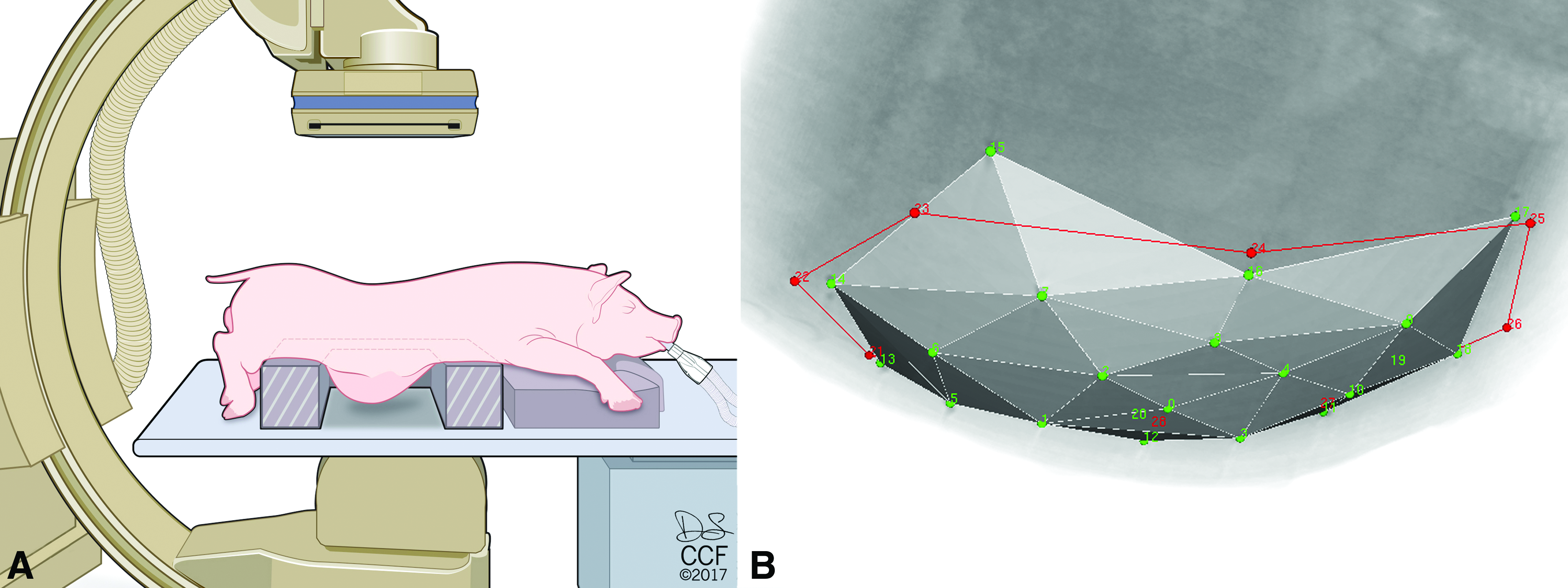
Postoperative CT imaging and analysis.
Euthanasia
Immediately after CT imaging at postoperative week 12, a systemic muscle relaxant (0.7 mg/kg rocuronium bromide, IV) was administered to prevent postmortem muscle contracture for subsequent inflation and mechanical testing. 32 After 5 min, the pigs were euthanized (0.2 mL/kg Beuthanasia, IV; Intervet/Merck Animal Health, Madison, NJ).
Endpoint inflation testing
Immediately following euthanasia, with the pigs in a supine position, the abdomen was opened and skin flaps were raised up to the flanks. A 16-inch diameter latex balloon was inserted into the peritoneal cavity through a 9-cm-long suprapubic incision. Cotton umbilical tape was tied to the cranial end of the balloon and brought out through a 1-cm incision near the xiphoid process. The balloon was connected to a silicone tube through a three-way stop cock. The silicone tube and the umbilical tape were used to center and secure the balloon under the graft repair region, and the suprapubic incision was closed (Fig. 4). The balloon was inflated with water using a peristaltic pump (Masterflex 7553; Cole-Parmer, Vernon Hills, IL) at 1 L/min. CT scans were obtained (as in the Euthanasia section) at 0, 1, and 2 L of inflation to visualize the radiopaque markers and calculate repair volume (0 L) and change in repair volume upon inflation (1 and 2 L).
