
Abstract
Bone graft materials are commonly used to regenerate various bone defects, but their application is often limited because of the complex defect shape in various clinical conditions. Hence, customized bone grafts using three-dimensional (3D) printing techniques have been developed. However, conventional simple bone defect models are limited for evaluating the benefits and manufacturing accuracy of 3D-printed customized bone grafts. Thus, the aim of the present study was to develop a complex-shaped bone defect model. We designed an 8-shaped bony defect that consists of two simple circles attached to the rabbit calvarium. To determine the critical-sized defect (CSD) of the 8-shaped defects, 5.6- and 7-mm-diameter trephine burs were tested, and the 7-mm-diameter bur could successfully create a CSD, which was easily reproducible on the rabbit calvarium. The rate of new bone formation was 28.65% ± 8.63% at 16 weeks following creation of the defect. To confirm its efficacy for clinical use, the 8-shaped defect was created on a rabbit calvarium and 3D computed tomography (CT) was performed. A stereolithography file was produced using the CT data, and a 3D-printed polycaprolactone graft was fabricated. Using our 8-shaped defect model, we were able to modify the tolerances of the bone graft and calvarial defect to fabricate a more precise bone graft. Customized characteristics of the bone graft were then used to improve the accuracy of the bone graft. In addition, we confirmed the fitting ability of the 3D-printed graft during implantation of the graft. Our 8-shaped defect model on the rabbit calvarium using a 7.0-mm trephine bur may be a useful CSD model for evaluating 3D-printed graft materials.
Introduction
T
Three-dimensional (3D) printing technology or additive manufacturing is a process of fabricating 3D solid objects from a digital file. The creation of a 3D-printed object is achieved using additive processes, 4 in which an object is created by laying down successive layers of material.
Recently, 3D printing technology has rapidly expanded toward diverse medical applications.5–7 Since the 3D printing technique can produce defect-customized bone grafts,6,8,9 this technology can also solve the aforementioned hurdles of conventional-type bone grafts and become popular for the field of bone regeneration, especially in the craniomaxillofacial region owing to its particularly complex structure and greater esthetic requirements.
One of the most important aspects for evaluating the safety and efficacy of newly developed graft materials for bone regeneration before commercialization and clinical use is establishment of an appropriate standardized bony defect model. 10 The key requirements of an animal bony defect model are consistent reproducibility of the bony defect in size and shape on each attempt, feasibility of its evaluation, and safety for the experimental animal. In addition, determining the critical-sized defects (CSDs) is essential when evaluating the bone regeneration potential of a bone graft material by comparing the results to the natural healing capacity. In 1986, Schmitz and Hollinger originally defined a CSD as “the smallest size intraosseous wound in a particular bone and species of animal which will not heal of its own volition during the lifetime of the animal” 11 or during the experimental period in untreated bone defects. 12
To date, various CSDs with uniform shape have been used to evaluate the efficiency of different types of graft materials fabricated by traditional manufacturing methods for bone grafting. However, the defect shape of conventional CSD models is too simple to properly evaluate the unique characteristics of defect-customized bone graft materials using 3D printing technology.
In addition, based on a literature review, it was recommended that dogs, sheep, goats, pigs, or rabbits could serve as appropriate animal species for determining the effects of bone graft materials according to international standards; among these animals, the rabbit is one of the most commonly used models because of its ease of handling and size.13,14
To overcome the limitations of conventional bone defect models, in the present study, we designed a new animal model and experimental protocol with an 8-shaped bone defect in the rabbit calvarium, and suggest new criteria for evaluating the characteristics of 3D-printed customized bone grafts.
