
Abstract
Kidney regeneration is a complex process that can only be studied in vitro at a limited capacity due to the inherent structural and functional complexity of its tissues. Thus, a suitable platform for conducting cellular response and development should be established from decellularized tissues with intact microarchitecture. In this study, a modular streamlined system was developed to allow manageable handling and setup of in vitro studies using decellularized rat kidneys. The system is composed of commercially available parts that can be reused, interchanged, and reconfigured based on the desired experimental stage and process. Decellularization was confirmed through time-lapse observation, stained tissue sections, genetic material quantification, and protein analysis. The capacity of the bioreactor design to support cell-seeded decellularized kidney constructs was tested by determining viability of seeded podocytes and endothelial cells. Based on the results, decellularized kidneys with renal proteins and intact microstructures can be achieved in relatively shorter periods compared (12 h) to established protocols (96–120 h). The minimalistic kidney bioreactor design not only maintained sterility of decellularized kidney without cells but also permitted manageable maintenance of cell-immobilized constructs for up to 1 week. Through this streamlined system, sustainable and reproducible in vitro experiments for kidney regeneration can be designed and conducted using decellularized kidney as a platform for cell growth and development.
Introduction
W
Owing to the complex architecture of the kidney, repair and regeneration of diseased kidneys are very difficult. Conventional treatment for malfunctioning kidneys involves pharmaceuticals and dialysis, or total organ replacement. However, dialysis is not a suitable long-term solution for renal failure, while patients who are fortunate enough to receive renal transplants must maintain immune suppression for their entire lives to ensure graft patency.4,10–15
Over the past decades, there has been an increased interest in stem cells as therapeutic agents for kidney repair. Although noteworthy steps have been taken in developing cell-based therapies, stem cell-based treatments are most likely limited to mitigating reduced renal function rather than providing an actual, long-term solution to end-stage renal failure.16,17 Various studies have already been conducted on this issue using different animal models and different cell types.18–21
Parallel to developing cell-based therapies, attention toward using acellular biologically derived materials has also increased in the past decade. An ideal use for acellular tissue is in organ reconstruction/regeneration. If the decellularization method preserves the proper microarchitecture of a complex organ, the resulting extracellular matrix (ECM) could then be repopulated with cells suitable to the intended recipient.22–29 However, efficient cell delivery systems are still a long way from achieving functional regeneration of diseased kidneys under clinical conditions,18,30,31 and current studies using recellularized constructs are a long way from producing functional ex vivo organs.25,32–37
Thus, there is a substantial gap between the relevant research and the ability to translate derivative technology to organ regeneration. In response to this gap, a streamlined system should be developed to enable relatively high output of acellular kidneys with an integrated system that facilitates manageable transition to in vitro studies. This study aims to develop streamlined conditions for decellularization that will produce decellularized kidneys that possess original tissue architecture and structural integrity suitable for recellularization. The system can be adapted for both decellularization and recellularization experiments. The units comprising the system are composed of biologically inert components that can be sterilized and reused.
Experiments were conducted using rat kidneys as a small animal model; these organ samples were more suitable and practical for observing cell immobilization under in vitro conditions. Characterization of the resulting decellularized kidney tissue was done by surveying and analyzing the components that remain on the ECM. The sterility and functionality of the bioreactor design were tested by observing the viability of cells delivered through the renal artery and the ureter. Improvements regarding the decellularization technique were optimized for small animal models to achieve the fastest results.
Materials and Methods
Chemicals
Antibodies against Podocin, Nephrin, and Na-Cl cotransporter (NCCT) were purchased from Abcam (Cambridge, United Kingdom), while Na/K ATPase was purchased from Santa Cruz Biotechnology, Inc. (Dallas, TX). Calf pulmonary arterial endothelium (CPAE) cells, Eagle's Minimum Essential Medium (EMEM), and fetal bovine serum (FBS) were purchased from ATCC (Manassas, VA). Podocyte cells, conditionally immortalized cells from mouse, were given by Dr. Eun Young Lee and Dr. Jeong Suk Kang (Department of Internal Medicine, Soonchunhyang University College of Medicine, Cheonan, Korea) and cultured based on previous protocols.38–40 Dulbecco's Modified Eagle Medium (DMEM) was purchased from GE Healthcare Life Sciences (Little Chalfont, United Kingdom). Sodium dodecyl sulfate (SDS), Triton X-100 (TX), and phosphate-buffered saline (PBS) were all purchased from Sigma Aldrich. Penicillin/streptomycin (PS) and amphotericin B solution (WELGENE, South Korea) were used as antibiotic and antimycotic supplements.
Both the decellularization chamber and the recellularization bioreactors are composed of the same commercially available components that can be sterilized and reused, although they are configured differently. Most materials are preassembled before autoclave sterilization. A clean bench with functioning laminar air flow and UV sterilization is used as the main work bench for parts assembly and for the processes of decellularization and cell delivery.
Design of the decellularization system
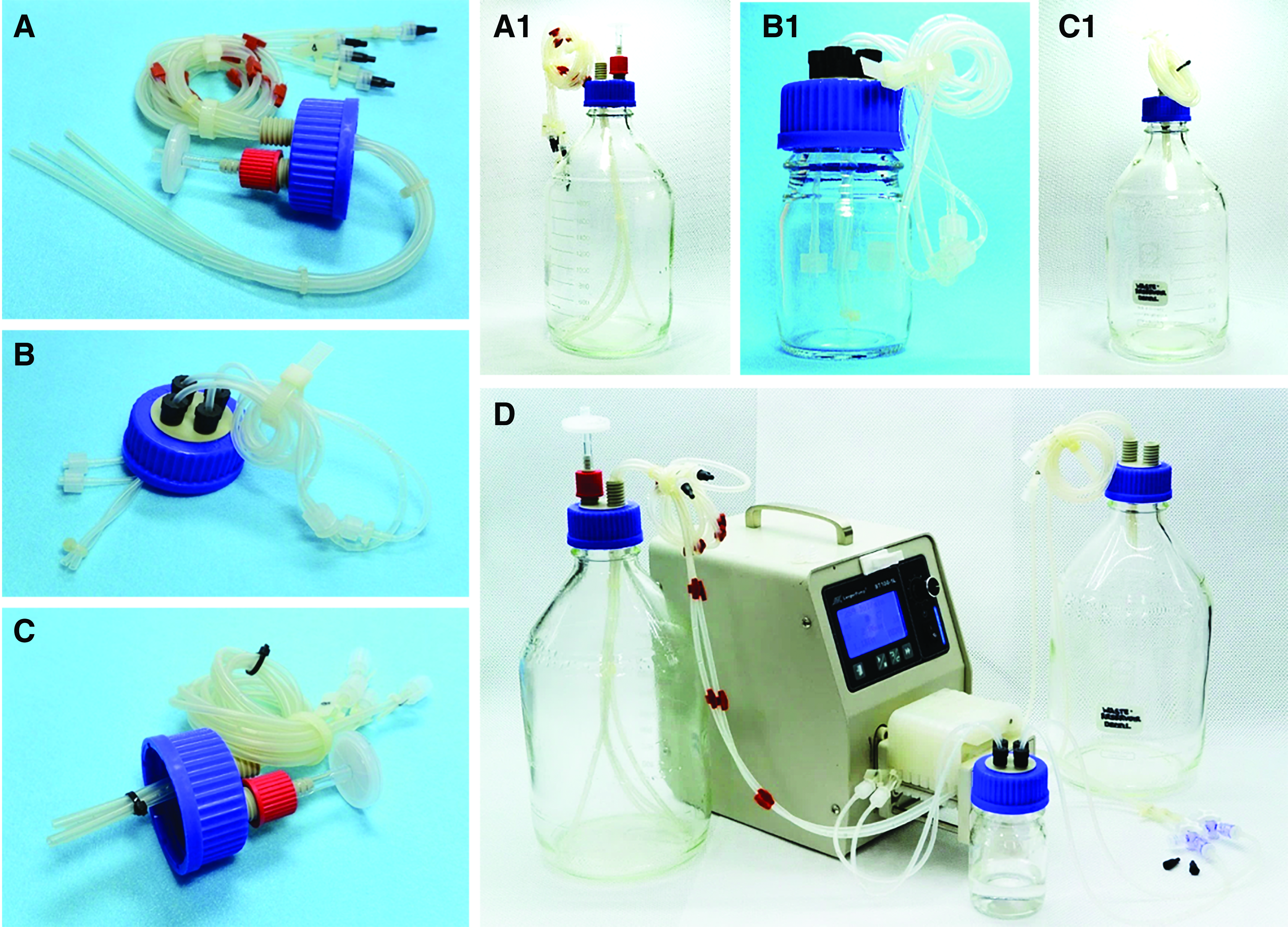