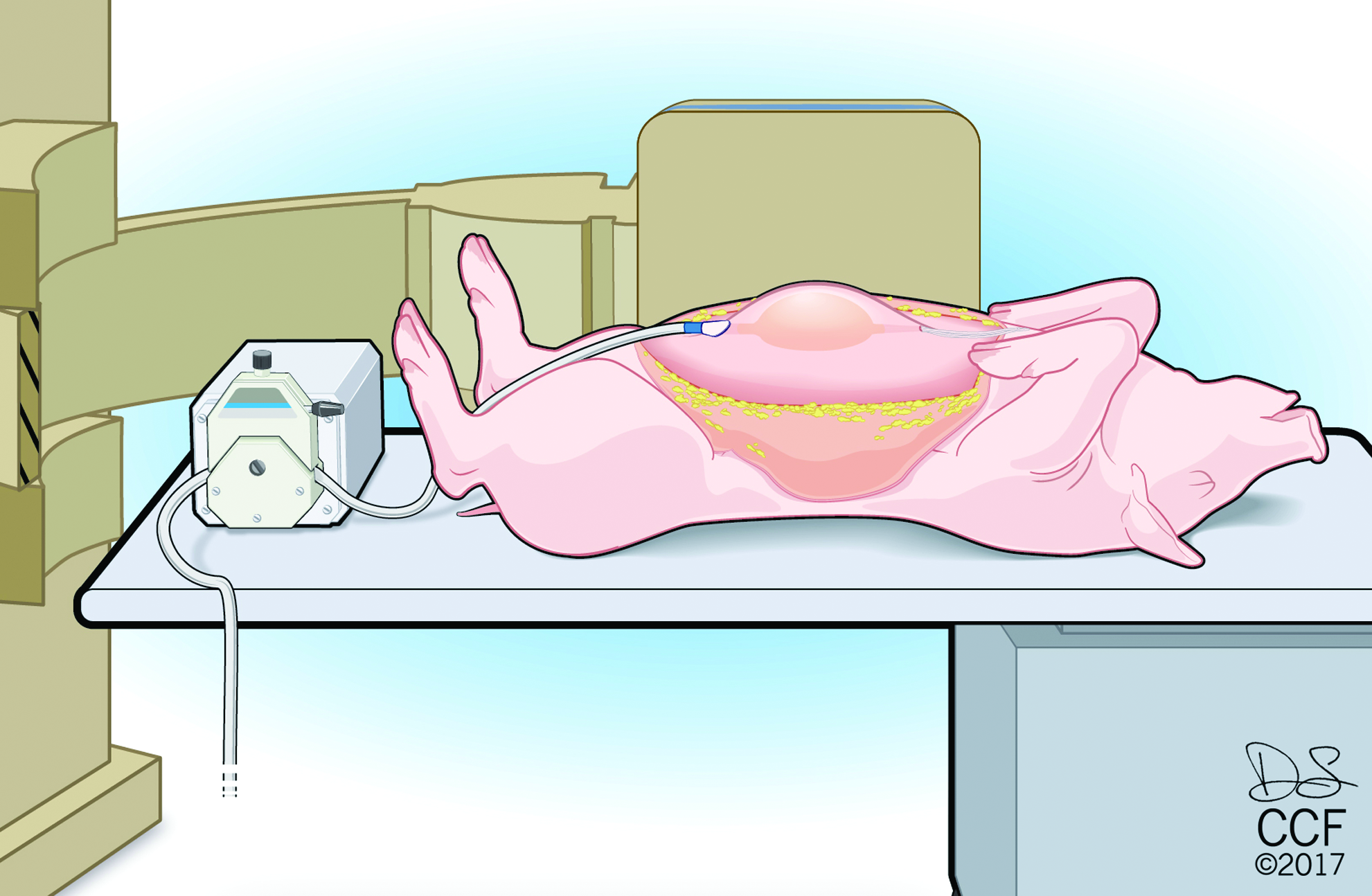
Endpoint inflation testing (12 weeks). After euthanasia, the pigs were placed in a dorsal recumbent position (supine) on the CT bed. Skin flaps were raised up to the flanks to expose the hernia repair area. A 16-inch diameter latex balloon was inserted into the abdominal cavity, positioned under the repair, and inflated with water using a peristaltic pump. CT scans of the abdomen were obtained at 0, 1, and 2 L of inflation to visualize the radiopaque markers. CT images were then analyzed using custom software to calculate hernia repair volume (0 L) and change in repair volume upon inflation (1 and 2 L). Reprinted with permission, Cleveland Clinic Center for Medical Art & Photography © 2017. All Rights Reserved. Color images available online at
Endpoint biaxial mechanical testing
After inflation testing, 25 × 25-cm portions of the ventral abdominal wall, including the repair region, were resected en bloc and tested within 2 h postmortem. Tests were conducted using a planar biaxial test machine (ADMET, Inc., Norwood, MA; Fig. 5) equipped with two 250 lb load cells and a synchronized video system (Scorpion SCOR-1450C CCD camera; Point Grey Research, Inc., Richmond, Canada; StreamPix image acquisition software; Norpix, Inc., Quebec, Canada). The explants were affixed to the test fixtures using metal hooks (seven per side). A 15 × 15-cm region of interest that included the repair region was denoted on the explant surface by eight ink marks (Fig. 5). For testing, the explants were first reapproximated to their 25 × 25 cm in vivo dimension, which was considered the zero position. Explants were then preconditioned equibiaxially (2–10 N, five cycles) and then loaded equibiaxially at 100 N/min to a subfailure load of 250 N. The eight ink surface markers on select test images were localized by texture correlation 33 using a custom software (Motion Analyst, v.1.5) 34 and then analyzed using a quadratic quadrilateral element-based finite element analysis (custom MATLAB script) to estimate average dilatational strains (percent increase in area) of the explant at given loads. The linear stiffness was calculated from the slope of a linear fit of the average biaxial load versus dilatational strain curve between 100 and 200 N of load.
