
Abstract
Objectives:
Tissue-engineered vascular grafts (TEVGs) have demonstrated potential for treating congenital heart disease (CHD); however, quantitative imaging for tracking functional and structural remodeling of TEVGs has not been applied. Therefore, we evaluated the potential of magnetic resonance (MR) imaging for assessing TEVG wall shear stress (WSS) and wall thickness in a large animal model.
Methods:
Cell-seeded (n = 3) or unseeded (n = 3) TEVGs were implanted as inferior vena cava interposition grafts in juvenile lambs. Six months following implantation, two-dimensional phase-contrast MR imaging was performed at 3 slice locations (proximal, middle, and distal) to assess normalized WSS (i.e., WSS-to-cross sectional area). T2-weighted MR imaging was performed to assess TEVG wall thickness. Histology was qualitatively assessed, whereas immunohistochemistry was semiquantitatively assessed for smooth muscle cells (αSMA), macrophage lineage cells (CD11b), and matrix metalloproteinase activity (MMP-2 and MMP-9). Picrosirius Red staining was performed to quantify collagen content.
Results:
TEVG wall thickness was significantly higher for proximal, middle, and distal slices in unseeded versus cell-seeded grafts. Significantly higher WSS values existed for proximal versus distal slice locations for cell-seeded TEVGs, whereas no differences in WSS existed between slices for unseeded TEVGs. Additionally, no differences in WSS existed between cell-seeded and unseeded groups. Both groups demonstrated elastin formation, without vascular calcification. Unseeded TEVGs possessed greater content of smooth muscle cells when compared with cell-seeded TEVGs. No differences in macrophage, MMP activity, or collagen content existed between groups.
Conclusion:
MR imaging allows for in vivo assessment of functional and anatomical characteristics of TEVGs and may provide a nonionizing approach that is clinically translatable to children undergoing treatment for CHD.
Introduction
C
Biodegradable tissue-engineered vascular grafts (TEVGs) have been developed that demonstrate growth potential in large animal models of CHD5,6 and have recently been translated to clinical practice in children undergoing modified Fontan procedures.7–9 TEVGs undergo a period of remodeling mediated by various inflammatory processes 10 that facilitate the transition of the biodegradable TEVG into a functional neovessel capable of growing with the host. The TEVG remodeling process is thought to be at least partly mediated by macrophage infiltration11,12 and expression of matrix metalloproteinases,6,13,14 ultimately assisting in endothelialization and collagen deposition within newly formed neovessels. Prior work has also demonstrated that cell seeding of TEVGs with autologous bone marrow-derived mononuclear cells (BM-MNCs) before implantation may have a beneficial effect on the remodeling process of TEVGs and result in a decreased incidence of stenosis.6,12,15
The ability to serially monitor the in vivo growth and remodeling of TEVGs following procedures such as the modified Fontan operation is important. Noninvasive imaging approaches, such as echocardiography and X-ray computed tomography (CT), are clinically available tools for detecting anatomical or blood flow abnormalities in large vessels or tissue-engineered conduits; however, magnetic resonance (MR) imaging is currently the only imaging modality that can provide information related to hemodynamics, cardiovascular function, and anatomy within a single imaging session without the need for ionizing radiation. 16 Application of MR-based approaches such as phase-contrast (PC) imaging can provide functional information related to blood velocities and wall shear stress (WSS) on a slice-by-slice and pixel-by-pixel basis across the cardiac cycle, 17 which may possess clinical value for assessing remodeling TEVGs considering the role that WSS alterations may play in regulating endothelial gene expression, 18 atherosclerosis initiation and development, 19 and venous graft stenosis. 20
Therefore, in the present work, we sought to noninvasively assess in vivo WSS and wall thickness of cell-seeded and unseeded TEVGs 6 months after implantation in a juvenile lamb model by applying two-dimensional (2D) PC and anatomical T2-weighted MR imaging. We hypothesized that MR imaging would allow for in vivo analysis of differences in WSS and wall thickness along the length of TEVGs, as well as identify potential group differences in WSS and wall thickness that may exist between cell-seeded and unseeded TEVGs.
Materials and Methods
TEVG scaffolds
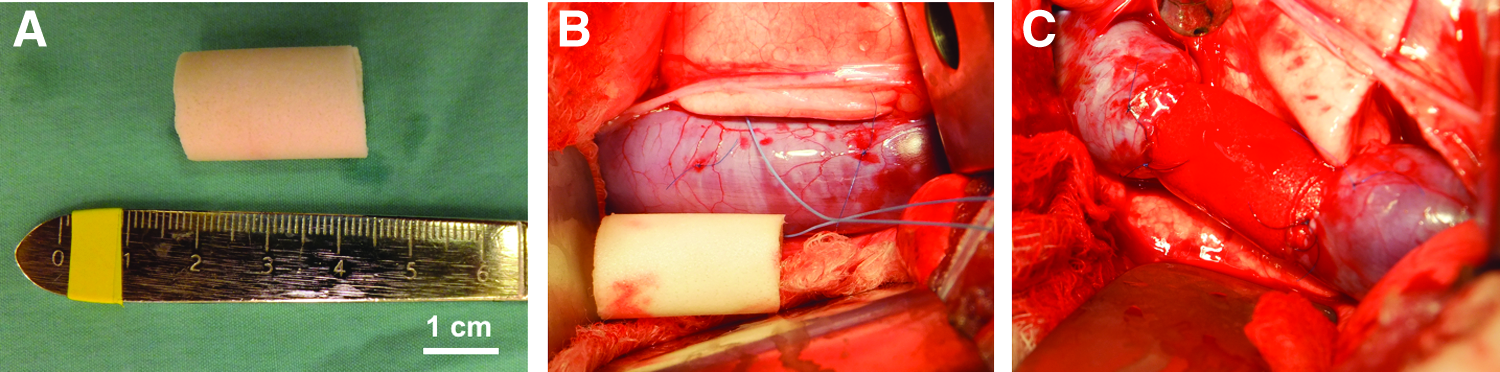
TEVG scaffolds were constructed using a nonwoven sheet of polyglycolic acid sealed with a 50:50 copolymer solution of poly (L-lactic acid-co-ɛ-caprolactone; Gunze Corp, Tokyo, Japan), as previously described. 8 Grafts had a luminal diameter of 18 mm, wall thickness of 1.5 mm, and approximate length of 20 mm before cell seeding and implantation (Fig. 1A).