Materials and Methods
Animal preparation and surgical process
Approval for this experiment was obtained from the Institutional Animal Care and Use Committee (IACUC) of the Asan Medical Center, University of Ulsan College of Medicine, Korea. New Zealand White rabbits (Orient Bio, Inc., Gyeonggi-do, Korea) weighing ∼2.5 kg (12–13 weeks old) were used and allowed a 1-week acclimatization period inside the cage before surgery. The animals were preanesthetized with atropine (0.5 mg/kg) and then anesthetized by intramuscular injection of Zoletil (15 mg/kg) and xylazine hydrochloride (3.5 mg/kg). The scalps were shaved and scrubbed with a povidone/iodine solution to avoid contamination. After subcutaneous injection of local anesthetic (lidocaine hydrochloride with epinephrine 1:100,000) for hemostasis and pain reduction, the calvarium was exposed with an ∼1.5-cm sagittal midline scalp incision using a sterilized scalpel so that the bregma (an intersection point of the coronal suture and sagittal suture perpendicularly) lay on the center of the opening.
To determine which defect size would meet the CSD criteria, we tested defects of two different sizes: outer diameter of 5.6 and 7.0 mm. Two full-thickness bony defects were created on each parietal bone using a hollow trephine bur.
To create a bone defect at a specific position, the defect was generated by holding the initial defect position at 2 mm in front of the lambdoid suture line of the calvaria. To create an 8-shaped defect, the 7-mm circle was overlapped by ∼1 mm. A bone defect was created symmetrically (2 mm apart) with respect to the sagittal suture line to produce the same 8-shaped defect on the other side. The complex bone defect was designed into an 8-shaped structure using two circles of the same size with a diameter of 7.0 mm (Fig. 1a).
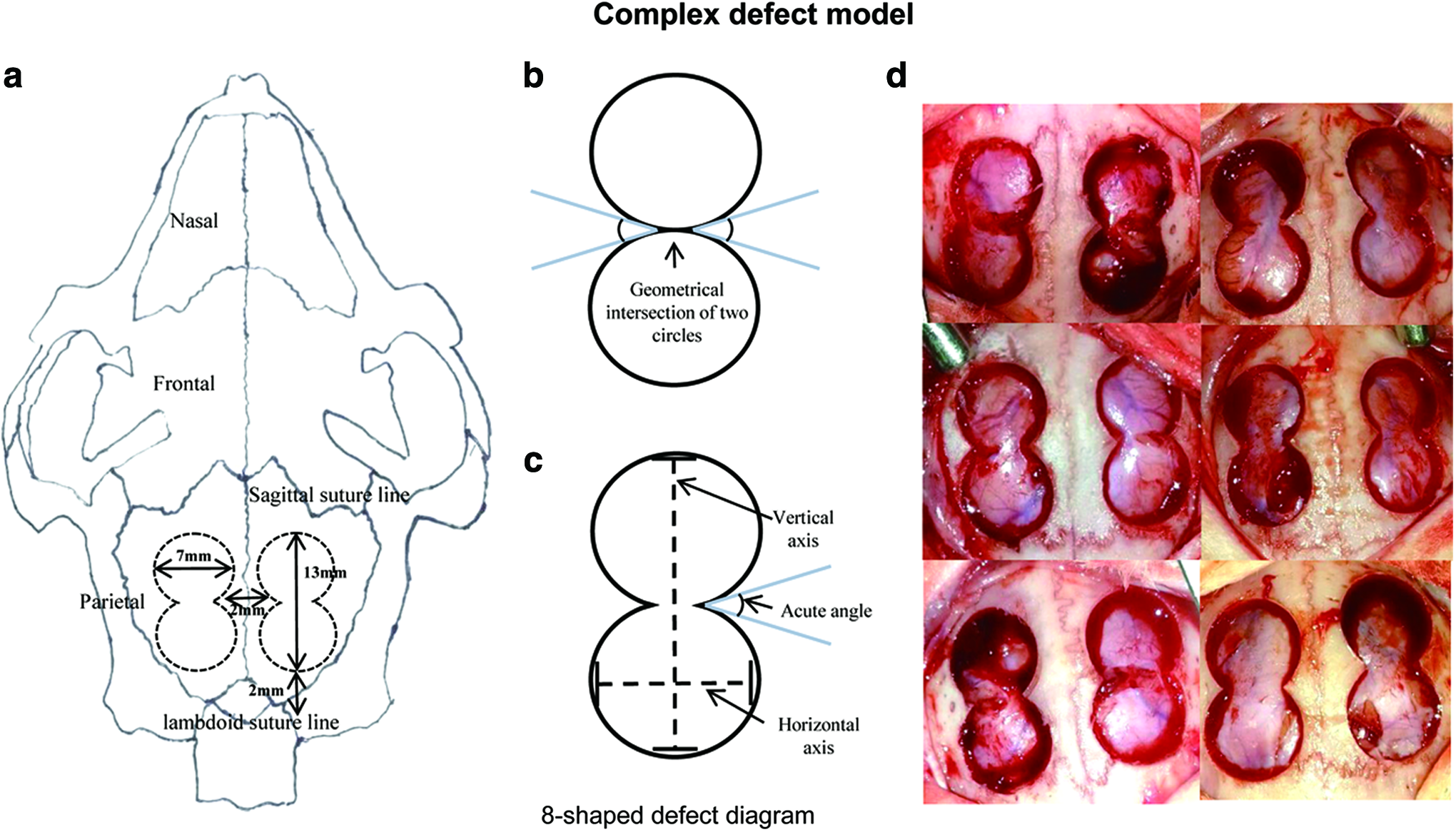
Complex defect model. Schematic diagrams of 8-shaped defects.
The 8-shaped bone defect was geometrically matched at a point where the two circles met. However, while creating the defect, the geometrical intersection of the two circles (Fig. 1b) became a full line because of the bur thickness. An acute angle was formed where the circles met. This acute-angled bone defect would be difficult to fill precisely using a conventional bone graft (i.e., powder or block-type grafts) (Fig. 1c).
