
Abstract
Anterior cruciate ligament (ACL) injuries are frequent, as >200,000 injuries occur in the United States alone each year. Owing to the risks for associated meniscus and cartilage damage, ACL injuries are a significant source of both orthopedic care and research. Given the extended recovery course after ACL injury, which often lasts 1–2 years, and is associated with limited participation in sports and activities of daily living for patients, there is a critical need for the evolution of new and improved methods for ACL repair. Subsequently, animal models of ACL reconstruction (ACLR) play a key role in the development and initial trialing of novel ACL interventions. This article provides a clear operative description and associated illustrations for a validated, institutional animal care and use committee, and veterinarian approved and facile model of ACLR to serve researchers investigating ACLR.
Impact Statement
Anterior cruciate ligament (ACL) injury and reconstruction is a central area of research in orthopedics due to high and increasing injury rates worldwide and profound potential effects on patient function, psyche, medical costs, and subsequent arthritis. Rabbit models provide the gold model of ACL reconstruction (ACLR) in the laboratory but have not been methodologically described for ready implementation at other institutions and for consistent surgical technique, with comparable results between research groups. This article provides the first well-described methodology for rabbit ACLR, with step-by-step directions and accompanying pictures including relevant pre- and perioperative protocols and materials.
Introduction
Anterior cruciate ligament (ACL) injuries are of high clinical relevance given their relative frequency and potential for associated meniscus and cartilage injury. 1 Given their incidence of 37–61 injuries per 100,000 person-years and prolonged recovery, often lasting 1–2 years, ACL research expenditure is among the highest in orthopedics.2,3 Although methods of ACL injury prevention are increasingly recognized and employed, the rate of ACL injuries continues to rise.1,4 Although various methods of ACL reconstruction (ACLR) have been described, the incidence of clinical ACLR failure is not trivial, with published rates as high as 15%. 2 Concurrently, the rate of osteoarthritis (OA) after ACL injury, even after ACLR, remains high, with studies demonstrating as high as a 39% increased OA risk at 14 years of follow-up compared with the contralateral non-injured side. 5
A key aspect of ACLR research has been biomaterials development and associated animal models, with rabbits, in particular, providing the gold standard for animal research models.6–9 Mouse models have been described, but there are limitations in the amount of material for subsequent molecular, histological, and biomechanical analysis, which has made rabbits the preferred species for research in this field.10,11 Furthermore, with use of rabbit models, a semitendinosus autograft can be harvested at the time of surgery, which provides a hamstring-based reconstruction, much as is performed clinically in humans. However, although many rabbit studies exist for ACLR, with >200 PubMed citations that result from the search terms “rabbit” and “anterior cruciate ligament,” to date, no study has provided a methodological guide for investigators. Therefore, the authors' documentation of rabbit ACLR methods is of significant research relevance given the volume of publications in this area, the need for repeatable methods, and the status of rabbits as the gold standard for small animal ACL research.
Materials and Methods
Animal species
Four-month-old 2.5 kg female New Zealand white rabbits (Covance, Princeton, NJ) were used in these studies. Female rabbits were selected to decrease potential biological variability between sexes given that male rabbits tend to be larger than females, which adds variation to experimental outcomes. In addition, male rabbits are difficult to group house and, therefore, the use of females is also of logistically strategic value.
Equipment
Anesthesia inhalation system (Ohmeda Modulus SE, 1004-9020-000)
Endotracheal tube (Jorgensen Laboratories, cat. no. J1350D)
Surgical drill, battery, and charger (Stryker, cat no. 4203, 4103-133, 4110-120, and 4115)
3 × 8 mm Biotenodesis kit (Arthrex, Naples, FL, cat. no. AR-1530DS)
Graft fixation:
3.5 mm suture button (Arthrex, cat. no. AR-8920), or
crimp sleeve (Loos & Co., cat. no. SL11-1) and Swager (Loos & Co., cat. no. 1-3-SBHS)
Sterile surgical gown, sterile gloves, mask (Kimberly-Clark Professional).
