
Abstract
Introduction:
The inflammatory cascade and production of prostaglandins may play a role in the pathogenesis of arthrofibrosis, a debilitating condition after joint replacement and other orthopedic procedures. Cyclooxygenase 2 (COX-2) inhibitors may mitigate the inflammatory response and formation of arthrofibrosis, but oral delivery is associated with risk of systemic side effects in many patients. The nonsteroidal anti-inflammatory drug, celecoxib, may have therapeutic benefits for arthrofibrosis, but current methods for its local delivery (e.g., biologically derived microspheres) are not translatable to immediate clinical use. Therefore, we investigated the use of a drug scaffold for sustainable intra-articular delivery of therapeutic doses of celecoxib.
Materials and Methods:
Celecoxib was eluted from clinically approved biodegradable collagen membranes over 7 days as measured by UV spectroscopy and high-performance liquid chromatography/mass spectroscopy. Eluted concentrations of celecoxib were examined for toxicity (live/dead staining) and profibrotic gene expression (real-time-quantitative polymerase chain reaction) in rabbit knee capsular fibroblasts in vitro.
Results:
Sustained concentrations of celecoxib eluted from the membrane over 7 days from both a wet and dry scaffold, with a burst release (30–45%) of celecoxib in the first 2 h. Rabbit cells treated with eluted concentrations experienced a toxic response to the burst release doses, and inhibitory effects on profibrotic genes were seen in response to the sustained doses eluted from the scaffold.
Conclusions:
This study characterized the novel use of collagen scaffolds for intra-articular drug delivery to treat arthrofibrosis. Scaffolds exhibit celecoxib release through an initial burst release followed by sustained release of antifibrotic doses over 7 days. Thus, collagen scaffolds are promising for clinician-directed treatment of arthrofibrosis.
Impact Statement
This study introduces a biodegradable drug scaffold for the treatment of arthrofibrosis. This scaffold elutes a sustained concentration of COX-2 inhibiting drug at anti-fibrotic doses over seven days. Placement of this scaffold in the intra-articular space may attenuate the arthrofibrotic disease process.
Introduction
A
One potential option includes the use of a drug delivery scaffold to deliver local and sustainable therapeutic doses of celecoxib. A celecoxib-loaded scaffold could be placed into the joint during surgery. This method would allow for a minimally disruptive and clinician-directed method, to sustainably deliver celecoxib into the joint. Furthermore, the scaffold investigated in this study is FDA approved, increasing the direct translatability of this treatment method. Moreover, our group has previously shown that this particular scaffold safely biodegrades without causing any osteochondral damage or fibrotic response within the joint.6,7
Before in vivo use, we sought to characterize the physical features of the scaffold, the celecoxib elution kinetics, and the effect of the observed eluted celecoxib concentrations on rabbit knee capsular fibroblasts in vitro.
Materials and Methods
Scaffold and drug
This study used the HeliMEND Advanced Collagen Membrane (LifeSciences Corporation, Plainsboro, NJ). The scaffold is an FDA-approved multilayered collagen membrane made of nonfriable, semiocclusive, type 1 bovine collagen matrix. The scaffold has a textured surface with a cross section showing condensed laminated sheets with a pore size of 0.004 μm, and biodegrades into surrounding tissues within 18 weeks (Product insert; LifeSciences Corporation). Celecoxib (99.9% pure; Tocris Bioscience Bristol, United Kingdom) was dissolved in a mixed solvent solution of DMSO (Sigma-Aldrich, St. Louis, MO) and phosphate-buffered saline (PBS, 1 × , pH 7.4; Thermo Fisher Scientific, Waltham, MA) at a ratio of 63% DMSO to PBS. A mixed solvent solution was required to account for the hydrophobicity of the drug and the hydrophilicity of the scaffold. The collagen scaffolds (1 × 1 cm) were submerged in the drug solution and placed on a rocking platform for 24 h. The amount of celecoxib loaded onto each scaffold was measured by estimating the total volume of drug solution absorbed by the scaffold as measured by micropipette.
Scanning electron microscopy
High-resolution scanning electron microscopy (SEM) images of the scaffold were taken immediately after being loaded with celecoxib. The scaffold was immersed in Trump's Fixative, rinsed with solutions of increasing concentrations of ethanol (with 100% ethanol used as a critical point dryer), and then fixed to an aluminum plate and sputter coated with gold palladium dust. Images were taken at low (30 × ), medium (200 × ), and high (1300 × ) magnification (Fig. 2A–F).