The configuration of the components of the decellularization system is shown in Figure 1. The decellularization setup is composed of three main parts: a solution reservoir, a decellularization chamber, and a waste reservoir. The solution reservoir is a 2000 mL bottle (Schott Duran® Laboratory Bottle Order No. 21 805 63) with a complete set of two-port cap (Schott Duran 2 Port GL45 Screw cap, Order No. 11 297 50) with four silicone tubing (Longer Precision Pump Co., Ltd., Peristaltic Silicone tubing 2 × 1) inserted in one port and a filter on the remaining port, which allows the reservoir to support at least four decellularization chambers at a time (Fig. 1A).
Reservoir cap configuration
Alternatively, the filter can be removed to allow insertion of four additional silicone tubing, which allows simultaneous perfusion into a maximum of eight decellularization chambers. The tubing extends from the inner bottom of the bottle to maximize the amount of solution that can be effectively delivered (Fig. 1A1). The distal portion of the tubing is equipped with 3/16″ male luer-lock polypropylene connectors (NanoNC, NNC-MF-3/32), which can then be attached to the inlet tubing of the decellularization chamber.
The decellularization chamber is a 100-mL bottle with a four-port GL45 (Schott Duran Laboratory Bottle Order No. 21 805 24) cap with silicone tubing inserted in each port (Fig. 1B). A pair of tubing with a male luer-lock adaptor along the inner length and extending inward about 1–2 cm from the cap is designated as the inlet for perfusion of the decellularization/washing solutions. The inlet tubing also has female luer-lock polypropylene connectors (NanoNC, NNC-FF-3/32) on the opposite end to allow for inclusion of a medical-grade three-way stopcock and for connection with the solution reservoir.
The remaining pair of tubing is designated as drains for the removal of waste solution and maintenance of fluid levels. The inner length of the drain tubes extends to the bottom of the chamber and they have male luer-lock connectors along their outer lengths. The decellularization chamber can accommodate a maximum of two small animal kidneys. The waste reservoir is composed of the same components as the solution reservoir. Only one port of the two-port cap is equipped with four silicone tubing, limiting the maximum number of decellularization chambers that can be supported to four.
The outer length of the tubing is equipped with a female luer-lock connector to allow for assembly with the decellularization chamber, and the inner length does not extend down to the bottom of the bottle (Fig. 1C–C1). The remaining port is connected to an external vacuum system that allows the removal of accumulated waste fluids without replacing the reservoir bottle. The silicone tubing attached to both the solution reservoir and the waste reservoir is mounted onto the pump heads (Longer Precision Pump Co., Ltd., DG-8) of the peristaltic pump (Longer Precision Pump Co., Ltd., BT100-1L) in an anterograde (input) and retrograde (drain) manner (Fig. 1D). All silicone tubing used for this setup have 1 mm thick walls, 2 mm inner diameter with ultra-smooth inner linings, low protein absorption, and good flexibility, and tolerates temperatures up to 238°C.
Procedure for kidney decellularization
Kidneys were extracted from animals (Sprague-Dawley rats) that were scheduled for sacrifice. This was done to maximize the use of animals being used for other experiments and to avoid unnecessary killing of pristine animals. Animal experimentation was done based on ethical guidelines with corresponding approval from the Soonchunhyang University Ethics Committee. Aseptic techniques were exercised during the extraction procedure to minimize contamination. All materials and surgical equipment were either medical grade or autoclaved.
1. Before extraction, the animal is anesthetized by inhalation of 2.0% isoflurane gas. Fur is shaved off from the abdominal area. Then an incision is made along abdomen, taking care not to puncture the intestines, to fully expose the abdominal organs.
2. Systemic heparinization is done by locating the major abdominal vein and injecting 1000 U/kg of heparin using a 24-gauge needle. The heparin is allowed to circulate for about 5 min, after which the animal is finally euthanized with an overdose of diethyl ether.
3. The internal organs are retracted to the left side and the kidneys are located along the length of the spinal column. The priority kidney, on the left side, is identified as the one located along the left side of the animal (right side facing the researcher). This kidney is preferred for sample preparation because it is associated with an ample length of artery and vein for processing.
4. The kidney capsule is carefully removed, together with the surrounding fat, and the corresponding ureter and vessels are identified. The ureter is cut to a length (≈2–3 cm) that allows proper isolation of the kidneys. Hemostatic clamps are used to clip the junctions on which the renal artery and veins originate from the inferior vena cava. This is done to avoid unwanted bleeding, which could occlude visibility. The vessels are severed along the sides of the clipped hemostats.
5. The isolated kidney is placed in sterile saline supplemented with 10% antibiotics (1:1 ratio of PS and amphotericin B) before processing.
6. To prepare the extracted kidney for decellularization, all remaining fat is carefully dissected away from the organ. The renal vein and artery are then identified and isolated, and a medical-grade catheter (30 gauge) is carefully inserted into the renal artery. All catheters are secured with 5-0 nylon sutures. The attached catheter then allows for connection to a silicone tubing using a male luer-lock adaptor. Cannulation of the ureter is optional based on the planned cell immobilization experiment.
7. Before mounting, the inlet tubing of the decellularization chamber is prefilled with distilled autoclaved water. The outer length of the inlet tubing is attached to the solution reservoir using a medical-grade three-way stopcock. The inlet tubing is then coupled to the peristaltic pump and the first decellularization solution is perfused until the chamber is half full.
8. Drainage is tested by attaching the drain tubing to the waste reservoir and coupling these with the pump in retrograde manner. The setup is run with an active inlet and drain at the highest possible flow rate for 2 min. If the level of fluid inside the chamber does not change, the system is considered functional; otherwise, adjustments are applied to reach the necessary equilibrium (Fig. 1D).
