
Abstract
The use of biomaterials and regenerative medicine has been well recognized as a promising means to repair dural defects. However, there have been few reports on preclinical large animal models of dural defects, which are crucial to evaluate the performances of dural repair materials. In addition, the methods of preparing animal models vary among studies. To ensure high-quality research results and prevent unnecessary financial losses, a standard method of animal model preparation needs to be established. In this study, we designed and evaluated three different surgeries (methods A, B, and C) involving different temporal muscle and skull incision techniques to prepare beagle dog dural defect model. It was found that method C was associated with an appropriate surgical duration and better postoperative recovery without obvious complications compared with methods A and B. Moreover, the surgical approach used in method C avoided the potentially dense vascular region in the cranial midline and retained an adequate blood supply for the temporal muscle. Our results suggest that method C is a safe and effective procedure that allows the preparation of a stable large animal model for studies on dural repair materials and regenerative medicine.
Impact Statement
Using biomaterials and regenerative medicine to repair tissue defects has been a very hot research field, during which the development of stable large animal models with appropriate biotechnology is crucial. Recently, more and more researchers are paying attention to dural defect repair. However, the lack of widely recognized stable large animal models has seriously affected the related further research. In this study, a stable large animal dural defect model is developed exactly for the first time. Therefore, the article would attract considerable attention and be highly cited after publication.
Introduction
Tissue defects healing is still a challenge in today's clinical routine, and the development of dural repair materials, an alternative to autologous dural grafting, is the current focus of interest. The dura mater is the toughest layer and plays a key role in protecting the brain tissue. 1 It is involved in not only complex metabolic processes and neuromodulation2–5 but also in the pathogenesis of many diseases.6–8 However, the integrity of the dura mater is often destroyed by conditions such as craniocerebral trauma, cancer, brain surgery, and congenital dysplasia, among others.9–11
For dural defects reconstruction, allografts have achieved the best theoretical results, but the source is limited. In view of the advantages of dural repair materials such as wide source, low price, and no potential virus infection, the utilization of these is a promising approach for repairing the defects and restoring functions. 12 An ideal dural repair material needs to possess good mechanical strength and excellent biocompatibility. For instance, the ideal repair material should have good toughness to withstand suture and excellent scaffold structure to promote the formation of new dura mater without adhesion to brain tissue. In addition, the chemical composition of materials should not induce an adverse body reaction and should be biodegradable and nontoxic.
The performance of dura repair materials should be evaluated by both in vitro and in vivo experiments before clinical trials. In vitro experiments provide information on cytotoxicity, genotoxicity, cell proliferation, and differentiation, but cannot establish a tissue response to the materials because of no systemic factors such as foreign body or immune system response, vascularization, oxygen and nutrient supply, and so on. 13 Therefore, animal models are essential for more comprehensively and accurately assessing the biocompatibility, tissue response, and repair effect of any dural repair materials before clinical application. However, there is still a lack of widely recognized stable animal models.
At present, animal models of dural defects are prepared using small animals or large animals. Small animal models are generally prepared in mice and rabbits, although details regarding the method of preparation in published studies remain unclear.14–17 In addition, the results of studies using small animal models are of limited value because the dura mater in these animals is small and the anatomical structure of the skull is significantly different from that of the human skull. Large animal models are usually prepared in dogs and pigs and provide a greater dural defect area. In addition, the anatomical structure of the skull in large animals is similar to that of the human skull. Therefore, these models reportedly simulated the actual conditions of human dural defects in previous studies in a better manner.18–21
Again, details of the modeling process for large animals were not clearly mentioned in these studies. For instance, the method of incising the scalp, temporal muscle, and skull was not described, and the shape and size of the skull flap and dural defects were inconsistent. Furthermore, in some studies, a risk of postoperative brain injury because of sharp and irregular edges of the skull window was observed.19,21 Consequently, the applicability of the findings of previous studies is limited because of nonreproducibility and nonuniformity of the modeling process.
To ensure high-quality research results and prevent unnecessary financial losses, a standard method of large animal model preparation for future studies on dural repair materials and regenerative medicine needs to be established. Therefore, in this study, we designed three different methods for the preparation of beagle dog dural defect model and evaluated the feasibility of each method.