Any debris or bone chips remaining were irrigated with sterile normal saline, and the periosteum and skin were closed separately with 3-0 polypropylene sutures and scrubbed with povidone/iodine solution. After the operation, computed tomography (CT; Siemens AG, Munich, Germany) images were taken of the calvarium and then postoperative management was conducted by intramuscular injection of ampicillin (50 mg/kg) and ketorolac tromethamine (1 mg/kg) twice a day for 3 days to prevent infection and pain, respectively.
Fabrication and implantation of 3D-printed bone graft materials
Figure 2 shows the overall experimental procedure. In brief, stereolithography (STL) files were obtained from the CT images of the bone defects and converted into a solid model. The solid model was then used to design the 3D-printed customized graft. The customized polycaprolactone (PCL) graft was manufactured by a 3D printer with a precision extruder deposition head (nozzle size 400 μm) system (Wonkwang University, Iksan, Korea). The pore size of the graft was 500 μm and the porosity was 51.80%. Three-dimensional-printed grafts were sterilized under ultraviolet light overnight and then rinsed three times with 75% ethanol and 1× phosphate-buffered saline. On postoperative day 3, the calvarium was reopened and the customized 3D-printed PCL graft was implanted in the left defect site, while the right defect site was left empty as a control (Fig. 2). After implantation, the overlying muscle and skin were closed with 3-0 polypropylene sutures and scrubbed with povidone/iodine solution (Fig. 2d). According to our postsurgical protocol, intramuscular injection of ampicillin (50 mg/kg) and ketorolac tromethamine (1 mg/kg) twice a day for 3 days was given to prevent infection and pain. CT scanning was performed on the calvarial bone at 1, 2, 4, 8, 12, and 16 weeks following implantation. The animals were sacrificed at 4, 8, 12, and 16 weeks after implantation, and calvarial bone samples were immediately harvested and fixed in 4% (w/v) paraformaldehyde for further micro-CT analysis and histological staining.

Process of preparing a customized 3D-printed bone graft for a complex bone defect.
CT and micro-CT analysis
Using the CT data, the threshold and region of interest were set to the 8-shaped defect with a diameter of 7 mm. After selecting the thickness for measurement (1.0 mm), the amount of new bone volume was measured using Asan J software (Asan Medical Center, Seoul, Korea) based on the ImageJ (NIH, Bethesda, MD) plug-in package.