Elution protocols (dry and wet)
Two elution protocols were used; for the purpose of this study, they are named “dry” and “wet.” The dry protocol measured the elution properties from a dried scaffold impregnated with celecoxib. This required removing the scaffold from the drug solution and placing it in a 37°C sterile incubator for 24 h to fully dry. Once dry, the scaffold was placed in PBS to measure elution. Conversely, the wet protocol investigated the elution properties of a freshly loaded scaffold. In this protocol, the scaffold was removed from the drug solution and immediately placed into PBS to measure its elution. All experiments were completed in triplicate. At the beginning of both protocols, the scaffold was suspended in a 1 mL PBS solution and placed in a 37°C incubator. The PBS was drawn off at each time point (1 h, 2 h, 4 h, 8 h, 16 h, 24 h, 3 days, and 7 days) and then each scaffold resuspended in a fresh 1 mL of PBS. The experimental conditions are summarized in Figure 1A.
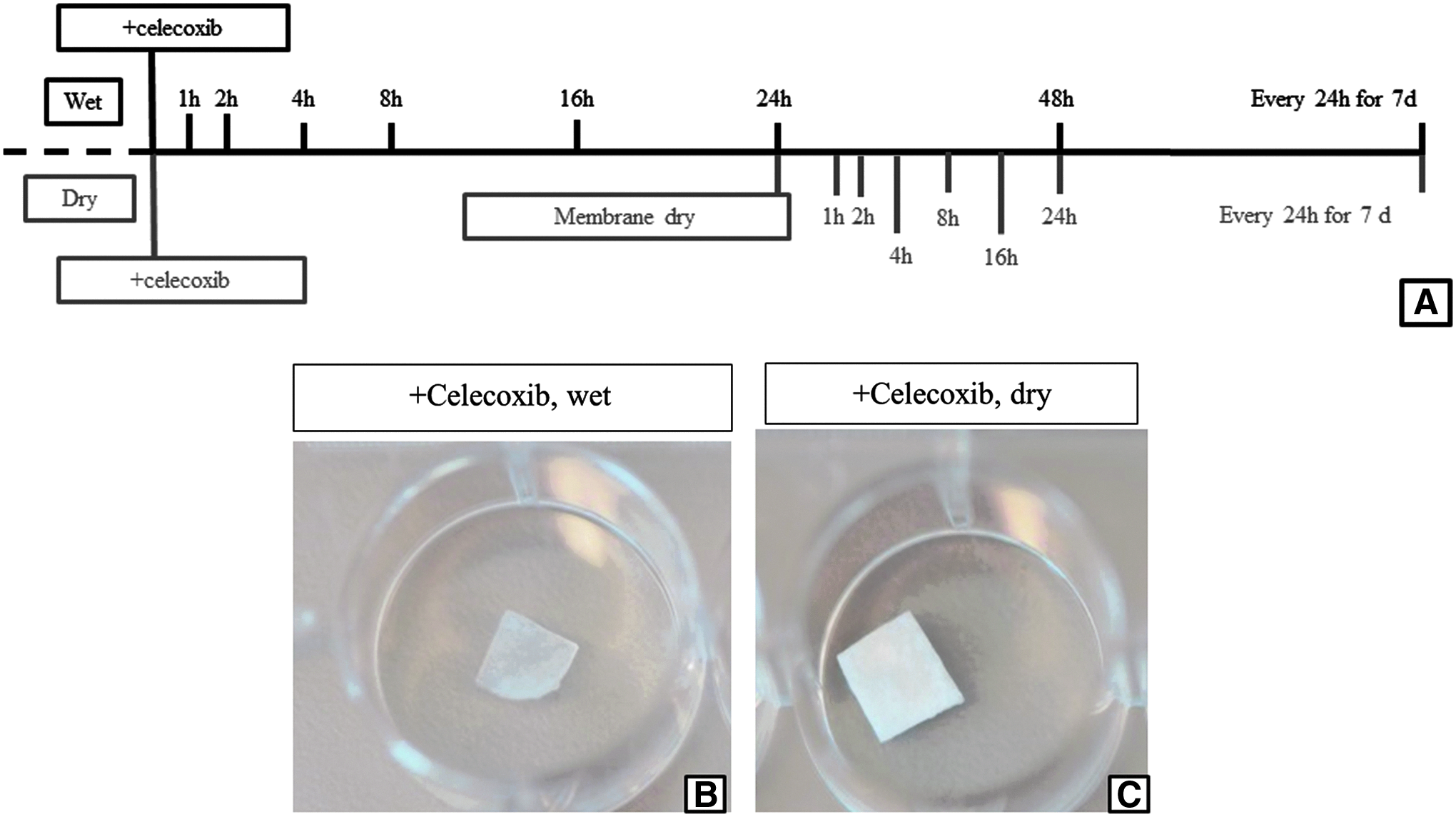
Elution study design and loaded scaffold.
