
Abstract
The umbilical cord offers a source of readily available mesenchymal stromal cells (MSCs) for use in research and ultimately therapeutic application. However, methods of isolating these cells vary between investigators, and no standard method has been adopted. The aims of this work were to (i) develop a methodology for the isolation of umbilical cord matrix cells without the use of enzymatic digestion or complicated dissection; (ii) investigate the use of pooled maternal serum (MS) as a media supplement; and (iii) demonstrate that the cells isolated were MSCs. We have demonstrated that incubating tissue explants of less than 2 mm3 in serum for an hour, followed by the gradual addition of serum containing culture medium can increase cell yield compared to incubation in serum containing culture medium alone. More importantly, our method demonstrated that the use of pooled serum from women >37 weeks pregnant (pooled MS) yields higher cell numbers than the use of fetal bovine serum or pooled umbilical cord serum. Irrespective of the type of serum used, the isolated cells were MSCs according to the minimal criteria set out by the Mesenchymal and Tissue Stem Cell Committee of the International Society for Cellular Therapy. In conclusion, MS has the potential to be used as an alternative to fetal bovine serum for isolation and expansion of umbilical cord MSCs for clinical purposes.
Impact Statement
The umbilical cord is a source of readily available mesenchymal stromal cells (MSCs) for use in research and ultimately therapeutic application. However, alternative serum sources to fetal bovine serum (FBS) are needed to maximize the use of MSCs for clinical purposes. This article demonstrates that pooled serum from women >37 weeks pregnant (pooled maternal serum [MS]) could be used as an alternative for isolation and expansion of umbilical cord mesenchymal stromal cells, as it avoids the issues surrounding the use of FBS. It is also shown to be more effective than FBS and cord serum in producing a larger yield of MSCs, which is promising for future stem cell therapy.
Introduction
The umbilical cord matrix or Wharton's Jelly, which surrounds the two umbilical arteries and one umbilical vein, is known to contain MSCs.1,2 MSCs are spindle shaped cells that have the ability to self-renew and undergo osteogenic, adipogenic, chondrogenic, myogenic, and stromal cell differentiation, demonstrating a high degree of plasticity.3–5 Given the interest in the use of MSCs in regenerative medicine and the ethical challenges imposed by embryonic stem cells, the umbilical cord offers a readily available source of MSCs for use both in basic research to better understand human MSC biology and in therapeutic applications.
Many different methods of isolating MSCs from umbilical cord have been investigated, and no standard method has been adopted. The main differences in methods used are associated with whether or not the blood vessels were drained and/or removed, whether enzymatic treatment was used, the methods of harvesting Wharton's jelly, and the culture approach used (either culture of the tissue or of the isolated cells). There is some variation in the culture media used, but Dulbecco's modified Eagle's medium (DMEM) is typical.
Compounding the variation in methods used to isolate the cells are the different MSC characterization methods used, especially before 2006. In 2006, the minimal criteria to define human MSCs were set out by the Mesenchymal and Tissue Stem Cell Committee of the International Society for Cellular Therapy (ISCT). 6 The three minimal criteria are as follows: 1. plastic adherence; 2. expression of certain surface markers—at least 95% of the cell population must express CD73, CD90, and CD105, and less than 2% of the cell population can express CD14 or CD11b, CD34, CD45, CD79α or CD19, and human leukocyte antigen (HLA) class II (HLA-DR); and 3. differentiation potential—as a minimum, the cells must be able to undergo osteogenic, adipogenic, and chondrogenic differentiation. Since 2006, a number of investigators refer to these minimal criteria to define umbilical cord MSCs.7–11
Although different methods of isolating and characterizing MSCs from umbilical cord have been investigated, more recently, isolation methods have been referred to generally as either “enzymatic” or “explant”.8,12,13 Still, no standard method has been adopted as being the most effective. Different groups have adapted their own methods to suit their style of working. Some of these methods involve quick isolation of cells, but complicated methods of digestion.1,7,9,14 Others involve dissection of the umbilical cord by removal of blood vessels.10,12,15,16 Two important factors to consider when choosing an isolation method are cell yield and the time taken to achieve a desirable cell yield; these must be well balanced for therapeutic gain.
Recently, it has been highlighted that there is a need to find alternatives to FBS for use as a media supplement for MSC culture, due to the risk of transmitting pathogens that may cause viral infections and bacterial infections, transmission of prions, inflammatory reactions due to contamination with bovine proteins, and ethical issues with collection of animal products.11,12,15,17 The following alternatives have been considered: MSCs have been cultured successfully in autologous18,19 and nonautologous20,21 human serum, human platelet lysate,12,17,20 autologous cord blood serum (CS),20,22 and autologous cord blood platelet-rich plasma.23,24 Serum is collected from whole blood after it is left for a specific set time to clot and is then subsequently centrifuged.25,26 Special blood tubes are available for serum collection containing no anticoagulants and plasma collection containing anticoagulants. 26 Plasma is collected from whole blood by centrifugation, which can be followed by further centrifugation to remove platelets.26,27 Platelet-rich plasma is produced when the platelet pellet is resuspended in the plasma after centrifugation.24,27 Platelet lysate is produced when the platelet-rich plasma is taken through a number of freeze/thaw cycles.25,28,29 To our knowledge, serum taken from the blood of the Mother has not been investigated as a culture supplement for umbilical cord MSCs.
