
Abstract
Blood concentrates are obtained by centrifugation of the patient's own peripheral blood. These concentrates revealed increasing importance in the regenerative medicine and tissue engineering. Many limitations are faced in preclinical research concerning the volume of blood needed to produce platelet-rich fibrin (PRF) matrices (10 mL). This study evaluated for the first time three different centrifugation protocols to obtain injectable PRF (i-PRF) matrices using a small blood volume of 3 mL. Small tubes were specially produced for this study. Blood was collected from 24 Wistar rats (ca. 200 g) for this study using the cardiac puncture technique. From each animal, two tubes were collected: the first was prepared according to the standard PRF protocol without anticoagulation and used for in vitro culturing and histology; the second was anticoagulated and used for automated cell count. Three different relative centrifugation forces (RCFs; high [710 g], medium [177 g], and low [44 g]) were evaluated in this study (n = 8 per RCF). The obtained PRF matrices were cultured over 10 days, and the supernatants were collected for quantification of growth factors (GFs), vascular endothelial growth factor (VEGF), transforming growth factor beta 1 (TGF-β1), and platelet-derived growth factor-BB (PDGF-BB). The results showed that it is possible to produce i-PRF using a small blood volume of 3 mL. Reducing the RCF led to a significant increase in the number of platelets and leukocytes, specifically lymphocytes, within the i-PRF matrices. GF release (VEGF, TGF-β1, and PDGF-BB) was continuously measurable in all evaluated i-PRF matrices over 10 days. The i-PRF matrices prepared using low RCF released significantly more GF compared to those prepared using a medium or high RCF over 10 days (p < 0.05). These findings are in accordance with the previously described low-speed centrifugation concept (LSCC), which was first established using human blood, and may serve as a proof of concept of the LSCC in another species, that is, rats. Reducing the initial blood volume provides many possibilities to implement PRF matrices in preclinical research as an autologous system. However, further studies are needed to evaluate the therapeutic effects of PRF matrices obtained using 10 mL blood compared to those obtained using 3 mL blood.
Impact Statement
This study evaluated for the first time the composition and bioactivity of platelet-rich fibrin (PRF) produced from small animal blood by reducing the initial blood volume needed for the preparation of PRF from 10 to 3 mL. The results showed that different preparation protocols of PRF produced using 3 mL of animal blood exhibit the same composition, properties, and bioactivity as PRF prepared using 10 mL human blood.
Introduction
I
Several systems for blood concentrates exist, including platelet-rich plasma (PRP), plasma-rich growth factor (PRGF), and platelet-rich fibrin (PRF).3,4 These systems have different preparation and processing protocols: PRP and PRGF require the addition of anticoagulants before their centrifugation, and PRP is prepared by multiple-step centrifugation.4,5 The resulting blood concentrates in PRP and PRGF are liquid at first and then further treated with external chemicals to obtain a solid scaffold.4,5
A different strategy is followed in the preparation of PRF, which is the only blood concentrate system that does not require any additional chemicals or anticoagulants. 6 Directly after a single-step centrifugation, PRF is generated either as a solid or a liquid PRF matrix,7,8 which depends on the surface of the blood collection tubes used that were specifically modified to produce either a solid or a liquid PRF matrix. These technical improvements make PRF time saving and easy to implement in the clinical routine.
Several studies have shown the benefit of blood concentrates in clinical applications in oral and maxillofacial surgery, 9 as well as in traumatology. 10 Therefore, many preclinical and basic science studies have focused on understanding the mechanisms of regeneration systems, including blood concentrates, and optimizing the regeneration capacities of these systems.
A histological and immunohistological study investigated the influence of the relative centrifugation force (RCF) in the preparation of solid PRF ex vivo. It was shown that applying a medium RCF leads to a more even distribution of the platelets throughout the solid PRF, while a high RCF leads to the accumulation of cells toward the upper part of the clot. 2 In this sense, the low-speed centrifugation concept (LSCC) was introduced after a systematic analysis of the influence of RCF in three different RCF ranges (high, medium, and low) on the cellular distribution and growth factor (GF) release of injectable PRF (i-PRF) using human blood. 6 The results demonstrated that reducing the applied RCF leads to a significant increase in the number of platelets and leukocytes and the concentrations of key GFs, such as vascular endothelial growth factor (VEGF), transforming growth factor beta 1 (TGF-β1), and epidermal growth factor (EGF).6,7 Following a systematic translational research series, these aspects were further investigated in combination with cell cultures in vitro. 11 It was shown that the combination of i-PRF prepared according to the LSCC with outgrowth endothelial cells and osteoblasts induces a significantly higher rate of microvascular formation compared to the untreated cells. 11 Further in vitro studies showed that treatment with i-PRF significantly enhances the cellular migration rate and collagen-1 production of gingival fibroblasts cultured on titanium surfaces compared to treatment with PRP. 12
To date, for the preparation of PRF, a relatively large volume of peripheral blood (10 mL) is needed to obtain an adequately prepared PRF matrix in accordance with the established protocol of PRF and the rules of centrifugation. 13 As PRF matrices are produced by the centrifugation of fresh blood without anticoagulation, rapid blood sampling is required to obtain homogeneous and uncoagulated blood followed by immediate centrifugation before coagulation starts. 2 Therefore, until now, preclinical in vitro research on blood concentrates has depended on healthy voluntary human donors.7,8,11,12,14 These limitations make preclinical research more complicated in regard to the in vivo evaluation of blood concentrates in small animals. The most commonly used species for well-established in vivo models, mice and rats, exhibit a limited blood volume. 15 Established blood collection techniques of peripheral blood using different anatomic locations, such as the tail vein, facial vein, or even femoral vein, provide slow blood flow and only a small blood volume. 16 Therefore, alternative implantation models, such as the use of severe combined immunodeficiency (SCID) models, were implemented for the in vivo evaluation of PRF produced from human donors. 17
As a first step toward the preparation of PRF from the blood of small animals, the present study investigated for the first time whether it is possible to obtain PRF matrices using a small blood volume of 3 mL. For this purpose, small blood collection tubes were specially produced for this study. In addition, the composition and regenerative capacity of the obtained PRF matrices were characterized to evaluate the quality of PRF obtained from rat blood according to the LSCC as a proof of concept in animals.
