
Abstract
There have been many advances in tissue engineering with respect to in vitro and in vivo models of oral mucosa equivalents (OMEs). To apply in vitro reconstructed oral mucosa models to regenerative medicine and alternatives to animal testing, it is necessary to develop the technology of reconstructing different types of oral tissues, such as control of epithelial differentiation and introduction of appendages. We previously reported that functional three-dimensional (3D) tissue models could be quickly constructed by using a layer-by-layer (LbL) cell coating technique that assembles extracellular matrix (ECM) nanofilms to a cell surface. In this study, 3D human OMEs composed of lamina-propria, keratinized or non-keratinized epithelium, and blood capillaries were constructed by using the LbL cell coating technology. Human oral mucosal fibroblasts (HOMFs) were coated with ECM nanofilms and accumulated for the construction of oral mucosal lamina-propria. To construct OMEs with keratinized or non-keratinized epithelium, human oral keratinocytes isolated from gingiva (human oral gingival keratinocytes: HOGKs) or human oral keratinocytes isolated from oral mucosa (human oral mucosal keratinocytes: HOMKs) were used in this study. We further studied the construction of epithelialized OMEs with density- and size-controlled blood capillary networks by using human umbilical vein endothelial cells (HUVECs). It was revealed that these constructions had barrier functions in accordance with their histological characterization. The OMEs with keratinization (K-OMEs) showed higher transepithelial electrical resistance (TEER) values compared with OMEs with non-keratinization (N-OMEs). The constructed epithelialized OMEs with blood capillaries are useful for in vitro/ex vivo research models and regenerative medicine as in oral tissue regeneration. The results suggest that OMEs with oral tissue appendages are more promising alternatives to animal testing and can be applied to the design of in vitro oral models that mimic human tissue organs.
Impact Statement
Three-dimensional (3D) tissue models of the human oral mucosa have been advanced in recent years. In this study, we prepared 3D human oral mucosa equivalents (OMEs) by using our developed cell coating technique, which employs cell surface coating by layer-by-layer assembled extracellular matrix films. The different keratinized types of OMEs were established, and the blood capillaries were successfully incorporated into the lamina-propria part of the OMEs. The results suggest that OMEs allowing incorporation of oral tissue appendages are more promising alternatives to animal testing, and they can be applied to regenerative medicines as oral mucosa tissue regeneration.
Introduction
The study regarding tissue engineering of human three-dimensional (3D) tissue constructs has progressed and these 3D tissue models have become a useful and versatile tool in both academia and industry. In the past decade, 3D reconstruction of various human tissues using primary cells or induced pluripotent stem (iPS) cell technology was led by advances in the tissue engineering field. In recent years, a large body of research has focused on the construction of more complex tissue-engineered organs with improved functionality, biological properties, viability, and survival for clinical transplantation and substitution of damaged or lost parts of a living body. In addition to the clinical applications, 3D models of various human tissue types have also been developed for in vitro applications as alternatives to animal testing. They can be used to evaluate the biological response of living tissues. Moreover, by constructing diseased organs such as 3D cancer models or tissue infection models, it can be possible to examine the mechanisms of disease initiation and progression and to evaluate the treatment effects of developed drugs.1–3
Oral mucosa provides barrier protection for the oral cavity. Tissue-engineered oral mucosa models have been developed for both in vitro and in vivo applications.4,5 Clinical applications, such as artificial dermis and absorbable suture reinforcement felts, have been developed and applied widely for the supplementation of mucosal defects. However, the main healing mechanism using these materials is scar healing, resulting in marked scar contracture at the recipient site tissue. Moreover, autologous transplantation, which is another method of grafting, requires the sacrifice of donor site tissue. At present, for clinical applications, intra-/extra-oral grafting of reconstructed oral mucosa models has been used to replace the lost mucosal soft tissues with successful outcomes.6–8 Reports on in vitro applications, such as oral biocompatibility testing, dental material testing,9–11 oral disease models,12–14 and the development of novel drug delivery systems 15 using reconstructed oral mucosa models, have been extensively published in the literature. For these applications, research on tissue engineering of various types of oral mucosa models has also progressed and the technologies of reconstruction are currently being established.4,5 The reconstructed oral mucosa models can be divided into two classes, one consisting of only differentiated oral epithelium (epithelial substitutes), 16 and the other additionally consisting of lamina-propria comprising oral fibroblasts embedded in scaffolds, such as collagen gels (full-thickness oral mucosa substitutes). 17 It is, however, necessary to improve the existing 3D oral mucosal models for use as academic or industrial tools, including applications in regenerative medicine and alternatives to animal testing. To prepare 3D oral mucosa models that better imitate biological human oral tissues, the technology of reconstructing different types of oral and dental soft/hard tissues, control of keratinization, differentiation, and morphology, or introduction of appendages, will require further development.18,19 In particular, vascularization is critical in tissue engineering, because blood vessels are needed to supply nutrients and oxygen to maintain the tissue. However, there are currently no conventional technologies to generate oral mucosal equivalents with blood capillaries.
Various techniques for the fabrication of 3D tissues have recently been reported, including multilayer scaffolds, 20 cell sheet engineering, 21 and 3D bio-printing technologies.22,23 Although these techniques are able to fabricate cells into 3D constructs, they have restrictions due to the difficulties in handling the fragile cell sheet or residual scaffolds in the constructs. Moreover, it is difficult to regulate the thickness and components of an extracellular matrix (ECM), which is an important factor for controlling tissue function in constructed tissues.
We have recently reported on a bottom-up approach for 3D reconstructed tissues, called the cell accumulation technique. This uses a novel cell coating technique that we developed based on the concept of layer-by-layer (LbL) assembly to efficiently create in vitro 3D tissue models. The cell coating technique is able to form nanofilms consisting of ECM proteins, such as fibronectin (FN) and gelatin (G), on the cell surfaces.24,25 The FN with RGD sequence and collagen-binding domain can bind to integrin α5β1 on a cell surface and G. By repeating the LbL cell coating with FN and G, FN-G nanofilms as a molecular glue to promote cell-cell binding are formed on the cell surfaces.