Fixed specimens were wrapped with parafilm to prevent drying and examined by micro-CT (SkyScan 1176; Skyscan, Kontich, Belgium). The specimens were scanned at a high resolution with an aluminum filter (0.5 mm). Scan settings were as follows: energy of 50 kV, intensity of 500 μA, resolution of 35.76-μm pixels, rotation step size of 0.7°, and tomographic rotation of 531 (531 projection images were acquired by a tomographic scan over a 180° sample rotation). Projection images of cone-beam acquisition and reconstruction were saved as 16-bit TIFF files. All scanning and reconstruction parameters were identical for all specimens and calibrations.
Custom fitting ability evaluation
To determine whether the customized 3D-printed bone graft was precisely fabricated and fits tightly to the 8-shaped defects, we observed the fitting of the graft at the defect site. The yellow dotted line indicates the thickness of the calvarial range (∼1.3 mm) and was scored as follows: 0, the scaffold remained in place; 1, less than half of the scaffold moved from the calvarial range; and 2, more than half of the scaffold moved from the calvarial range (Fig. 3). In addition, at 16 weeks after implantation, micro-CT image sections were made using the CT-Vox program (Skyscan), and the micro-CT images of six rabbits were analyzed to determine whether the graft was maintained in the original position of grafting.
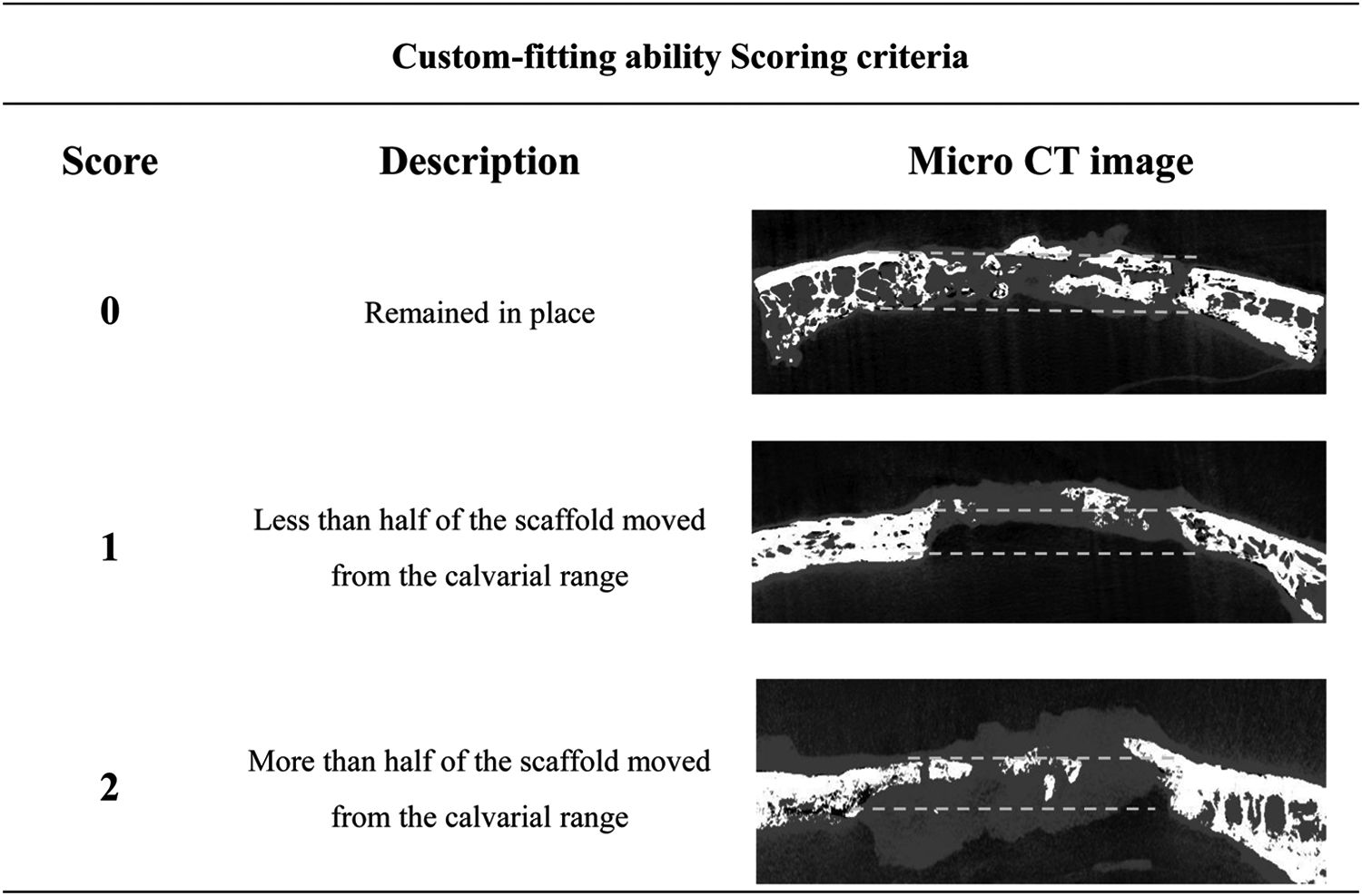
Scoring criteria for custom fitting ability of the graft. To evaluate whether the customized 3D-printed bone graft was precisely fabricated and fit tightly to the 8-shaped defects, and the dotted lines indicate the thickness of the calvarial range (∼1.3 mm) and was scored as follows: 0, the scaffold remained in place; 1, less than half of the scaffold moved from the calvarial range; and 2, more than half of the scaffold moved from the calvarial range.
Statistical analysis
Differences between groups are expressed as mean ± standard deviation. Statistical analysis was carried out using single-factor analysis of variance through SPSS version 24.0 software (IBM Corp., Chicago, IL). p-Values less than 0.05 were considered statistically significant.
Results
Determination of the CSD in the complex rabbit calvarial defect