Materials and Methods
Animals
The design, analyses, and reporting of this experiment were performed following the ARRIVE guideline checklist for reporting animal research. 18 All the animals participating in this experiment were part of an approved project by the animal care facility (ZFE, Frankfurt am Main, Germany) from the Department of Medicine of the Johann Wolfgang Goethe University in Frankfurt and the regional council committee according to German law (§ 4 Abs. 3 TierSchG). This experiment focused on the technique of blood withdrawal and the protocols to obtain PRF from rats.
Twenty-four outbred female Wistar rats (Rattus norvegicus) purchased from Charles River (Sulzfeld, Germany) at 7–9 weeks of age and weighing ∼200 g were used in this experiment. Two blood samples of 3 mL were obtained per animal; the first was used for in vitro cultivation, GF release quantification, and histology, and the second was used for automated cell count (Fig. 1).
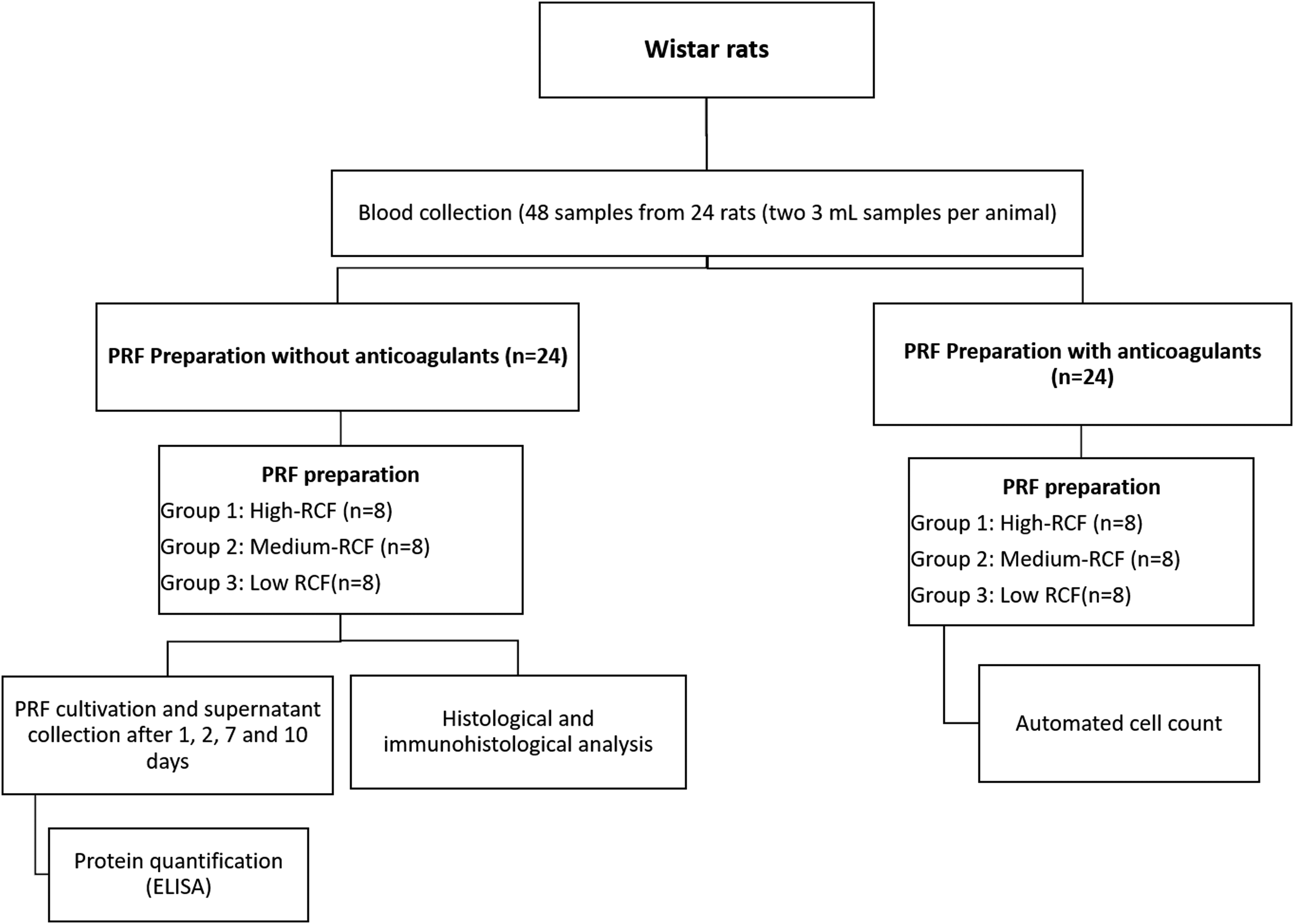
Flowchart of the study design. ELISA, enzyme-linked immunosorbent assay; i-PRF, injectable platelet-rich fibrin; RCF, relative centrifugation force.
The animals were housed in groups of four for 1 week before the experiments for acclimatization and during the postoperative period in a controlled environment (Temp: 20°C, 12-h light/12-h dark cycles, and humidity of 40–70%). They were fed regular rodent pellets and water ad libitum. For blood collection, the animals were euthanized using an intraperitoneal injection of overdosed ketamine/xylazine to induce unconsciousness and asphyxia. Blood sampling was performed by heart puncture as described below.