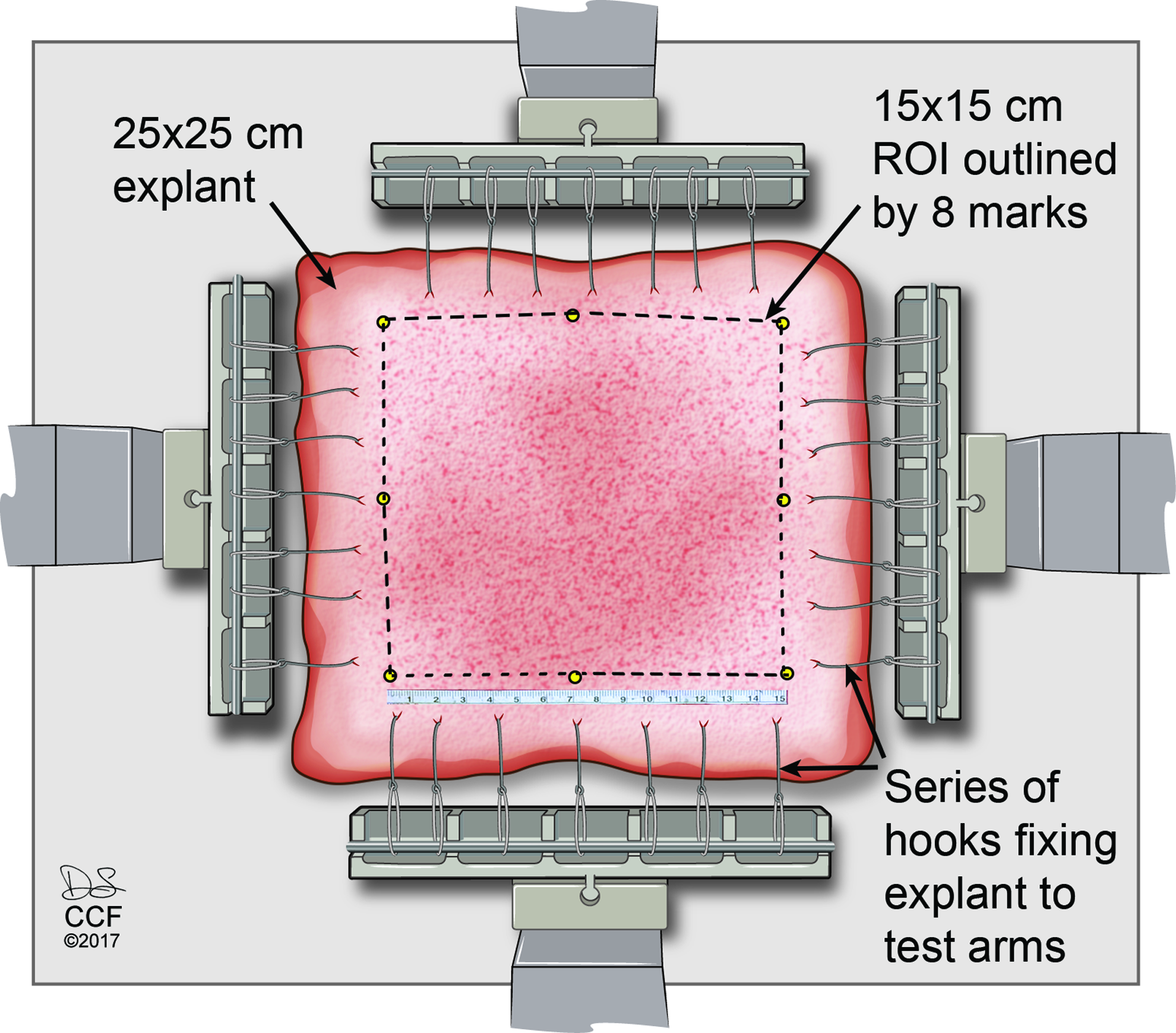
Endpoint biaxial mechanical testing (12 weeks). A 25 × 25-cm portion of the ventral abdominal wall inclusive of the hernia repair region was resected en bloc and tested using a custom planar biaxial test machine equipped with a synchronized video system. A 15 × 15-cm region of interest was denoted on the explant surface by eight ink marks and used to monitor displacement. The explants were loaded equibiaxially at 100 N/min to a subfailure load of 250 N. ROI, region of interest. Reprinted with permission, Cleveland Clinic Center for Medical Art & Photography © 2017. All Rights Reserved. Color images available online at
Necropsy and histology
After inflation and subfailure mechanical testing, the abdominal wall explant was carefully inspected for thickness and nature of any hernia sac and evidence of graft remodeling and incorporation. Subsequently, three 1 × 2-cm transverse tissue strips were harvested from around the defect/hernia interface. The tissue samples were fixed in 10% neutral buffered formalin and processed for routine paraffin embedding and histology. After hematoxylin and eosin (H&E) staining, the histology sections were scanned in their entirety at 20 × using a Leica SCN400F scanner (Leica Microsystems, GmbH, Wetzlar, Germany). A representative section from each animal was descriptively reviewed for general morphology of the hernia sac and graft repair.