To determine the appropriate CSD in the complex bone defect model, the animals were divided into the following two groups according to defect size: two 8-shaped bone defects with a 5.6-mm-diameter hollow trephine bur, and two 8-shaped bone defects with a 7.0-mm-diameter hollow trephine bur. After 16 weeks of defect formation without treatment, the 8-shaped bone defects from the 5.6-mm-diameter hollow trephine bur were filled with new bones up to more than 60% on both the left and right sides (Fig. 4b), while the 8-shaped bone defects from the 7.0-mm-diameter hollow trephine bur showed minimal new bone formation, except for the waist region of the 8 shape (Fig. 4d). The critical size of the newly designed 8-shaped defect created using a 7.0-mm hollow trephine bur was a diameter of 7.0 mm and length of 13–14 mm. The rate of new bone formation was higher for defects made with the 5.6-mm hollow trephine bur compared with those made with the 7.0-mm bur (Fig. 5).

Experiment on the rabbit calvarium to determine the appropriate CSD. Bone defect model of an 8-shaped form created by a 5.6-mm hollow trephine bur. CT image after 1 week (left)

Change in the regenerated bone volume of an 8-shaped bone defect. The full defect volume was 81.01 ±4.73 mm3. At the 16th week when the animals were sacrificed, the rate of new bone formation was 28.65% ± 8.63% (*p < 0.05, **p < 0.01, ***p < 0.001). Thus, healing had not reached 50% by the time of sacrifice, and the CSD was effective. In addition, the difference in standard deviation was constant and reproducibility was confirmed.
Correction of allowance of the 3D-printed graft
To prepare the 3D-printed graft for individual 8-shaped defects in the rabbit, related CT images were used for each graft. However, because of the resolution of the CT machine, there were differences between the reconstructed in silico model and actual defect. To reduce this dimensional error, two scale-up models and two scale-down models were fabricated with the reconstructed defect model. First, a 3D graft model was designed using CATIA V5 R13 software with an 8-shaped defect based on the CT data. Because manufacturing error between the design and fabricated object is possible, we tested the magnitude of any manufacturing error and tried to reduce the error before conducting in vivo experiments. To reduce this manufacturing error, the design of the reconstructed 3D graft model was scaled up and down by 3% and 6% with the in-plane direction of the 8-shaped defect. The 8-shaped graft was fabricated using these five different designs, and the five fabricated grafts were tested for their fitness to the defect. We observed that the 6% scale-up model had the best result, and therefore adopted the 6% scale-up design to all models for in vivo experiments.