We previously reported that the LbL FN-G cell coating technique makes it possible to quickly construct functional 3D tissue models. Using this technique, we constructed 3D models of human tissue; skin models, 26 liver models, 27 myocardial models, 28 peritoneal models, 29 and islet models. 30 This technique has a wide range of applications, with the potential to be used for several other 3D tissue models. Moreover, when normal human dermal fibroblasts (NHDFs) are coated with FN-G nanofilms and combined with human umbilical vein endothelial cells (HUVECs), a 3D structure possessing a dense vascular network can be formed. The blood capillaries that are constructed using the cell coating technique are morphologically similar to native vessels. 25 Using the base technique, we developed full-thickness human dermo-epidermis skin equivalents (DESEs) with density-controlled blood capillaries. 31 The skin models are more promising alternatives to animal testing and can be applied to the design of physiologically relevant in vitro skin models. 32
In this study, 3D human oral mucosa equivalents (OMEs) composed of lamina-propria, epithelium, and blood capillaries were constructed by using the cell coating technology. The construction of OMEs was based on technology previously developed by our group for the production of DESEs.26,31 Oral mucosa has a stratified epithelium that is either keratinized or non-keratinized depending on its location in the oral cavity. Therefore, it is important to control the keratinization of the epithelium to mimic native oral mucosa. Human oral mucosal fibroblasts (HOMFs) were coated by FN-G nanofilms and accumulated for construction of oral mucosal lamina-propria equivalents. To construct OMEs with keratinized or non-keratinized epithelium, human oral keratinocytes isolated from gingiva (human oral gingival keratinocytes: HOGKs) or human oral keratinocytes isolated from oral mucosa (human oral mucosal keratinocytes: HOMKs) were used in this study. We further studied the construction of OMEs with density- and size-controlled blood capillaries using HUVECs. The tissue engineering of blood capillaries not only yields valuable in vitro/ex vivo research models but is also useful for regenerative medicine as in oral tissue regeneration.
Materials and Methods
Cell culture
Human oral mucosal fibroblasts from adult oral gingiva (HOMFs; Cell Research Corporation, Singapore) (passage was <7) and normal human dermal fibroblasts from neonatal tissue (NHDFs; Lonza, Basel, Switzerland) (passage was <7) were cultured in Dulbecco's modified Eagle's medium (DMEM; Wako Pure Chemical Industries, Osaka, Japan) containing 10% fetal bovine serum (FBS; Life Technologies, Carlsbad, CA), 100 U/mL penicillin, 100 μg/mL streptomycin, and 0.25 μg/mL amphotericin B. HUVECs (Lonza) (passage was <6) were cultured in endothelial growth medium (EGM™-2MV) BulletKit™ Medium (Lonza). These fibroblasts and HUVECs were maintained in 5% CO2 at 37°C and subcultured with 0.05% trypsin +0.02% EDTA in phosphate-buffered saline (PBS; Wako Pure Chemical Industries). Human oral gingival keratinocytes from adult oral gingiva (HOGKs; Cell Research Corporation) (passage was <5), human oral mucosal keratinocytes from adult oral mucosa (HOMKs; ScienCell Research Laboratories, Carlsbad, CA) (passage was <5), and human skin epidermal keratinocytes from neonatal tissue (HSEKs; KURABO, Osaka, Japan) (passage was <3)were cultured in Epilife® Medium with 60 μM calcium (Life Technologies) supplemented with HuMedia-KG growth factor (KURABO) and subcultured with pronase (KYOKUTO, Tokyo, Japan).
Construction of lamina-propria equivalents using HOMFs with LbL FN-G cell coating technique
As shown in our previous reports, 25 HOMFs were coated with fibronectin (FN; Sigma-Aldrich, MO) and gelatin (G; Wako Pure Chemical Industries) by a centrifuge-based LbL FN-G cell coating technique (Fig. 1a). HOMFs were suspended with 0.04 mg/mL FN and G in PBS, and they were alternately incubated for 1 min. After each process, PBS was added to the cells and unabsorbed proteins were removed by centrifugation at 800 g for 1 min. After nine steps of immersion, single-cell surfaces were covered with FN-G nanofilms. LbL cell-coated HOMFs (1 × 10 6 cells/300 μL) were seeded into the 24-well transwell cell culture insert (culture area 0.33 cm 2 ) with a 0.4-μm pore polyester membrane (Corning, NY; Cat. No. 3470) coated with an FN monolayer. Two milliliters of DMEM with 10% FBS was added into the 24-well plate (out of the culture insert), and the cells were then incubated in 5% CO2 at 37°C. After 1 day of incubation, thick tissues consisting of HOMFs multilayers were prepared on the insert membrane. These tissues as lamina-propria equivalents were used for further experiments. Rhodamine-labeled FN (Rh-FN) and fluorescein-labeled G (FITC-G) were used to confirm that ECM proteins were coated onto the cell surface. After the LbL FN-G cell coating process, the cells were observed with a confocal laser scanning microscope (CLSM) (FV10i; Olympus).

Oral lamina-propria equivalents were constructed by using a LbL cell coating technique and compared with the LbL-uncoated tissues.
Measuring the thickness and porosity of the lamina-propria equivalents
To assess the effect of the LbL technique for 3D tissue construction, the thickness and porosity of tissues using either LbL cell-coated [LbL(+)] HOMFs or -uncoated [LbL(−)] ones were compared. LbL(−) HOMFs were prepared by the nine steps of immersion in PBS (without FN or G). The thickness of the tissues was measured in Mayer's hematoxylin (MUTO PURE CHEMICALS Co., Ltd, Tokyo, Japan) and eosin (Sakura Finetek Japan Co., Ltd, Tokyo, Japan) (HE)-stained cross-sectional images at five points in four arbitrarily selected representative samples.
In the lamina-propria equivalents constructed using LbL cell-coated HOMFs only, the porosity of the tissue was also calculated by using the following equation:
P (%) = I/T × 100 (P: the porosity of the tissue area, T: the total area of the tissue, and I: the intercellular space area as measured by ImageJ 1.50i software) (National Institutes of Health) (Supplementary Fig. S1a).