9. The extracted kidneys are mounted inside the prefilled decellularization chamber after first suspending the multiport cap using a clamping mechanism. The flow rate is decreased to 0.5 mL/min. Using serrated hemostatic clamps, the catheter of the renal artery is coupled with the male luer-lock connector of the inlet tubing (Fig. 2A). The coupled organ is then carefully lowered into the chamber, using the prefill solution as a suspension to avoid decannulation.
10. The kidneys are pumped full of 1% SDS for 4 h followed by 1% TX for another 4 h (Fig. 2B1–3). The rate is increased every 2 h from 1.0 to 2.0 mL/min, with rate increases equally divided into the 8-h period.
11. The decellularized kidney is then washed with autoclaved distilled water for 1 h to ensure complete removal of decellularization agents (Fig. 2B4). This is followed with a sterile PBS flush, after which antibiotics consisting of 5% penicillin–streptomycin and amphotericin B are loaded through the three-way stopcock (Fig. 2B5–6). Samples can be kept in the decellularization chamber or transferred into a sterile bottle containing antibiotic-supplemented PBS, and stored at 4°C until use.
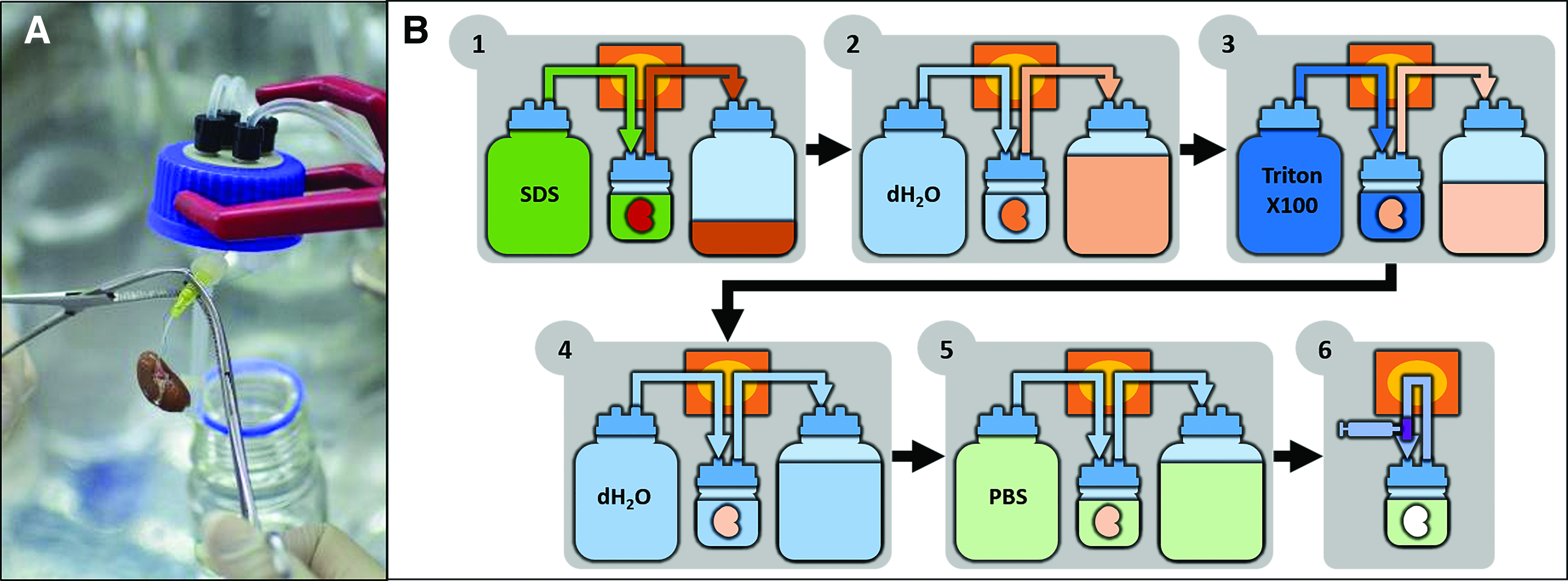
Procedure for kidney decellularization. Mounting of cannulated rat kidney in the decellularization chamber using hemostatic clamps
Confirmation of kidney decellularization
Time-lapse imaging
The decellularization process was documented by time-lapse photography using a mirrorless camera with a built-in intervalometer. The decellularization chamber containing mounted kidney samples was placed in focus, as was a clock that served as a time stamp for each frame taken. The in-camera timer was set to take one picture every minute. All pictures were then compiled into either a video file or an animated gif file using Adobe Photoshop.
Tissue staining and DNA quantification
After achieving kidney decellularization, samples were either frozen for biomolecular analysis or fixed in 10% formalin overnight for tissue sectioning. Formalin-fixed samples were dehydrated with an alcohol series and then transitioned for paraffin embedding using a xylene series. Tissue sections (3.0–5.0 μm) of native and decellularized samples were stained with hematoxylin and eosin (H&E). Whole tissue sections and high magnification micrographs were taken to compare all the samples.
Tissue sections were deparaffinized followed by antigen retrieval by immersion in sodium citrate buffer at 70–80°C. After the slides were cooled, tissue sections were washed with PBS and blocked using 5% bovine serum albumin (BSA) from Sigma-Aldrich. Na/K ATPase antibody was coincubated with either Podocin or NCCT at 4°C overnight. Samples were then fluorescently stained by incubating them in Alexa 488 (green: Podocin/NCCT) and Alexa 549 (red: Na/K ATPase) for 2 h at room temperature. Sections were then washed with PBS and stained with Hoechst 33342 (1 μg/mL in PBS) for 10 min. All samples were treated with mounting solution (Sigma-Aldrich) and observed using an FV10i-W confocal microscope (Olympus) with FV10i-ASW 2.0 Viewer software for imaging and analysis.
Renal tissue samples from native and decellularized kidneys were freeze dried for 3 h and their dry weights were measured. Tissue samples were then homogenized and incubated overnight at 55°C in a combination of lysis buffer (0.5 M EDTA, 5 M NaCl, 1 M Tris-HCl pH 8.0, and 20% SDS) and protease K (10 mg/mL). After centrifugation, the supernatant was transferred to a new tube and an equal volume of isopropanol was added. The DNA pellet was isolated by centrifugation, washed with 70% ethanol, and suspended using autoclaved water. DNA content was analyzed using a nanophotometer.
Protein identification
The proteins remaining in decellularized kidneys were isolated through sodium dodecyl sulfate polyacrylamide gel electrophoresis (SDS-PAGE) and identified by mass spectrometry. Tissue samples of native and decellularized kidneys were lysed and homogenized using RIPA buffer (150 mM NaCl, 50 mM Tris-HCl pH 8.0, 1% NP-40, 0.5% sodium deoxycholate, 0.1% SDS, 1 mM DTT, and 1 mM Na3VO4) and protease inhibitor from Sigma-Aldrich (St. Louis, MO). Homogenates were centrifuged and the supernatants were isolated. Lysates containing the protein extracts were then analyzed using 8% SDS-PAGE gel stained with GelCode Blue safe protein stain (Thermo Fisher scientific, Rockford, IL). The gel was then washed with distilled water, after which sections were cut and sent to the Korea Basic Science Institute (KBSI) for mass spectrometry and protein identification.