Custom fitting ability evaluation
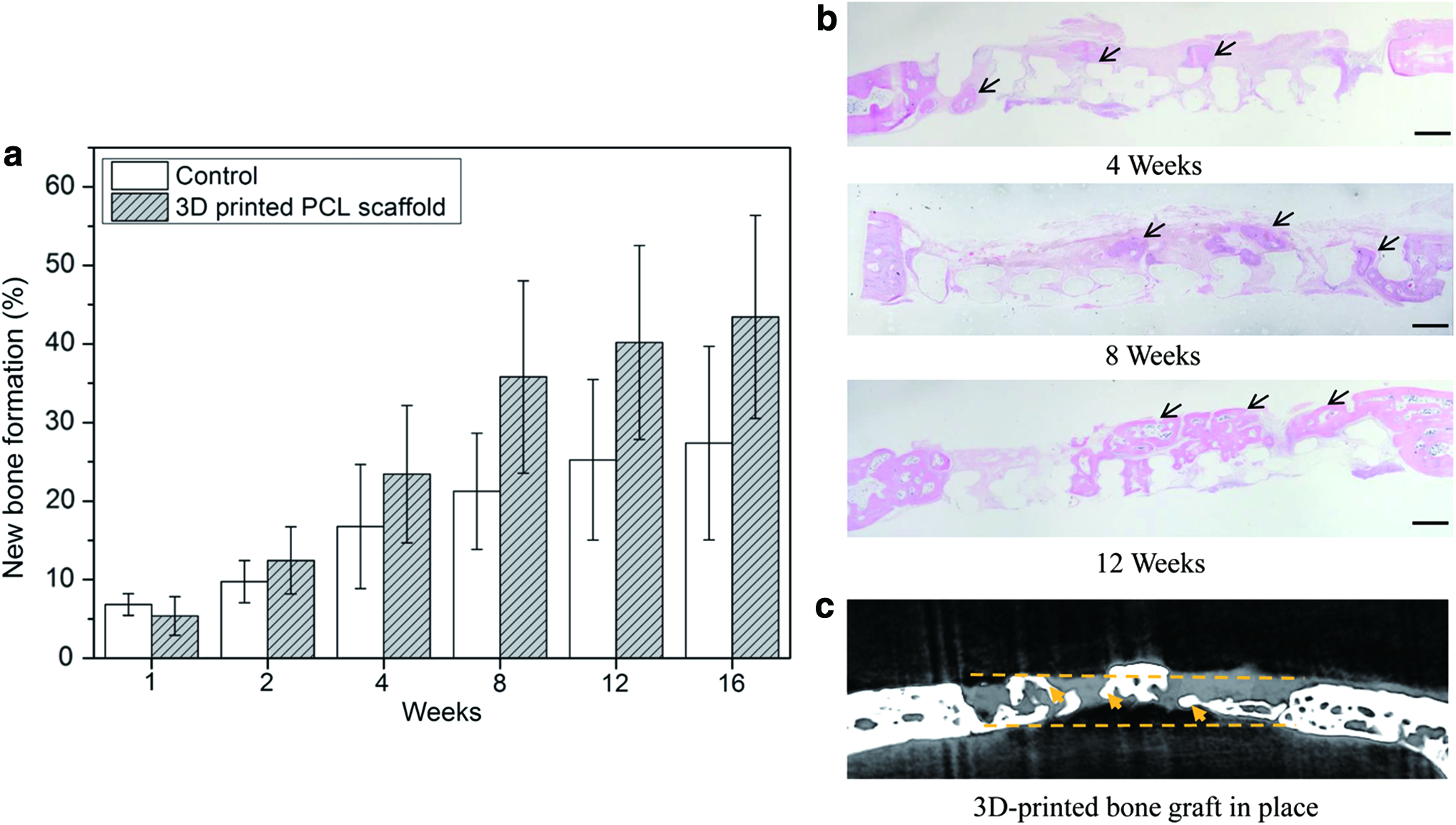
Evaluation of the fitting ability of the graft showed that the average score of fitting ability was 0.33 (±0.51) out of a total possible score of 2, indicating that most grafts fit the defect in a pressed-fit manner (Table 1). The micro-CT images of bone graft at 16 weeks after implantation in rabbits showed that the grafts remained properly almost in the same place in which they were grafted (Fig. 6c).