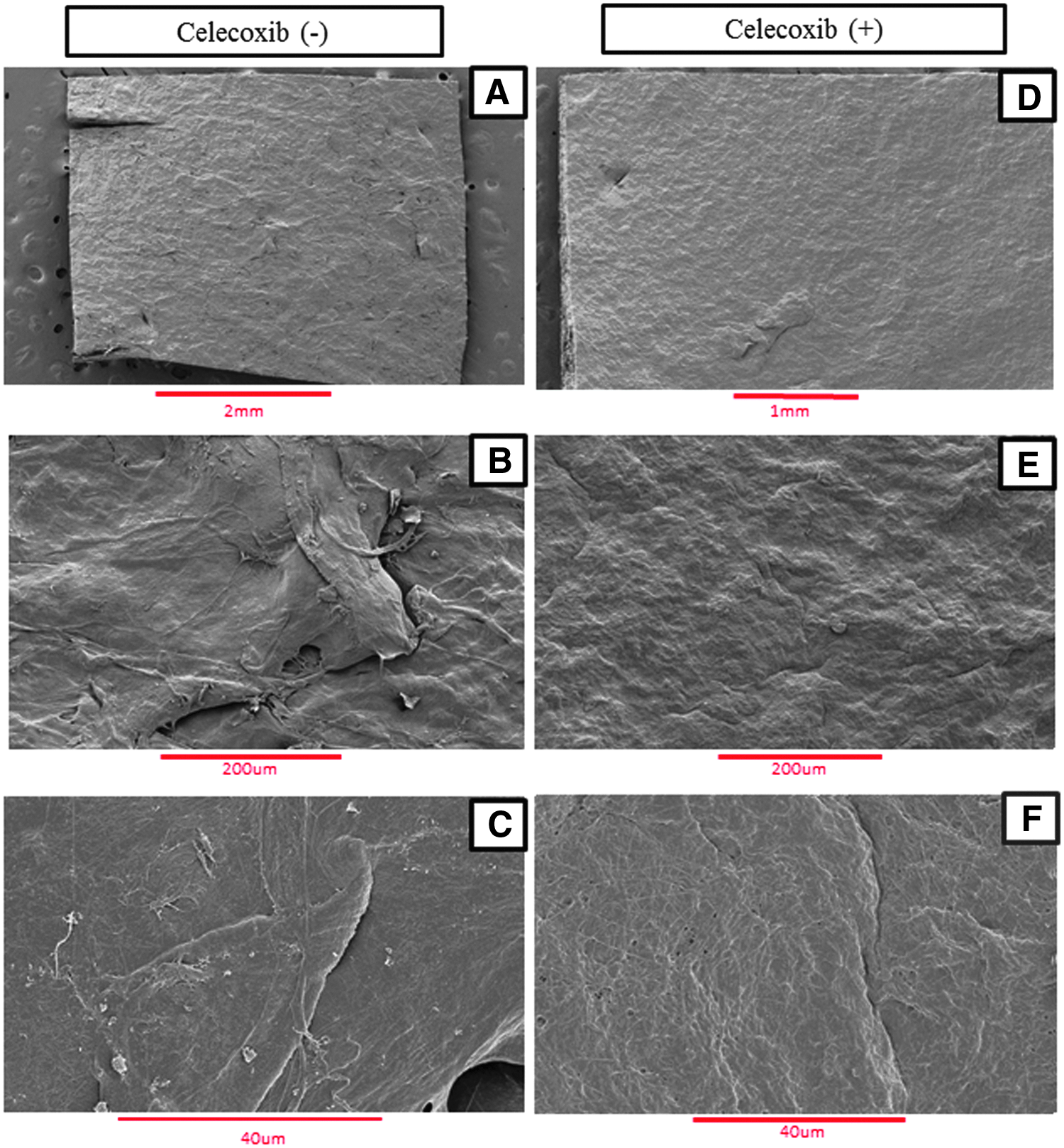
SEM images of scaffold.