In this study, the aims were to (i) optimize a protocol for the isolation of umbilical cord matrix MSCs without the use of complicated digestion or dissection methods; (ii) investigate the use of pooled MS as a media supplement for isolation and culture of umbilical cord matrix MSCs; and (iii) demonstrate that the isolated cells are MSCs as defined by the Mesenchymal and Tissue Stem Cell Committee of the ISCT.
Materials and Methods
Ethics and samples
Umbilical cords and umbilical cord blood were collected from women undergoing elective caesarean section at full term (>37 weeks of gestation) at Singleton Hospital, Swansea. Women undergoing elective section for fetal or maternal anomalies were not recruited; therefore, samples were typically from women scheduled for caesarean section due to breech presentation, cephalopelvic disproportion, or emergency caesarean section at previous delivery. Maternal blood was collected from women in the 1–3 days leading up to their elective caesarean section. All samples were collected with informed written consent and ethical approval was obtained from the South West Wales Research Ethics Committee (REC No. 11/WA/0040). Serum was prepared by collecting blood into serum separation tubes (Greiner Bio-one, Gloucestershire, United Kingdom), allowing clotting for 90 min and centrifugation to collect serum, which was aliquoted and stored frozen at −80°C. After centrifugation, samples were processed aseptically in a class II tissue culture cabinet.
Umbilical cord collection and preparation
The placenta was collected at elective caesarean section and a 10–12 cm long piece of umbilical cord proximal to the placenta was excised within 2 h of delivery. This was washed in phosphate-buffered saline (PBS; Life Technologies, Paisley, United Kingdom) two to four times to remove excess blood. The piece of cord was then placed in Hank's Balanced Salt Solution (Life Technologies) and kept in the refrigerator until processing (2 h).
Optimizing MSC isolation protocol
Size of umbilical cord explants
An explant approach was taken to isolate MSCs from the umbilical cord. The effect on MSC yield of explant size at the initiation of culture was investigated first. Segments of cord measuring 2 cm were cut in half. Each pair of halves was then cut into (i) 6 pieces of equal size, (ii) 10 pieces of equal size, or (iii) multiple small pieces measuring <2 mm3. Pieces generated from each half were placed into individual T25 tissue culture flasks (two flasks/tissue size; Greiner Bio-One) with 4 mL low-glucose, phenol red-free DMEM supplemented with 1% glutamax, 10% FBS, 1% penicillin streptomycin fungizone (PSF) (100 U/mL penicillin, 100 μg/mL streptomycin, and 0.25 μg/mL amphotericin B), and 0.1% nonessential amino acids (NEAA) (all Life Technologies), hereafter called complete DMEM. This was designated as day 0. On day 2, an extra 2 mL of the same medium was added to each flask.
In parallel, another 2 cm segment of umbilical cord was cut in half, each half was chopped into small pieces (<2 mm3), placed into T25 flasks, and 500 μL of FBS was added. An hour later, 1 mL complete DMEM medium was added to each flask (designated day 0). A further 1 mL of medium was added to the flasks every day until day 5.
On day 8, the tissue and medium were removed from all flasks, the flasks were rinsed with PBS (Life Technologies), and fresh medium was added. On day 15, the cells were harvested and counted (as described in the section titled Cell harvesting and counting).
Serum used
FBS was compared with umbilical CS and pooled serum prepared from peripheral blood of women >37 weeks pregnant (pooled MS). Umbilical cord serum,20,22 umbilical cord platelet-rich plasma,23,24 and human serum (not from pregnant donors)18,20,21 have been reported elsewhere as a supplement in MSC isolation media. Segments of cord measuring 1 cm were cut in half, each half was chopped into small pieces (<2 mm3), and the small pieces were placed into six-well plates. FBS, CS, or MS was then added 250 μL/well in duplicate (not paired cord halves). After 1hr, 500 μL low-glucose phenol red-free DMEM supplemented with 10% FBS, CS, or MS (+ glutamax, PSF, and NEAA as above) was added and then 500 μL every day until day 3, to give a final volume of 2 mL in each well. On day 8, the tissue and medium were removed, each well was rinsed with PBS, and fresh corresponding medium was added. On day 15, the cells were harvested and reseeded in T25 culture flasks (one well to one T25 flask). On day 18, the cells were harvested and counted.
Cell harvesting and counting
For harvesting, the cells were first rinsed with PBS to remove any remaining medium and then detached using 0.05% Trypsin/ethylenediamine tetraacetic acid (Life Technologies) at 37°C for 8–10 min. Trypsin was neutralized by the addition of FBS containing medium. The cells were pelleted by centrifugation at 400g for 5 min. Cells were resuspended in complete medium and counted using a C-Chip disposable hemocytometer (Labtech International, East Sussex, United Kingdom).