Reagents and surgical materials
Ketamine HCl injection, USP, 100 mg/mL (Ketalar, NDC 42023-115-10)
Xylazine sterile solution, 20 mg/mL (Akorn, Inc., NADA 139-236)
Antibiotic: cefazolin (Novaplus, NDC 0143-9262-01)
Antiseptic: povidone-iodine solution (Aplicare, NDC 52380-1905-6)
Ethanol (Brenntag Great Lakes, cat. no. 693509)
Isoflurane (Cardinal Health, cat. no. 4985248)
Buprenorphine hydrochloride, sustained release, 3.0 mg/mL (ZooPharm, available upon individual compounding request)
Eye ointment (Dechra, NDC 17033-211-38)
Phosphate-buffered saline (PBS) (Gibco, cat. no. 10010-023)
Sterile gauze sponge (Curity Covidien, cat. no. 397110)
21 gauge needle (BD, cat. no. 305165)
22 gauge needle (BD, cat. no. 305156)
24 gauge butterfly catheter (Jelco, cat. no. 4053)
60 mL syringe (BD, cat. no. 309653)
#15 scalpel blade (Bard-Parker, cat. no. 371115)
Sutures:
3-0/2 metric FiberWire (Arthrex, cat.no. AR-7227-01)
2-0 Vicryl (Ethicon, cat. no. J426H)
4-0 Vicryl (Ethicon, cat. no. J339H)
Scalpel handle
Forceps
Needle driver
Scissors
Electric hair trimmer (Philips)
Weighing scale.
Graft fixation constructs
Although 3.5 mm suture buttons (Arthrex) provide good graft fixation and are available through clinical catalogs (Fig. 1A), we have found that stainless steel crimps allow for the creation of effective suture anchors at 1–2 orders of magnitude decreased costs and are well tolerated and durable for biologic use while also allowing fixation that is appropriate for immediate weight bearing without any restrictive devices. Crimp-based buttons are created employing a 1/32 inch crimp and a 3-0 FiberWire (Fig. 1B). A loop of 3-0 FiberWire is passed through the crimp (Fig. 1C) and, subsequently, the loop is tightened until 1 mm of gap remains between the suture and the crimp. Thereafter, the construct is crimped (Fig. 1D) and the leftover tails of the construct are trimmed (Fig. 1E). The resultant construct (Fig. 1F) with a FiberWire loop for graft fixation and suspension is safe, effective, and inexpensive. They can be sterilized by allowing them to soak for 1 h in 70% ethanol and then aseptically transferring the constructs into a sterile container for intraoperative use.

ACLR graft fixation. Commercially available suture buttons (3.5 mm suture button; Arthrex)
Preoperative preparation
Rabbits are obtained and kept in an off-site institutional quarantine for 5 days before transfer to the research laboratory. After clearance by veterinarian staff, rabbits were transferred to the research destination and allowed to acclimate for 24–48 h before undergoing a surgical procedure. Metal surgical instruments were prepared by autoclaving followed by drying in an oven. Sterilization of any graft materials (i.e., crimp sleeves) was achieved by soaking in 70% ethanol for 1 h followed by storage in sterile containers at 4°C for up to 1 month before the surgical procedure.
Surgical induction
All procedures were conducted upon approval from the Institutional Animal Care and Use Committee (IACUC) at Mayo Clinic and performed in agreement with the institutional and national regulations for animal handling and use.
Weight rabbit
Sedate rabbit with intramuscular ketamine (35 mg/kg) and xylazine (5 mg/kg) and a 22 gauge needle. At the time of sedation, cefazolin (22 mg/kg) is provided as perioperative antibiotic prophylaxis.
Intubate the rabbit and obtain intravenous access at the marginal ear vein with a 24 gauge butterfly catheter.
Animal preparation
With an electric shaver, remove hair around the region of the operative extremity, and create a clear area to accommodate a 4 cm incision on the anterior aspect of the knee.
Apply lubricating eye ointment to prevent dryness of eyes during surgery.