Ultraviolet spectrophotometry and high-performance liquid chromatography/mass spectroscopy
Ultraviolet spectrophotometry (UV-Spec) measurements were used to quantify the celecoxib concentration of the eluates of the dry and wet protocols. These measurements were made using a NanoDrop 2000 Spectrophotometer (Thermo Fisher Scientific). One microliter of eluate was pipetted directly onto the measurement pedestal. The absorbance at 252 nm was used to quantify the amount of celecoxib in each solution. The absorption for the eluates was plotted along a standard curve (Appendix 1). A high-performance liquid chromatography/mass spectroscopy (HPLC-MS) system was used to quantify celecoxib in a confirmatory elution study. The details and specifications of the HPLC method and hardware used are found in Appendix 2.
Cell lines and culture conditions
Rabbit knee synovial capsule primary outgrowth cells (rPOGs) were obtained from surgical waste tissue collected from a previous rabbit study. 7 The rPOGs were passaged 3–5 times before experimentation and cultured in 10% fetal bovine serum supplemented with or without celecoxib. For experimentation, all cells were cultured on 6-well polystyrene plates (Corning, Inc., Corning, NY) at 10,000 cells/cm2.
Live/dead assay
The toxicity of observed celecoxib eluates on rPOG cells was quantified using a Live/Dead cytotoxicity stain. Celecoxib-treated rPOG (0, 12.5, 25, 50, 100, and 200 μM) were cultured for 3 days, with live/dead assays performed on the third day. The fluorescence of the Live/Dead stains was quantified using an Infinite 200 PRO multimode plate reader (Tecan, Mannedorf, Switzerland).
mRNA analysis
Transcript levels of celecoxib-treated rPOG cells were measured using real-time-quantitative polymerase chain reaction (qPCR). Cells were treated with 0, 5, and 30 μM concentrations of celecoxib, and RNA was extracted at days 0, 3, and 7. Details of mRNA extraction and RT-qPCR methods are found in Appendix 2.
Statistical analyses
A Wilcoxon rank-sum test was used to compare the amount of drug eluted from the wet and dry scaffolds. The same test was used to compare gene expression values for cells treated with celecoxib versus untreated controls. All statistical analyses were performed using JMP statistical software.
Results
Physical properties of scaffold
Qualitative observations of the scaffold (1 × 1 cm) loaded with celecoxib revealed a hard, nonpliable membrane when dry (Fig. 1C), and a thin, pliable membrane when wet (Fig. 1B). SEM revealed layered collagen sheets as evidenced by the spread layers at the border of the scaffold (Fig. 2A, D). Higher magnification revealed distinct qualitative differences in the scaffold surface texture between the celecoxib-loaded scaffold and the unloaded scaffold—specifically a “smoothing” out of the textured surface, giving the appearance of a “painted on” drug solution (Fig. 2A–C vs. Fig. 2D–F). In addition, SEM revealed a “swelling” of the scaffold after being loaded with celecoxib, suggesting that the drug solution fully absorbed into the inner collagen sheets of the scaffold (Fig. 2D–F).
Celecoxib elution
All scaffolds (both dry and wet) experienced a burst release (24–30% of total drug) in the first hour. This roughly halved for each time point thereafter, with each scaffold consistently reaching a low release dose (∼1% of total drug) per time point for 7 days (Fig. 3C, F). After 7 days, the dry scaffold released a higher percentage of loaded celecoxib compared with the wet scaffolds (89% vs. 67%; Fig. 3C, F). In addition, the dry scaffold released a greater amount of loaded drug within the first 24 h (77% vs. 62%; p < 0.05, Fig. 3B, E). Finally, the dry scaffold's initial burst release (1 h) was lower than the wet scaffold (24.5% vs. 30.2%, Fig. 3A, D).

Celecoxib elution from scaffold.
The concentration of celecoxib released at the 1-h time point ranged from ∼125 μM to ∼380 μM (Fig. 4D). This variability was reduced at later time point, with consistent release rates of ∼30–75 μM per unit time (Fig. 4D). Dry scaffolds had a lower burst release in the first hour compared with wet scaffolds (120 μM vs. 380 μM). In addition, dry scaffolds eluted a more consistent profile than wet scaffolds, although they released a lower percentage of the total drug loaded (Fig. 4D). Finally, the elution profile observed using HPLC-MS was similar to the elution profile observed using UV-Spec (Appendix 3).