Cell cryopreservation and resuscitation
Cells were cryopreserved in 1 mL of 10% dimethyl sulfoxide (DMSO) (Sigma-Aldrich, Dorset, United Kingdom) in complete DMEM with 1 × 106 cells per vial. Cryopreservation vials (2 mL, Greiner Bio-One) were placed in a Nalgene cryopreservation 1°C freezing container (Thermo-Scientific, Leicestershire, United Kingdom) containing 250 mL of 2-propanol (Sigma-Aldrich) at −80°C for 24 h with a decrease in temperature of 1°C/min. The vials were then transferred to liquid nitrogen storage.
For cell resuscitation, vials were removed from liquid nitrogen and warmed media were added to the vials gradually to thaw the cell suspension. Once thawed, the cell suspensions were transferred to larger vessels containing warmed medium. The cells were then pelleted by centrifugation at 400g for 5 min to remove any DMSO.
Cell characterization
Cell surface phenotype by flow cytometry
The phenotype of previously cryopreserved cells isolated using FBS, CS, and MS were investigated by incubating 1 × 105 cells with antibodies shown in Table 1 (all from eBioscience, Hatfield, United Kingdom), including markers used for phenotyping as set out by the ISCT 6 and an unstained control. The cells were incubated with preoptimized concentrations of antibody in the dark on ice for 30 min. After washing the cells with 0.2% bovine serum albumin/0.05% sodium azide in PBS, the cells were fixed (BD Cytofix; BD Biosciences, Oxford, United Kingdom) and acquired on a flow cytometer (FACS Aria I; BD Biosciences) within 24 h. Compensation was conducted using single stained cells for each fluorochrome used. Analysis of acquired data was undertaken using Kaluza Flow Cytometry Analysis software (version 1.2, Beckman Coulter). The signal indices were calculated by dividing the median fluorescence of the stained cells by the median fluorescence of the unstained cells.
Antibodies Used for Flow Cytometry
APC, allophyocyanin; FITC, fluorescein isothiocyanate; PE, phycoerythrin; HLA, human leukocyte antigen.
Differentiation
Adipogenesis
Cells were seeded at 3 × 103 cells per cm2 in a 24-well plate. After 5 days of culture, the media were removed and replaced with 500 μL/well adipogenesis differentiation medium (Adipocyte Differentiation Basal Medium supplemented with 10% Adipogenesis supplement, 1% PSF; Life Technologies). The media were replaced every 3–4 days. On day 16, the cells were fixed with 4% paraformaldehyde (Sigma-Aldrich) and stained with Oil Red O staining solution (300 mg Oil Red O powder (Sigma-Aldrich) in 100 mL 99% isopropanol (Fisher Scientific); 6 mL of this solution was added to 4 mL of distilled water, incubated for 10 min at room temperature, and then filtered through Whatman filter paper (Whatman International, Maidstone, United Kingdom).
Chondrogenesis
Cells were seeded at 1 × 105 cells in 5 μL droplets of low-glucose phenol red-free complete DMEM in the center of a well in a 24-well plate. After 2 h, 500 μL/well chondrogenesis differentiation medium (Chondrocyte Differentiation Basal Medium supplemented with 10% Chondrogenesis supplement, 1% PSF; Life Technologies) was added. The media were replaced every 2–3 days. On day 23, the cells were fixed with 4% paraformaldehyde (Sigma-Aldrich) and stained with Alcian Blue staining solution (1 mg Alcian Blue powder [Sigma-Aldrich] in 99 mL 0.1N hydrochloric acid, HCl [Sigma-Aldrich]).
Osteogenesis
Cells were seeded at 6 × 103 cells per cm2 in a 24-well plate. After 4 days of culture, the media were removed and replaced with 500 μL/well osteogenesis differentiation medium (Osteocyte Differentiation Basal Medium supplemented with 10% Osteogenesis supplement, 1% PSF; Life Technologies). The media were replaced every 3–4 days. On day 25, the cells were fixed with 4% paraformaldehyde (Sigma-Aldrich) and stained with Alizarin Red S staining solution (2 g Alizarin Red S powder [Sigma-Aldrich] in 100 mL distilled water and the pH was adjusted to 4.2).
Statistical analysis
Paired t-tests and analysis of variance (ANOVA) were performed on the results of the MSC isolation experiments using the SPSS statistical software package (version 19, IBM). A p-value <0.05 was considered significant.
Results
Optimizing the isolation protocol–size of umbilical cord explants
The number of putative MSCs isolated from the umbilical cord increases with decreasing size of the tissue explants (Fig. 1). However, the only significant difference (for pieces + media) was between 10 pieces of tissue and 6 pieces of tissue (p = 0.041; n = 3). Seeding <2 mm3 explants of tissue onto 500 μL FBS and then increasing the total volume of media in the flask gradually over the next 5 days yielded significantly more putative MSCs than seeding explants of the same size directly with 4 mL media (p = 0.011; n = 3; Fig. 1).