n = number of animals.
Bone regeneration after implantation in the 8-shaped bone defect
Evaluation of follow-up CT images showed that the volume of newly generated bone by implanting 3D-printed PCL grafts in 8-shaped bone defects was better than that in the group without the graft (Fig. 6a). According to the histological evaluation, new bone gradually migrated from the margins of the defect in both groups; however, interestingly, numerous bony islands were also observed in the spaces in the 3D-printed grafts (Fig. 6b). The implanted graft was nearly intact and remained present at the end of experiment.
Morbidity of the experimental animals
No animals died and no infections were observed during the study period. Only one animal showed partial wound dehiscence and thus was excluded from this study.
Discussion
Numerous animal models have been developed to test the safety, biocompatibility, and efficacy of bone graft biomaterials.15,16 Many defect sites have been created to mimic clinical situations, and most previous studies have used mono, rectangle, or cylinder shapes for bone defect models in rabbits,17,18 dogs, 19 and sheep. 20 Rabbit is one of the most commonly used animal models for musculoskeletal research because of the ease of housing and handling. In particular, the use of appropriate implantation site areas and skeletal structures can avoid pathological fracture, 10 despite the dissimilarities in macrostructure and microstructure of the human and rabbit bone.21,22
Calvarial defect models have the following advantages: it is not necessary to fix the bone to stabilize the graft, bone regeneration is neither affected by mobility nor muscular activity, and two equal contralateral bone defects can be created with only one incision and suture to facilitate a paired design model.
To validate our 8-shaped bone defect as a CSD, the appropriate characteristics of a CSD must first be determined. The appropriate CSD differs according to the animal species used23,24: 4 mm in mouse calvaria,23,25 8 mm in rat calvaria,23,26 6–10 mm in rabbit calvaria,23,27–30 and 20 mm in sheep calvaria.23,31 In a recent study, the CSD was defined as a bone defect that does not recover during the experiment period. 12 The 8-shaped defect models created with the 7-mm outer diameter trephine bur did not recover for 16 weeks (the end of the experimental period), and were thus chosen as the appropriate CSD of practical significance for evaluating and comparing the results of experiments.
Craniomaxillofacial bony defects often occur in complex shapes due to congenital defects, trauma, and tumor surgery.32–34 In addition, compared with the bones of other sites, craniomaxillofacial bones have more complex shapes due to their complex function; bony defects in this region often have more complicated margins, with multiple sharp edges and narrow angles. Thus, a new defect model that can accurately simulate this complex in vivo situation is needed. Accordingly, recent 3D printing technologies have enabled the bone graft to be more precisely fabricated to reconstruct such defects. Besides the enhancement of function and esthetics after reconstruction, 3D-printed customized graft is advantageous in that no fixation is needed, as our study has shown. Also, the precise contact between the defect margin and the graft could facilitate the healing process by allowing better communication of the biofactors.35,36 In this sense, our 8-shaped defect model could fulfill the current need of a new bone defect model that can simulate complex bone defects. In particular, the acute angle part of our 8-shaped defect model plays a key role for simulating complex-shaped defects with sharp edges and narrow angles, which can be observed in common craniomaxillofacial defects.