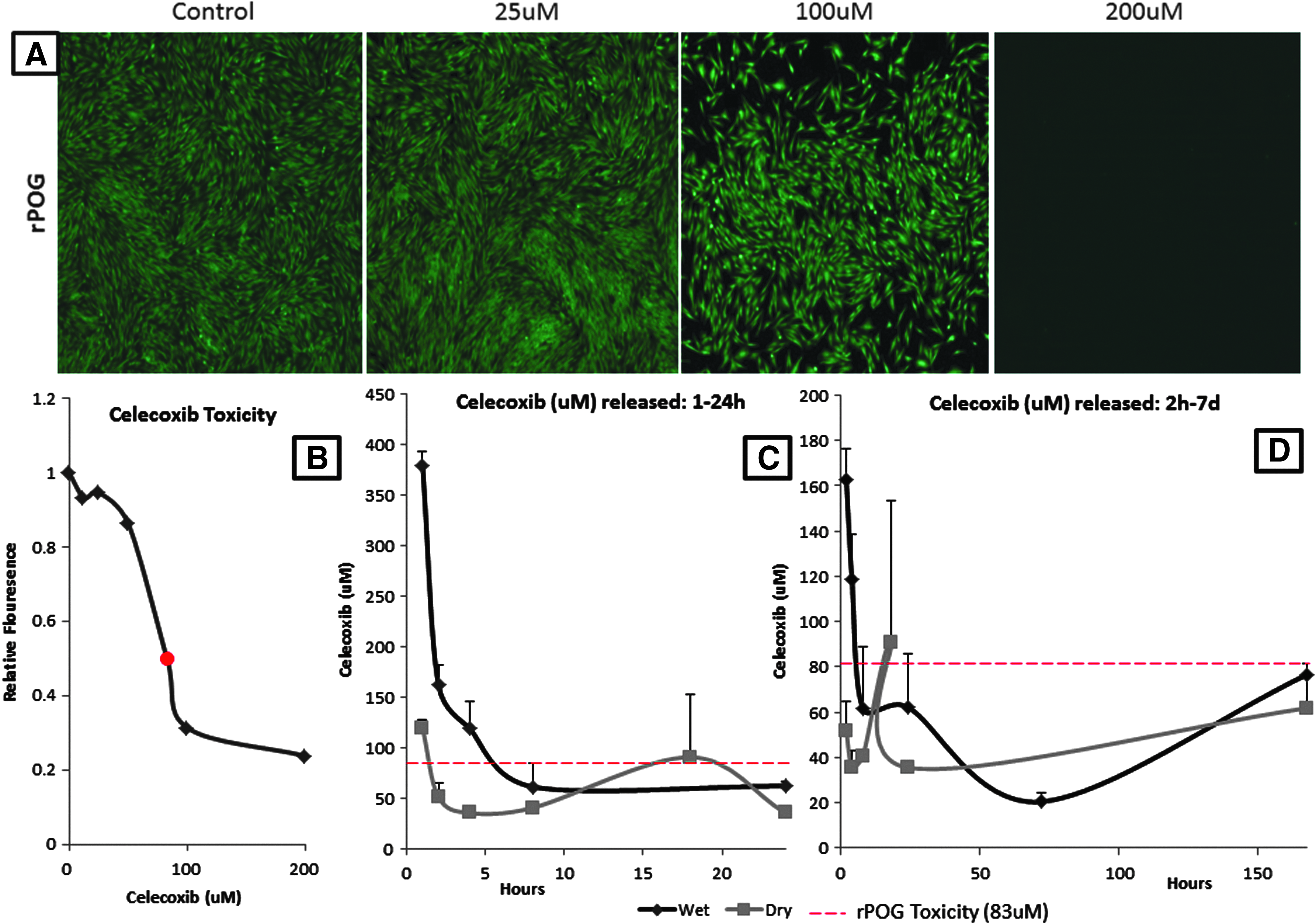
Toxicity of eluted doses of celecoxib on rPOG cells.
Cell toxicity
The cell viability of rPOGs sharply declined at concentrations greater than 50 μM. A 50% reduction of live-cell fluorescence occurred at a dose of 83 μM (Fig. 4B). Notably, at doses of 200 μM, there were no living cells visible. At lower concentrations (0–50 μM), there were negligible differences in cytotoxicity (Fig. 4A, B). The relationship between the concentration of celecoxib eluted from the scaffold and the cytotoxicity was clearly visualized (Fig. 4C, D).