Materials and Methods
Experimental animals and instruments
Twelve beagle dogs (1 year old, male or female, weight 9–10 kg) were randomly selected to undergo one of three surgical methods for the preparation of dural defects (method A, n = 4; method B, n = 4; method C, n = 4). All dogs were purchased from the Laboratory Animal Academy of Sichuan Medical Sciences Institute (license no. SCXK2004–15), and they received standard dog food and free access to water. This study was approved by the Animal Care and Use Committee of Sichuan University, and all animal experimental procedures met the recommendations for laboratory animal care established by the National Society for Medical Research.
The instruments used in our experiments included conventional surgical instruments (Shanghai Medical Instrument [Group] Co., Ltd, Surgical Instrument Factory, China), instruments for cerebral surgery (Xinhua Surgical Instrument Co., Ltd, China), microinstruments (Xinhua Surgical Instrument Co., Ltd), a high-frequency electric knife (Covidien, Tyco Healthcare International Trading [Shanghai] Co., Ltd, China), 4-0 absorbable sutures with needles (Shanghai Pudong Jinhuan Medical Products Co., Ltd, China), 3-0 silk sutures (Johnson & Johnson Medical [Shanghai] Ltd, China), the Strong 90/102 micromotor handpiece and control box (Saeshin Precision Co., Ltd, Korea) and diamond drills (Guangzhou Chinatrau Medical Instrument Co., Ltd, China).
Preoperative preparation
The animals were made to fast for 12 h before surgery. Each dog underwent surgery under general anesthesia, which was induced by intramuscular injections of atropine 0.04 mg/kg and ketamine 15 mg/kg and an intravenous injection of thiopental sodium 14–20 mg/kg, followed by isoflurane and oxygen inhalation for maintenance. After successful induction of anesthesia, the animal was fixed on the operating table in the prone position and the scalp was shaved. The surgical area was disinfected with iodophor and draped with sterile surgical towels.
Surgical procedures
Three different dural defect modeling procedures (methods A, B, and C) were designed on the basis of a review of previously described methods, pictures, and legends.18,20,22 Each of the three methods is described in detail hereunder.
Method A
Scalp incision