Design of the kidney bioreactor system
In contrast to the decellularization setup, the kidney bioreactor is primarily composed of a small bottle designated as the main bioreactor chamber, which can hold a single decellularized kidney for cell immobilization. This bottle also serves as a medium reservoir. The basic configuration of the kidney bioreactor is a modified configuration of the decellularization chamber (Fig. 3A). Two ports (opposite to one another) of the four-port GL45 cap are inserted with silicone tubing. The first port is designated as an inlet, with a male connector placed along its inner length. The second port is designated as an outlet for recirculating the media. The third is designated for gas exchange and can be equipped with a membrane filter or simply left open. The remaining port can be configured as an auxiliary port for the cannulated ureter.
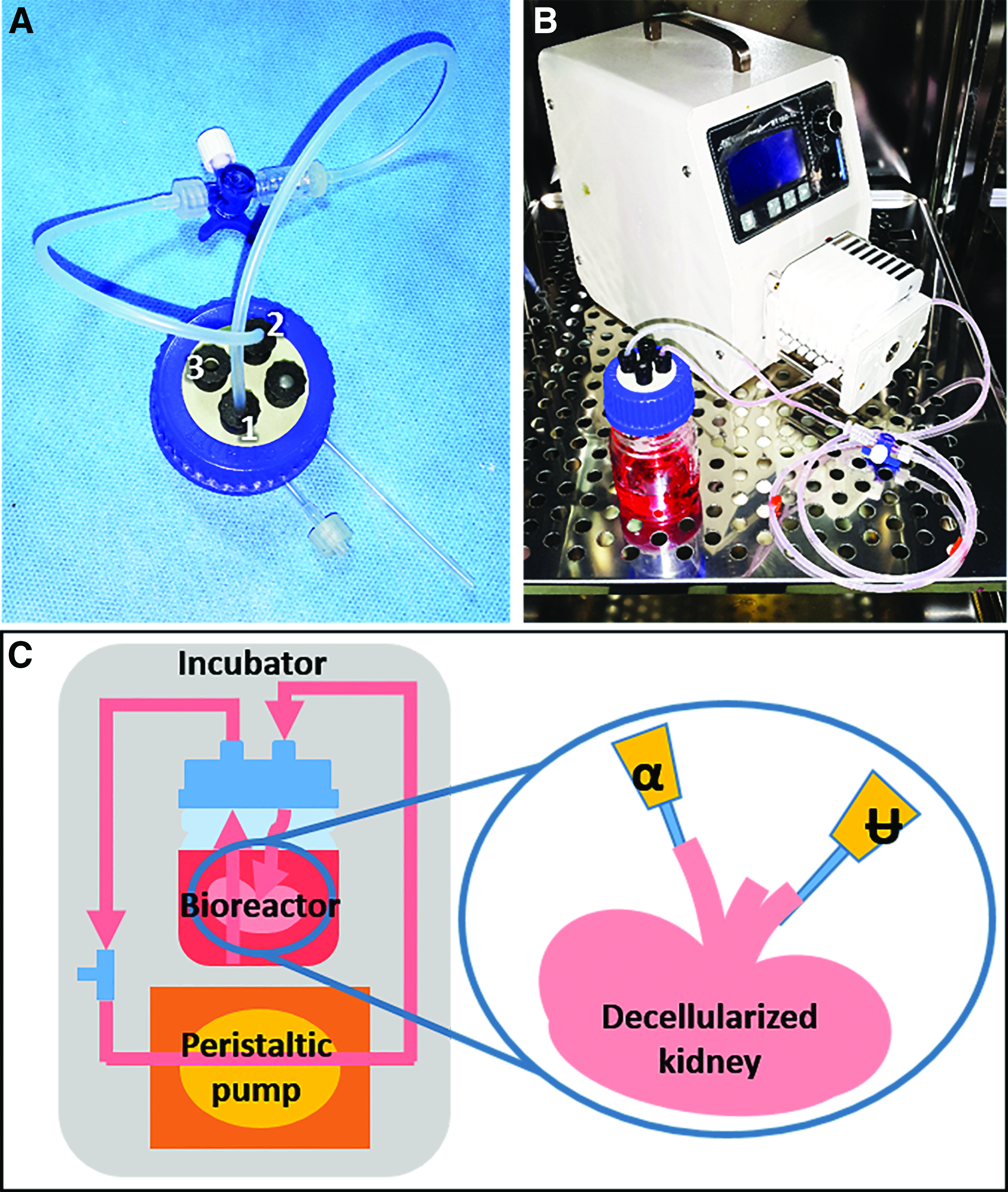
Modified configuration of the GL45 cap used for the decellularization chamber [
Like the decellularization setup, the kidney bioreactor is coupled to a peristaltic pump (Longer Precision Pump Co., Ltd., BT100-1L) capable of operating up to 40°C under the humidified environment of the incubator with an adjustable flow rate that is capable of accommodating at least eight chambers for active perfusion. Upon assembly and during operation, the setup is housed in an incubator with fixed parameters suitable for in vitro cell maintenance (Fig. 3B, C).
Culture of endothelial cells and podocytes
Before recellularization experiments, both CPAE and mouse podocytes were cultured and expanded based on established protocols. As per manufacturer's instructions, CPAE was cultured using EMEM containing 20% FBS supplement and 1% PS in a humidified CO2 incubator at 37°C. Immortalized mouse podocytes were cultured in DMEM with 10% FBS supplement and 1% PS in a humidified incubator at 33°C. Endothelial cells were expanded in regular T175 cell culture flask, while podocytes required 0.1 mg/mL collagen-coated culture plates. Cell suspension was prepared from confluent populations of both cells by trypsin detachment, followed by centrifugation and resuspension in suitable media.
Procedure for cell seeding in decellularized kidneys inside the bioreactor
Two methods are implemented for cell immobilization in the decellularized kidney. The first method primarily concerns delivery of endothelial cells into the vascular network of the acellular construct through the renal artery (Fig. 4). The second method is for delivery of cells to the parenchymal tissue through the ureter. Before implementation of either of these cell immobilization methods, the tubing of the bioreactor is prefilled with 50–60 mL of cell media and coupled with the peristaltic pump.