Blood collection and PRF preparation
The analyses and reporting on PRF in this study followed the previously published on recommendation on standardization of relative centrifugal force values. 19 After euthanasia, the animals were placed in a supine position, and a vertical midline incision was performed along the sternum from the sternal notch to the xiphoid process using a scalpel. The incision was followed by osteotomy of the sternum using Metzenbaum scissors (median sternotomy). During the osteotomy, the thoracic cavity was lifted upwards to avoid injury to the heart. This approach allows the direct vision of the heart for a rapid and precise heart puncture of the right atrium.
Two 3-mL samples of heart blood were collected per animal through a direct cardiac puncture of the right atrium using a 24-gauge butterfly needle. Special focus was placed on blood collection and PRF preparation, as it is important to centrifuge the blood before coagulation starts.
The i-PRF matrices were prepared using small tubes specially designed for this experiment. The first blood sample was directly collected into the sterile plain plastic vacuum tubes (3 mL) (Process for PRF™, Nice, France; Mectron, Cologne, Germany) without anticoagulants and immediately centrifuged (Duo centrifuge, Process for PRF™; Mectron).
The second sample was drawn in clinically approved 3-mL tubes, including trisodium citrate solution (S-MONOVETTE®, Nümbrecht, Germany), homogenized and transferred to the i-PRF tubes (Process for PRF™). After centrifugation, the total i-PRF volume was collected, of which 50 μL was used for automated cell counting.
In addition, the use of these small tubes required adaptors designed to fit with the centrifuge. The centrifuge has a fixed angle rotor with a radius of 110 mm and no brake. At the end of the centrifugation time, the centrifugation process ends automatically.
The i-PRF preparation was performed following the LSCC as previously described 6 (Table 1). Eight i-PRF samples were obtained from eight different rats per protocol.
Different Protocols of Centrifugation Used for the Production of Injectable Platelet-Rich Fibrin Samples
PRF, platelet-rich fibrin; RCF, relative centrifugation force.
RCF expressed in gravitational force (g) was calculated according to the following formula as previously described
17
:
Automated cell counting
Automated cell counting was performed as described before.6,7 The analysis was performed at the German Red Cross Blood Donation Service in Baden-Württemberg-Hessen, Frankfurt am Main, Germany, using a cell counter (HEMAVET®; Drew Scientific, Inc., Miami Lakes, FL). The focus of the analyses was to determine the concentrations of total leukocytes and lymphocytes, as well as platelets, using the centrifugation protocol.
PRF-matrix cultivation
After the centrifugation process, two layers can be observed inside the tubes: the red blood cells at the bottom and the liquid PRF at the top (Fig. 2a–c). From each tube, the total volume of i-PRF was collected, and 200 μL was then added to 24-well cell culture plates (CELLSTAR®; Greiner Bio-one) and incubated at 37°C for 1 h until clotting was complete. Afterward, 400 μL Roswell Park Memorial Institute medium supplemented with 1% penicillin/streptomycin (Biochrom GmbH, Berlin, Germany) was added per well and further incubated at 37°C. Subsequently, the supernatants were collected after 1, 2, 7, and 10 days and frozen at −80°C for GF analysis and replaced with fresh medium.

The rest of the i-PRF samples were incubated until clotting was complete and further processed for histological analysis.
Enzyme-linked immunosorbent assay
A quantification of the content of GFs within the i-PRF matrices was performed using quantitative sandwich enzyme-linked immunosorbent assay (ELISA) kits (Quantikine® ELISA; R&D Systems, Minneapolis, MN) according to the manufacturer's instructions. The quantified proteins were vascular endothelial growth factor (VEGF), TGF-β1, and platelet-derived growth factor-BB (PDGF-BB). The absorbance assay was conducted using a microplate reader (Infinite® M200; Tecan, Grödig, Austria) set to a wavelength of 450 nanometers with a reference reading at 570 nm. The output data were analyzed using a four-parameter logistic curve fit and presented graphically using GraphPad Prism version 7.0 (GraphPad Software, Inc., La Jolla). The experiments were performed in triplicate for each i-PRF sample.
Tissue processing and histological preparation
The clotted i-PRF matrices were fixed in 4% buffered formalin (Roti-Histofix 4% acid-free pH 7; Carl-Roth, Germany) for 24 h, processed using a tissue processor (Leica TP1020) as previously described, 20 and embedded in paraffin. Eight samples per centrifugation protocol were analyzed. Three sections per sample were cut using a rotary microtome (Leica RM 2255, Wetzlar, Germany) to obtain slices of 2–3 μm thickness as previously described.21,22 For immunohistochemical and immunohistological staining, the sections were deparaffinized using a series of decreasing concentrations of xylene and rehydrated using alcohol in increasing concentrations. The slices were then stained for hematoxylin and eosin, anti-CD-61 (platelets), and anti-CD-45 (leukocytes).
Standardized immunohistochemical staining was performed according to standardized methods as previously described.7,23 After deparaffinization and rehydration, the antigen was retrieved by the heat-induced epitope retrieval method using pH 6 citrate buffer at 95°C for 20 min. An autostainer (Lab Vision™ Autostainer 360; Thermo Scientific) was used for further staining procedure. The autostainer was loaded with a suitable solution and antibody concentrations (CD-61 1:2000 [ab225742] and CD-45 1:50 [ab10558]). Finally, anti-mouse secondary antibody was used (HRP UltraVision Quanto Detection System; Thermo Fisher Scientific), and chromogenic visualization was achieved using AEC peroxidase (Dako). The slides were then counterstained with hemalum for 30 s, washed with water, and covered with Aquatex® (Merck Millipore, Darmstadt, Germany).