Cell isolation and cell seeding of grafts
Autologous BM-MNCs were isolated from the iliac crest or femoral head of juvenile Dover lambs (n = 3) while under general anesthesia. A previously developed closed disposable system (Pall Corporation, Port Washington, NY) was utilized for isolation of MNCs from 50 mL of harvested autologous bone marrow using a filtration/elution method, and scaffolds were subsequently cell seeded using a vacuum seeding technique (−50 mmHg), followed by a 2-h period of incubation, as previously described. 21
TEVG implantation
TEVGs were implanted as IVC interposition grafts (Fig. 1B, C) (three seeded scaffolds; three unseeded scaffolds) in six juvenile Dover lambs (implantation weight, 22.1 ± 3.1 kg). Animals were sedated and anesthetized as previously described. 6 The IVC was isolated through right thoracotomy and then underwent 5 min of clamping followed by 2 min of unclamping; this process was repeated three times for preconditioning. An approximately 2-cm long TEVG was implanted using running monofilament 5-0 suture. Radiopaque markers were placed at the anastomoses to assist with future identification. Fibrin sealant (TISSEEL; Baxter International, Deerfield, IL) was used to ensure hemostasis. Animals were treated with fentanyl patches and flunixin meglumine (Banamine; Merck Animal Health, Whitehouse Station, NJ) for postoperative analgesia.
The Institutional Animal Care and Use Committee at Yale University approved the use of animals and all procedures. All animals received humane care in compliance with the “Guide for the Care and Use of Laboratory Animals” published by the National Institutes of Health, Animal Welfare Act, and Animal Welfare Regulations.
In vivo PC MR imaging and analysis
MR imaging was performed 6 months following TEVG implantation on a 3 Tesla whole-body scanner (TIM Trio, Siemens Medical Systems, Erlangen, Germany) using a built-in single-channel transmitter coil and multichannel body and spine phased array coils. Following sedation, animals were intubated and mechanically ventilated (Venturi, Cardiopulmonary Corp, Milford, CT) with 35% oxygen, 65% nitrous oxide, and 1–3% isoflurane. Before imaging, all animals underwent an overnight fast and received an intravenous 500 mL bolus of normal saline to attain euvolemia.
Blood velocities in the TEVG were measured at multiple slice locations using an ECG-gated 2D phase-contrast FLASH sequence (FL-PC), in which the PC was obtained by applying bipolar velocity encoding gradients through the image plane. MR imaging planes were placed perpendicular to the TEVG and were always coplanar for FL-PC imaging (Fig. 2). A minimum of six contiguous imaging planes were placed along the TEVG to ensure full-length coverage of the scaffold. Sixteen to thirty blood velocity measurements were acquired during each R-R cycle. An encoding velocity of 150 cm/s was used for quantification of blood velocity, except during cases of phase wrapping, where a higher encoding velocity of 250 cm/s was alternatively used. Scan time for each slice level ranged from 20 to 35 s, with each acquisition achieved during breath holds that were performed using temporary ventilator disconnection to facilitate reduction of respiratory and cardiac motion. The parameters for the FL-PC were as follows: TR/TE = 20.4/2.19 ms; flip-angle = 25 degrees; slice thickness = 5 mm; pixel-size = 1.0938 × 1.0938 mm; and imaging-matrix = 128 × 256.