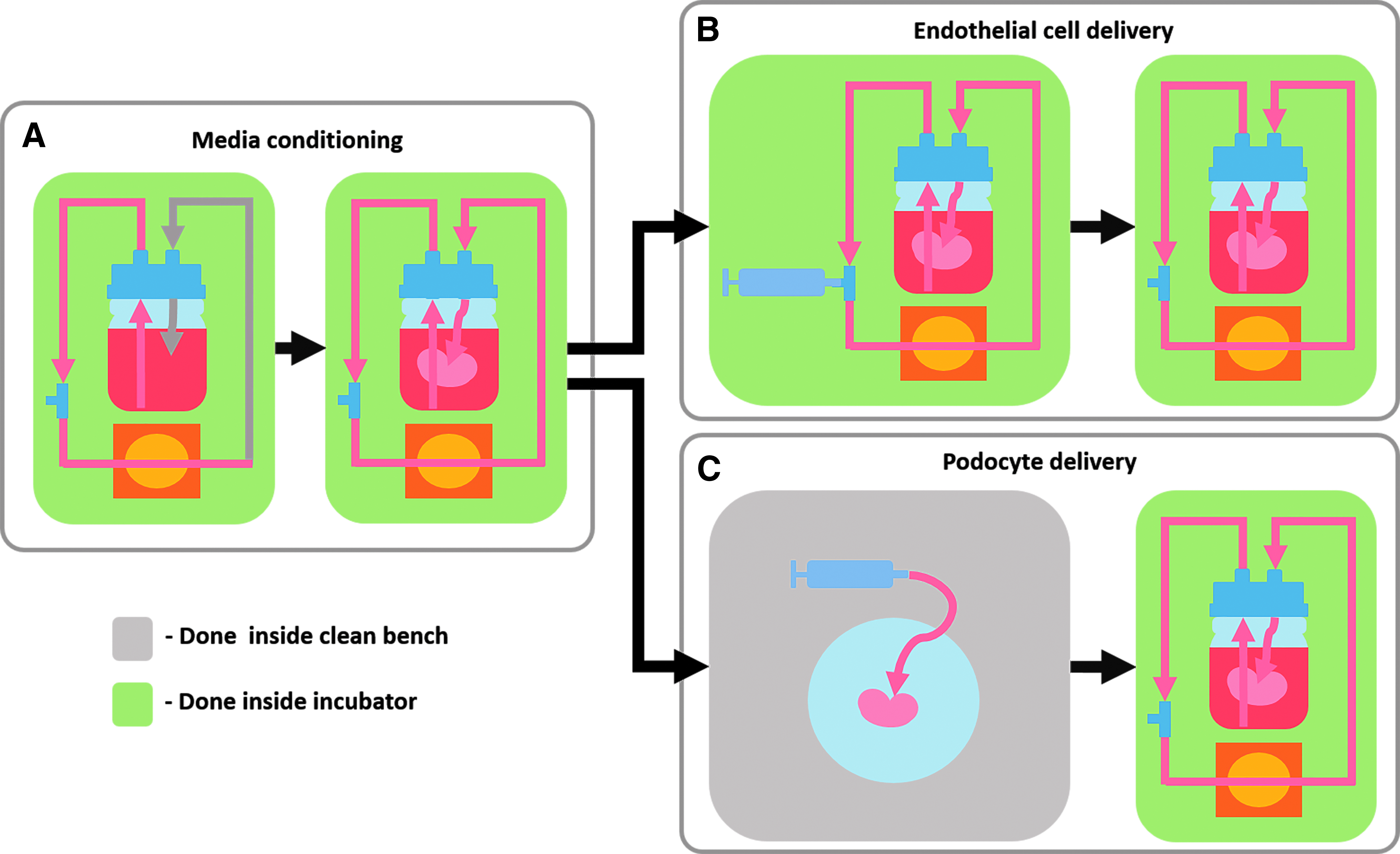
Procedure for cell seeding in decellularized kidneys inside the bioreactor. The bioreactor is prefilled with media and acclimatized inside the incubator. Decellularized kidney is attached and conditioned with the media
The whole setup is placed inside the incubator and media are recirculated for 10 min to equilibrate the temperature (Fig. 4A). After equilibrium is reached, the decellularized kidney is mounted inside the bioreactor by attaching the catheter of the renal artery to the included male luer-lock connector of the inner length of the inlet tubing. The completed setup is run for another 10 min to ensure proper perfusion and recirculation of cell media and facilitate acclimatization and conditioning of the acellular matrix (Fig. 4A). Cell seeding through the renal artery is conducted inside the incubator using aseptic handling methods. Perfusion seeding of endothelial cells is detailed below (Fig. 4B).
1. CPAE cell suspension (1 × 108 cells/mL) with suitable media is prepared in a medical-grade syringe for the perfusion of endothelial cells along the vascular network of the decellularized organ.
2. Perfusion is ceased and the three-way stopcock is set to allow flow from the auxiliary port toward the inlet port.
3. The syringe containing the cell suspension is attached to the auxiliary port and the cell suspension is injected into the inlet tubing.
4. Upon complete injection of the cell suspension into the tubing, the three-way stopcock is set to disable incoming access from the auxiliary port and only allow parallel flow through.
5. The pump is run at a rate of 1.0 mL/min for 2–3 min, enough to permit perfusion of the cell suspension through the renal artery and vascular network of the decellularized kidney.
6. After the brief perfusion run, the three-way stopcock is closed and the pump is turned off for at least 24 h to allow cell attachment. Upon completion of the stipulated attachment period, the flow is resumed at a rate of 2.0–2.5 mL/min for the remainder of the experiment.
Before cell seeding on the parenchymal tissue, decellularized kidneys should have been cannulated through the ureter. Otherwise, the cell suspension can only be delivered through direct injection. Cell seeding for the parenchymal tissue is described below (Fig. 4C). Injection of podocyte cells is conducted inside a clean bench rather than inside an incubator unless provisions for external access are provided through auxiliary tubing as detailed previously.
1. A podocyte cell suspension (1 × 108 cells/mL) in suitable media is prepared in a medical-grade syringe for the perfusion of cells into the parenchymal tissue of the decellularized organ. The volume of the cell suspension is adjusted based on ∼50–70% volume of the decellularized organ.
2. Media perfusion is ceased and the three-way stopcock is closed. The bioreactor is disengaged from the pump and transferred from the incubator to the clean bench.
3. The multiport cap is screwed open and suspended using the clamp setup to reveal the decellularized organ tethered to the inlet port through the cannula.
4. Using the sterile serrated medium-sized curved hemostatic clamps, the decellularized organ is dismounted from the inlet port connector and placed in a sterile petri dish for manipulation and injection of cells.
5. The cell suspension is either directly injected into the acellular organ or injected through the catheter cannulated into the ureter. The duct is then closed using a knotted suture.
6. After cell delivery, the seeded construct is remounted in the bioreactor by connecting the vascular catheter to the inlet port connector of the multiport cap. The seeded organ is carefully lowered into the glass chamber and the cap is securely screwed in place.
7. The bioreactor is transferred back inside the incubator. The stopcock is opened and the tubing is reengaged with the peristaltic pump as per the original configuration. The pump is run at a flow rate of 2.0–2.5 mL/min immediately after cell seeding.
The aforementioned bioreactor system was run at the target flow rate for 3–7 days. The cell media were replaced every day to maintain optimum quality.
Validation of cell immobilization in decellularized kidneys
To verify that the cells delivered into the decellularized kidneys were still viable, 3-(4,5-dimethyl-2-thiazolyl)-2,5-diphenyl-2H-tetrazolium bromide (MTT) solution was perfused into the recellularized construct after continuous media flow for 7 days. Samples were incubated at 37°C for 2 h until purple formazan salts appeared within the seeded constructs inside each bioreactor. Incubated constructs were photographed with backlighting to clearly visualize the chromogen.
Micrographs of cell-seeded decellularized kidneys were also visualized with live-dead cell staining (L-3224; Invitrogen). Briefly, cell-seeded samples maintained in bioreactors for 1 week were removed from the chambers and cut in half with sterile surgical blade. Unfixed sectioned samples were then gently washed with PBS after which the working solution containing ∼2 μM calcein AM (Cal-AM) and 2 μM ethidium homodimer (EthD-1) was added to stain the cells. PBS containing appropriate amounts of supplements was added to stained cells before microscopy.