Histological evaluation
Qualitative histological analysis was performed by three of the authors independently (S.G., S.A.-M., and C.H.-V.), and the slides were blinded. The analysis was performed using a light microscope (Nikon Eclipse 80i; Nikon, Tokyo, Japan) equipped with a Nikon DS-Fi1 digital camera and a Nikon Digital sight unit DS-U3 (Nikon) to capture representative histomicrographs.
Statistical evaluation
The quantitative data were analyzed and illustrated using the graphing and statistics software GraphPad Prism 7 (GraphPad Software, Inc.). The values were expressed as the mean ± standard deviation. Statistical analysis was performed using one-way (automated cell count) and two-way (GF release) analysis of variance with a Tukey multiple comparisons test (α = 0.05). The values were considered significant at *p < 0.05 and highly significant at **p < 0.01, ***p < 0.001, and ****p < 0.0001.
Results
Quality and volume of i-PRF matrices
Median sternotomy and rapid blood collection were achieved in all the animals. From each animal, a volume of 6 mL was collected within 30–40 s, which allowed the complete filling of two small i-PRF tubes.
Immediately after centrifugation, the quality of the obtained i-PRF was evaluated. All centrifuged blood samples were in liquid condition directly after centrifugation (Fig. 2a, b) and clotted within 15 min after transfer to the 24-well cell culture plate and incubated at 37°C.
The volume of the obtained i-PRF varied according to the applied centrifugation protocol. In the protocol of high RCF, the highest volume of i-PRF was 1000 ± 97 μL, followed by those of medium RCF (870 ± 60 μL) and low RCF (260 ± 50 μL) (Fig. 2c).
Numbers of leukocytes, platelets, and lymphocytes
The number of cells within the differently centrifuged i-PRF matrices showed significant differences.
Platelets were lowest in high-RCF PRF. Medium-RCF PRF exhibited a significantly higher concentration of platelets compared to that of high-RCF PRF (**p < 0.01). Furthermore, low-RCF PRF showed the highest concentration of platelets among all evaluated protocols, which was significantly higher compared with high-RCF (**p < 0.01), whereas no statistically significant difference was shown compared to medium-RCF PRF (Fig. 3a).

Automated cell count
A similar pattern was observed for the numbers of leukocytes within the evaluated groups. In this case, high-RCF PRF again showed a significantly low number of leukocytes compared to those of medium-RCF PRF (**p < 0.01) and low-RCF PRF (**p < 0.01). Low-RCF PRF included a significantly high number of leukocytes compared to medium-RCF PRF (*p < 0.05) (Fig. 3b).
The number of lymphocytes within the evaluated i-PRF matrices resulted in a similar pattern. High-RCF PRF showed a significantly low number of lymphocytes compared to those of medium-RCF PRF (*p < 0.05) and low-RCF PRF (***p < 0.001). In addition, low-RCF PRF showed a significantly high number of lymphocytes compared to that of medium-RCF PRF (*p < 0.05) (Fig. 3c).
Cellular distribution
The histological analysis using hematoxylin and eosin confirms the observations during direct cell counting in liquid culture, that is, an inverse correlation between cell concentrations and the applied RCF. The cell number increased as the applied RCF was decreased (Fig. 4).
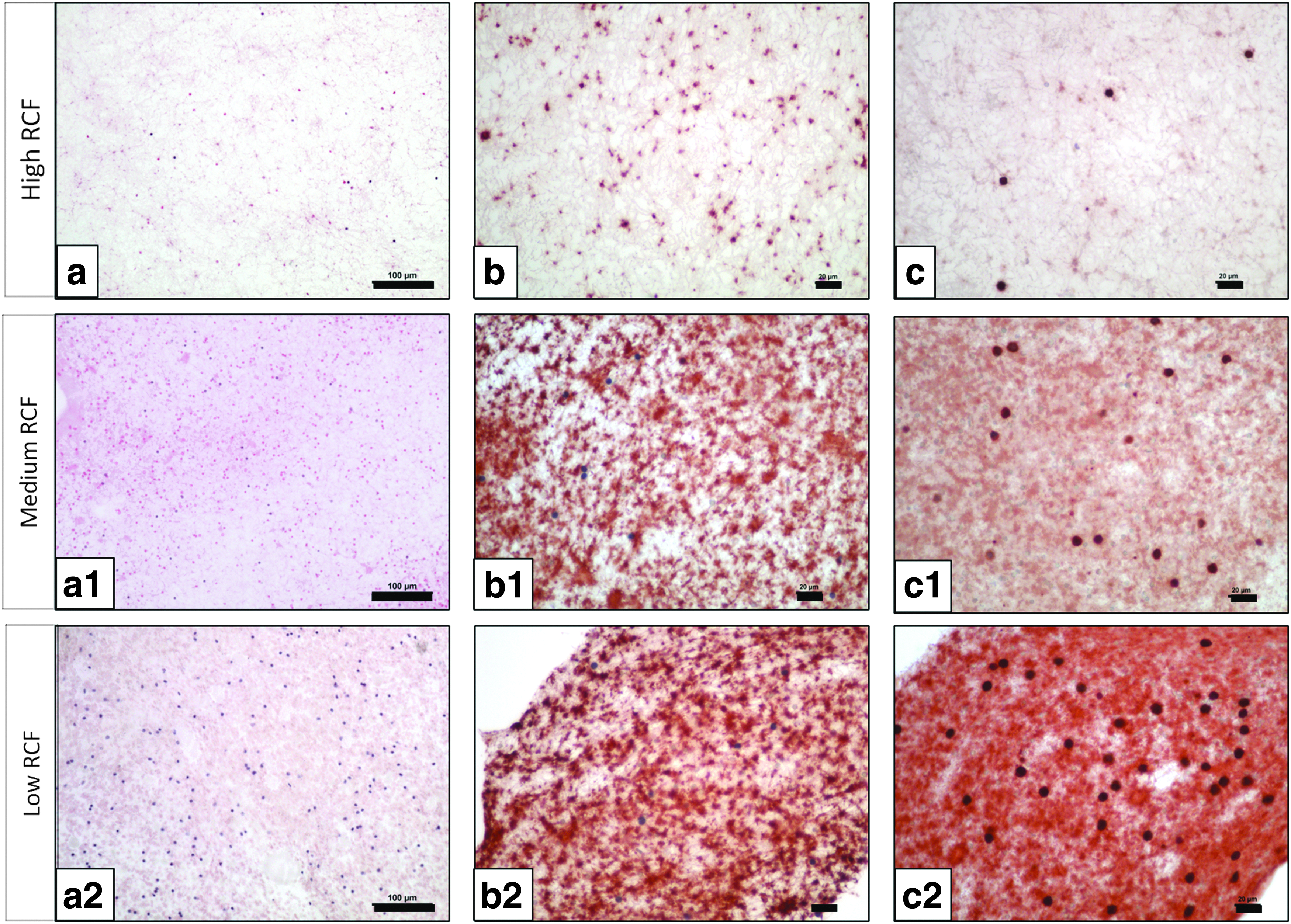
Histological analysis of the differently prepared i-PRF matrices showing the cellular distributions of platelets and leukocytes.