First, the scalp (skin, superficial fascia, and galea aponeurotica) was longitudinally incised along the skull midline; the incision length was ∼8 cm. Then, the scalp and subgaleal connective tissue were carefully separated using the high-frequency electric knife, and the subgaleal connective tissue was exposed after the scalp flaps were retracted on both sides. Finally, the temporal muscles were exposed after the subgaleal connective tissue was longitudinally incised along the cranial midline and the flaps were retracted on both sides (Fig. 1A).
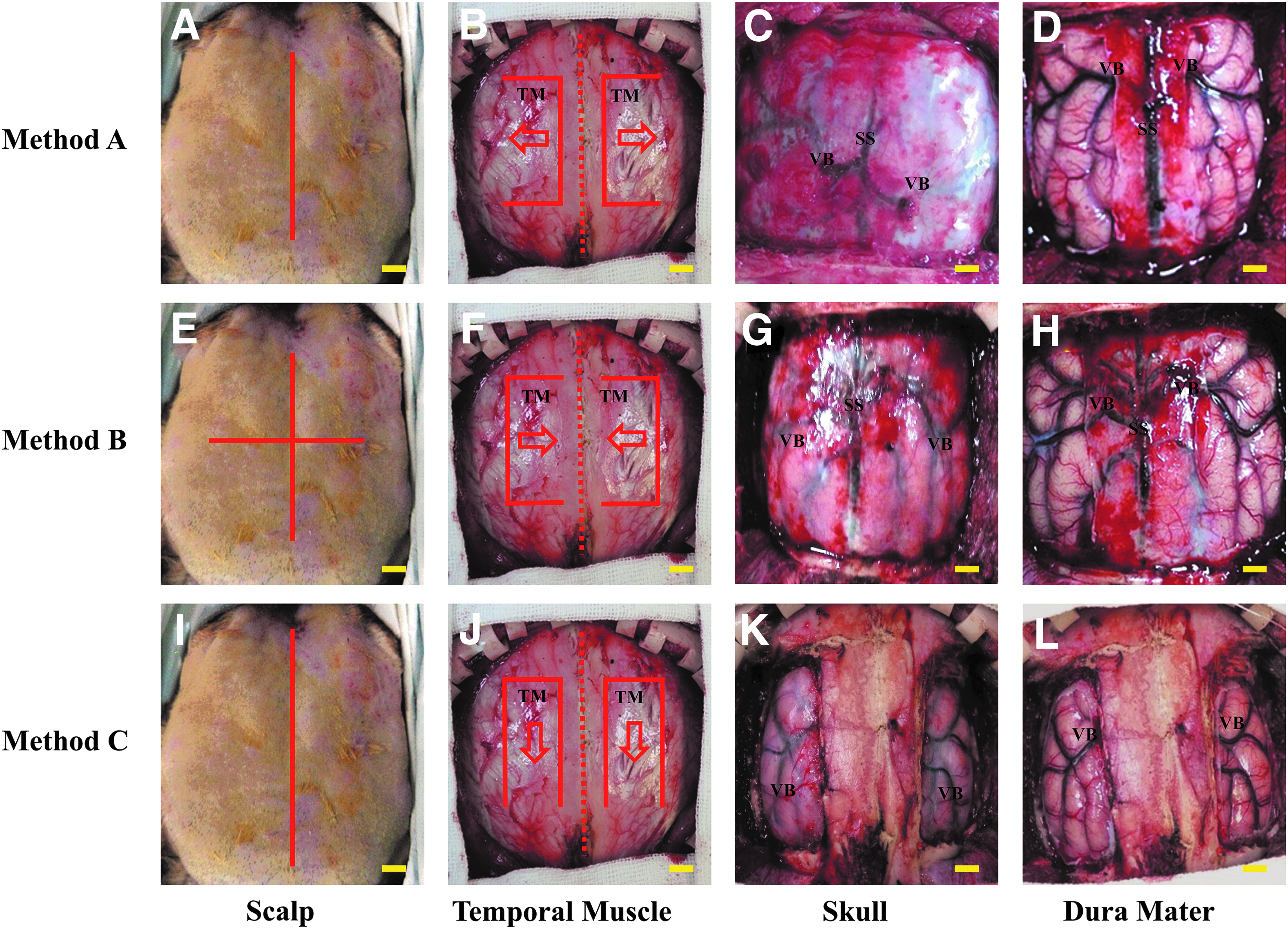
The three methods used for the preparation of a dural defect model in beagle dogs.
Temporal muscle incision
First, the temporal muscles were longitudinally incised for ∼6 cm along the medial origin (0.5 cm from the centre of the skull), with the upper edge of both incisions placed 1.5 cm from the eyebrow. Then, at the upper and lower edges of the incisions, the muscles were incised in a mediolateral direction for ∼3.5 cm. Subsequently, the temporal muscles and the skull were carefully separated, and temporal muscle flaps were pulled to the lateral side. Finally, the electric knife was used for careful hemostasis and the surface of the skull was exposed (Fig. 1B).
Skull incision
The upper edge of the skull window was placed 1.5 cm from the eyebrows, whereas the left and right borders were 3.5 cm from the median line of the skull. The length of the longitudinal side was ∼4 cm. Then, the entire skull flap was carefully drilled and removed according to the marked window to achieve a 4 × 7 cm rectangular skull defect (Fig. 1C).
Dura mater incision
First, the upper margins of two dural defect windows were placed 0.5 cm from the edge of the skull, whereas the left and right edges were placed 0.5 and 2.0 cm, respectively, from the median line of the skull. This would prevent damage to the vascular branches of the superior sagittal sinus. The length of the longitudinal side was ∼3 cm. Finally, without damage to the arachnoid membrane, the dura mater was carefully cut and removed according to the marked boundaries to achieve two 1.5 × 3.0 cm rectangular dural defects on both sides of the cranial midline (Fig. 1D).
Method B
Scalp incision
First, the scalp was longitudinally incised along the midline of the skull; the length of the incision was ∼8 cm. Then, a 6 cm long transverse incision was placed at the midpoint of the longitudinal incision. The remaining surgical procedure was the same as method A (Fig. 1E).
Temporal muscle incision
Compared with method A, temporal muscle flaps were pulled to the central side in method B (Fig. 1F). The rest of the operation was similar to method A.