Confocal microscopy revealed living cells stained with Cal-AM (green), while dead cells were stained with EthD-1 (red). Micrographs were taken using a FV10i-W (Olympus). DNA quantification was also conducted to confirm increase in genetic content after recellularization. To observe the actual locations of the cells delivered into the decellularized kidneys, paraffin sections of the recellularized kidneys were also prepared from cell-seeded samples and stained with H&E. Micrographs were taken with a BX53 research microscope (Olympus) with an attached DP72 digital camera (Olympus).
Results and Discussion
The decellularization system was designed to accommodate kidneys extracted from small animals. This system is composed of the assembled components, and the step-by-step procedure through which the decellularization process is carried out and the method of mounting the resulting decellularized kidney in a bioreactor for observing the in vitro cell response were described herein.
The fully assembled decellularization chamber is an open system designed to deliver treatment solutions and remove waste or excess fluids. Both inlet and drain rely on the same perfusion pump through anterograde (input) and retrograde (output) attachments, respectively. The foremost indication of decellularization during active perfusion is the reduction in the original color and opacity of the kidney (Fig. 5A), which takes place during decellularization. The kidney transitions from opaque to translucent, revealing the vascular network of the organ. During the continuous perfusion of the different solutions, the remaining blood and cellular components flow out from either the renal vein or the ureter.

Compiled time-lapse photographs of kidney decellularization
The compiled time-lapse photographs (Supplementary Data; Supplementary Data are available online at
To determine if the active perfusion decellularization process yielded an intact vascular network, red marker dye was injected into the renal artery (Fig. 5B). The decellularization process resulted in a significant 40% reduction in size of the whole kidney compared to the native organ, as shown in low-magnification micrographs of the stained tissue sections (Fig. 5C). Higher magnification revealed extensive removal of the cells from both the vascular network and the parenchymal tissue. Although the removal of cells resulted in a decrease in the size of the organ and associated structures, the general microarchitecture of the glomerulus and tubules remained intact (Fig. 5C). Because removal of the cells, reintroduction of new cells, and circulation of media primarily take advantage of these microstructures, the maintenance of an intact vascular network and renal microarchitecture is a decisive factor for successful decellularization and cell immobilization.23,24,32
To visualize and compare the presence of remaining kidney proteins, paraffin-embedded tissue sections of native and decellularized kidneys were subjected to immunofluorescence staining (Fig. 6). Podocin was used as a protein marker for the glomerulus, while Na/K ATPase and NCCT were used to identify the proximal tubules and distal tubules, respectively. In native kidney tissue, Podocin (Fig. 6A, green) can be seen in a grape-like cluster of cells of the glomeruli, which are located along the cortical region. Around the glomeruli, Na/K ATPase protein can be seen lining the proximal tubule, similar to a monolayer endothelial lining (Fig. 6A, red). The presence of NCCT was observed along the medullary regions of the native tissue where most of the distal tubules reside. NCCT protein can be clearly seen (Fig. 6B, green), while Na/K ATPase was also detected to some extent along the distal tubules (Fig. 6B, red). A strong presence of genetic material within the intact cell nuclei was observed in all regions of the native kidney (Fig. 6A/B, native merged).
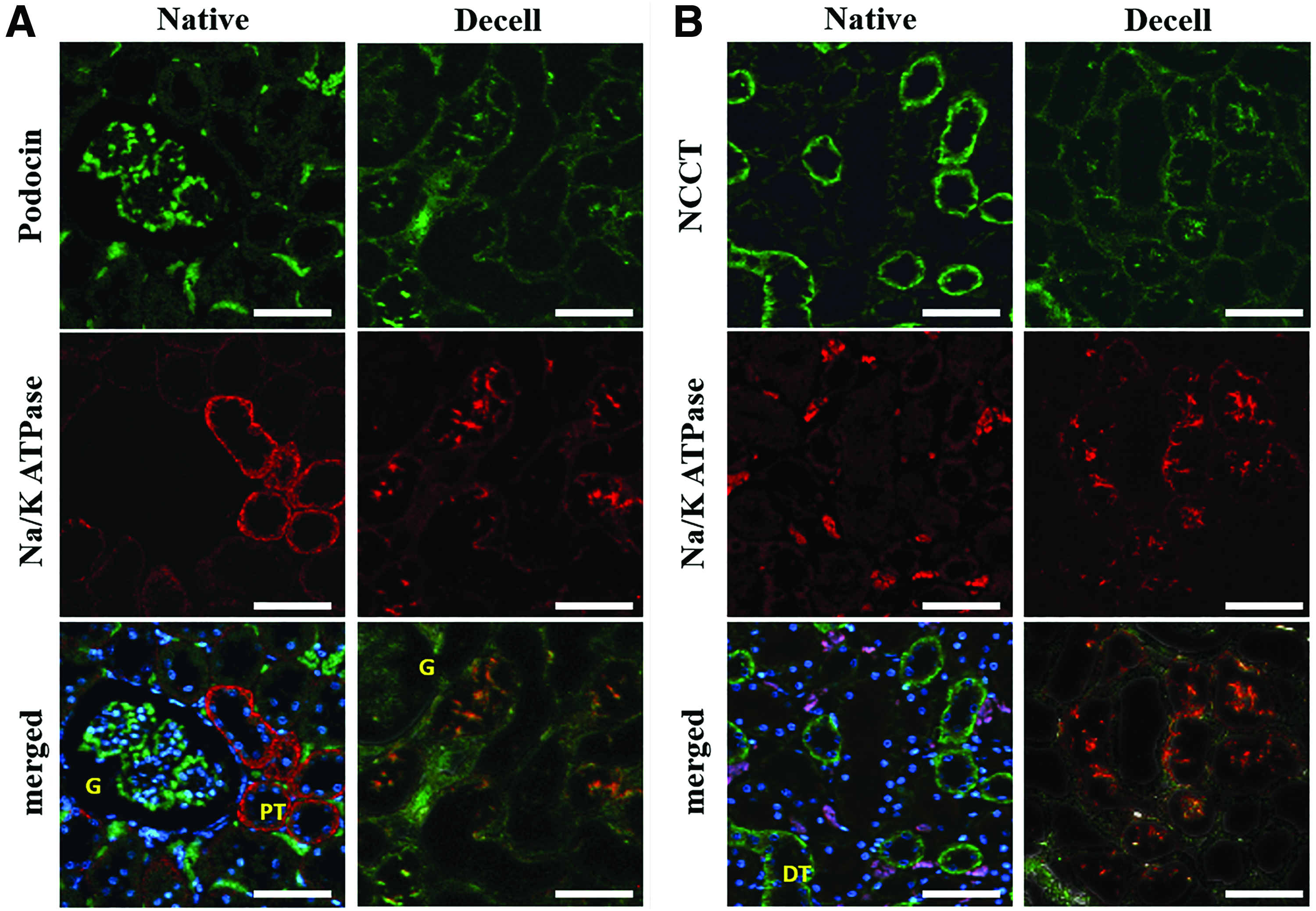
Immunofluorescent stained tissue sections of native and decellularized kidneys. Images taken both along the cortical
After decellularization, cell nuclei can no longer be observed (Fig. 6A/B, Decell merged). Although some expression of Podocin and Na/K ATPase can still be observed in their respective regions, both proteins are generally dispersed along the whole ECM structure (Fig. 6. A, Decell). Remnants of NCCT protein along the renal medulla can still be observed, which aids in the identification of the distal tubules, even though the distribution is no longer similar to that in native tissue. Some expression of Na/K ATPase can also be observed within the same structures (Fig. 6B, Decell). This demonstrated that, although the ECM architecture was retained after decellularization of the kidney, the original distribution of the proteins associated with the glomeruli, proximal tubule, and distal tubule has been significantly reduced and the distribution has been modified.