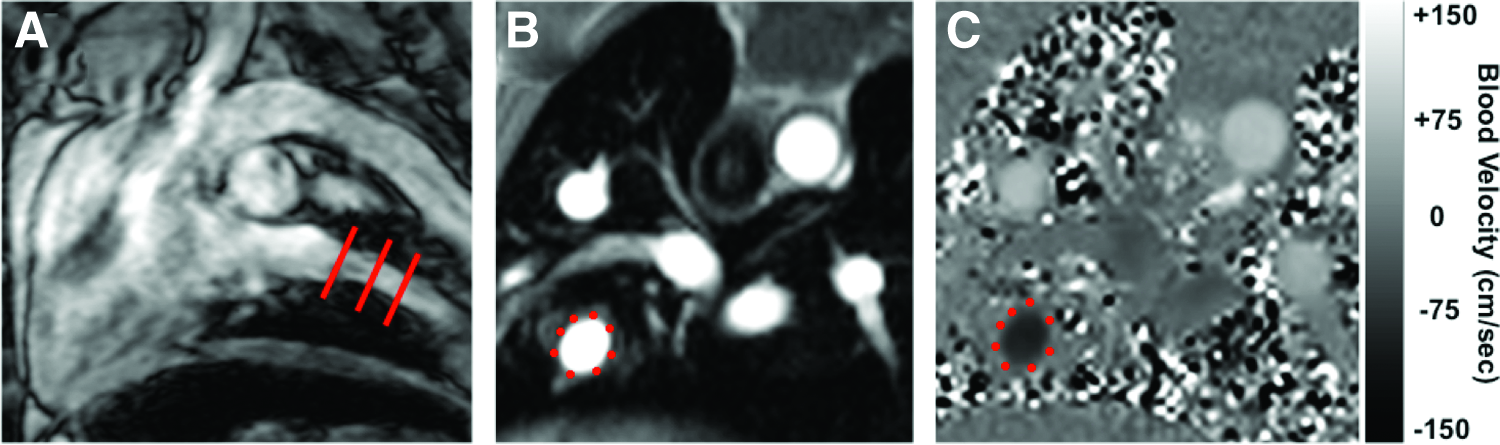
MR imaging of an IVC interposition TEVG for a representative animal at 6 months after implantation.
A phase change of
In vivo T2-weighted MR imaging and analysis
ECG-gated 2D turbo spin-echo (TSE) T2-weighted imaging was used for assessing wall thickness of the TEVG at three slice levels (i.e., proximal, middle, and distal) that were coregistered to FL-PC images (Fig. 3). T2-weighted imaging parameters were as follows: TR/TE = 2000/42 ms; flip angle = 90 degrees; slice thickness = 5 mm; pixel size = 0.875 × 0.875 mm; imaging matrix = 160 × 320; and turbo factor = 9. The scan time for each slice level was 24 s, with each acquisition achieved during breath holds that were performed using temporary ventilator disconnection.

In vivo MR imaging of vessel wall thickness and color-coded 2D map of WSS in TEVGs.
T2-weighted anatomical images were analyzed for TEVG wall thickness using free DICOM viewer software (OsiriX v5.8.2; Pixmeo Sàrl, Switzerland). Specifically, 20 measurements of wall thickness were acquired around the circumference (5 measures per quadrant with 1 average value per quadrant) for each of the proximal, middle, and distal slice locations of the TEVG, and average wall thickness was calculated for each slice location.
Histology and immunohistochemistry
Following explantation of the TEVG at 6 months, portions of the TEVG tissue and native IVC were fixed in 10% formalin, dehydrated, embedded in paraffin, and slides were prepared from 5-μm sections. For histological analysis, slides from each graft explant and native IVC samples were stained following standard histological techniques for Hematoxylin and Eosin (H&E), Masson's trichrome (MT), Alcian Blue (AB), Elastica van Gieson (EVG), and Picrosirius Red (PSR). Immunohistochemistry (IHC) was used to identify vascular smooth muscle cells (αSMA positive), macrophage lineage cells (CD11b positive), and matrix metalloproteinase (MMP) activity (MMP-2 and MMP-9 positive) in the TEVG explants.
Briefly, slides were deparaffinized, rehydrated, and heat-induced epitope retrieval was performed through the citrate buffer method (pH 6.0). Slides were blocked for endogenous peroxidase activity (3% H2O2) and nonspecific binding (Background Sniper, BioCare Medical), then incubated overnight at 4°C with either mouse anti-human αSMA (1:250 Dako), rat anti-human CD11b (1:500; Abcam), rabbit anti-sheep MMP-2 (1:100; Abbiotec), or rabbit anti-human MMP-9 (1:100, Novus Biologicals). Antibody binding was detected with species-appropriate biotinylated IgG (1:200–300, Vector) followed by incubation with streptavidin–horseradish peroxidase and chromogenic development with 3,3-diaminobenzidine. Nuclei were counterstained with Gill's Hematoxylin (Vector) and slides dehydrated and coverslipped.
IHC and PSR image acquisition and analyses
Photomicrographs were obtained on a Zeiss AxioObserver.Z1 inverted microscope with a Zeiss Axiocam 105 digital camera. Representative histological images were acquired at 5 × (with stitching), 10 × , or 20 × . For quantification of IHC and PSR stains, 10–12 random 10 × images were acquired from one midgraft section of each TEVG. Images of native vein samples were acquired in a similar manner. Photomicrographs were converted to the hue, saturation, and lightness color space followed by pixel-specific thresholding to isolate positively stained cells, as previously described using Image J (National Institutes of Health, Bethesda, MD). 23 Reported area fractions correspond to the percentage of pixels satisfying the threshold requirements in the analyzed region of interest, normalized to the mean area fraction of positive staining in the native vein samples.
Statistical analyses
All statistical analyses were performed using commercially available software (GraphPad Prism v7.0 for Mac OS X, GraphPad Software, La Jolla, CA). Between- and within-group differences in wall thickness and WSS were analyzed using two-way ANOVA with Tukey's correction for multiple comparisons. Between-group differences for IHC data (α-SMA, CD11b, MMP-2, and MMP-9) were analyzed using unpaired two-tailed t-tests. Between-group differences for total collagen were also analyzed using an unpaired two-tailed t-test. Differences in collagen fiber thickness were assessed using two-way ANOVA with Tukey's correction for multiple comparisons. p-values <0.05 were considered statistically significant. All values are expressed as mean ± SD unless stated otherwise.