Theoretically, the length of our 8-shaped defect was 14 mm at the vertical axis (8-shaped defect diameter) and 4 mm at the middle horizontal axis (the intersection of circles) at the contact point between the two circles (Fig. 1c). However, when we created the 8-shaped defects, the length was 13 ± 0.26 mm at the vertical axis and 3.7 ± 0.43 mm at the middle horizontal axis. This discrepancy may be due to the curvature of the calvarium and vibration of the bur, which is driven by motors. Our CT data showed that bone healing started from the margin of our 8-shaped model, and the middle waist area (the shortest distance) had closed by 8 weeks after defect creation. At 12 weeks, less than 30% of the bone was filled with newly generated bone. These results are comparatively in accordance with previous studies regarding conventional CSD in a rabbit calvarial simple circular model. 37
The most useful advantage of this 8-shaped defect is the feedback of the accuracy of the 3D-printed graft. To produce a 3D-printed graft material, several critical engineering processes are needed. First, the 3D CT images should be converted to an STL file for transfer to a 3D printer. Each step in the manufacturing of 3D-printed products may result in some distortions of the shapes and sizes from the original defect. As we hypothesized, a complex design such as our 8-shaped defect exhibited this difference more clearly compared with a simple shape such as a circle (data not shown). Indeed, we could clearly detect this difference when the fabricated graft was first implanted at the defect, especially at the 8-shaped defect waist area, which has a sharp edge and narrow angles.
In terms of the reproducibility of the 8-shaped defect model, the size of the initial defect was significantly similar in all cases, although the 8 shape was different from the theoretical ideal 8 shape (Fig. 1d). In our experience, when creating the 8-shaped defect properly, three major points must be considered. The first is the difference between the cutting plane of the trephine bur and natural calvarial curvature, which may cause the defect to have an unfavorable shape. The second is to control the pressure of the trephine bur because it may cause substantial penetration of the rabbit brain, which is often fatal. The third is to suture the periosteum of the calvarium. As the periosteum has the highest potential for regenerating a bone defect, covering the defect with the periosteum may affect new bone formation. Therefore, some surgical training might be needed to create a consistent 8-shaped defect to ensure experimental quality.
Fitting ability evaluation showed that most grafts fit tightly to the defects, demonstrating that the 3D-printed grafts were well fabricated and did not require additional fixation. At 16 weeks after implantation, the grafts were found in the same place that they were implanted and were gradually replaced by newly regenerated bone. The goal of the study was not to test new bone formation, but rather to evaluate the feasibility of using 3D-printed bone graft for reconstruction of a complex bony defect; nevertheless, we observed that new bone formation tended to be more rigorous at the graft site compared with the control site, although the difference was not statistically significant. One possible explanation for this lack of significance is that the bone graft materials we fabricated in this study were made from PCL, which has been proven to be not resorbed for 3 years in vivo. 38 Therefore, our bone graft remained almost intact during our observation period. Only the porous area in the scaffold was able to become regenerated with new bone. This was corroborated by the fact that the amount of newly regenerated bone at 16 weeks was similar to that of the porous area of the intact scaffold. As recent studies have reported, the material of bone graft that can be fabricated by 3D printing technology can be improved according to the purpose of graft.34,39
In terms of morbidity of the animals due to defects on the calvarium, no serious complications or fatalities occurred during the study period, demonstrating that this model meets the animal experiment regulations of our institution. An additional advantage of this rabbit model is that the calvarial size allowed for two 8-shaped defects with CSD, enabling comparison of groups with different conditions in the same animal. In conclusion, this study suggests that our 8-shaped defect using a 7-mm trephine bur could provide a CSD and is useful to evaluate 3D-printed grafts in diverse bone regeneration studies.
Footnotes
Acknowledgments
The license of the Mimics program used to convert the CT images to 3D images was obtained with the help of Professor Shim Jin-Hyung of Korea Polytechnic University (KPU). We thank the Laboratory of Animal Research core facility at the ConveRgence MEDIcine Research CenTer (CREDIT), Asan Medical Center for support and instrumentation. This research was supported by a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HI14C2143).
Disclosure Statement
No competing financial interest exists.