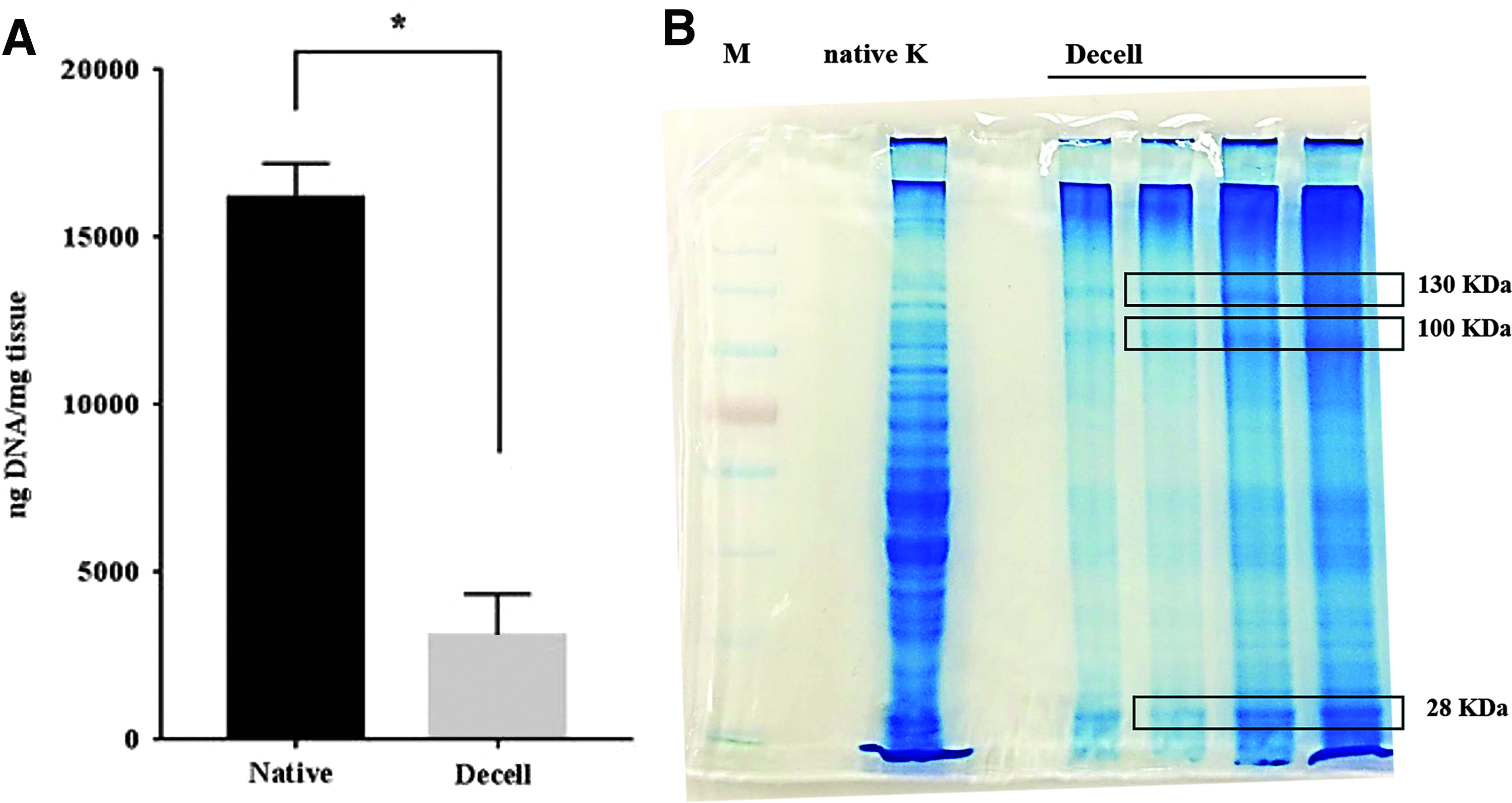
Remaining genetic molecules and proteins in the decellularized kidney were isolated, quantified, and compared with that in the native tissue (Fig. 7A). As expected, the DNA concentration in the decellularized kidney was significantly reduced relative to that in the native tissue, owing to the complete removal of cells. To identify the proteins remaining in the decellularized kidney, extracts from the native and decellularized tissue samples were run on SDS-PAGE gels to segregate them based on molecular weight.
DNA quantification
Results showed significant reduction of protein content after decellularization as evidenced by the faint bands when using lower concentrations of isolates (Fig. 7B, box). Sections of the gel containing proteins/peptides from the decellularized samples weighing 130, 100, and 28 kDa were sent for identification by mass spectrometry (Fig. 7B). These ranges of molecular weights were selected due to improved resolution after electrophoresis at higher concentrations.
The identified proteins listed in Table 1 were also cross referenced using online human protein atlas (
Proteins highly related to kidney tissue.