Results
Assessment of TEVG wall thickness
In vivo T2-weighted imaging demonstrated significantly greater average TEVG wall thickness at every slice location in unseeded versus cell-seeded lambs at 6 months after implantation (Fig. 4A). Specifically, average wall thickness was greater in unseeded TEVGs for the proximal (unseeded: 3.0 ± 1.0 mm; seeded: 1.8 ± 0.4 mm; p < 0.0001), middle (unseeded: 2.6 ± 0.8 mm; seeded: 1.8 ± 0.2 mm; p = 0.02), and distal (unseeded: 2.7 ± 0.7 mm; seeded: 1.8 ± 0.2 mm; p = 0.002) slice locations.
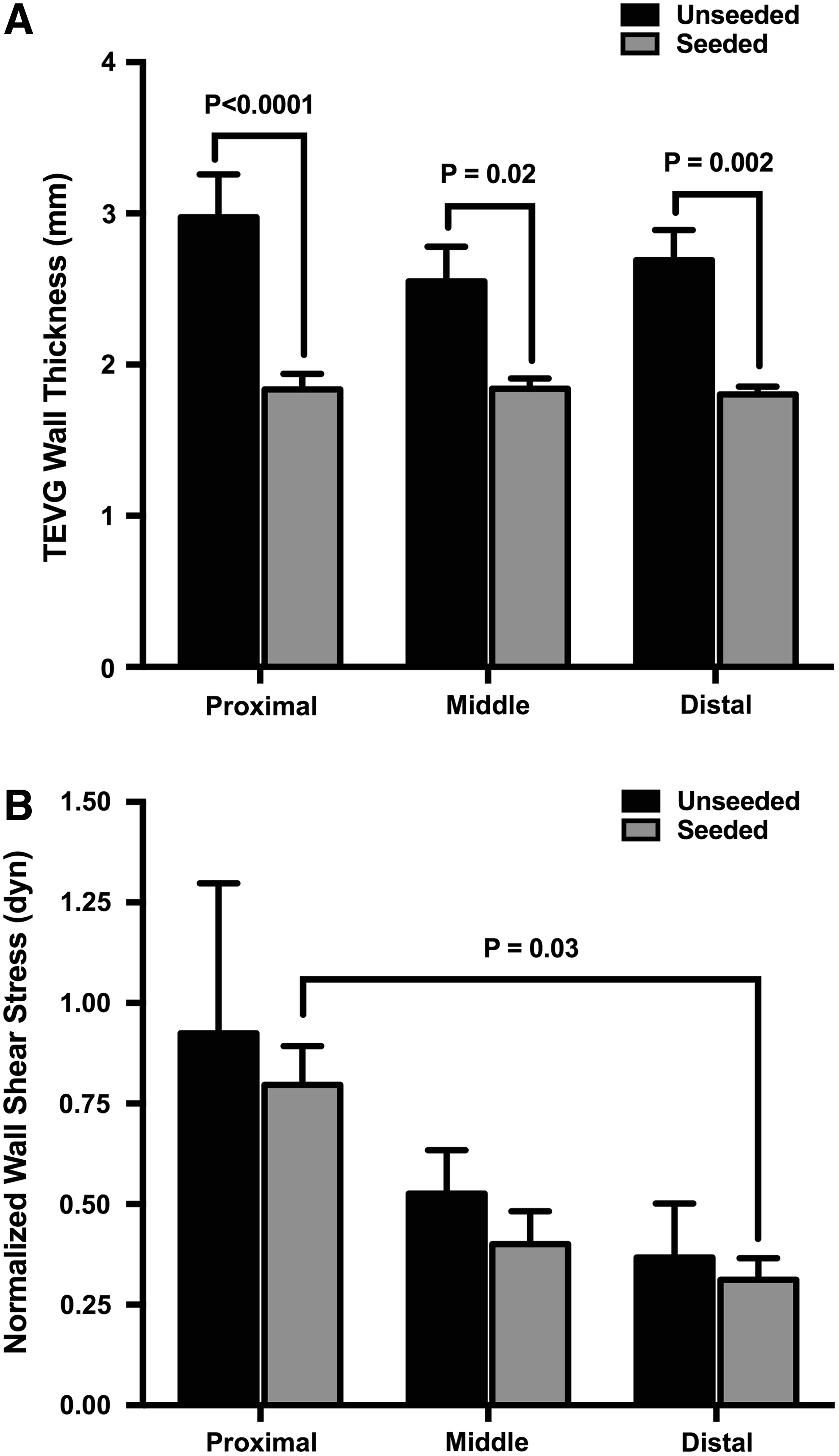
Quantification of in vivo MR imaging.
Assessment of TEVG WSS
In vivo PC imaging revealed no significant differences in WSS between unseeded and cell-seeded TEVGs for any slice location (Fig. 4B). Cell-seeded TEVGs demonstrated significantly higher normalized WSS values in the proximal 2D slice (0.8 ± 0.2 dyn) compared with distal (0.3 ± 0.1 dyn; p = 0.03) slice location.
Histological assessment
Histology of unseeded and seeded TEVGs suggests advantageous vascular neotissue formation in both groups compared with native IVC, without evidence of critical stenosis, aneurysmal dilation, or ectopic calcification (Fig. 5). Samples from both groups demonstrated a collagen-rich extracellular matrix (ECM) with some evidence of elastin formation, although unorganized and immature.