Skull incision
The size of the skull window defect in method B was the same as the defect in method A (Fig. 1G). To reduce the operation time, only one side of the skull window was drilled completely, and the remaining three sides were drilled by two-thirds and the other part was pierced with a bone knife.
Dura mater incision
Compared with the edges of dural defect windows in method A, the left and right edges of defect windows in method B were placed 1.0 and 2.5 cm, respectively, from the median line of the skull. This would avoid damage to the vascular branches of the superior sagittal sinus. Two 1.5 × 3.0 cm rectangular dural defects were also made on both sides of the cranial midline (Fig. 1H).
Method C
Scalp incision
The length of the incision was ∼12 cm and the remaining surgical steps were the same as method A (Fig. 1I).
Temporal muscle incision
Compared with methods A and B, temporal muscle flaps were retracted to the trailing end of the skull (Fig. 1G). The size of temporal muscle flaps in three methods was the same.
Skull incision
Two 3 × 4 cm rectangular skull window defects were made on the left and right sides of the cranial midline (Fig. 1K). The operation method of craniotomy was similar to that of method B.
Dura mater incision
Two 1.5 × 3.0 cm rectangular dural defects were made on both sides of the cranial midline according the procedure described in method B (Fig. 1L).
Incision closure
After resection of the dura mater, no material or autologous dura mater was used to repair the defect. Then, the skull flap and the surrounding intact skull were fixed with sutures. After rinsing the incision area with saline, the temporal flaps and the scalp flaps were sutured back in situ. Finally, the stitched wound was sterilized and wrapped with gauze.
Postoperative treatment and observation of experimental animals
All animals were fed in individual cages and administered cefazolin (500 mg intravenously) once a day for 3 days after surgery. The surgical duration was recorded for all dogs. Wound healing, diet, urination and defecation, mental state, and motor function were also recorded daily after surgery for all dogs.
If the food intake of dogs was decreased, glucose in normal saline (GNS) was administered. If the diet still did not improve, an intravenous GNS drip was administered. For symptoms such as irritability, malaise, and vomiting, mannitol, antibiotics, and sedatives were intravenously administered. Rehydration measures and nutritional support were provided for sick dogs.
In case of exudation from the wound or seroma or infection development, timely debridement surgery was performed. If the animal died after surgery, an autopsy was immediately performed to investigate whether death was associated with the surgical procedure.
Macroscopic and histopathological observations
At 1, 2, 3, and 6 months after surgery, dogs were killed by barbiturate overdose. After killing, specimens were obtained for macroscopic examinations, including observation of tissue adhesion (to the brain or cranium). Then, the specimens were fixed in 10% neutral-buffered formalin and subjected to hematoxylin and eosin and Masson's trichrome staining procedures for histopathological analysis. To analyze the level of inflammatory cell infiltration in the specimen, immunohistochemical staining was performed on the paraffin section. The primary antibody used in this study was anti-CD68 (1:2000; abcam/ab125212; Cambridge, MA). The specimens were then incubated with goat anti-rabbit (abcam/ab205718) second antibodies conjugated with horseradish peroxidase for 0.5 h. 3,3′–diaminobenzidine solution was used to visualize inflammatory cell infiltration.
Statistical analysis
All variables were coded as continuous data and presented as mean ± standard deviation. The data were analyzed using one-way analysis of variance (ANOVA) with Tukey's test to determine differences between groups. Values of p < 0.05 were considered statistically significant. Statistical analysis was performed using GraphPad® Prism 7 (GraphPad Software, Inc., La Jolla, CA).
Results
Intraoperative findings, surgical duration, and postoperative recovery
Method A
Surgery was successfully completed in an average duration of 6.5 h with method A. However, because of poor skull exposure and short incisions on the scalp and temporal muscles, the incisions and sutures in the skull and dura mater were obstructed by the scalp and temporal muscle flaps. In addition, a few vascular branches of the superior sagittal sinus were present near the cranial midline and were mainly distributed ∼0.5 cm from the midline. Therefore, a distance of >0.5 cm between the dura mater incision and cranial midline was considered adequate to prevent damage to these vascular branches.
All four dogs exhibited a normal diet and normal urination and defecation. Although two dogs exhibited a poor mental state for 2 days after surgery, they gradually recovered by the third day without any special treatment. The wound healed well within 1 week after surgery in all dogs, with no infection, seroma, or other abnormal conditions (Fig. 2A, B).