Results
Clinical course
All pigs had an uneventful recovery from surgery. One pig in the excisional model developed a deep surgical site infection secondary to drain line infection in the second postoperative week. The infection was managed with antibiotics (oral cephalexin and IM metronidazole), but based on the 4-week CT findings of compromised graft integrity, the pig was euthanized and excluded from the study. No postoperative complications were observed in the other pigs. None of the five pigs with the incisional model developed a hernia at any postoperative time, whereas all pigs with the excisional model developed hernias by 8 weeks that enlarged over the subsequent 4 weeks (Fig. 2 and Table 1).
Defect area and repair volume
Defect area and repair volume did not change appreciably over time in pigs with the incisional model, but increased significantly in pigs with the excisional model (Fig. 6 and Table 2). Comparing the two models, defect area was significantly lower in the incisional model compared with the excisional model at all time points (p < 0.001). Repair volume in the two models was not significantly different at week 0 (p = 0.118), but repair volumes were significantly higher in the excisional model by 4 weeks and thereafter (p < 0.05).
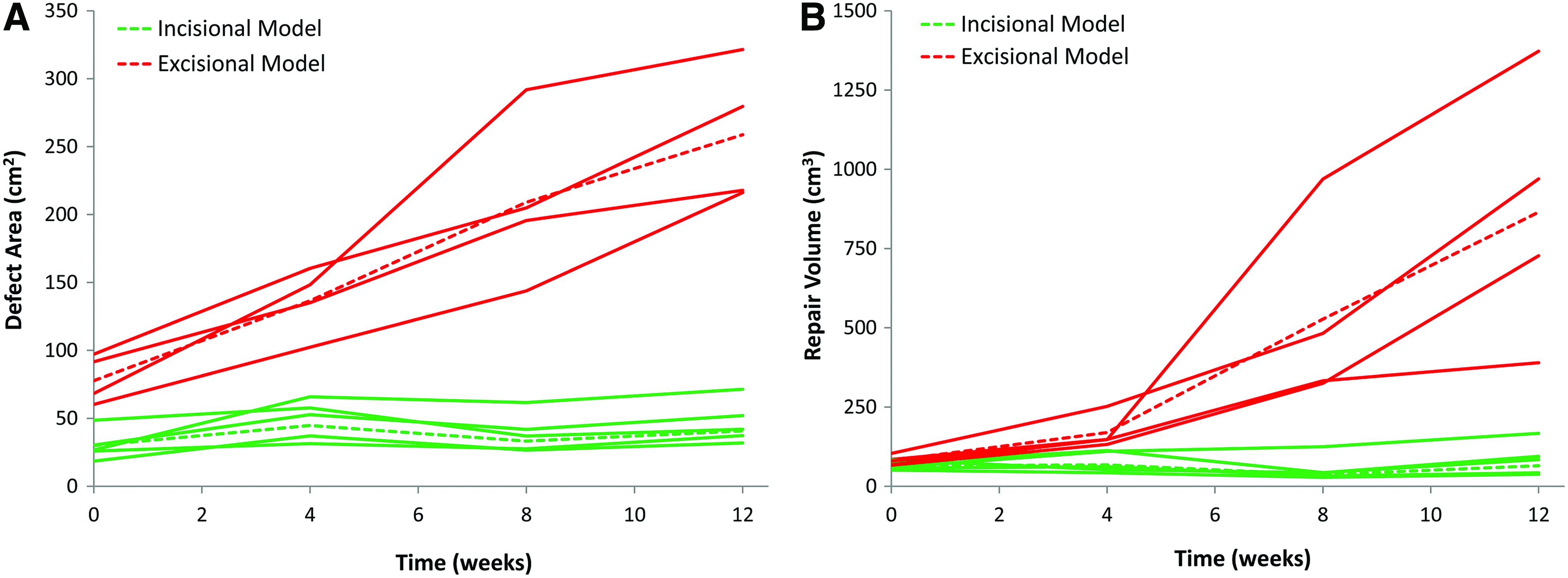