Gene expression
The response of human adipose derived mesenchymal stem cells to celecoxib was tested over the course of 7 days (Fig. 5A). Cells treated with low concentrations of celecoxib (30 μM) were examined for a panel of mRNA markers to understand cell phenotype-related changes in gene expression (Fig. 5B). Celecoxib treatment resulted in statistically significant downregulation of key fibrotic biomarkers, including expression of mRNAs for α-smooth muscle actin (αSMA or ACTA2) and the α1-chain of collagen type I (COL1A1), within 7 days of drug treatment (p < 0.05). This pattern of gene expression indicated that cells lost their ability to produce a myofibroblast-related αSMA/ACTA2 and the main collagenous COL1A1 protein that forms the extracellular matrix of fibroblasts in fibrotic tissue.
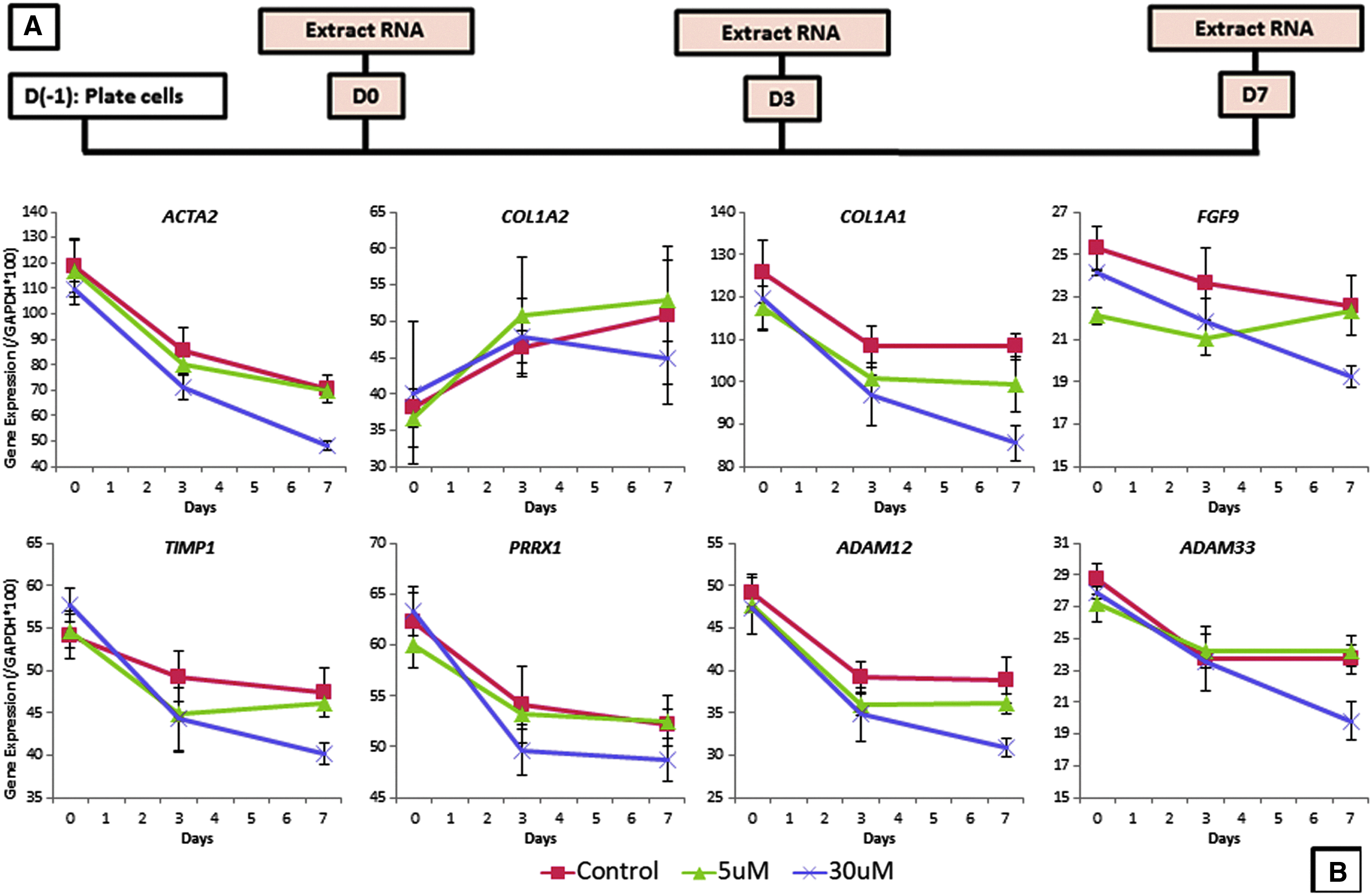
rPOG cellular response to eluted doses of celecoxib.