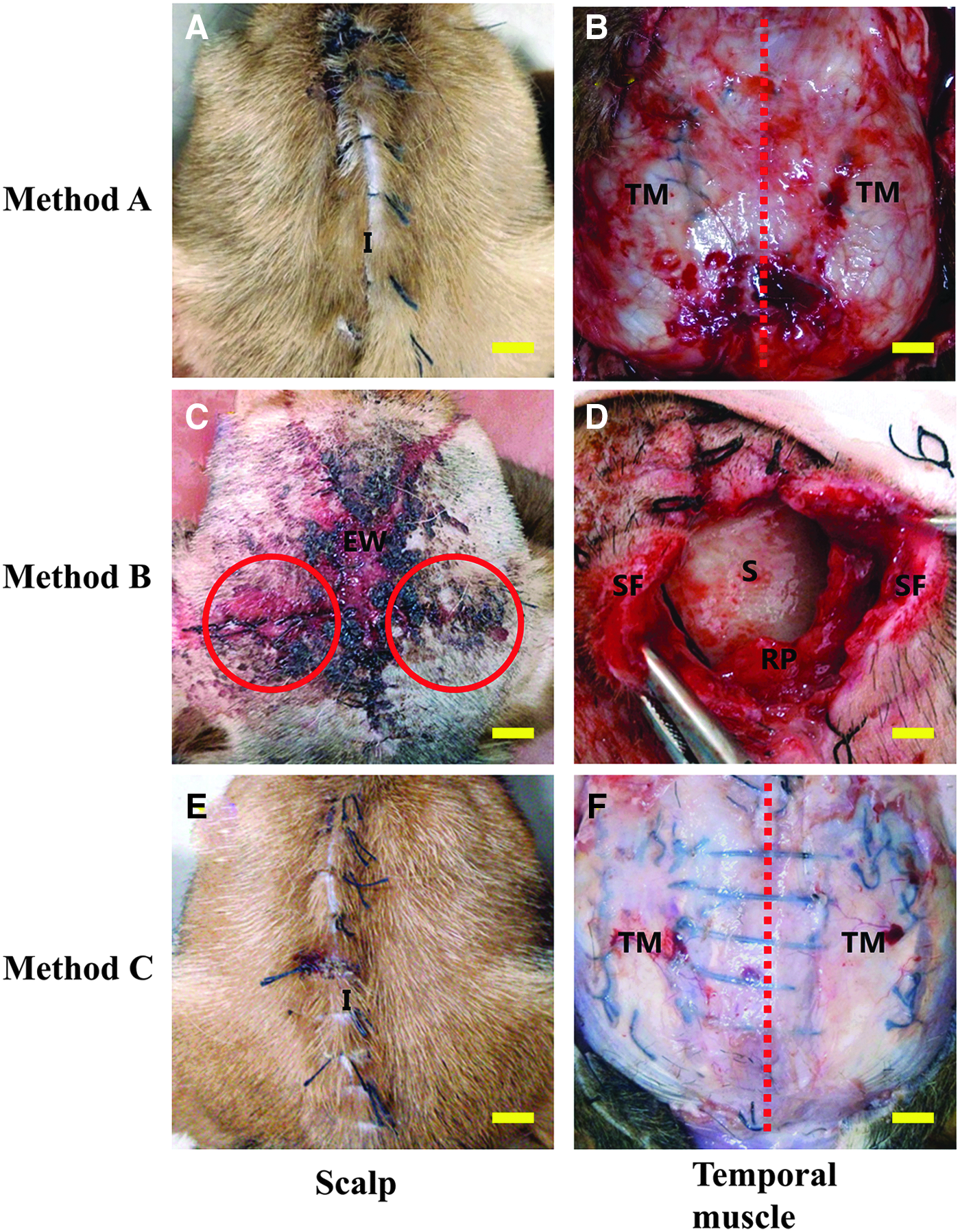
Wound healing after dural defect preparation using three different methods in beagle dogs. The scalp and temporal muscle incisions recovered well after the surgery with method A (a,b). However, exudation from the scalp incision and temporal muscle necrosis were observed after the surgery with method B (c,d). The scalp and temporal muscle incisions recovered well after the surgery with method C.