Construction of epithelialized OMEs with keratinization or non-keratinization
The epithelia were constructed on the surface of the obtained HOMF lamina-propria equivalents (Supplementary Fig. S2). To enhance adhesion of keratinocytes, the outer layer of the HOMF lamina-propria equivalents was coated with collagen type IV (Col IV; Sigma-Aldrich) by addition of 100 μL of 0.2 mg/mL in PBS for 30 min. HOGKs or HOMKs (1, 3, or 6 × 10 5 cells/300 μL) were then seeded onto the surface of the HOMF lamina-propria equivalents, and 2 mL of DMEM/EpiLife mixed medium (1:1 v/v) was added into the 24-well plate (out of the culture insert). After 1 day of incubation, the HOMFs-HOGKs or HOMFs-HOMKs constructs were lifted to the air-liquid interface. The entire medium of inner and outer culture inserts was removed; then, 500 μL of cornification medium (DMEM/EpiLife mixed medium (1:1 v/v) supplemented with 25 μg/mL ascorbic acid) was added into the 24-well plate (out of the culture insert) (air-lift culture); and the medium was changed every day. After 7 days of the air-lift culture, the epithelialized OMEs with keratinization (K-OMEs) composed of the HOMFs-HOGKs and non-keratinization (N-OMEs) composed of the HOMFs-HOMKs were fabricated.
Construction of epithelialized OMEs with blood capillaries
LbL FN-G cell-coated HOMFs (1 × 10 6 cells) and uncoated HUVECs (0.5, 1, or 2 × 10 5 cells) were mixed in seeding medium and placed on a culture insert precoated with FN. The tissues were cultured in the same way as the lamina-propria equivalents after seeding LbL cell-coated HOMFs and HUVECs. After 1 day incubation of lamina-propria equivalents with blood capillaries constructed with LbL cell-coated HOMFs and HUVECs, the epithelium was fabricated by using the same process (air-lift culture) as described earlier. After 7 days of incubation, OMEs with widespread and dense blood capillaries were fabricated (Supplementary Fig. S3). After construction of the OMEs, the HUVECs were immunofluorescence stained by using a mouse monoclonal anti-human CD31 primary antibody (Dako, Glostrup, Denmark), a goat anti-mouse IgG secondary antibody (Alexa Fluor 546 conjugate) (Life Technologies), and 4,6-diamidino-2-phenylindole dihydrochloride (DAPI; Life Technologies). Fluorescently stained vascularized OMEs were observed by using CLSM. For quantitative analysis of blood capillary formation in the OMEs, the covered percentage (%) area of the blood capillaries was measured by ImageJ 1.50i software (Supplementary Fig. S1b). In addition, the total tube length and number of branching points of blood capillaries were measured by AngioTool64 0.06a software (National Institutes of Health).
Histology and immunohistochemical staining
The lamina-propria equivalents, OMEs and our previously reported DESEs were fixed in 10% formalin solution (Wako Pure Chemical Industries) or 4% paraformaldehyde/phosphate buffer solution (Wako Pure Chemical Industries) and processed for paraffin embedment. After paraffin-embedded formalin-fixed tissues were sectioned at 4 μm, the sections were stained with HE or processed for immunohistochemistry (IHC) for examination for the tissue morphology, epithelial differentiation, and thickness change.
For IHC, the sections were deparaffinized, and the antigens were retrieved by using citrate buffer (pH 6), Tris-HCL buffer (pH 9), or Proteinase K (DAKO). Then, the sections were blocked with 3% hydrogen peroxide for 10 min at room temperature, blocked with 5% bovine serum albumin (BSA; Sigma-Aldrich) for 1 h at room temperature, and incubated with a primary antibody overnight at 4°C. The primary mouse monoclonal antibodies against human: anti-cytokeratin (CK) (AE1/AE3) (Dako), anti-cytokeratin 10 (CK10) (Thermo Fisher Scientific, Waltham, MA), anti-cytokeratin 13 (CK13) (Abcam, Cambridge, United Kingdom), anti-cytokeratin 14 (CK14) (Thermo Fisher Scientific), anti-E-cadherin (Dako), anti-Ki67 (Cell Signaling Technology, Danvers, MA), anti-collagen IV (Dako), anti-laminin (Leica Biosystems Newcastle Ltd., Newcastle upon Tyne, United Kingdom), and anti-CD31 were used to label OMEs and DESEs. After washing, the sections were incubated with a secondary antibody: EnVision System-HRP-labeled polymer anti-mouse IgG (DAKO) for 30 min at room temperature. Next, the sections were incubated with DAB substrate for 5 min followed by hematoxylin staining. The microscopic slides were visualized and recorded with EVOS® FL Auto Cell Imaging System (Life Technologies). In K-OMEs, the thickness of the cornified layer, that is the layers except those in the epithelium (granular layer, spinous layer, and basal layer) and lamina-propria equivalents were measured. In N-OMEs, the thickness of the epithelium and lamina-propria equivalents were measured.
Transepithelial electrical resistance profiles of OMEs
The transepithelial electrical resistance (TEER) values were measured during air-lift culture for 1 week by using Millicell ERS-2 (Millipore Co. Ltd.). Before measurements, the K-OMEs and N-OMEs were washed with PBS, and, subsequently, 1 mL and 300 μL of PBS were added to the outer and inner wells of the 24-well transwell cell culture insert. The TEER values were measured three times per sample, and average values (Ω × cm 2 ) were used.