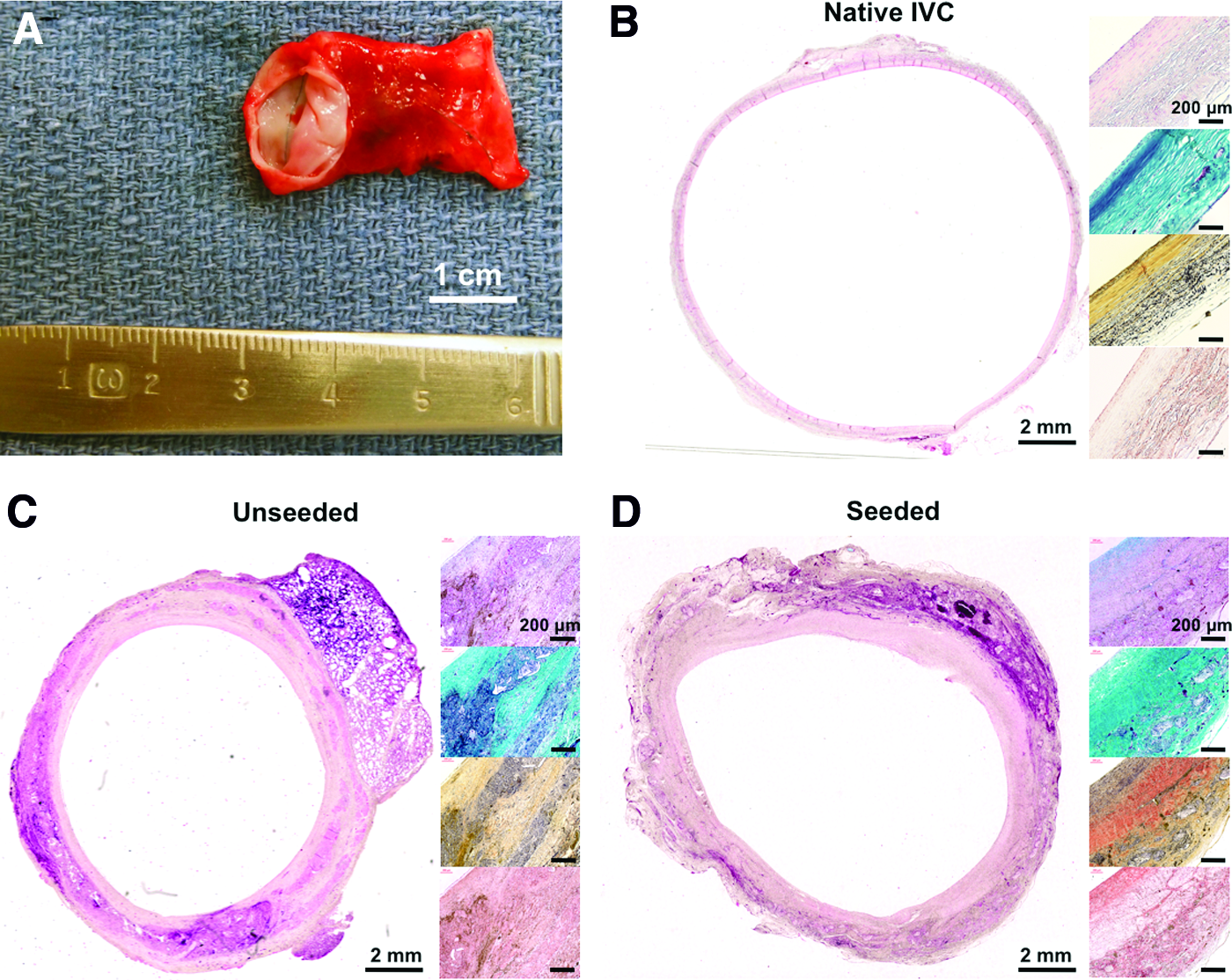
TEVG explant and histological assessment.
Immunohistochemical assessment
IHC staining for α-SMA-positive cells identified a laminated neo-media composed of vascular smooth muscle cells in both groups. Unseeded TEVGs contained a significantly greater amount of smooth muscle cells than cell-seeded TEVGs (Fig. 6A, p = 0.03). CD11b-positive macrophage lineage cells were identified in both groups, supporting previous reports describing the inflammation-mediated process of TEVG remodeling; however, no statistically significant difference in CD11b-positive cells was identified between groups at the 6-month time point (Fig. 6B, p = 0.2). Similarly, no significant differences in MMP-2 and MMP-9 activity existed between seeded and unseeded TEVGs (Fig. 6C, D; MMP-2: p = 0.2, MMP-9: p = 0.06).