Discussion
Current treatments for arthrofibrosis are limited and subject to high rates of disease recurrence.1–4 Inflammatory-induced prostaglandin synthesis has recently been implicated as a key mediator of the arthrofibrosis disease process. As such, disruption of this pathway, specifically through the use of COX-2 enzyme inhibition, may offer novel therapeutic attenuation of arthrofibrosis. The use of COX-2 inhibitors, celecoxib specifically, is widely used to reduce inflammation, although this drug is typically administered orally. Sustained delivery of celecoxib within the joint space has shown limited success in vivo and typically requires the use of complex biologically derived lipoprotein vesicles with limited translatability. Furthermore, the use of celecoxib lipoproteins would likely require repeated intra-articular injections, which carries risks to patients' joints. The use of such a disruptive delivery method could potentially induce a fibrotic cascade and increase the risk of joint infection.8,9 Therefore, a minimally disruptive method of delivering celecoxib into the joint space for the treatment of arthrofibrosis would have strong potential for clinical translation and application. This study characterized the properties of an FDA-approved collagen membrane, and its ability to sustainably elute therapeutic doses of celecoxib in vitro.
The drug delivery scaffold studied was a thin nonfriable “paper-like” collagen membrane. The physical properties changed slightly depending on whether the loaded scaffold was dry or wet, with the dry scaffold being stiffer than the wet scaffold. These observed physical properties suggested that this scaffold is ideal for intra-articular implantation, as the membrane is capable of being easily placed into the joint by a surgeon without damaging the scaffold or surrounding tissues. Specifically, the dry scaffold would be preferable to the wet scaffold because it is less likely to become damaged during intra-articular implantation due to its stiffness.
Closer examination using electron microscopy of the scaffold without celecoxib revealed a multilayered collagen sheet with a roughened surface. SEM images of the scaffold loaded with celecoxib showed the drug solution “smoothing” the roughened surface. In addition, the scaffold appeared swollen, suggesting incorporation of the drug into the layers of collagen. The properties observed by SEM provided a mechanistic explanation for the burst drug release seen in the first time points of the elution studies, through which the majority of potentially therapeutic agents are administered quickly. This pattern of drug delivery is preferable for the treatment of arthrofibrosis in vivo, as previous studies have illustrated that immediate postsurgical inflammation is the critical time point for the development of arthrofibrosis.10–14 In addition, the impregnated appearance of the scaffold could explain the sustained release of small amounts of celecoxib over 7 days, as the drug may have deeply embedded itself within the internal collagen sheets of the scaffold. Sustained release at small doses is also suitable for the treatment of arthrofibrosis, as previous studies have shown elevations of profibrotic genes in the first 14 days of contracture development. A slow release of therapeutic doses of celecoxib during this time period would be critical to interrupting of the progression of arthrofibrosis.
The elution kinetics of celecoxib from the scaffold showed a burst release in the first 4 h and a slow sustained release over 7 days. The dry scaffold provided a smaller burst release, but a more pronounced sustained release when compared with the wet scaffold. Interestingly, under no experimental conditions did 100% of the drug elute from the membrane by the seventh day. This suggests that between 15% (dry scaffold) and 35% (wet scaffold) of the celecoxib was tightly bound to the scaffold. It is important to note that the scaffold is biodegradable and will slowly incorporate (within 18 weeks) into the surrounding tissues. As the scaffold degrades, the tightly bound celecoxib may continue to elute from the scaffold. To confirm this, additional elution studies that degrade the scaffold in vitro would reveal the fine-scale coupling of scaffold degradation and tightly bound celecoxib elution.