Transfer the animal to a heating pad overlaid with sterile drapes (Fig. 2A) and initiate maintenance anesthesia within 15 min of sedation using isofluorane (2.5–3.5%) titrated to comfort without concurrent respiratory depression.
Disinfect the shaved region by gentle swabbing with sterile cotton gauze dipped in povidone–iodine.
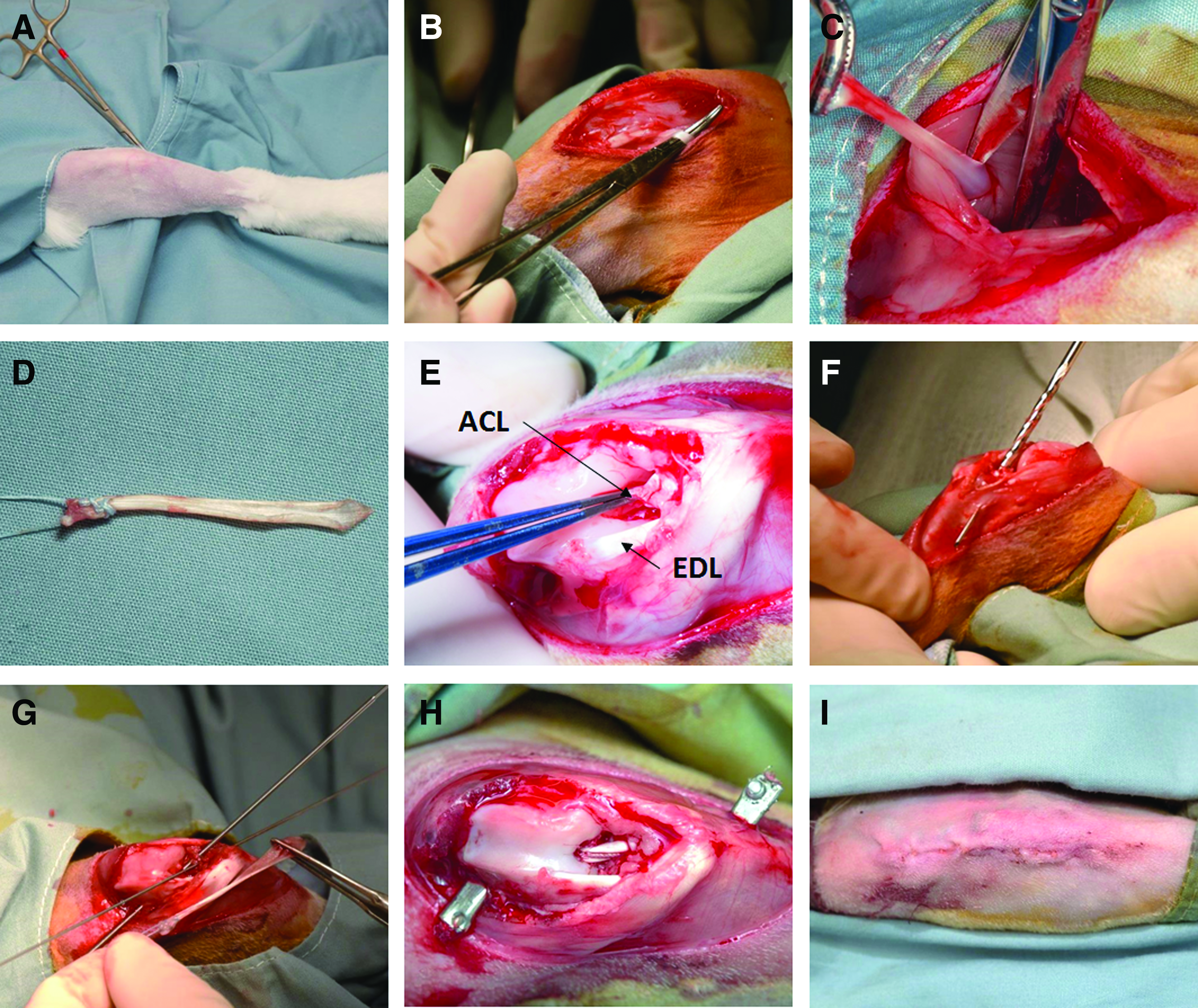
Operative procedure for ACLR. Preoperative rabbit positioning and preparation
Operative procedure: ACLR
Under sterile conditions and using a sterile #15 scalpel, a midline incision was made centered over the anterior aspect of the knee and patella, ∼4 cm in length. Ensuring that the tissue layers are incised together for future repair, the incision was taken down to the level of the quadriceps/patellar tendon.