Method B
Surgery was successfully completed in an average duration of 3.0 h with method B. The incisions on the scalp and temporal muscles were long enough and the skull was well exposed; therefore, there were no obstructions when the skull and dura mater were cut and sutured. At the cranial midline in two dogs, there was a vein between the dura mater and skull, and there was a possibility of rupture and uncontrolled bleeding during removal of the skull flap. Furthermore, several vascular branches of the superior sagittal sinus were present near the cranial midline in two dogs, and most of these were distributed ∼0.5 cm from the cranial midline. A few branches were also present between 0.5 and 1.0 cm from the cranial midline. Therefore, a distance of >1.0 cm between the dura mater incision and cranial midline was considered adequate to prevent damage to the vascular branches.
Two of the four dogs exhibited a poor mental state and diet for 3 days after surgery, whereas one exhibited irritability and vomiting for 4 days after surgery. These dogs gradually recovered with nutritional support and symptomatic treatment (including mannitol, antibiotics, and sedatives). However, the wounds in three dogs exhibited an excessive amount of reddish exudate and did not heal. Moreover, seromas with fluctuation developed under these wounds. The necrotic temporal muscles were treated with timely debridement surgeries, following which the wounds in all three dogs showed gradual healing (Fig. 2C, D).
Method C
Surgery was successfully completed in an average duration of 3.5 h with method C. The incisions on the scalp and temporal muscles were long enough and the skull was well exposed; therefore, there were no obstructions when the skull and dura mater were cut and sutured. In addition, because the width of the remaining intact skull at both sides of the cranial midline was ∼0.5 cm, a distance of >0.5 cm between the boundaries of the skull defect and dura mater incision was considered adequate to prevent damage to the dense vascular area. Therefore, the dura mater incision was not affected by the vascular branches of the superior sagittal sinus.
All four dogs exhibited a normal diet and normal urination and defecation. In addition, the wounds healed well within 1 week after surgery in all dogs, with no infection, seroma, or other abnormal conditions (Fig. 2E, F).
Macroscopic observation
Different degrees of adhesion existed at the boundary of the defects at 1, 2, 3, and 6 months after surgery with each method. Generally, adhesions at the surface facing the skull were more severe than those at the surface facing the brain. However, the degree of adhesion at the same time point showed no significant differences among the three methods (Fig. 3).

Macroscopic observation of tissue adhesion after dural defect preparation using three different methods in beagle dogs. The adhesions existed at the boundary of the defect areas at 1, 2, 3, and 6 months after surgery with methods A, B, and C. However, the degree of adhesion at the same time point showed no significant differences among the three methods. (a: normal dura mater, b: tissue adhesion, c: cerebral cortex, scale bar = 200 μm.) Color images are available online.
Histopathological observation
At 1, 2, and 3 months after surgery, the arachnoid membrane and pia mater were clearly intact. There was no obvious necrosis of the brain tissue and no inflammatory cell infiltration at the surfaces of the arachnoid membrane and pia mater (Fig. 4). At 6 months after surgery, the arachnoid membrane and pia mater were thickened without inflammatory cell infiltration (Fig. 4). For immunohistochemical staining, the deprivation of the primary antibody CD68 was used as the negative control. The porcine small intestinal submucosal material used for dural repair in dogs was used as the positive control. Positive staining for CD68 was observed in macrophage around the porcine small intestinal submucosal material (Fig. 5). However, at 1, 2, 3, and 6 months after surgery with methods A, B, and C, no significant macrophage infiltration was found in the arachnoid membrane and pia mater (Fig. 5).