Results and Discussion
Effects of LbL FN-G cell coating technique on structures of HOMF lamina-propria equivalents
First, to confirm whether ECM protein, FN, and G were coated on the cell surface by using the LbL cell coating technique, HOMFs were coated with fluorescein-labeled FN and G. After LbL cell coating, Rh-FN and FITC-G were observed on the surface of each cell, which was visualized in a merged CLSM image as a yellow ring (Fig. 1b). Next we investigated whether 3D tissue could be constructed by using cells treated with the LbL cell coating technique. As shown in Figure 1c, stratified HOMF lamina-propria equivalent was constructed after 1 day of incubation when 1 × 10 6 HOMFs treated by the LbL cell coating technique were added to a 0.33 cm 2 insert. Histological examination of the tissue constructed without LbL cell coating (LbL(−) tissue) revealed a more porous structure (Fig. 1c). The thickness of LbL(+) tissue was 46 ± 3 μm, and the porosity of LbL(+) tissue was 21% ± 3%. In contrast, the thickness of LbL(−) tissue was 113 ± 11 μm and the porosity of LbL(−) tissue was 48% ± 6%. The LbL(−) tissue was significantly thicker and more porous than the LbL(+) tissue (Fig. 1d, e). These results suggest that LbL(−) tissue was an insufficient fragile construct because of weak intercellular adhesions. By directly comparing LbL(+) and LbL(−) tissues, the utility of the LbL cell coating technique in tissue construction was demonstrated. From these results, it was suggested that intercellular adhesions of LbL cell-coated HOMFs were facilitated by coating FN-G nanofilms. We could confirm that the LbL cell coating technique was useful for generating 3D tissues. For the construction of 3D tissues using HOMFs, it was demonstrated that the LbL cell coating technique was as effective as our previous reports. 25
Construction of OMEs with keratinization (K-OMEs)
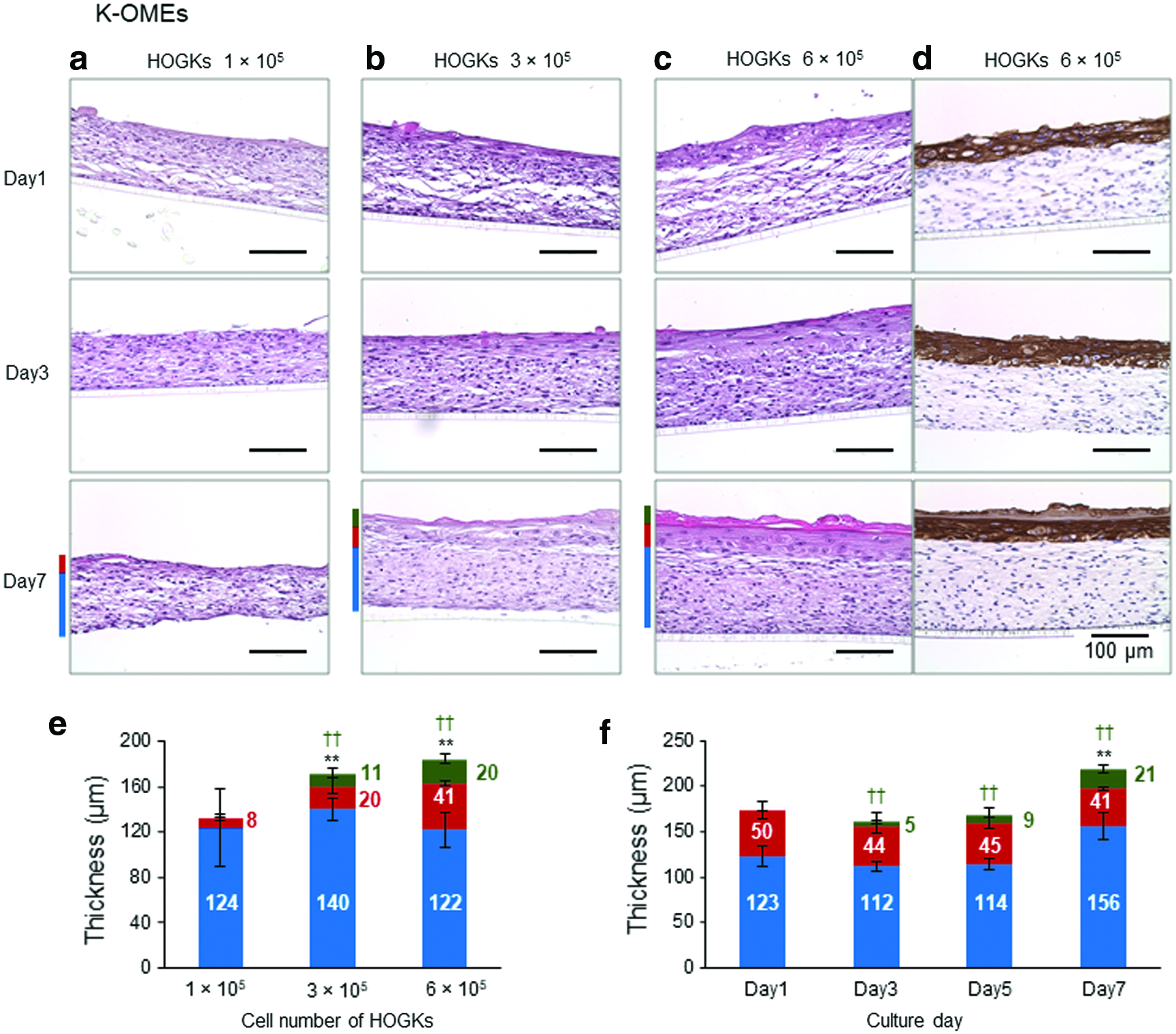
We constructed K-OMEs by using LbL cell-coated HOMFs for lamina-propria equivalents and HOGKs for the epithelium. The air-lift culture of HOGKs on HOMFs layers was carried out for HOGKs differentiation of the epithelium (Fig. 2 and Supplementary Fig. S4). Figure 2a, b, and c show HE-stained images of 3D tissues constructed by 1 × 10 6 HOMFs and each cell number condition of HOGKs after differentiation for 1, 3, and 7 days of air-lift culture. The cell numbers of HOGKs in each condition were 1 × 10 5 , 3 × 10 5 , and 6 × 10 5 . In models using 1 × 10 5 HOGKs, the thicknesses and differentiations of epithelium were insufficient (Fig. 2a, e and Supplementary Fig. S4a). In models using 3 × 10 5 (Fig. 2b and Supplementary Fig. S4b) and 6 × 10 5 HOGKs (Fig. 2c, d and Supplementary Fig. S4c), differentiation and keratinization as seen in human keratinized oral mucosa were observed. We were able to fabricate full-thickness K-OMEs. Cross-sectional HE-stained images clearly indicated the formation of the cornified, granular, spinous, and basal layers as K-OMEs, and that the keratinocytes of the cornified layer were enucleated. The thickness changes of each layer of K-OMEs due to the difference of seeding HOGK number (Fig. 2e) and during differentiation by air-lift culture (Fig. 2f) were estimated from HE and anti-CK (AE1/AE3) immunostained images (Fig. 2 and Supplementary Fig. S4). The homogeneous formation of a cornified layer, and boundary of epithelium and lamina-propria equivalents were clearly observed during the process of epithelial differentiation by air-lift culture, and the thickness of the cornified layer and epithelium increased with increasing seeding HOGK cell number (Fig. 2e) and air-lift culture time (Fig. 2f). We could control the thickness of the K-OMEs by changing the cell number of cultured HOGKs. In these our prepared tissues, the models using 6 × 10 5 HOGKs (Fig. 2c, d and Supplementary Fig. S4c) were the most abundant and histologically comparable to human native tissues. Therefore, we verified K-OMEs in the cell number condition of 6 × 10 5 HOGKs.