Change in hernia
a–g: letters indicate significant differences (p < 0.05) in one-way repeated measures ANOVA.
n = 4, as one pig was euthanized at 4 weeks due to surgical site infection.
ANOVA, analysis of variance.
Endpoint inflation testing
The repair volume approximately doubled with inflation in both models, with essentially all of the volume change occurring by 1 L inflation (Fig. 7). The absolute increase in repair volume was an order of magnitude higher (280 cm3) in the excisional model compared with the incisional model (47 cm3). The differences between the two groups were significant at 0, 1, and 2 L of inflation (p < 0.05).

Endpoint inflation test results (12 weeks). The repair volume approximately doubled with inflation in both models, with essentially all of the volume change occurring by 1 L inflation. The absolute increase in repair volume was an order of magnitude higher (280 cm3 vs. 47 cm3) in the excisional model (red lines; all pigs developed clinical hernias) compared with the incisional model (green lines; no pig developed a clinical hernia). Dashed lines represent the average curves of each group. a–d: letters indicate significant differences (p < 0.05) in one-way repeated measures ANOVA. *n = 4, as one pig was euthanized at 4 weeks due to surgical site infection. ANOVA, analysis of variance. Color images available online at
Endpoint biaxial testing
Biaxial load versus dilatational strain curves are shown in Figure 8. Compared with the incisional model, repairs in the excisional model appeared to be more compliant. The excisional model showed a trend of having higher dilatational strain at average biaxial load of 250 N (p = 0.062) and lower stiffness (p = 0.048) compared with the incisional model.
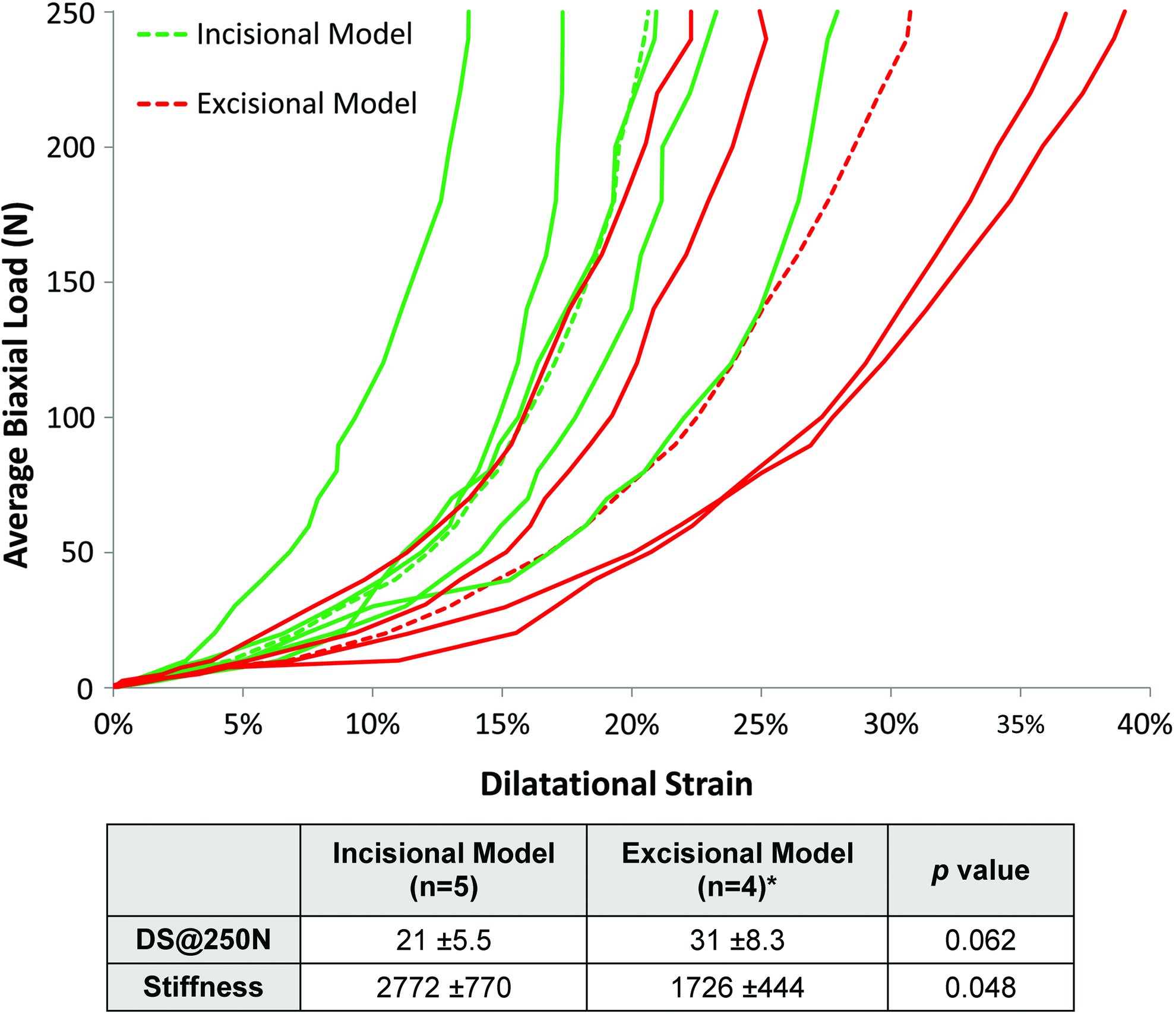
Endpoint biaxial test results (12 weeks). Compared with the incisional model (green lines; no pig developed a clinical hernia), repairs in the excisional model appeared to be more compliant (red lines; all pigs developed clinical hernias). Dashed lines represent the average curves of each group. *n = 4, as one pig was euthanized at 4 weeks due to surgical site infection. DS@250 N: dilatational strain at average biaxial load of 250 N. Color images available online at
Necropsy and histology
Pigs with the incisional model had a contracted hernia defect that was filled with scar tissue overlying a partially resorbed dermis graft in the retrorectus space (Table 1 and Fig. 9A). In contrast, pigs with the excisional model had an enlarged hernia defect lined by a thin hernia sac overlying a partially resorbed dermis graft in the preperitoneal space (Table 1 and Fig. 9B).
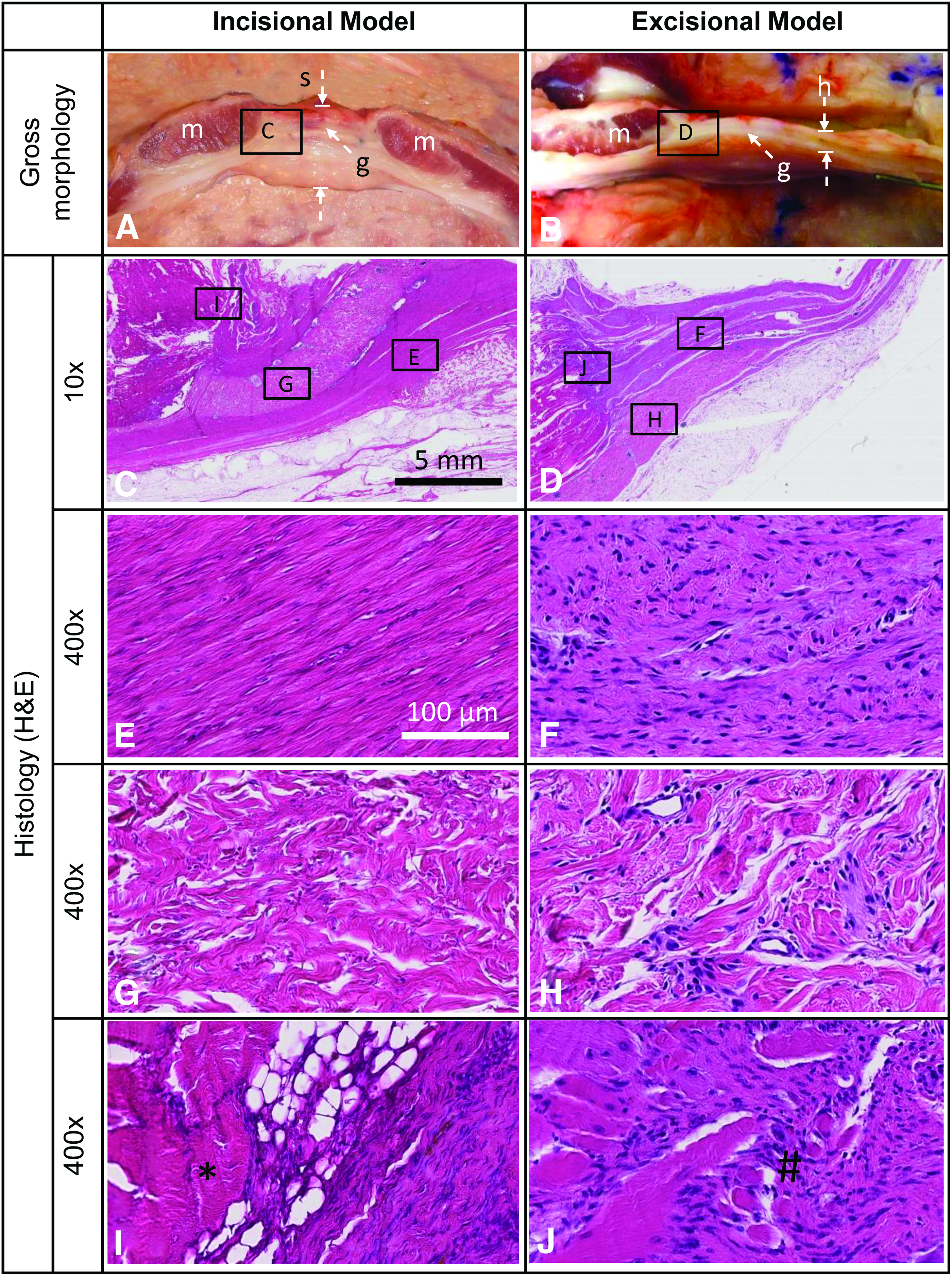
Representative necropsy and H&E-stained histology images (12 weeks).
Representative H&E sections from the defect edge are shown in Figure 9C–J. In the incisional model, the defect was bridged by dense fibrotic scar tissue with relatively few cells (Fig. 9C, E). In the excisional model, a thin hernia sac that was relatively less fibrous and highly cellular spanned the defect (Fig. 9D, F). The dermis graft showed evidence of vascularization and cellular infiltration by inflammatory cells and spindle-shaped fibroblast-like cells in both models (Fig. 9G, H). In the incisional model, the defect edge showed intact rectus muscle lined by fibro-fatty fascial tissue (Fig. 9I). In the excisional model, the defect edge showed evidence of muscle injury, repair (muscle fibers with abnormal irregular cross sections, multiple central nuclei), and inflammation (Fig. 9J).
Discussion
We investigated the healing and persistence of a hernia following repair using a human dermis graft in two surgically induced models of hernia injury in the pig that have previously been shown to form persistent hernias in the absence of a graft repair. 30 We found that the 10-cm, partial-thickness, incisional defect model did not form a hernia following repair using a human dermis graft. However, the 8 × 8-cm, full-thickness, excisional defect model repaired with a human dermis graft formed a large persistent hernia during the 12-week study.