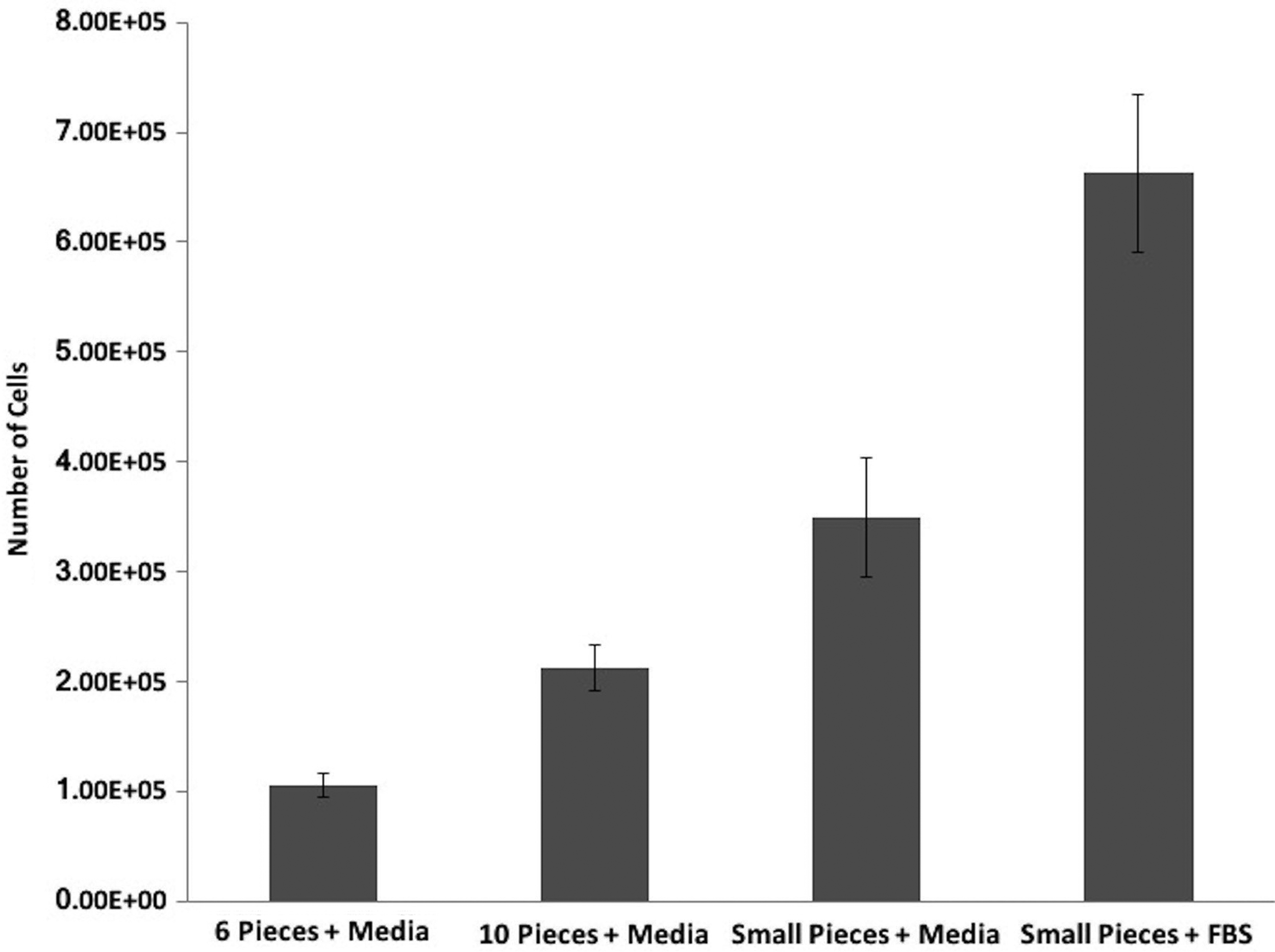
The effect of umbilical cord explant size on the yield of putative MSCs. Explants of umbilical cord of varying size were cut from the cord as detailed in the Materials and Methods section. Pieces were seeded into 4 mL complete DMEM with 2 mL additional media on day 2 or, in the case of small (<2 mm3) explants + FBS, pieces were seeded onto 500 μL FBS and then 1 mL media was added after 1 h and every day until day 5. On day 8, the tissue was removed, the media were replaced, and the putative MSCs were cultured for a further 7 days before harvesting by trypsinization and counting. All experiments were conducted in T25 culture flasks. Cell counts are shown as mean ± SEM. n = 3 different umbilical cords, each in duplicate. MSCs, mesenchymal stromal cells; DMEM, Dulbecco's modified Eagle's medium; FBS, fetal bovine serum; SEM, standard error of the mean.
Optimizing the isolation protocol–serum used
Having shown that seeding small explants onto a bed of FBS rather than into 4 mL complete medium increased the yield of putative MSCs, the possibility that different serum substrates might further improve cell yield was investigated. The substrates chosen were umbilical cord serum and pooled MS prepared from women who were >37 weeks pregnant. The use of pooled MS gave the greatest yield of cells (Fig. 2); significantly more than FBS (p = 0.004; n = 3) and more than cord serum, but not significantly so (p = 0.065; n = 3).