HE-stained images of oral mucosa equivalents with keratinization (K-OMEs) consisting of HOMFs (1 × 10
6
cells) and
Construction of OMEs with non-keratinization (N-OMEs)
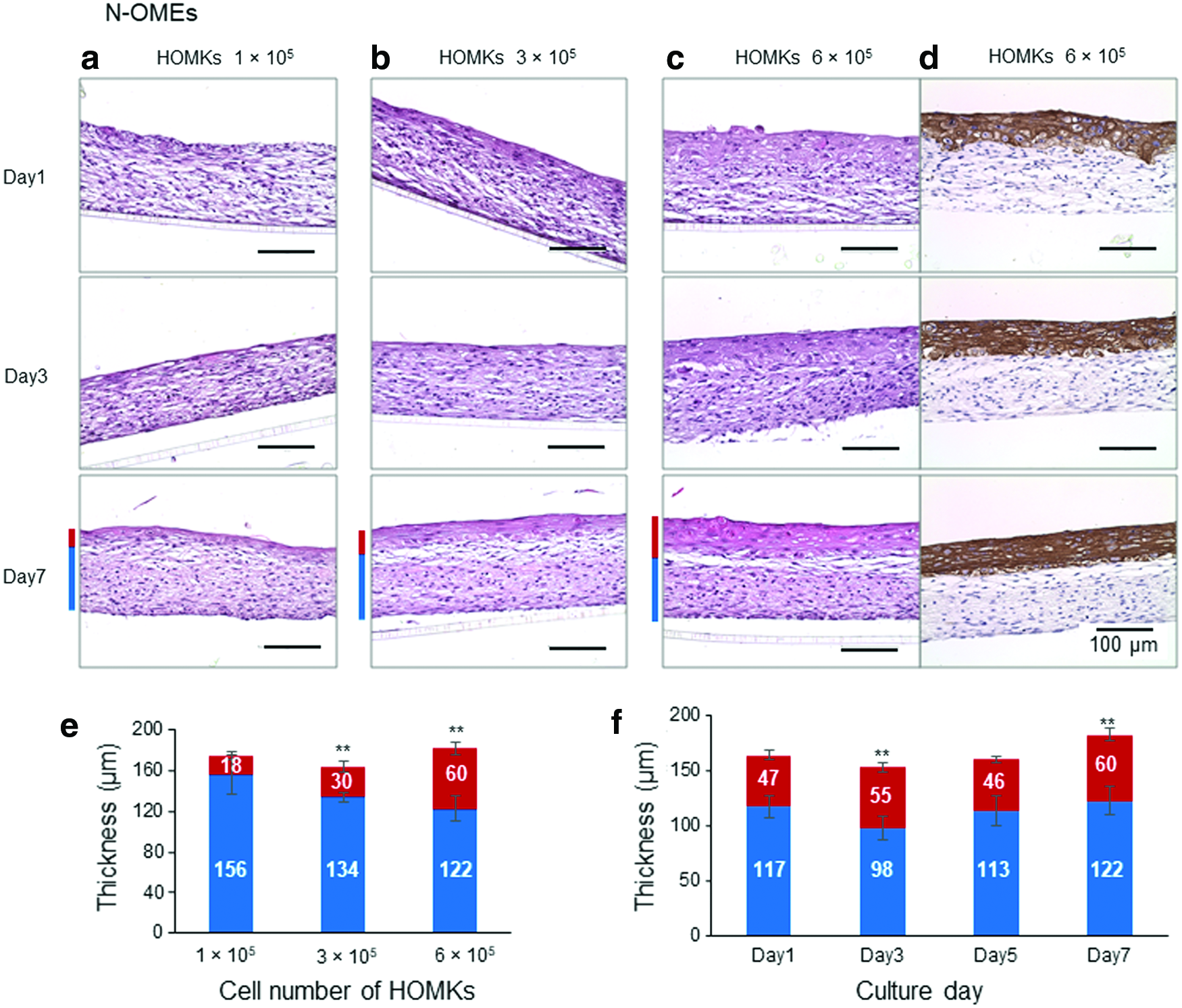
Using the same culture technique and conditions as that for K-OMEs, we were able to fabricate N-OMEs by using LbL cell-coated HOMFs for lamina-propria equivalents and HOMKs in each cell number condition for epithelial layers (Fig. 3 and Supplementary Fig. S5). In N-OMEs constructed by using 3 × 10 5 (Fig. 3b and Supplementary Fig. S5b) and 6 × 10 5 HOMKs (Fig. 3c, d and Supplementary Fig. S5c), the stratification and differentiation of the epithelium were observed (Fig. 3e, f). However, in the constructions using 1 × 10 5 HOMKs, the thickness and differentiation of the epithelium were insufficient (Fig. 3a, e and Supplementary Fig. S5a). Cross-sectional HE-stained images indicated the formation of the spinous and basal layer. In N-OMEs, the surface layer was not keratinized and enucleated and the granular layer did not exist. The non-keratinizing behavior of HOMKs was observed in the case of OMEs consisting of HOMKs alone (epithelium equivalents), but proliferation and differentiation of HOMKs on the culture insert membrane were not observed. The thickness of epithelial layers in N-OMEs was affected by the cell number of HOMKs (Fig. 3e). Further, the culture time promoted the differentiation of the epithelium (Fig. 3f). The histology of N-OMEs was similar to human native oral non-keratinized mucosa. In these prepared tissues, the models using 6 × 10 5 HOMKs (Fig. 3c, d and Supplementary Fig. S5c) were the most abundant and histologically comparable. Therefore, we verified N-OMEs in the cell number condition of 6 × 10 5 HOMKs.