For semitendinosus autograft reconstruction, a medial flap was subsequently developed by exposure of the medial collateral ligament. Medial to this ligament, a transverse 2 cm incision was made in the muscular fascia, being careful to avoid the vascular bundle that runs on the posterior edge of the fascia.
The medial edge of the quadriceps was then lifted and the semitendinosus was exposed and retracted from underneath the quadriceps (Fig. 2B). The distal insertion of the tendon was released sharply using the scalpel and retracted to allow for mobilization of the tendon to its proximal muscular aspect employing reverse scissoring. Thereafter, the proximal aspect of the tendon was divided by employing scissors, providing 3–4 cm of tendon autograft for subsequent reconstruction (Fig. 2C).
Krakow sutures were placed one end of the tendon employing 3-0 FiberWire sutures and the tendon was placed into PBS to prevent desiccation during graft tunnel preparation (Fig. 2D).
Next, attention was turned to the knee. A medial parapatellar arthrotomy was performed and the knee was opened by sliding the patella laterally. The infrapatellar fat pad was debrided to assist surgical visualization and, subsequently, ACL was identified and excised, with debridement of the associated tibial and femoral footprints (Fig. 2E). Care was taken to avoid damaging the extensor digitorum longus tendon, which in rabbits originates from the lateral distal femur as compared with the tibial origin found in humans.
Tibial and femoral bone tunnels were created using K-wires to establish tunnel trajectory and subsequently overdrilling with the 2.5 mm drill from the biotenodesis kit, employing an inside-out technique and the native ACL footprint as a starting point (Fig. 2F).
Thereafter, the looped K-wires from the tenodesis kit were passed through the tunnels to allow for antegrade graft passage through the tunnels. Subsequently, the semitendinosus autograft was compared with the overall bone tunnel–intra-articular space–bone tunnel length (Fig. 2G) and trimmed to length.
The final length of tendon autograft was cleaned of muscle employing gentle sweeps of the scalpel in a perpendicular direction and the second end was sutured by employing a Krakow stitch, as had previously been done on the first end.
The proximal end of the graft was attached to the chosen button or crimp construct just before passing the tendon through the bone tunnels so that the button/crimp can serve as an extraosseous endpoint during graft passage.
The graft was then passed through the tunnels and secured by tying down the second sutured end extraosseously using buttons or crimp constructs (Fig. 2H). The knee was ranged through full range of motion to ensure no restrictions to motion and isometric graft placement.
Before commencing closure, the joint was irrigated with sterile PBS. Thereafter, the arthrotomy was reapproximated with interrupted 2-0 Vicryl suture. Metal graft fixation (buttons or crimps) was sutured flush to the periosteum to avoid soft tissue irritation, placing the metal fixation below the quadriceps proximally and underneath the medial fascial flap developed during semitendinosus harvest distally. Thereafter, the subcuticular layer was closed by employing subcuticular interrupted 4-0 Vicryl suture materials under loupe visualization (Fig. 2I). We recommend subcuticular suture placement to prevent braided material from wicking bacteria from the skin surface and also to avoid the necessity of nonabsorbable suture removal.
As final checks, the knee was again ranged through full range of motion to ensure no restrictions and a robust closure. In addition, an anterior-posterior radiograph was obtained to ensure satisfactory tunnel placement and the absence of an intraoperative fracture.