The effect of different sera used at seeding and as a medium supplement throughout culture on the yield of putative MSCs from umbilical cord explants. Small (<2 mm3) explants of umbilical cord were seeded onto 250 μL of FBS, pooled umbilical cord serum from full-term nonlabored deliveries, or pooled serum from women >37 weeks pregnant. After 1 h and then each day until day 3, 500 μL of media containing the same serum as used for seeding was added to each flask. On day 8, the tissue was removed and the media were replaced with fresh corresponding media. On day 15, the cells were harvested and reseeded before harvesting and counting on day 18. All experiments were conducted in six-well culture plates until day 15 and in T25 culture flasks from day 15–18. Cell counts are shown as mean ± SEM. n = 3 different umbilical cords, each in duplicate.
Characterization of umbilical cord matrix-derived cells
Plastic adherence
Irrespective of the substrate used for seeding and culture (FBS, cord serum, and pooled MS), the cells derived from the umbilical cord matrix explants were plastic adherent and had a fibroblast-like structure on day 18 (Fig. 3).
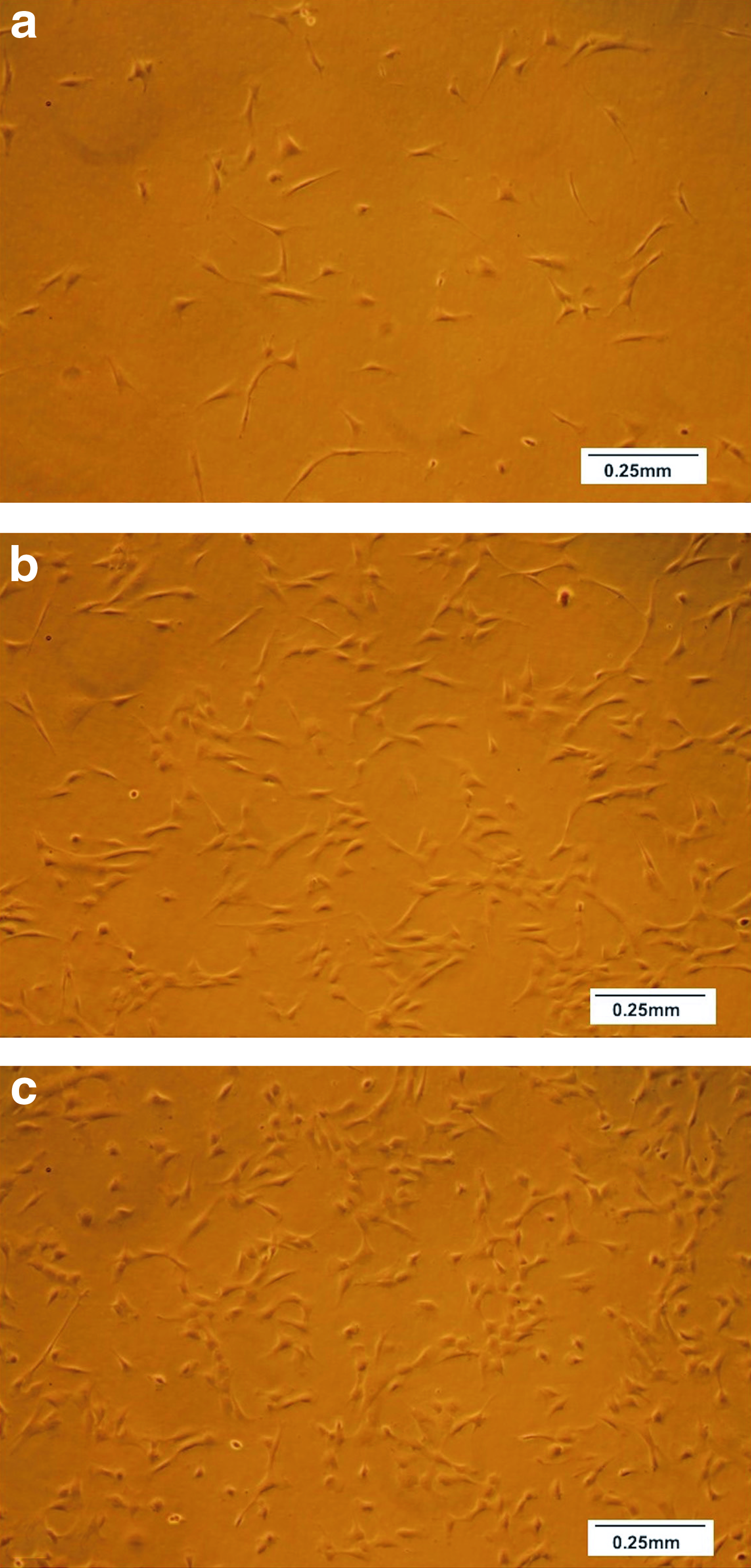
Plastic adherence of putative MSCs isolated from umbilical cord explants cultured in three different sera. Small (<2 mm3) explants of umbilical cord were seeded onto different sera and then cultured in medium supplemented with the same sera as described in the Materials and Methods section. On day 18, photomicrogrpahs were taken before harvesting and cryopreservation of the cells. Representative examples of six preparations of cells isolated using
Phenotype marker panel by flow cytometry
To confirm that irrespective of the serum used, the cells isolated were MSCs, cell phenotypes were studied using flow cytometry. The cells isolated using FBS, umbilical cord serum, or pooled MS were all negative for CD14, CD19, CD34, CD45, and HLA-DR (Fig. 4a) and were all positive for CD73, CD90, and CD105 (Fig. 4b). Overall, there were no differences in the level of expression of these markers on MSCs isolated using different sera with the exception of CD105, which was significantly higher on cells isolated using umbilical cord serum (p = 0.047; ANOVA; Fig. 4c).