HE-stained images of oral mucosa equivalents with non-keratinization (N-OMEs) consisting of HOMFs (1 × 10
6
cells) and
Necrosis of cells in OMEs was not observed, although the thickness of our OMEs was more than 100 μm. It was suggested that OMEs in the air-lift culture were supplied the nutrients through the membrane at the bottom of the insert.
Immunohistochemical staining of K-OMEs and N-OMEs
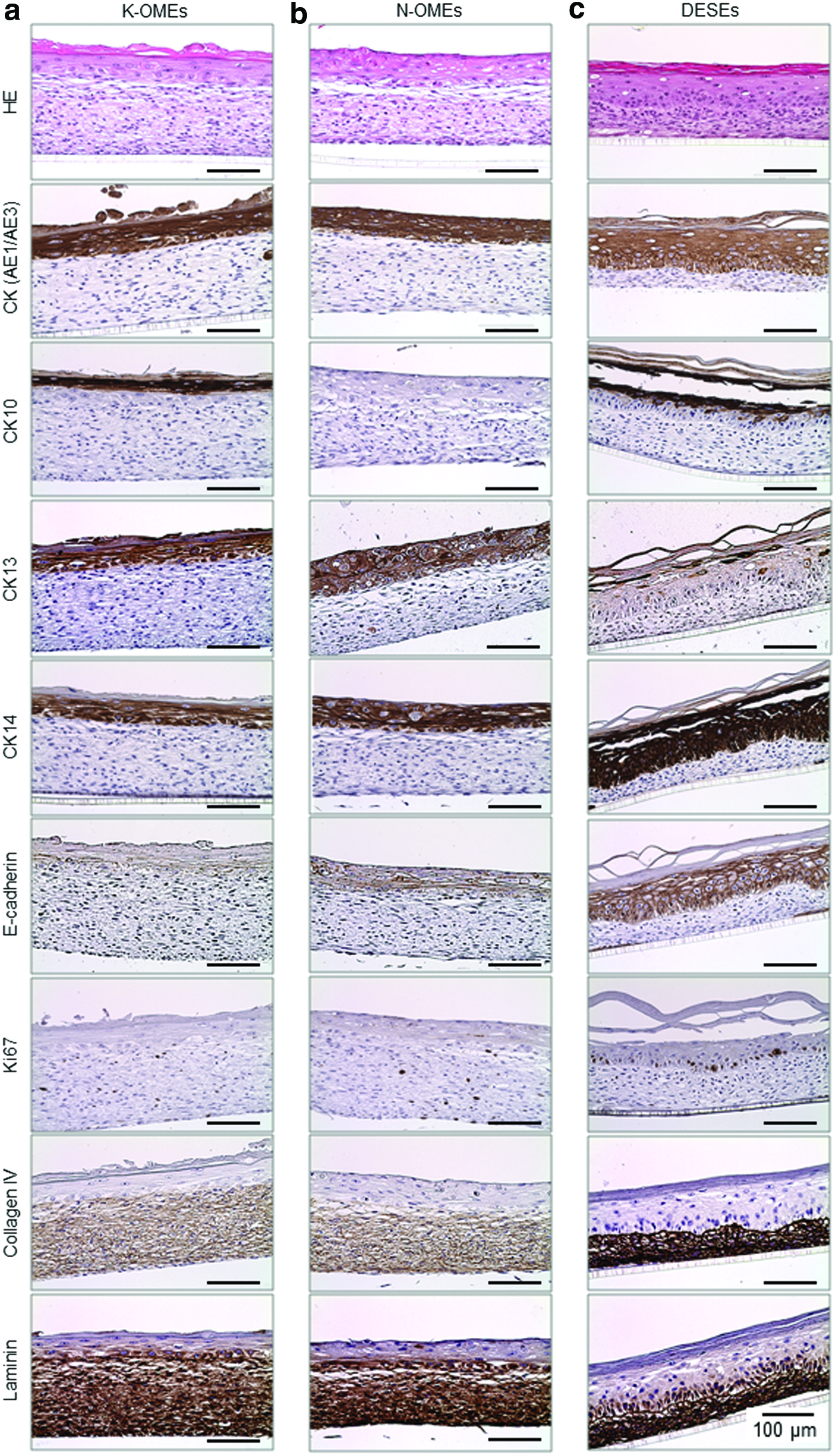
The constructed oral mucosa equivalents (K-OMEs and N-OMEs) were revealed to be histologically similar to human oral mucosa tissue. To understand the differentiation in detail, immunohistochemical staining with CK (AE1/AE3), CK10, CK14, E-cadherin, Ki67, collagen IV, laminin, and CK13 was performed (Fig. 4). We also compared the structure and differentiation between not only K-OMEs (Fig. 4a) and N-OMEs (Fig. 4b) but also our previously reported DESEs (Fig. 4c). DESEs were constructed by the methods described in our previous reports.26,31 CK (AE1/AE3) was strongly expressed in all of the epithelial layers of K-OMEs, N-OMEs, and DESEs. Although the cultured cell numbers of fibroblasts and keratinocytes were the same conditions in these models, the thickness of the epithelium and fibroblast layers caused differences. It is suggested that the differences in the proliferation and turnover of keratinocytes and fibroblasts between oral mucosa and the skin may affect the tissue structure. 33
HE staining and immunostaining images of
CK10, a marker of keratinized epithelium, was expressed in the keratinized epithelium except in the basal layer of K-OMEs and DESEs. In N-OMEs, it was found to be completely absent. In bio-tissue, ortho-keratinized epithelium, such as the skin and the palate, contains CK10. However, gingiva and parakeratinized oral mucosa contain CK10 or CK13.18,19 The results of immunohistochemical staining reflected the characteristics of these equivalents; K-OMEs and DESEs had the keratinized epithelium, and N-OMEs had the non-keratinized epithelium.