To specify the types of cells, immunohistochemical analysis was performed to mark the platelets (CD-61) and leukocytes (CD-45). The analysis showed that, in each sample, more platelets than leukocytes were positively stained. However, when comparing the differently prepared i-PRF groups focusing on one cell marker, obvious differences could be identified. The largest number of platelets (CD-61-positive cells) was observed in low-RCF PRF, followed by medium-RCF PRF and high-RCF PRF (Fig. 4).
The distribution of positively stained leukocytes (CD-45-positive cells) showed a clear trend. Only some sporadically distributed leukocytes could be identified in the group of high-RCF PRF, whereas in the group of medium-RCF PRF, more leukocytes were observed throughout the evaluated samples. Low-RCF PRF showed the highest number of positively stained leukocytes compared to those of the other two groups. These cells were evenly distributed throughout the samples and easily identifiable (Fig. 4).
Bioactivity and GF release
Three different GFs were analyzed in the evaluated i-PRF groups as follows: VEGF, TGF-β1, and PDGF-BB. The GF concentrations were analyzed at each time point and collectively as accumulated release over 10 days.
Vascular endothelial GF
A general trend was detected over 10 days, showing that reducing the applied RCF in the i-PRF matrices leads to enhanced VEGF release.
On day 1, a significantly higher VEGF concentration was released by low-RCF PRF compared to those of medium-RCF PRF (*p < 0.05) and high-RCF PRF (***p < 0.001). No statistically significant difference was detected between high-RCF PRF and medium-RCF PRF at this time point. After 2 days of cultivation, VEGF concentration in the medium-RCF PRF was higher than those of high-RCF PRF. However, no statistically significant difference was observed at this time point. Toward day 7, a clear trend was observed between the evaluated groups. In this case, low-RCF PRF released significantly more VEGF compared to medium-RCF PRF (***p < 0.001) and high-RCF PRF (***p < 0.001), whereas no statistically significant difference was detected between high-RCF PRF and medium-RCF PRF. On day 10, a similar trend was observed, but no statistically significant difference was detected (Fig. 5a).
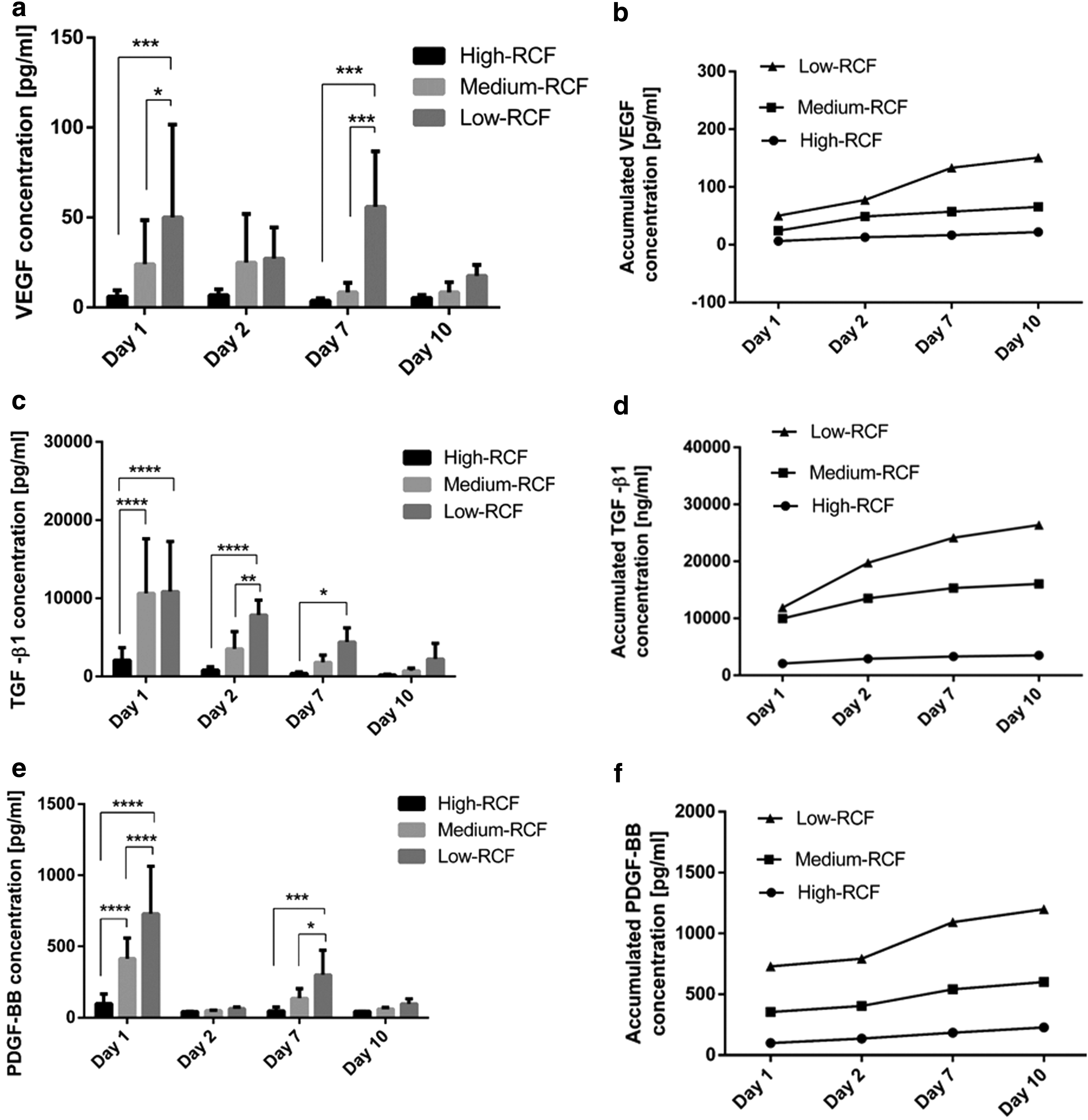
The accumulated VEGF release showed continuous and increasing release over 10 days. On day 10, the accumulated VEGF released from low-RCF PRF was significantly higher compared to those of medium-RCF PRF (**p < 0.01) and high-RCF PRF (***p < 0.001). However, no statistically significant difference was detected between high-RCF PRF and medium-RCF PRF (Fig. 5b).
Transforming GF beta-1