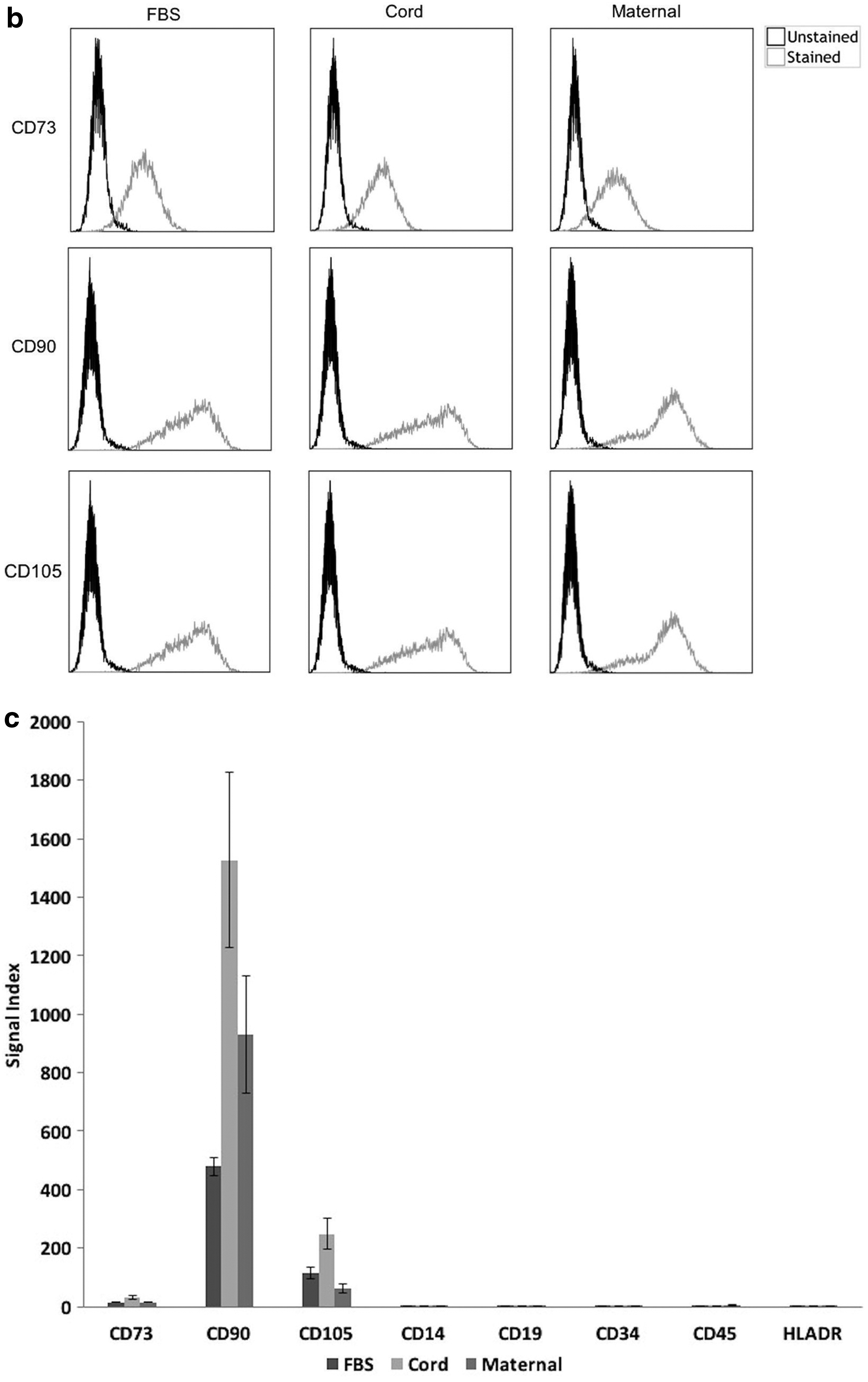
Phenotype of putative MSCs isolated from umbilical cord explants cultured in three different sera. Small (<2 mm3) explants of umbilical cord were seeded onto different sera and then cultured in medium supplemented with the same sera as described in the Materials and Methods section. On day 18, cells were harvested and cryopreserved; the cells were then resuscitated and stained for flow cytometry with fluorochrome conjugated antibodies to
Differentiation
Cells isolated using FBS, umbilical cord serum, and pooled MS were all able to undergo adipogenesis, chondrogenesis, and osteogenesis (Fig. 5).