CK14, a marker of the stratum basal layer of the epithelium, was expressed in all epithelial layers, including the basal layer in these models. Comparing the images immunostained with CK10, the stained area expands to the basal layer. From the immunostained images with CK10 and CK14, the existence of the basal layer in these models was confirmed. E-cadherin, a marker of intracellular adhesions in the epithelium, was detected at the edge of the keratinocytes (between epithelial cells) in the epithelium. This corresponded to the characteristics of human oral epithelial tissue.
Ki67, a marker of proliferative cells, was only detected in the basal cells of DESEs. However, the expression was found to be completely absent in K-OMEs and N-OMEs. The decrease in the number of cells expressing Ki67 has already been shown in the course of kinetic proliferation in oral mucosa models, 34 passing from a maximum proliferative state in the early stages of culture. This is due to the fact that the highest proliferation rate in a developing oral mucosa is the early stage of epithelial formation and it decreases progressively as time passes.
Collagen IV and laminin are proteins of the basement membrane in oral mucosa or the skin. These markers were expressed in the basement membrane of other 3D oral mucosa models using biocompatibility materials such as collagen and matrigel for lamina-propria equivalents. 35 Collagen IV was expressed in lamina-propria equivalents of OMEs and the dermis of DESEs in our experiments. It was reported that in the case of co-culture of fibroblasts and keratinocytes, collagen IV was predominantly produced by fibroblasts.36,37 The immunostaining images of collagen IV suggested that collagen IV was mainly produced by fibroblasts, and it was distributed in lamina-propria equivalents of OMEs and the dermis of DESEs. Laminin was strongly expressed in basal cells and lamina-propria equivalents of OMEs and the dermis of DESEs. Several studies demonstrated that basal cells and fibroblasts produce various kinds of laminin. 38 These findings indicate that fibroblasts in lamina-propria equivalents of OMEs and the dermis of DESEs may be important for formation of basal layer and basement membrane.
CK13, the differentiation-associated marker of non-keratinized oral mucosa, was strongly expressed in both K-OMEs and N-OMEs, but its expression in DESEs was weak. In the epithelium of K-OMEs and DESEs, epithelial cells were enucleated and had keratosis whereas the epithelial cells of N-OMEs retained their nuclei and stratum corneum was absent. In the N-OMEs, the strong expression of CK13 and the absence of CK10 supported the non-keratinized differentiation of the epithelium in tissues even after air-lift culture at 1 week. Although the epithelium of K-OMEs was keratinized, the difference of CK13 expression between K-OMEs and DESEs may be caused by the difference of characteristic of keratinocytes. It is suggested that HOGKs have an intermediate characteristic of keratinized and non-keratinized epithelium. 39 These immunostained images verified that our constructed OMEs have characteristics as human oral mucosa, and we could separately prepare different keratinized OMEs. A comparison between OMEs and DESEs enabled us to understand the differences in detail.
TEER profiles of K-OMEs and N-OMEs
To compare the barrier functions of the epithelium in the K-OMEs, N-OMEs, and DESEs, TEER values were measured during the 7 days of differentiation (Fig. 5). The TEER values of these equivalents increased day by day with epithelial differentiation. The differences in values finally became apparent at day 7: The largest was DESEs, followed in order by K-OMEs and N-OMEs (DESEs > K-OMEs > N-OMEs) (Fig. 5a, b). The TEER values of DESEs were more than 15 times higher than OMEs. In OMEs, the values for K-OMEs were significantly higher than those for N-OMEs (Fig. 5a). The factors affecting TEER values were thickness, intercellular adhesion, differentiation, and keratinization. The difference in TEER values between K-OMEs and N-OMEs was attributed to the difference of keratinization of the epithelium in OMEs. In this study, we compared the OMEs and DESEs in the same conditions of cell numbers of keratinocytes and fibroblasts and culture methods. Clearly, the epidermis and cornified layers of DESEs were thicker and differentiation of the epidermis was higher than OMEs. These were suggested to be factors in the differences of TEER values in these models. The establishment of histological and functional standard values of biological tissue and constructed 3D tissue models will make it possible to optimize and generalize the oral mucosa model.

TEER profiles of
Construction of lamina-propria equivalents with blood capillaries
To fabricate advanced human OMEs with blood capillaries, we performed a co-culture of HUVECs based on our previous reports 25 where we constructed blood capillaries in NHDF layers. Using the same approach, we were able to construct lamina-propria equivalents consisting of LbL cell-coated HOMFs with blood capillaries (Supplementary Fig. S3). The CLSM images (Fig. 6a) and cross-sectional images (Supplementary Fig. S6) immunostained with anti-CD31 antibody clearly showed the existence of tubular structure. The covered % area, total tube length, and the branching points of blood capillaries in the lamina-propria equivalents increased with increases in the seeding number of HUVECs (Fig. 6b–d). These assessments provided evidence of active neovascularization of tissues with co-cultured HUVECs. Further, we compared the formation of blood capillary in LbL(+) and LbL(−) HOMFs layers (Supplementary Fig. S7a). The covered % area, total tube length, and the number of branching points of blood capillaries in LbL(+) HOMFs were significantly larger than in LbL(−) HOMFs (Supplementary Fig. S7b–d). It was suggested that densely packed LbL(+) HOMFs layers allowed HUVECs to vascularize. The LbL FN-G cell coating technique was also demonstrated to be effective in the construction of vascularized lamina-propria equivalents. In our previous research of 3D liver models composed of NHDFs, HUVECs, and hepatocytes, we demonstrated that human vascular endothelial growth factor (hVEGF) produced by NHDFs in LbL(+) tissues was higher than that of LbL(−) tissues, because cell-cell interactions are enhanced by LbL FN-G cell coating. 40 Thus, it is suggested that HOMFs were similarly affected functionally by the LbL FN-G cell coating technique.