The highest release of TGF-β1 in all evaluated groups was detected after 1 day. At this time point, both medium-RCF PRF and low-RCF PRF showed comparable concentrations that were significantly higher than those of high-RCF PRF (****p < 0.0001 for both). After 2 days, an obvious trend was detected when comparing the differently prepared i-PRF matrices, in which low-RCF PRF released significantly more TGF-β1 compared to medium-RCF PRF (**p < 0.01) and high-RCF PRF (****p < 0.0001). No statistically significant difference was detected when comparing medium-RCF PRF and high-RCF PRF. On day 7, a trend similar to that of the previous two time points was observed. In this case, low-RCF PRF released significantly more TGF-β1 compared to high-RCF PRF (*p < 0.05). However, no statistically significant difference was found between high-RCF PRF and medium-RCF PRF or between medium-RCF PRF and low-RCF PRF. At the last observation time point, day 10, the same tendency was detected as that from the previous time points, but no statistically significant difference was detected (Fig. 5c).
The accumulated TGF-β1 release was continuous over 10 days. All evaluated groups showed increasing TGF-β1 release over the observation time. On day 10, the accumulated TGF-β1 release was significantly higher in low-RCF PRF compared to that in medium-RCF PRF and high-RCF PRF (***p < 0.001). In addition, medium-RCF PRF (***p < 0.001) showed significantly higher accumulated TGF-β1 compared to high-RCF PRF (**p < 0.01) (Fig. 5d).
Platelet-derived GF-BB
PDGF-BB was measurable at all evaluated time points. The release profile showed the highest concentration on day 1 in all investigated groups. After 1 day, low-RCF PRF released significantly more PDGF-BB compared to medium-RCF PRF (****p < 0.0001) and high-RCF PRF (****p < 0.0001). In addition, medium-RCF PRF released significantly more PDGF-BB compared to high-RCF PRF (****p < 0.0001). After 2 days, no statistically significant difference was measured between the evaluated groups. However, toward day 7, again an obvious difference was observed in which low-RCF PRF released a significantly higher concentration compared to those of medium-RCF PRF (*p < 0.05) and high-RCF PRF (***p < 0.001). No statistically significant difference was detected between high-RCF PRF and medium-RCF PRF. On day 10, a similar tendency was observed as the previous time point, although the apparent differences did not reach statistical significance (Fig. 5e).
The accumulated PDGF-BB release showed continuous and increasing values over 10 days in all evaluated groups. On day 10, the measured accumulated PDGF-BB released from low-RCF PRF was significantly higher than those of medium-RCF PRF (***p < 0.001) and high-RCF PRF (***p < 0.001). In addition, medium-RCF PRF showed significantly higher accumulated PDGF-BB release compared to high-RCF PRF (*p < 0.05) (Fig. 5f).