Several properties of the dry membrane suggest that it is a more viable drug delivery method than the wet scaffold. First, the dry scaffold is capable of providing a significant burst release, while also sustaining a high dose release over 7 days. Alternatively, the wet scaffold provided a high burst release, but does not sustain a high dose release over 7 days. In addition, the dry scaffold would be easier for surgeons to implant in the operating room, as they would not have to load the drug onto the scaffold during surgery. A celecoxib-loaded dry scaffold prepackaged and ready for implantation would allow for clinician-directed use of this therapeutic. More specifically, the human knee capsule is ∼7 × wider than the rabbit knee capsule, 15 suggesting a scaffold of roughly 7 × 7 cm with a maximum celecoxib drug load of ∼7 mg of celecoxib.
After observing the amount of celecoxib eluted from the scaffold, this study investigated the effects of such doses on rPOG in vitro. These cells were chosen because they closely resemble the cells of arthrofibrosis patients. The burst release doses of celecoxib from both the dry (120 μM at 1 h) and wet (380 μM at 1 h) membranes induced a cytotoxic effect on the rPOG cells in vitro. Observed toxic effects of celecoxib showed that 50% cell death occurred at a concentration of 83 μM, and concentrations below 50 μM resulted in 5–15% cell death compared with untreated controls. The dry scaffold sustained a sublethal release of celecoxib at every time point for 7 days, with the exception of the burst release at 1 h. This provides further evidence that the dry membrane is preferable to the wet membrane—as the wet membrane's initial highly toxic release may damage surrounding tissues.
To investigate whether observed eluted concentrations from the membrane provided therapeutic antifibrotic effects on rPOG cells, cells were treated with low (5 μM) and moderate (30 μM) doses of celecoxib. These doses were both below the observed toxic threshold and comparable with the eluted concentrations observed from the dry scaffold. The low dose, compared with untreated controls, resulted in negligible reductions in the expression levels of profibrotic genes. The moderate dose, however, produced significant reductions in several key profibrotic markers—notably αSMA/ACTA2 and collagen type I/COL1A1. These genes have been implicated as the primary drivers of arthrofibrosis,13,14,16 and this observed reduction in their expression suggests that the dry scaffold is capable of delivering a therapeutic dose of celecoxib over a 7-day timecourse.
Important to note, this study did not coculture the rPOG cells with the collagen membrane. Culturing the rPOG cells in the same well as the collagen membrane proved technically difficult, as the foreign body disrupted the otherwise well-controlled culture conditions. Furthermore, a previous animal study demonstrated the safety, and potentially antifibrotic effects, of the collagen membrane in vivo. 7 Given this demonstrated safety of the scaffold in vivo, this study sought to answer whether concentrations of observed celecoxib elution from the scaffold could attenuate fibrotic gene expression at a sublethal dose.
There were several limitations to this study. First, it is possible that the process of loading the scaffold with celecoxib modifies the molecular properties of the drug. This study did not investigate the effect of the drug on cells as it eluted from the scaffold, as coculturing rPOGs and a drug scaffold proved technically challenging. Future studies could optimize this cell culture method, or treat cells with the celecoxib eluate directly from the drug scaffold. Second, this study did not deeply investigate the reasons why less than 100% of the drug eluted from the membranes in each study. Attempts were made to enzymatically degrade the membrane and quantify drug elution, but the separation of the collagenase enzyme and the eluted celecoxib proved technically difficult. Further elution studies could investigate the hypothesis that the drug irreversibly binds to this drug scaffold.
In conclusion, this study investigated the properties of an FDA-approved collagen membrane as a potential celecoxib delivery scaffold for the treatment of arthrofibrosis. Our findings suggest that this scaffold, when loaded with celecoxib and dried for 24 h, is capable of delivering a sustained antifibrotic dose of celecoxib within the joint space to treat arthrofibrosis. Further studies should test whether the scaffold is capable of reducing contractures in vivo using a rabbit model of arthrofibrosis.
Footnotes
Acknowledgments
We thank members of the orthopedic research laboratories and especially Afton K. Limberg, BS, Meagan E. Tibbo, MD, Amel Dudakovic, PhD, and Roman Thaler, PhD, for their expertise and guidance. Funding was provided by the National Institute of Arthritis and Musculoskeletal and Skin Diseases (F32 AR068134 to E.A.L; R01 AR072597 to M.P.A.; R01 AR069049 to A.J.v.W.; R01 AR072597). In addition, we thank the Anna-Maria and Stephen Kellen Foundation and William and Karen Eby for their charitable contributions that enabled us to pursue this work.
Disclosure Statement
No competing financial interests exist.