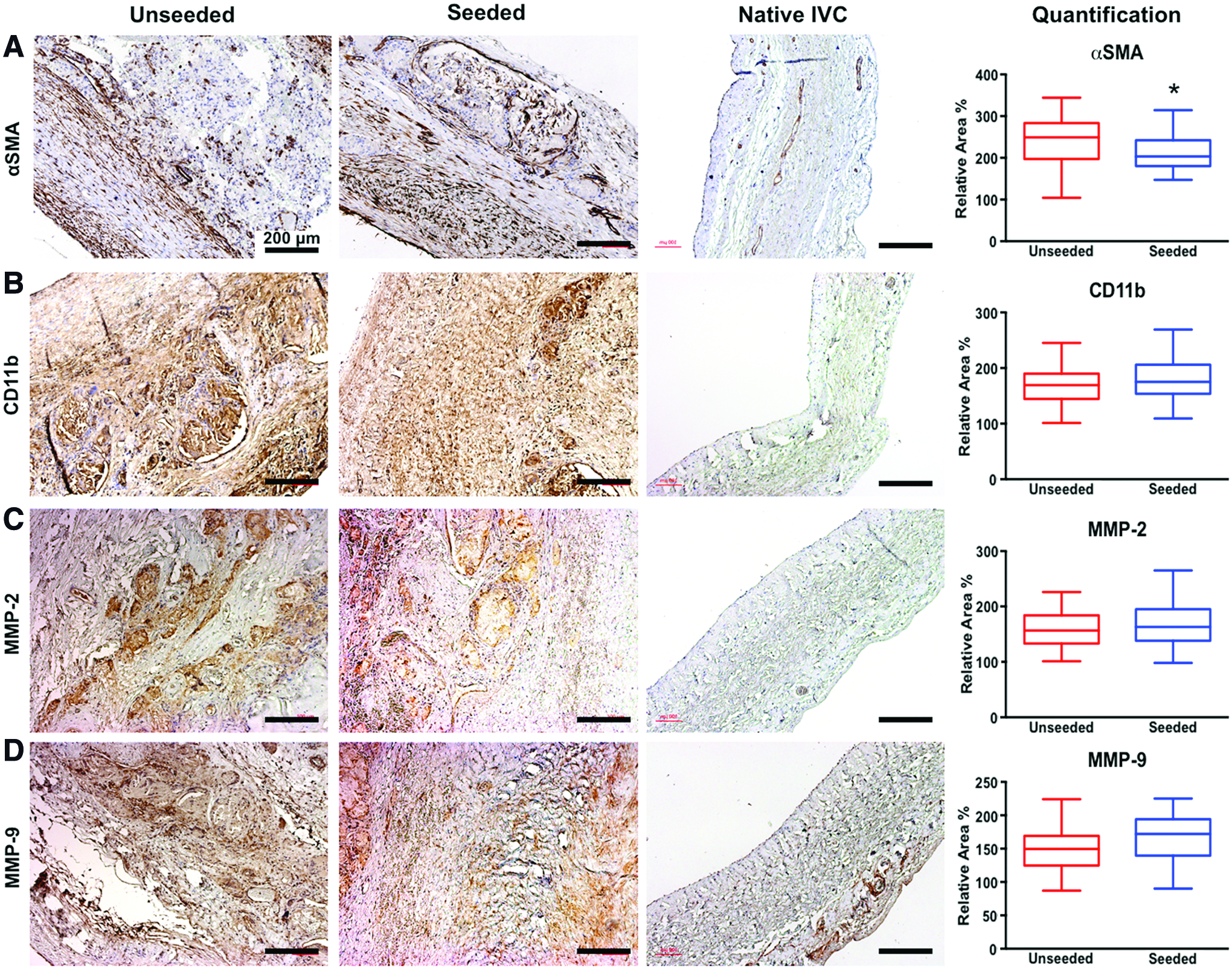
Immunohistochemical analysis comparing unseeded to cell-seeded TEVGs.
Collagen assessment
PSR stains of cell-seeded and unseeded TEVGs imaged with polarized light elucidated the collagen content, organization, and composition in the evolving neovessels (Fig. 7A, B). After normalization to the native IVC, there was no significant difference in total collagen content between the two groups (Fig. 7C, p = 0.9). Analysis of the collagen fiber subsets within the neovessels (red, yellow/orange, and green) corresponding to the gradient of thick/mature to thin/immature fibers demonstrated no differences between unseeded and seeded TEVGs (Fig. 7D).