Postoperative care
At the time of procedure end, rabbits were provided a 120 cc subcutaneous bolus of normal saline for postoperative hydration using two 60 cc syringes and a 21 gauge needle. In addition, sustained release buprenorphine (0.12 mg/kg) was provided at the time of surgical closure for postoperative analgesia. Rabbits were placed in Elizabethan collars to protect the surgical site and were monitored continuously during initial recovery and then every 12 h once they were ambulating. No postoperative immobilization was applied. Any potential complications such as cage sores, wound infections, weight loss, or wound dehiscence were reviewed with the veterinarian and managed in a way designed to minimize discomfort or suffering.
Results and Discussion
The current IACUC and veterinarian-approved method of ACLR was performed in >70 rabbits with well-tolerated effects and no significant complications, and previous results were published in peer-reviewed journals.6,12 With this model, we can provide reproducible ACLR with radiographically well-aligned constructs (Fig. 3A), which were biomechanically well fixed and appropriate for immediate weight bearing as tolerated. Furthermore, the fixation method described is novel and we have found that stainless steel crimps allow for the creation of effective suture anchors at 1–2 orders of magnitude decreased costs while providing fixation that is facile in application, well tolerated, and durable for biologic use.

Postoperative imaging of ACLR. Immediate postoperative radiograph of reconstruction
Using the described methods, no significant intraoperative complications have occurred to date, with each animal surviving both the immediate operative and postoperative period. Furthermore, no postoperative complications requiring euthanasia before experimental endpoints, as determined by independent veterinarian staff, have occurred. In addition to surgical reproducibility and safety, the described model demonstrates physiologic bony tunnel remodeling and ingrowth, visible on computed tomography at 4 weeks after ACLR (Fig. 3B–D). Simultaneous histologic inquiry has demonstrated that viable semitendinosus autograft remains present and intact at 4 weeks status postimplantation, with progressive ingrowth visualized in the bone tunnels (Fig. 4A, B). In addition, our previously published RNA sequencing analysis of the chosen autograft provides the basis for future polymerase chain reaction (PCR) and RNA sequencing-based comparisons when employing the described model. 12
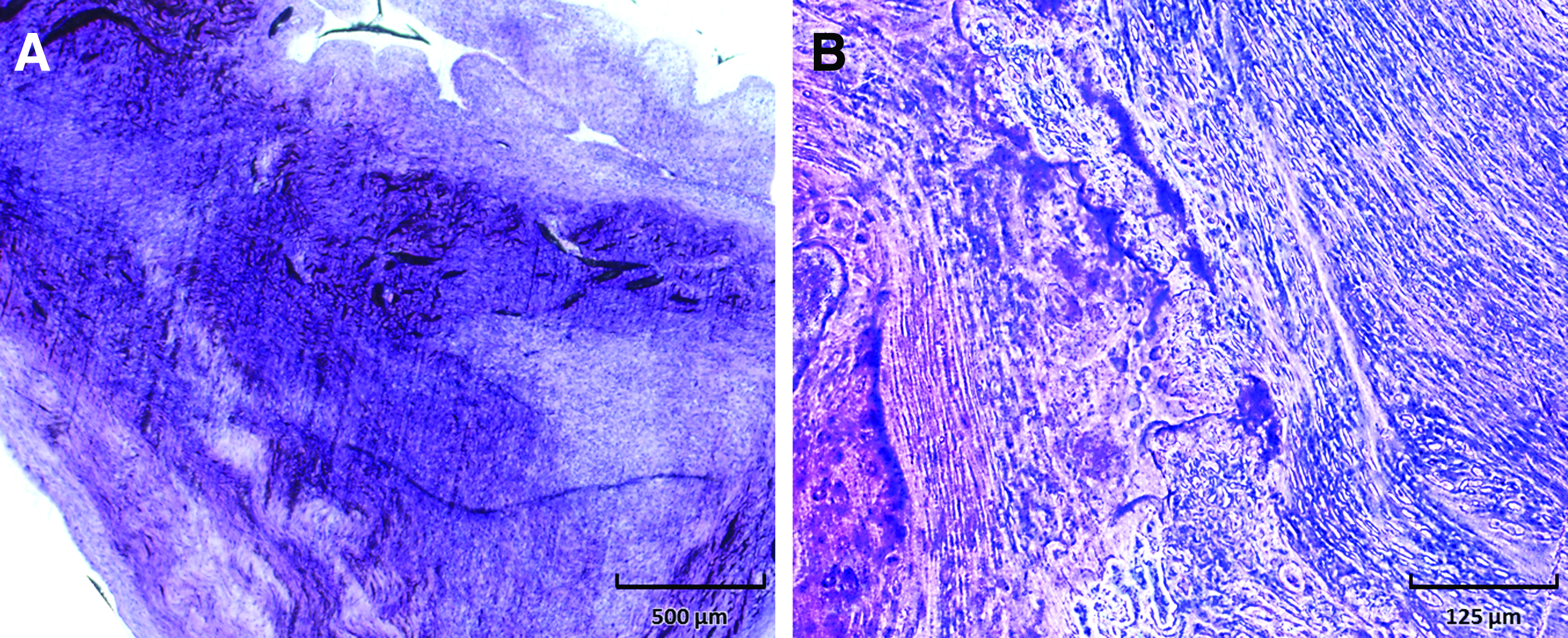
Hamstring autograft healing at 4 weeks postoperatively. Hematoxylin and eosin histology of viable hamstring intra-articular autograft tendon at 5 × magnification