Our results highlight the challenges of predicting clinical results using porcine hernia models. Although both models formed persistent hernias in the absence of graft repair, only the excisional model, but not incisional model, developed a hernia following repair with a dermis graft. This difference in clinical outcome could be attributed to differences in severity and/or plane of surgical defects in the two models. The smaller and less severe incisional model (40-cm2 defect with intact posterior rectus sheath) and the larger and more severe excisional model (100-cm2 defect with portions of rectus abdominis muscle and sheaths removed) were both repaired using similar 144-cm2 HADMs in a bridging sublay manner. It is likely that the graft was loaded to a higher extent in the larger and more severe excisional model, resulting in greater stretching and bulging than in the incisional model. Furthermore, since both models were repaired using similar sized grafts, the amount of graft–host tissue overlap was greater in the incisional model compared with the excisional model, potentially allowing superior integration and repair outcomes. It is also possible that the retrorectus space (between rectus muscle and posterior rectus sheath) where the graft was placed in the incisional model was more conducive to wound healing and fibrous tissue formation than the preperitoneal space (between posterior rectus sheath and peritoneum) where the graft was placed in the excisional model. It is noteworthy that our results of hernia occurrence/persistence in only the excisional model, but not the incisional model, correlate with clinical reports of increased hernia recurrence when biologic grafts are used in bridging repairs of large hernia defects in human patients.7,8,35,36
For an animal model of hernia repair to be clinically relevant, it should not only form persistent hernias in the absence of any repair but also allow repair using surgically relevant techniques and mesh sizes. The two models investigated in this study met the above criteria. 30 Furthermore, to be an appropriate model for studying graft repair interventions, the model must also demonstrate that repair with a graft that fails clinically (as hernia recurrence) also fails in the animal model. Results from this study show that the more severe, full-thickness excisional model, but not the partial-thickness incisional model, formed persistent hernias after repair using human dermis grafts. These findings suggest that the excisional model would be appropriate for studies aiming to demonstrate superior graft performance of new hernia meshes and grafts over HADMs.
We also described three novel test methods for functional assessment of hernia repair outcomes. First, we used postoperative CT imaging of radiopaque markers to longitudinally monitor hernia defect area and repair volume (bulging) under the physiologically simulated conditions of an unsupported abdominal wall. Second, we used endpoint inflation testing to assess hernia function in situ, and third, we used biaxial mechanical testing of the entire abdominal wall explant to assess hernia function ex vivo under well-defined boundary conditions. Biaxial construct testing of the entire abdominal wall simulates the two-dimensional nature of physiologic loading in the abdominal wall and arguably provides a clinically relevant assessment of graft mechanical performance that cannot be captured by uniaxial tests of tissue strips.37,38 We note that larger defect areas and repair volumes (measured by CT imaging) and higher repair strain/lower stiffness (measured by endpoint mechanical testing) were correlated with the clinical observations of hernia recurrence in our porcine subjects, suggesting their validity as functional outcomes for hernia repair. We expect these novel methods and outcomes will allow future researchers to objectively assess hernia repair function in the porcine model and investigate the effectiveness/superiority of interventional repair strategies while potentially reducing animal requirements.
Our study had a few limitations that are inherent to animal models. First, we surgically created acute hernias in young, healthy rapidly growing animals. Thus, our porcine models did not perfectly replicate the patient demographics and clinical scenario of incisional hernias, which commonly present as a chronic condition in older subjects with multiple comorbidities. Despite that limitation, the critical-sized porcine model developed in this study is a significant improvement over previous models and will permit preclinical investigation of grafts for hernia repair. Furthermore, graft assessment in animal models could potentially be supplemented by assessment in computational models that are based on human anatomical and biomechanical parameters. Second, we used a small number of animals and investigated hernia outcomes over a relatively short study duration. Nonetheless, we were able to demonstrate important characteristics that significantly differentiated the two models over the study duration, in part, because of longitudinal CT monitoring of hernia repair area and volume.
In conclusion, the more severe, full-thickness excisional model, but not the partial-thickness incisional model, formed persistent hernias after repair using human dermis grafts. We therefore propose the use of the excisional model as a critical-sized hernia model for preclinical investigation of comparative effectiveness of different grafts for hernia repair.
Footnotes
Acknowledgment
The authors thank Dave Schumick, MS, for preparing the artwork used in the study.
Authors' Contributions
S.S., K.A.D., and M.J.R. designed the study. S.S., A.R.B, and I.N.H executed the study. S.S. and A.R.B. collected the data. S.S. analyzed the data. All authors participated in data interpretation. S.S. drafted the article. All authors participated in critical revision of the article and approved the final version to be published.
Disclosure Statement
S.S. has patent applications on graft technologies, has rights to royalties related to the radiopaque marker used in this study, and owns stock in CR Bard, Medtronic, and Johnson & Johnson. K.A.D. has patent applications on graft technologies, has rights to royalties related to the radiopaque marker used in this study, and is a paid consultant for GlaxoSmithKline and Orthofix. M.J.R. has received funds from Bard Davol and W.L. Gore and Associates, Inc., as a paid consultant or speaker and serves on the board of Ariste Medical. Other authors report no proprietary or commercial interest in any product mentioned or concept discussed in this article. This research was funded, in part, by a Commercialization Grant (No. 1204) from Cleveland Clinic Innovations and a Development Grant from Department of Surgery, Cleveland Clinic.