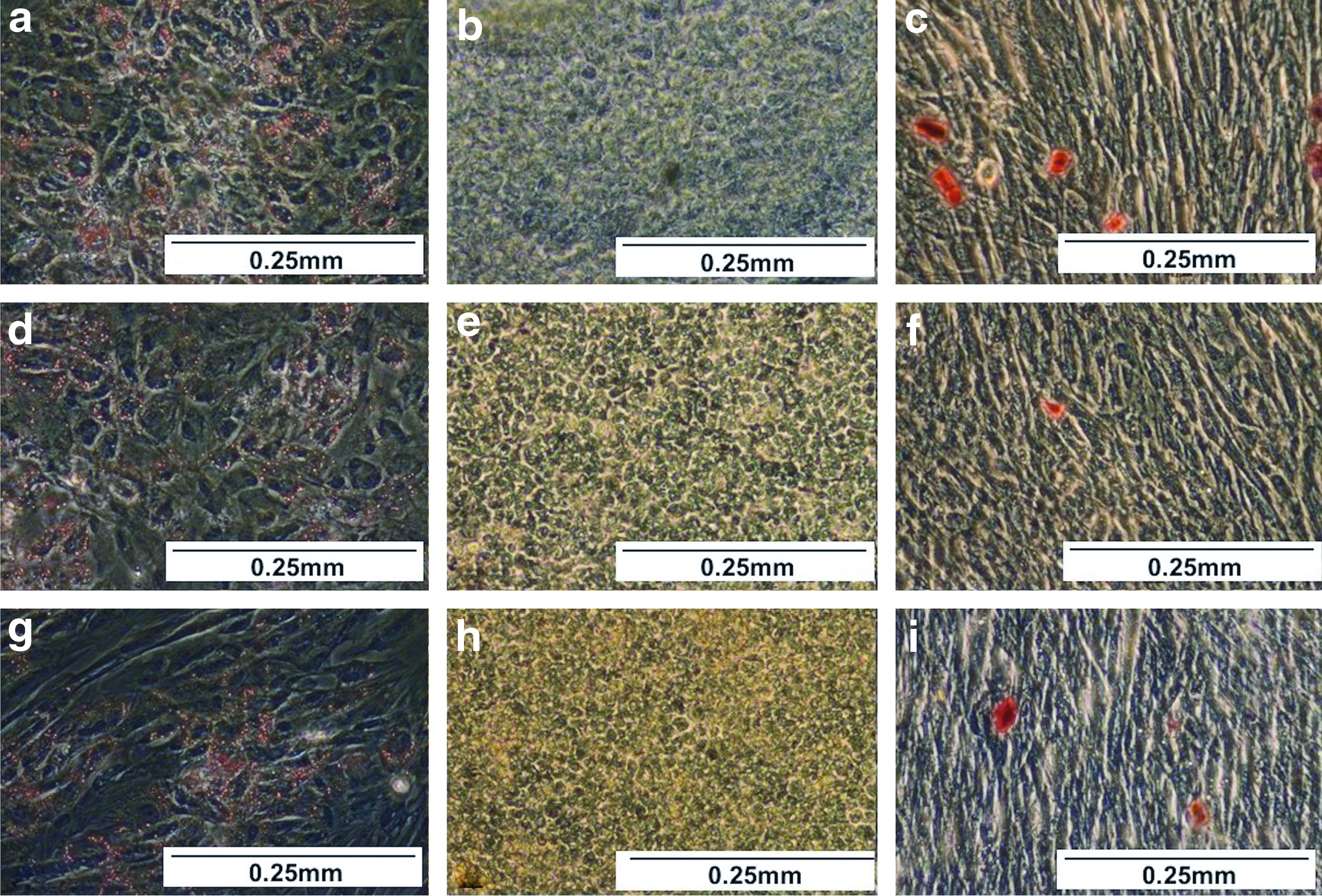
Differentiation of putative MSCs isolated from umbilical cord explants cultured in three different sera. Small (<2 mm3) explants of umbilical cord were seeded onto different sera and then cultured in medium supplemented with the same sera as described in the Materials and Methods section. On day 18, cells were harvested and cryopreserved; the cells were then resuscitated and adipogenesis, chondrogenesis, or osteogenesis was induced in the cells. After 16 days in adipogenesis differentiation medium, the cells were fixed and stained with Oil Red O, shown in
Table 2 summarizes the characterization results for the cells isolated using each of the three sera, confirming that they match the minimal criteria for MSCs as set out by the Mesenchymal and Tissue Stem Cell Committee of the ISCT. 6
Effect of Different Sera Selection on the Minimal Criteria for Defining Mesenchymal Stromal Cells as Set out by the International Society for Cellular Therapy
Discussion
In this study, we describe an explant method for isolation of MSCs from human umbilical cord matrix. The smaller the explant, the greater the yield, and seeding the explants on serum and gradually increasing the culture volume also enhanced yield. On comparing serum sources—FBS, umbilical CS, or serum from women >37 weeks pregnant—the latter gave the greatest yield of MSCs. Irrespective of the serum source used for seeding and media supplementation, the cells isolated from small explants of umbilical cord met the minimal criteria for MSCs based on surface marker expression and differentiation potential. 6
There is a belief that the minimal criteria set out by the Mesenchymal and Tissue Stem Cell Committee of the ISCT are no longer a robust enough method of determining MSC authenticity, 30 as they could be used to characterize fibroblastic cell strains. 31 Moreover, there are reports in the literature supporting a theory that transplanted MSCs themselves do not differentiate to form new tissue in vivo, but rather migrate to a site of injury or disease and secrete factors that stimulate the resident stem cells to construct new tissue. 32 This is clearly an important area for further research.