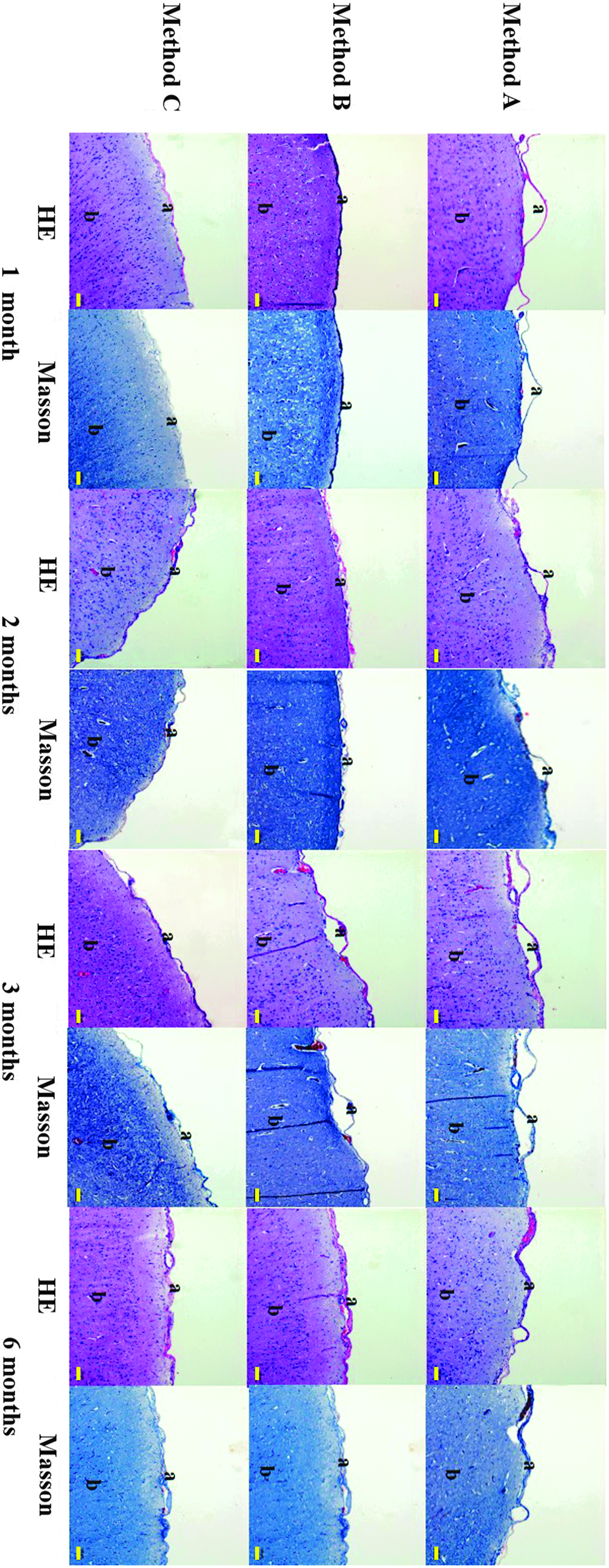
Histopathological staining after dural defect preparation using three different methods in beagle dogs. The arachnoid membrane and pia mater were clearly intact at 1, 2, and 3 months after surgery, without necrosis of brain tissue or inflammatory cell infiltration. At 6 months after surgery with methods A, B, and C, the arachnoid membrane and pia mater were thickened, without inflammatory cell infiltration. (a: intact arachnoid membrane and pia mater, b: cerebral cortex, scale bar = 100 μm.) Color images are available online.

Immunohistochemical staining of CD68 after dural defect preparation using three different methods in beagle dogs. Positive staining for CD68 was observed in macrophage at the implanted small intestinal submucosal material (as the positive control). At 1, 2, 3, and 6 months after surgery with methods A, B, and C, no significant macrophage infiltration was found in the arachnoid membrane and pia mater. (a: intact arachnoid membrane and pia mater, b: cerebral cortex, red arrow: macrophage, scale bar = 50 μm.) Color images are available online.
Discussion
Lack of widely recognized stable large animal models has seriously limited the development of dural repair materials. In this study, we designed three different methods for the preparation of an animal model of dural defects and evaluated the feasibility of each method in beagle dogs. Through comparative studies, a reproducible and feasible method to prepare a large animal dural defect model for preclinical biomaterial and regenerative medicine studies was established.
At present, in most studies on dural defect repair, the methods of incising the temporal muscle are described in a very basic manner; moreover, the specific surgical processes are unclear.23,24 In this study, however, we specifically focused on the temporal muscle and skull incision techniques during surgery for the creation of dural defects in beagle dogs. We found that the incision technique considerably influenced the surgical procedure and duration and postoperative recovery. Specifically, method C allowed for satisfactory skull exposure and maximum preservation of the temporal muscle blood supply compared with methods A and B. Thus, ischemic necrosis of the temporal muscles can be avoided with method C.