Discussion
In recent decades, blood concentrates gained tremendous momentum in regenerative medicine, which opened new avenues not only for clinical research but also for preclinical and basic science research.24–26 Blood concentrates, such as PRF, are highly complex systems consisting of different GFs, plasma proteins, blood cells, and their subgroups. 6 To begin to understand the molecular mechanisms of regeneration in these systems, extensive research is needed using systematic approaches, standardized models, and reproducible methods. In this context, different attempts have been conducted to produce PRF from small research animals and have faced great difficulties because of the limited blood volume in small animals and the technical limitations of the existing equipment, which was originally designed for clinical use in humans. 27
Although some studies used Wistar rats or rabbits as a model to investigate the regeneration capacity of PRF, these studies were not able to follow the original human PRF protocol in the preparation of their samples and, therefore, used modified techniques that deviated from the standards.28–30 Consequently, intense discussions in the literature have questioned the comparability of the pharmacological quality of the obtained PRF matrices as to whether it is adequate to consider these modified protocols for research and how to interpret their results, making their translation to clinical application even more complicated. 27 An alternative that has been considered in the in vivo research of blood concentrates is the use of SCID mice in combination with human samples. This model is relevant to show the potential impact of blood concentrates in the regeneration process, but cannot mimic the real clinical situation in terms of autologous regenerative capacity because it cannot assess contributions of the immune system, as well as it can only detect therapeutic contributions of species cross-reactive mediators. 31
Indeed, the use of large animals, such as dog, sheep, swine, goat, or cow, is more suitable for this approach. However, there are many limitations when considering large animals in research compared to small animals. Not only do their availability, requirement for special housing facilities, and financial issues need to be taken into account but also ethical issues. 32 Considering the standards of a successful translation study series, large animals should be used to fill the gap in the translational biomedical research from rodents to human. Therefore, it is generally accepted that the most suitable large animal models should be used to achieve specific research aims and not as a replacement for small animals. 33 In addition, there is a shortage of validated large animal models in the field of regenerative medicine, as well as validated tests and reagents, for tissue evaluation and immunobiology. 33
Therefore, the present study was designed to investigate, for the first time, whether it is possible to produce adequately prepared PRF matrices of similar quality as those of human donors, except using small blood volumes and rodent blood as a first step toward reducing the initial blood volume and establishing the PRF preparation protocols for human and preclinical in vitro and in vivo research involving small animal (murine) models.
In the present study, methodological challenges were taken into consideration with the aim to use small research animals (Wistar rats of ca. 200 g in weight) that are widely available and established in many countries. For the purpose of these studies, small PRF collection tubes were produced specially for this study. As a first step, the initial blood volume used in clinical application (10 mL) was reduced by more than threefold to 3 mL. This step was thoroughly considered for the minimum blood volume needed to obtain a sufficient amount of PRF from the obtained blood sample according to the hematologic references of rodents in terms of available volume,34,35 hematocrit,36,37 and coagulation time. 38 Moreover, the requirements for the preparation of PRF without anticoagulants presuppose rapid blood collection to assure a homogenous and uncoagulated whole blood sample before centrifugation. Different well-established methods have been used for blood sampling from small animals that are either performed in the conscious animal or when under anesthesia. 34
Rat peripheral blood can be obtained from different anatomical locations, including the tail vein, facial vein, saphenous vein, and femoral vein. These procedures are not very harmful to the animals and are therefore considered survival procedures with relatively safe recovery.16,34 Among the recommendations to be followed for the collection of blood in animals, the maximum amount withdrawn is one of the main factors for animal health maintenance. For studies in rats, the collection of up to 10% of the circulating blood volume is recommended, which should not exceed the value of 30% for animals at risk of hypovolemia. 39 The “good practices” in the management and removal of blood suggest 7 days as the time required to recover the 10% loss in blood volume. 39 Considering the body weight of widely used mice and rats, this blood volume is still not enough for the production of PRF. In addition, the anatomy of their veins shows small lumina and a fragile structure, making their capacity of collection limited to a very small amount of blood. Furthermore, blood flow from these vessels is very slow and requires a long time to collect the blood sample, and so the blood will likely start to coagulate during the sampling procedure. 16 Therefore, these techniques are not suitable for the preparation of blood concentrates, specially PRF that is prepared without additional anticoagulants.
In contrast, nonsurvival techniques, such as blood collection from the vena cava or the cardiac puncture technique, are considered terminal interventions that allow rapid collection of a large blood volume, 39 making them relevant for the preparation of PRF. In the present study, the cardiac puncture technique was implemented after median sternotomy to collect the blood from the right heart atrium in a short time. This technique allowed direct vision of the heart and avoided multiple heart punctures. The collection of blood accumulated in the thoracic cavity after injuring the heart and not direct from the heart atrium would provide blood that already initiated the coagulation process. In this case, the animals were sacrificed for use in research in terms of organ harvesting (i.e., blood), which is in consent with the standard ethical principles and guidelines for the use of animals in research. 40 Animal tissue and organs have been used for the development of several in vitro models and methods.41–43 In this context, some studies have investigated the impact of blood concentrates in vitro using animal cell cultures and human PRF. 44 In this case, serious concerns have to be taken into account as to whether the combination of samples from two different species is appropriate to investigate the regenerative capacity of the system or whether side effects, such as xenoimmunity or graft-versus-host reactions, may interfere with the results. 27
Even when using primary human cells, such as osteoblasts or endothelial cells, it is rare to obtain tissue samples for cell isolation and blood samples for PRF preparation from the same donor. 11 Therefore, cells and blood of different donors have been combined in a complex in vitro system to investigate the role of blood concentrates. 11 These limitations are being discussed in the literature, and the used methods are modified to mostly avoid potential influence or adverse reactions resulting from the combination of different donors or species. In an in vitro work, the impact of PRF on the regenerative capacity of human mesenchymal stem cells was investigated. 45 However, due to the limitation of donors for PRF and stem cells, the authors decided to filter the i-PRF matrices to exclude the leukocytes and thus avoid any potential cell–cell communication in the samples from different donors. 45 However, in this case, again this modification leads to a great limitation, and the experimental conditions are thus not able to mimic the clinical situation. In addition, when using human blood samples for the preparation of PRF, a large variety is found in the quality of the donated blood, which depends on a myriad of factors, such as general health condition, habits, diet, and fitness. This variety requires a large number of donors and experiments to reach statistically relevant results. All these aspects call for new perspectives to optimize the methods used in the research field of regenerative medicine and blood concentrates. A different situation is found in animals, as all animals used for research purposes are housed and fed under controlled and standard conditions, which is most likely a positive factor in terms of reproducibility and control of variability in the evaluated samples.