Nevertheless, the minimum criteria of the ISCT are still being used to define MSCs 33 as there has been no new guideline set out for MSC characterization. It is important to note, therefore, that even though our cells have met the minimal criteria, the true in vivo differentiation potential of these isolated cells remains unknown and is worth further investigation.
We have also demonstrated here that the cells met the minimum criteria through identification as being CD34 negative. There have been reports stating that MSCs are in fact CD34 positive.34,35 However, these reports also state that it has been demonstrated that any tissue-resident CD34-positive cells lose their expression after expansion in culture, which would account for our CD34-negative result. There may be CD34-positive MSCs within the umbilical cord matrix, but so far none has been identified.
An explant approach was chosen to avoid the limitations of introducing tissue digestion enzymes into the isolation procedure. The number of cells isolated from the umbilical cord increased with decreasing size of the tissue explants so that small pieces measuring <2 mm3 yielded the most. This approach likely increases the tissue surface area and enables more cells to migrate out of the tissue and onto the plastic surface of the culture flasks. Other authors similarly minced or cut the tissue into small pieces or fragments measuring around 1–5 mm2.5,12,16 We found that the cell yield could be increased further when the explants were first seeded onto a small volume of FBS for an hour, followed by the gradual addition of 1 mL of medium each day, rather than immediate seeding into culture media. The most likely explanation for this is exposure to increased concentrations of key factors, such as chemokines or growth factors, in the serum.
Given the need for alternative supplements to FBS for MSC culture, FBS was compared to cord serum and serum prepared from pregnant women (>37 weeks pregnant; full-term). After 18 days of culture, explants seeded on and cultured in pooled MS yielded more cells than either FBS or cord serum. This would suggest that pooled MS draws more cells from the explant and/or has a greater proliferative effect on the cells than FBS or cord serum, at least in the short term. While there are no reports comparing relevant mediator levels in FBS, cord, and serum from pregnant women, a number of studies highlight differences between serum from pregnant and not pregnant women. For example, TGFß1 is elevated in pregnant versus not pregnant women 36 and it would be worthwhile extending this phenotype to growth factors and cytokines with a role in MSC proliferation.
Alternative serum sources to FBS are needed to maximize the use of MSCs for clinical purposes, due to the risk of contamination, inflammatory reactions, and ethical issues.11,12,15,17 Alternative supplements have been used successfully, such as human serum,18–21 human platelet lysate,12,17,20 CS,20,22 and cord blood platelet-rich plasma.23,24 The difference between serum and platelet-rich plasma is that serum is collected from centrifuged whole blood that was left to clot,25,26 whereas platelet-rich plasma is collected when unclotted whole blood is centrifuged, the plasma is removed, and the platelet pellet is resuspended in the plasma.24,26,27 To our knowledge, the use of maternal blood serum has not been investigated. We now show that serum prepared from the blood of full-term pregnant women, with further investigation, has the potential to be an alternative to FBS for isolation and expansion of umbilical cord MSCs for clinical purposes. The use of serum prepared from the blood of full-term pregnant women would be more convenient than cord serum, especially where delayed cord clamping is employed. Its use does, however, pose other potential problems because the invasive nature of collection limits the volumes available from any one pregnant woman. Pooling of samples could overcome this; however, any immunological effect on the cells of pooling samples from different women would have to be investigated. Also, investigation of why serum from pregnant women had this effect is warranted and might identify a growth factor mix that could be used instead.
In conclusion, we have developed an umbilical cord matrix MSC isolation approach using small explants first seeded on pooled MS and then cultured in medium containing the same serum, which yields cells that meet the criteria of MSCs. While pooled MS gives the greatest yields, further work is required, including detailed investigation of how this affects MSC phenotype and function, especially the immunomodulatory properties of these cells. Further investigation is also needed into the characterizing of these cells, including by means of an in vivo transplantation.
Footnotes
Acknowledgments
The authors would like to thank the staff of the antenatal day assessment unit and the delivery suite at Singleton Hospital, Swansea, and the women who volunteered to donate samples. Ll.B.D. was supported by a Prince of Wales Innovations Scholarship.
Disclosure Statement
No competing financial interests exist.