Using the provided methods, a strong ACLR construct is made possible through the use of the tendinous portion of the semitendinosus as compared with its flat thin portion as it courses proximally along the muscular aspect of the semitendinosus. In our experience, the mean thickness of a single strand of the tendon is 2.36 mm in this area, which provides a graft that satisfactorily fills the 2.5 mm drilled tunnel and provides a small area of space for running scaffolds and functionalized sutures alongside the tendon. This practice is supported by other articles that have described other single-strand semitendinosus constructs employing the distal tendinous portion of the graft.9,13 In addition, by employing the distal tendinous portion of the graft, muscular contamination is limited, which is of importance given the substantial potential effects of high muscular gene transcription and expression on subsequent PCR and RNA sequencing-based analyses.
Although ACLR has been described in rabbits previously in the literature, the surgical protocols previously presented generally involve single-paragraph high-level descriptions that are difficult to reproduce precisely.9,13–15 In contrast, the methods provided in this article are comprehensive and include the necessary materials, preoperative preparation, and step-by-step directions for ACLR, enabling others to prepare and establish ACLR models through accurate reproduction of the comprehensive and methodological instructions. In addition, the novel crimping method described provides a cost-effective approach with immediate stability at the bony ends of the tunnels and has been well tolerated, without any noted skin issues in the animals, especially given the subquadriceps (proximal) and subfascial (distal) placement of the crimps. In such a manner, the small 2 cm incision employed to create a medial flap for semitendinosus harvest functions both provides ready access to this tendon without the need for special tendon harvesting supplies and provides soft tissue coverage for the distal metal fixation.
Conclusion
This article describes a straightforward, practical, and facile model useful for the study of ACLR in rabbits. This model permits assessment of bony tunnel healing and ligament biomechanics in an in vivo setting in a reliable and reproducible manner and offers a reconstruction that is anatomically analogous to that used in the clinical setting.
Footnotes
Acknowledgments
The authors acknowledge the generous philanthropic support of William and Karen Eby and thank the members of our laboratory, including Janet M. Denbeigh, PhD, Eric R. Wagner, MD, Mason Carstens, and Joshua A. Parry, MD, for stimulating discussions. The authors also acknowledge the support and assistance of Steve Krage, Joanne M. Pedersen, and Teresa D. Decklever with micro-CT, and Phillip K. Edwards with the Biomedical Imaging Core Laboratory at Mayo Clinic, Rochester.
Disclosure Statement
No competing financial interests exist.