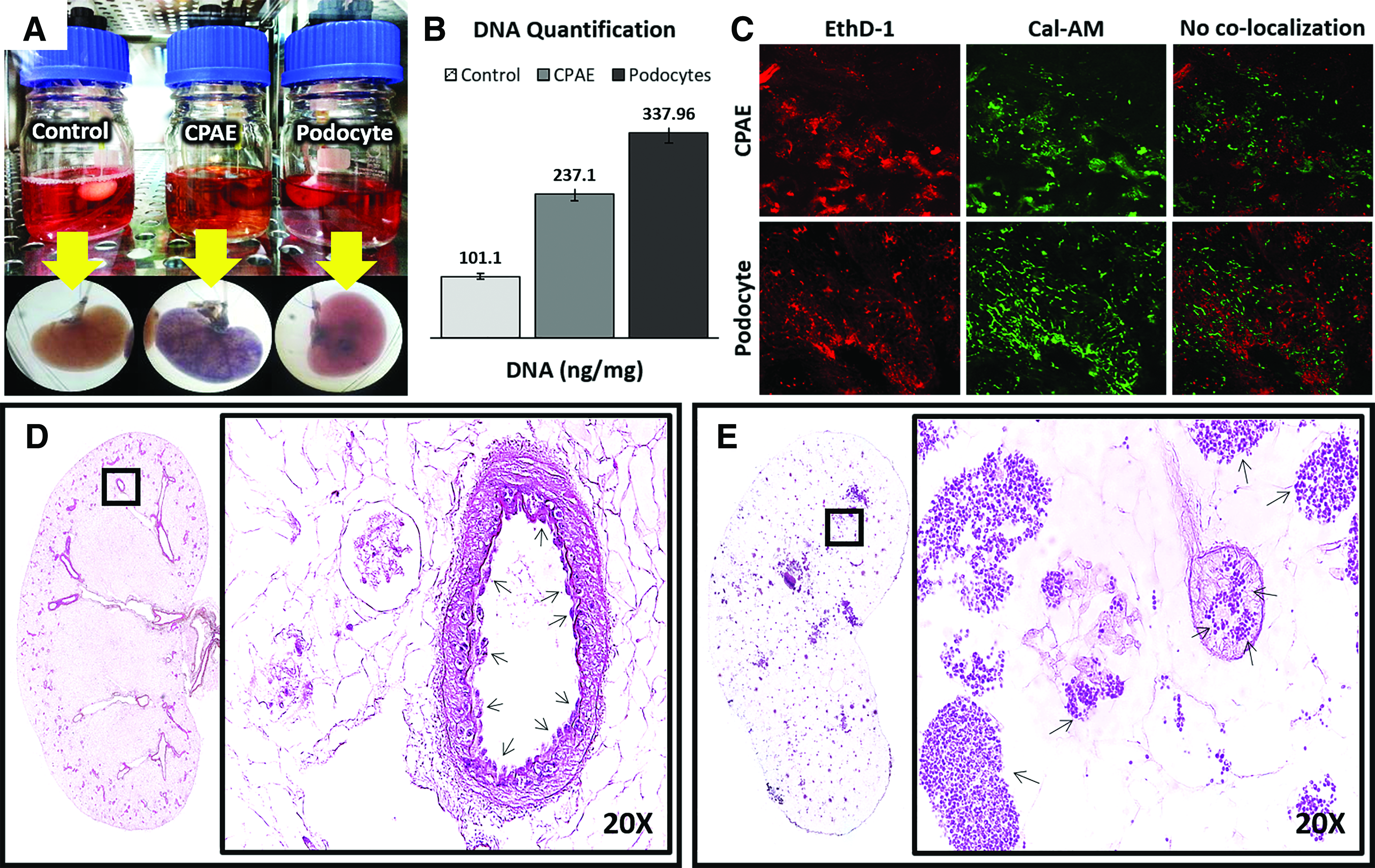
The viability of the injected/perfused cells was confirmed by injection of MTT solution in the seeded constructs. In principle, if the cells inside the construct survived the procedure and the conditions inside the bioreactor, purple formazan salts would form through the natural metabolic processes of these cells. This would also reveal the general distribution of cells along the whole cell-seeded construct. Figure 8A shows three fully assembled and functional bioreactors used to confirm both cell viability and sterility of the system. The first bioreactor from the left contains a decellularized kidney perfused with media without any cells, which is included as a negative control. The second and third bioreactors housed decellularized kidneys seeded with CPAE and podocytes, respectively (Fig. 8A). Among the setups, only the control setup did not generate purple stain after incubation with MTT solution. This not only serves as a negative control but also validates the sterile conditions required for conducting proper in vitro studies.
Assembled functional bioreactors
Both the CPAE- and podocyte-seeded kidneys formed localized purple stains, although with different patterns of distribution. Cells seeded through the renal artery (Fig. 8, CPAE) were more evenly distributed than were cells injected through the ureter (Fig. 8, podocyte). It should be noted that although conditions for culture and expansion of mouse podocytes varied from that of the bioreactor system, the cells would simply undergo differentiation at 37°C and limit the capacity for proliferation, but not reactivity to metabolic chromogen such as MTT. Likewise, presence of the purple stain after incubation with MTT proves that these cells are still alive and the culture condition can be modified in the future to accommodate in situ expansion of podocytes within the decellularized scaffold. DNA quantification after recellularization indicated 2.4-fold increase in DNA in samples perfused with CPAE cells and 3.7-fold increase in samples injected with podocytes (Fig. 8B).
Sectioned samples of decellularized kidneys seeded with endothelial cells and podocytes are shown on Figure 8C–E. Presence of viable cells was further confirmed through live-dead cell staining of sectioned recellularized kidneys (Fig. 8C). To better visualize the viable cells, confocal images were separated into respective color channel images. Using ImageJ, the red channel image (EthD-1) was subtracted from the green channel image (Cal-AM) to eliminate colocalized elements (yellow) and reveal the independent green- and red-stained cells. Decellularized kidneys without cells would only stain red (not shown). Micrographs of H&E-stained tissue sections of kidneys with either CPAE (Fig. 8D) or podocytes (Fig. 8E) were observed to confirm the location of the delivered cells.
Whole sections of cell-seeded samples reveal highly stained portions of the decellularized kidney. High magnification of the selected regions reveals the attachment of CPAE cells unto the inner lining of vessels (Fig. 8D, 20 × ). Podocytes introduced through the ureter can be seen within the tubules and some cells have also reached the glomerular capsule (Fig. 8E, 20 × ). These results indicate that although the system is capable of maintaining the viability of cells delivered in decellularized constructs for at least 1 week, cell-seeding procedures can still be improved. Future studies can make use of the auxiliary port as an alternative drain/input or, as previously mentioned, as a third connection for the ureter, and pressure modification could also be possibly applied by attaching a pump on the gas exchange port.
A streamlined system for implementing the decellularization and recellularization setup should be developed to allow for studies on the potential of using decellularized kidneys for organ regeneration. The proposed decellularization system and bioreactor offer a fully modular approach that provides the sterile environment necessary for conducting in vitro studies using decellularized kidneys. The main chambers housing the organ/construct use the same interchangeable components and do not require highly customized fabrication. The simplicity of the bioreactor design not only presents the potential for modification but also minimizes the venues for contamination through a reduction in the number of parts and exclusion of a medium reservoir.
Previous studies on decellularization have specified at least 96–120 h of processing.46,47 Rather than relying on pressure-induced flow reminiscent of other existing protocols,24,43 the proposed system takes full advantage of active perfusion of decellularization and washing solutions, which in turn allows for faster decellularization (within 12 h). This significantly increases the number of kidneys that can be processed at one time and minimizes the potential for contamination during routine handling. Since both the decellularization system and the recellularization bioreactors are composed of similar components, failure of one or more parts can be easily resolved through interchanging parts. Although the streamlined system proposed in this study is somewhat limited in terms of developing an actual functional kidney, it can be widely adapted and further modified to facilitate different recellularization experiments.
Conclusion
Interest in developing ECM-based biomaterials for tissue regeneration has significantly increased over the past decade. Although several milestones have been achieved, the full potential of using ECM as a biomaterial still needs to be extensively investigated under controlled conditions before actual translation as a viable technology. This need can only be realized using an efficient in vitro model. Based on these results, the proposed system and the outlined protocols for decellularization of kidneys and cell delivery into decellularized kidney are suitable for conducting in vitro studies. Using the complete streamlined modular system, an in vitro study using decellularized kidneys can be properly established within 2 days. The system can also be modified to accommodate the requirements of future experimental designs, which will be essential for the development of an actual functional regenerated kidney.
Footnotes
Acknowledgment
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Education (2015R1A6A1A03032522), and partially supported by Soonchunhyang University.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.