Construction of OMEs with blood capillaries
After the co-culture of HUVECs (0.5, 1, or 2 × 10 5 ) with LbL cell-coated HOMFs, 1 × 10 6 HOGKs or HOMKs were seeded onto the top of co-cultured fabrications and lifted to the air-liquid interface for differentiation of the epithelium (Supplementary Fig. S3b). After 7 days of air-lift culture, obvious network structures of HUVECs in the lamina-propria equivalents and epithelium consisting of differentiated HOGKs or HOMKs on the lamina-propria equivalents were observed (Figs. 7a–l and 8a–l). The thickness and differentiation behaviors of the epithelium in K-OMEs and N-OMEs were not changed by the presence of blood capillaries and the number of mixed HUVECs (Figs. 7m and 8m). Some tendency was observed in the case of DESEs in our previous report.

Cross-sectional

Cross-sectional
The CLSM images immunostained with anti-CD31 antibody clearly showed tubular structure existing inside the HOMF lamina-propria equivalents after 7 days of epithelial differentiation. The area where capillaries were present in the K-OMEs and N-OMEs increased with increases in the seeding number of HUVECs (Figs. 7j–l and 8j–l). These results indicate that the density of blood capillaries could be controlled by adjusting the seeding cell numbers of the co-cultured HUVECs, even though an epithelial layers existed on lamina-propria equivalents. It is suggested that the production of not only hVEGF 40 but also laminin in lamina-propria equivalents of OMEs (Fig. 4) promoted the vascularization and construction of blood capillary networks. 41 Further, cross-sectional images immunostained with anti-CK13 (Figs. 7d–f and 8d–f) and anti-CD31 antibody (Figs. 7g–i and 8g–i) showed tissues maintaining mucosal characteristics with blood capillaries. We have previously reported the construction of co-individual networks of blood and lymph-like capillaries in skin dermis equivalents.26,42 In addition, it has been demonstrated that the implanted tissue with blood capillary networks was connected with the host circulatory system by anastomosis. 43 This method is an attractive technique for engineering pre-vascularized tissues for transplantation.
In tissue engineering research of OMEs, fabrications with blood capillaries have yet to be reported. Our vascularized K-OMEs and N-OMEs have great potential for applications in regenerative medicine and drug screening tests. In particular, high transplantation efficiency in clinical studies using human OMEs with blood capillaries is expected because of faster nutrient and oxygen supply from the host blood capillaries through the connected blood capillaries. The recent progress in reprogramming of adult cells toward iPS cells introduces a new dimension to the field of drug development and regenerative medicine. The technology allows the fabrication of tissue-, disease-, and patient-specific cells. The construction of patient- or disease-specific OMEs by using iPS cell-derived specific cells would allow for the high versatility and utility of OMEs. Further experiments using the K-OMEs and N-OMEs with blood capillaries are now in progress for in vitro and in vivo application.
Although the human skin models have been generally used for irritation and toxicity tests as defined by Organization for Economic Co-Operation and Development test guidelines, the reactivity of oral mucosa models for drug stimulus was not unified quantitatively and qualitatively in previous reports of oral mucosal models. For evaluating reactivity using our OME, we must clarify closeness (similarity) between our OMEs and human bioactive oral mucosa. Further, the majority of human oral mucosa models hitherto reported are composed of epidermis only, or composed of epidermis and lamina-propria, which is constructed by biocompatible materials and oral mucosa fibroblasts. Co-culture with epithelial cells and fibroblasts is important because fibroblasts affect the differentiation of epithelial cells.34,44 However, these oral mucosa models could be further improved by the addition of other types of cells and organs, such as immune cells, endothelial cells, stem cells, salivary glands, 45 and bones.46,47 The construction method of OMEs described in this study would allow for incorporation of various types of cells in the lamina-propria region. The findings of this study suggest that there are a wide range of potential applications for oral mucosa 3D tissue models.
This study has limitations related to the structure and function of constructed blood capillaries in OMEs. The blood capillaries were successfully prepared into the lamina-propria whole region of the OMEs. However, it is difficult to control the diameter of blood capillaries using LbL cell coating technology. Further, the effect of vascular structure on the function of OMEs is not clear in this study. The development of a method for regulating vascular structure in OMEs, and clarification of the structure of constructed blood capillaries is required in future studies.
Conclusion
At present, 3D oral mucosal models are available commercially, such as Epioral/Epigingival (MatTek, Ashland, MA)48,49 and SkinEthic oral epithelium (SkinEthic Laboratories, Nice, France) 50 consisting only of oral epithelium without lamina-propria. Fibroblasts contained in lamina-propria play an important role in epithelial differentiation. Further, the epithelial phenotype and profile of cytokeratin expression is influenced by the nature and origin of the underlying fibroblasts.34,44 In this study, we constructed different keratinized types of 3D epithelialized OMEs by using the LbL cell coating technology. Histological analysis of the constructed OMEs revealed distinct layers reflecting human oral mucosa. K-OMEs consisted of four layers: a basal, spinous, granular, and cornified layer in the epithelium and lamina-propria. On the other hand, in N-OMEs, the granular layer was replaced by the surface layer, the cells of which lack keratohyaline granules. The blood capillaries were successfully incorporated into the lamina-propria region of the K-OMEs and N-OMEs. For functional characterization, the OMEs were evaluated by permeation tests. It was confirmed that permeation of OMEs reflected the keratinization and differentiation. The OMEs with blood capillaries have potential for various applications, such as drug effect testing, toxicology, and tissue engineering. In particular, it is expected that they will be used as an alternative method to animal testing. Further, for medical application, our models have potential as alternative treatment tools to conventional methods for medical graft surgery.
Footnotes
Acknowledgments
The authors wish to thank Takuma Okuda (Lion Corporation) for his insightful comments and suggestions in this study. This work was funded by Grants-in-Aid for Scientific Research (KAKENHI) from the Japan Society for the Promotion of Science (no.17K11872).
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.