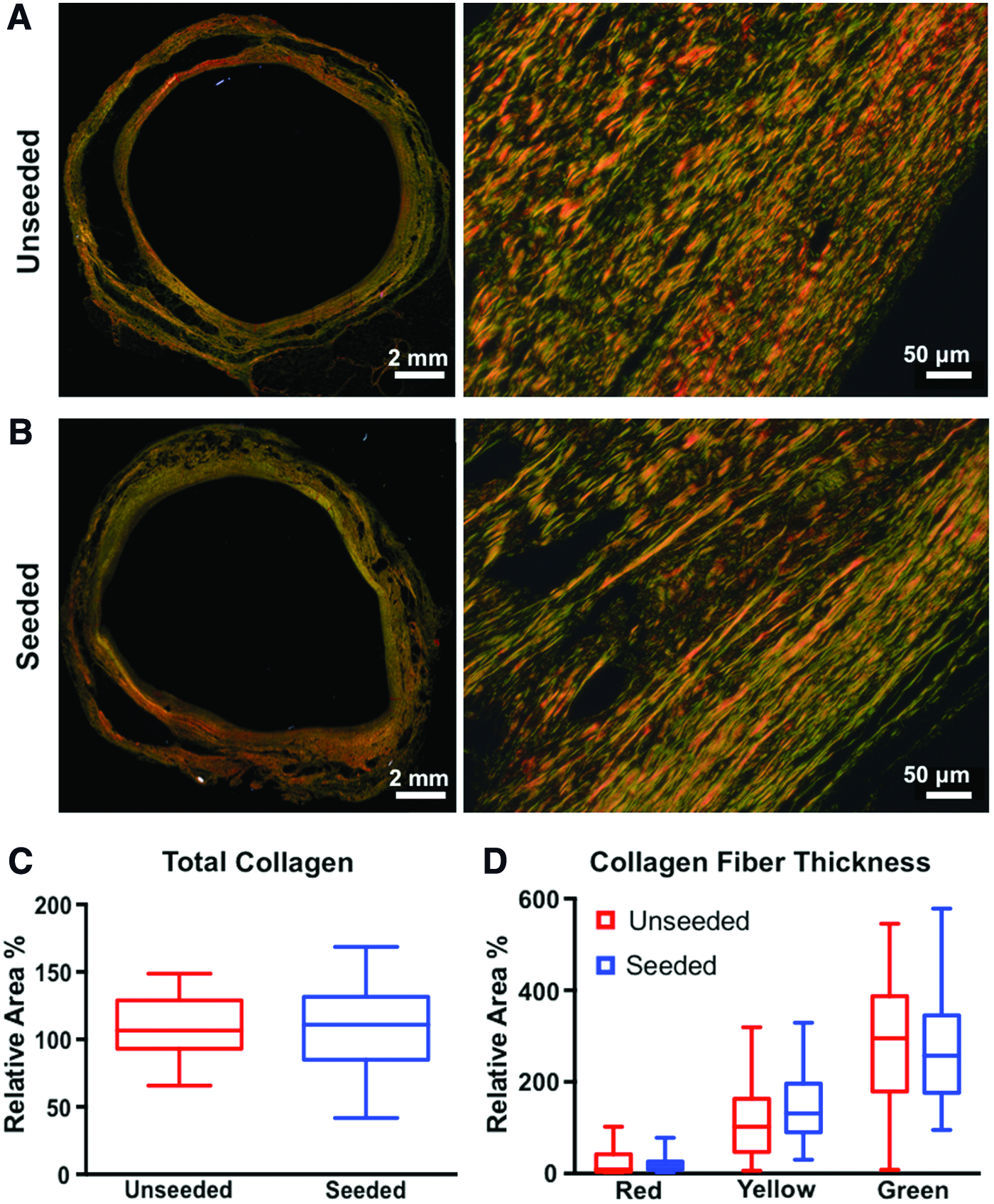
TEVG collagen content analysis. Polarized light microscopy of PSR stained sections from
Discussion
In prior work, our research team has relied upon the mouse model of TEVG implantation to investigate cellular and molecular mechanisms of neovessel formation. 11 We have discovered that in the absence of cell seeding, graft implantation results in an elevated host immune response, directed primarily by host platelet, monocyte, and macrophage infiltration and activity within the scaffold. 12 This excessive inflammation triggers secretion of ECM proteins and hyperproliferation of fibroblasts and smooth muscle cells in the remodeling vessel, which can result in graft stenosis. 12 Consistent with findings from our clinical trial, stenosis is the most prevalent TEVG-related complication in preclinical models. We have recently reported that BM-MNC seeding of the scaffold before implantation mitigates this adverse immune response in a dose-dependent manner, yielding a patent and fully functional neovessel. 24
As we continue to clinically translate TEVGs, a method to verify biological mechanisms underlying the efficacy of cell seeding, observe the natural history of neovessel formation, and monitor the development of stenosis in higher-order species is of critical importance. We have previously investigated the utility of intravascular ultrasound (IVUS), 25 single-photon emission computed tomography (SPECT)/CT imaging, 6 and CT angiography 6,21 to noninvasively assess the effect of cell seeding on TEVG remodeling in the lamb model, but each of these imaging modalities is limited in their ability to provide both high-resolution anatomical (wall thickness) as well as functional (WSS) images of TEVGs.
In the present study, we have demonstrated for the first time the utility of MR imaging for assessing WSS and wall thickness in TEVGs implanted in the IVC of a large animal model. Specifically, 2D PC-MR imaging discriminated significant differences in normalized WSS values between proximal and distal slice locations in cell-seeded TEVGs 6 months after implantation (Fig. 4B). In addition to noninvasively identifying significant differences in WSS between specific slice locations using PC-MR imaging, we have demonstrated significant differences in wall thickness at 6 months postimplantation between cell-seeded and unseeded TEVGs across multiple slice locations using T2-weighted MR imaging (Fig. 4A). Furthermore, we found that quantitative differences in MR-derived measures of TEVG wall thickness between cell-seeded and unseeded TEVG groups also corresponded with a significant difference in smooth muscle cell content between study groups. This association supports the use of PC-MR imaging to potentially monitor the degree and progression of intimal hyperplasia driven by migration and proliferation of synthetic vascular smooth muscle cells in the TEVG neotissue.