In previous studies, the skull defects were prepared by one of the two incision techniques. In one technique, most of the parietal bone and part of the frontal and occipital bones were removed to achieve a large rectangular defect at the top of the skull.23,25 This technique was similar to methods A and B in this study. In the other technique, two small, independent skull defects were created on the left and right sides of the cranial midline 22 ; this method was similar to method C in our study. Although the scalp, temporal muscle, and skull incision techniques differed among the three methods in our study, the dural defects were prepared using the same technique.
In this study, method C exhibited the following advantages compared with methods A and B. First, a dense vascular region near the cranial midline was observed during exploration with methods A, B, and C, and the range of the region was wider (∼1–2 cm). Method C provided an adequate width of the remaining skull at the cranial midline, which prevented injury to the vascular area when the skull was cut. Moreover, the dural incision was not affected by the vascular area. Second, the surgical duration was decreased when the skull was drilled completely on only one side of the skull flap, whereas two-third of the entire skull layer on the other three sides was drilled and the remaining one-third was pierced with a bone knife. Third, because the skull defects on the left and right sides of the cranial midline are relatively independent, different materials can be used to repair the dura mater, with no interaction between materials.
In previous studies, it was unclear whether the skull flaps should be returned to their original position after preparation of the dural defects.17,21 In this study, restoration of the skull flaps to their original position was found to be beneficial for the protection of brain tissue and anatomical support. Furthermore, the size and shape of dural defects were inconsistent in previous studies.14,19,21,22 The rectangular defects prepared in this study were regular in shape, which simplifies calculation of the defect area and the placement of materials.
With regard to postoperative symptoms such as irritability, apathy, and vomiting, the reason for these complications was cerebrospinal fluid leakage. There are many possible reasons for this leakage. First, the dura mater was not repaired and the arachnoid membrane was damaged during surgery. Second, the arachnoid membrane itself was permeable and slowly released a small amount of cerebrospinal fluid. Third, the dogs became restless and disturbed after surgery, which caused friction between the arachnoid membrane and the rough inner surface of the skull to result in cerebrospinal fluid leakage. In all our dogs, the complications associated with cerebrospinal fluid leakage gradually resolved with treatment.
With regard to postoperative tissue adhesion, a certain degree of adhesion was observed at the edge of the dural defects prepared by all three methods. These adhesions resulted in a closed space between the arachnoid membrane and skull, which stopped the cerebrospinal fluid from leaking. If the defects had been repaired using dural substitutes, the complications and degree of adhesion would have decreased, occasionally with no obvious adhesions at the edge of the dural defect.9,18,20
Finally, histopathological analysis showed that the arachnoid membrane and pia mater were intact and there was no obvious inflammatory reaction or necrosis of brain tissue at 1, 2, and 3 months after surgery. However, hyperplasia of the arachnoid membrane was observed at 6 months after surgery; this indicated that the arachnoid membrane thickens to protect the brain tissue together with the pia mater after removal of the dura mater.
However, there were three limitations in our study. First, the sample size was small and the sex or age of the dogs may have had an impact on the experimental results. Second, the preoperative and postoperative cognitive functions of the dogs were not evaluated. Third, there was no use of electroencephalography to evaluate complications such as epilepsy. At present, we are trying to evaluate different materials in dural regeneration by our established dural defect model. Our preliminary results show that the model established by method C is stable and the operation process of material repair is standardized (Supplementary Fig. S1). We believe that more scientific evaluation results of biomaterials and regenerative medicine for dural defect repair by our established stable large animal model will be presented in near future.
In conclusion, our results suggest that method C is a safe, effective, feasible, and reproducible procedure that allows the preparation of a stable large animal model for preclinical efficacy evaluation of dural repair materials and regenerative medicine.
Footnotes
Acknowledgments
This work was supported by grants from the National Key R&D Program of China (Nos. 2017YFC1104702 and 2017YFC1104703), 1.3.5 project for disciplines of excellence, West China Hospital, Sichuan University (No. 2YJC18002), State Key Laboratory of New Ceramic and Fine Processing (Tsinghua University), Fund of Key Laboratory of Advanced Materials of Ministry of Education (Tsinghua University), and the 111 Project (No. B13003).
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.