The volume of i-PRF is prescribed by the interface between the red blood phase and the i-PRF phase. Therefore, the observed results are most likely related to the fact that a high RCF leads to a higher acceleration of the cellular components, especially red blood cells, toward the bottom of the tube than a low RCF would. The result is a higher volume of red blood cell-“free” concentrate, which is considered i-PRF, generated in the high RCF range and vice versa. Accordingly, the volumes of the obtained i-PRF are also influenced by the centrifugation protocol.
In general, the results of cellular analysis showed that the obtained i-PRF matrices in all RCF ranges (high, medium, and low) included platelets, leukocytes, and lymphocytes in different concentrations. This finding proves that the i-PRF matrices generated from rat blood exhibit similar cellular components as those in i-PRF matrices produced using human blood.6,7 In addition to the i-PRF volume, the cellular components of the resulting i-PRF matrices were directly influenced by the use of different RCF values. RCF inversely correlated with the recovered concentration of platelets, leukocytes, and lymphocytes. These data are in accordance with the previously described characterization of i-PRF matrices that were established using human blood.6,7 Therefore, the present study showed for the first time that it is possible to produce PRF matrices with similar characteristics to human PRF using rodent blood by respecting the preparation protocol and using the appropriate technique and equipment.
Moreover, the bioactivity of the produced i-PRF matrices was evaluated over 10 days. In this context, the release of three GFs (VEGF, TGF-β1, and PDGF-BB) was quantified at four different time points. When comparing the three evaluated groups, different concentrations of GFs were released according to the applied centrifugation protocol. The accumulated concentrations of VEGF, TGF-β1, and PDGF-BB over 10 days were significantly higher in i-PRF matrices prepared using a low RCF compared to those in i-PRF matrices prepared using a high or medium RCF. Except for VEGF, no statistically significant difference was shown between high RCF and medium RCF in the accumulated concentrations of the GFs over 10 days. However, in all evaluated GFs and time points, a clear trend was shown in that the reduction in the applied RCF correlated directly with the concentration of the released GF, showing that reducing the applied RCF enhances the bioactivity of the i-PRF matrices. These results are in harmony with the previous findings of i-PRF matrices produced using human blood.6,7 In this context, the results of this study showed great similarity in the composition and bioactivity of the i-PRF matrices produced using rat blood and human blood, which validate the introduced method for i-PRF preparation using rat blood. One limitation of the present study has to be stated at this point, the here introduced results cannot prove that the 3 mL PRF obtained by different centrifugation speeds has the same therapeutic effect as standard isolation procedures. Therefore, further studies are ongoing to address this aspect.
Altogether, the data presented in this study are in accordance with the previously described LSCC, which was first established using human blood.6,7 Therefore, the results of the present study can serve as a proof of concept of the LSCC in another species, that is, rats.
For the implementation of PRF matrices produced using animal blood in vivo, the main aim of the present study was the reduction in the initial blood volume needed for the preparation of PRF matrices. 2 Therefore, reducing the initial blood volume by more than threefold (i.e., from 10 to 3 mL) and developing small PRF tubes with the same characteristics as those of the clinically used tubes for animal research provide many possibilities to use small animals for PRF research.
Considering small rats, a limitation of the present study has to be addressed. The method presented in this study for blood collection, that is, cardiac puncture, is a nonsurvival method, making the implementation of this method for PRF as an autologous material in the in vivo research of small rats more complicated. However, it may be possible to use PRF matrices from the same strain of the animal for the donor and recipient, as PRF is used locally and not systematically and is therefore not comparable to blood transfusion or organ transplants that may cause considerable immunologic reactions in the recipient. This method may be relevant for both inbred and outbred strains. This suggestion is supported by an in vivo study that showed successful regenerative results by the transplantation of rat adipose-derived stromal cells for periodontal regeneration without any adverse reactions in both inbred and outbred rat strains. 46 However, establishing such model first requires sufficient validation to be considered for this type of research. Alternatively, the possibility presented here to use small PRF tubes may allow adequate preparation of PRF using different animal models that are considered small animals, such as larger Sprague Dawley rats or rabbits, and peripheral blood from a different access than that presented here in a survival procedure, such as blood sampling from the ear vein or tail vein. Therefore, ongoing studies of our group are evaluating different possibilities to implement this technique for the validation of an in vivo model in small animals to fill a methodological gap in translational regenerative medicine with regard to blood concentrates.
Conclusions
The present study evaluated different preparation protocols of PRF from small animal blood. The composition and bioactivity of the produced PRF were thoroughly investigated using automated cell count histology and protein quantification. The results showed for the first time that it is possible to produce adequately prepared PRF matrices using a small initial blood volume of 3 mL by otherwise following the standard protocol of PRF preparation but using small tubes with otherwise identical characteristics as those used clinically. The number of leukocytes, platelets, and lymphocytes within the i-PRF matrices increased significantly along with the reduction in the applied, that is, was inversely correlated with the applied RCF. While continuous release of different GFs (VEGF, TGF-β1, and PDGF-BB) was observed for at least 10 days in all evaluated i-PRF matrices, the use of a low-RCF promoted a significant increase in the release of GFs. These data are in accordance with the previously described low speed centrifugation concept, which was established using human blood and may, therefore, serve as a proof of concept in another species, that is, rats. The method presented in this study provides many possibilities for the implementation of PRF as an autologous system in both in vitro and in vivo research to further understand the mechanisms of regeneration using blood concentrates such as PRF. However, further studies are needed to proof the therapeutic effect of PRF prepared using animal blood.
Footnotes
Acknowledgment
The authors thank Mrs. Verena Hoffman for the excellent technical assistance.
Disclosure Statement
The authors declare that they have no conflict of interest. J.C. is the owner of PROCESS.