Prior studies have applied MR-based approaches for noninvasive monitoring of TEVGs through the imaging of seeded cells labeled with ultrasmall superparamagnetic iron oxide (USPIO) nanoparticles; however, these studies focused on the feasibility of imaging implanted TEVGs or tracking the fate of seeded cells.26–28 In the present study, we sought to apply both PC and T2-weighted MR imaging techniques for functional assessment of WSS and wall thickness in TEVGs implanted as IVC interposition grafts within a large animal model. Through the application of in vivo PC-MR imaging, we demonstrated that cell-seeded TEVGs had significantly higher WSS values in the proximal compared with distal slice location at 6 months postimplantation, whereas unseeded TEVGs did not differ in WSS values between slice locations (Fig. 4B). These findings suggest that PC imaging possesses sensitivity for detecting regional alterations in WSS characteristics, which may be of clinical relevance in TEVGs considering that prior work by Misra et al. 20 has demonstrated in venous hemodialysis grafts that early postimplantation elevations in WSS coincide with the early activation of matrix regulatory proteins (VEGF-A, MMP-2, MMP-9, VEGFR-1, VEGFR-2, and TIMP-1) that have been implicated in late-stage neointimal thickening. The lack of differences in WSS between groups at our 6-month imaging time point in the present study might suggest that any group differences in WSS that did occur may have occurred earlier postimplantation. It is possible that WSS values may have begun to taper off by 6 months postimplantation and associated elevation of molecular markers may have also decreased by this time. Postmortem tissue analysis of TEVGs at 6 months partially supports this notion, as no differences in macrophage or MMP activity between cell-seeded and unseeded TEVGs (Fig. 6) corresponded with no differences in MR-derived measures of WSS between the same groups (Fig. 4B). Although the present study was not designed to evaluate the potential effects of TEVG degradation on WSS and wall thickness, future application of serial MR imaging in TEVGs may elucidate the changes in WSS that occur after implantation as well as following degradation and clarify how these temporal changes are potentially associated with the progression of neointimal thickening and stenosis development.
The lack of differences in MMP-2 and MMP-9 activity between cell-seeded and unseeded TEVGs somewhat differs from our previously published work, which utilized MMP-targeted SPECT/CT imaging to demonstrate significantly higher MMP activity in unseeded versus cell-seeded TEVGs at 6 months postimplantation. 6 However, our prior SPECT imaging work utilized a radionuclide that targeted a broad spectrum of MMP activity (targeting MMP-2, -3, -7, -9, -12, and -13) across the entire length of TEVGs, whereas the present work specifically evaluated MMP-2 and MMP-9 activity from histological slices sampled from the mid level of TEVGs. Nonetheless, our data does agree with that of Cummings et al., 13 who evaluated MMP activity in tissue-engineered pulmonary artery (PA) constructs implanted in lambs and found elevated MMP-2 and MMP-9 activity, relative to native PA tissue, for up to 80 weeks after implantation in tissue-engineered constructs. Although the critical period of TEVG remodeling likely occurs before 6 months in the lamb model, levels of macrophage and MMP activity remain greater in TEVGs when compared with native IVC tissue at 6 months, thus indicating potential chronic, subclinical MMP/macrophage activity, and residence within TEVG scaffolds that persists for longer than 6 months after implantation.
In vivo MR imaging demonstrated significantly greater wall thickness in unseeded versus cell-seeded TEVGs at multiple locations along the length of the graft (Fig. 4A), which corresponds with prior work that has shown cell seeding of TEVGs with autologous BM-MNCs facilitates beneficial remodeling and lower rates of TEVG stenosis.6,12,15 Both PC and T2-weighted image analysis demonstrated adverse remodeling of the proximal slice location of TEVGs, where a noticeable trend in higher WSS values was apparent in the proximal slice locations of TEVGs. The finding that unseeded TEVGs also possessed significantly higher smooth muscle cell content at 6 months postimplantation (Fig. 6A) further supports the benefits of cell seeding.
Our research team has previously demonstrated that smooth muscle and endothelial cell residence in the seeded TEVG scaffold arises from migration of the neighboring native blood vessel into which the scaffold is interposed. 29 Cell seeding is integral to this process by regulating the host immune response to scaffold implantation.24,30 Therefore, cell seeding mitigates host inflammation following TEVG implantation, permitting migration and proliferation of adjacent vascular cells within the scaffold, resulting in successful neovessel formation. In the case of unseeded scaffolds, an extended and excessive immune response to scaffold implantation can exist, which often results in graft stenosis. In cases of patent unseeded grafts, we expect that similar mechanisms of neighboring cell recruitment underlie neovessel formation, yet this hypothesis has yet to be directly tested. Although no differences in total collagen content or collagen fiber thickness were observed between the two study groups (Fig. 7), data in the present study collectively suggest persistent remodeling in both seeded and unseeded grafts 6 months after implantation that may be characteristic of neovessel maturation.
Collectively, the present study demonstrates that PC and T2-weighted MR imaging are useful, relatively fast noninvasive tools that may be used to provide in vivo assessment of both WSS and wall thickness within tissue-engineered vascular constructs. Future studies investigating the potential of these MR-based approaches for serial in vivo tracking of vascular graft remodeling are warranted and could be directly translated into patients receiving TEVGs for palliation of CHD.
Footnotes
Acknowledgments
This work was supported in part by the National Institutes of Health (NIH) grants R01 HL098228 and T32 HL098069, and the Charles W. Ohse Research Award (Department of Surgery, Yale University School of Medicine). Funding was also provided by the Pall Corporation. Funding sponsors of this work had no part in the study design, data collection, data analysis, interpretation of data, or writing of the article.
Disclosure Statement
Drs. Breuer and Shinoka received grant support from the Pall Corporation and Gunze Corporation. Dr. Breuer is on the Scientific Advisory Board of Cook Biomedical. All other authors have no relevant conflicts of interest to disclose.