
Abstract
In vivo
liver decellularization has become a promising strategy to study in vivo liver engineering. However, long-term survival after in vivo liver decellularization has not yet been achieved due to anatomical and technical challenges. This study aimed at establishing a survival model of in vivo partial liver lobe perfusion-decellularization in rats. We compared three decellularization protocols (1% Triton X100 followed by 1% sodium dodecyl sulfate [SDS], 1% SDS vs. 1% Triton X100, n = 6/group). Using the optimal one as judged by macroscopy, histology and DNA content, we characterized the structural integrity and matrix proteins by using histology, scanning electron microscopy, computed tomography scanning, and immunohistochemistry (IHC). We prevented contamination of the abdominal cavity with the corrosive detergents by using polyvinylidene chloride (PVDC) film + dry gauze in comparison to PVDC film + dry gauze + aspiration tube (n = 6/group). Physiological reperfusion was assessed by histology. Survival rate was determined after a 7-day observation period. Only perfusion with 1% SDS resulted in an acellular scaffold (fully translucent without histologically detectable tissue remnants, DNA concentration is <2% of that in native lobe) with remarkable structural and ultrastructural integrity as well as preservation of main matrix proteins (IHC positive for collagen IV, laminin, and elastin). Contamination of abdominal organs with the potentially toxic SDS solution was achieved by placing a suction tube in addition to the PVDC film + dry gauze and allowed a 7-day survival of all animals without severe postoperative complications. On reperfusion, the liver turned red within seconds without any leakage from the surface of the liver. About 12 h after reperfusion, not only blood cells but also some clots were visible in the portal vein, sinusoidal matrix network, and central vein, suggesting physiological perfusion. In conclusion, our results of this study show the first available data on generation of a survival model of in vivo parenchymal organ decellularization, creating a critical step toward in vivo organ engineering.
Impact Statement
Recently, in vivo liver decellularization has been considered a promising approach to study in vivo liver repopulation of a scaffold compared with ex vivo liver repopulation. However, long-term survival of in vivo liver decellularization has not yet been achieved. Here, despite anatomical and technical challenges, we successfully created a survival model of in vivo selected liver lobe decellularization in rats, providing a major step toward in vivo organ engineering.
Introduction
Recently, decellularization using detergents has become an attractive technique that is widely used in tissue engineering studies. This technique is applied to fabricate a biological nonimmunogenic acellular matrix, which can be used for further generation of an engineered tissue or organ. The potential applications of decellularized matrix followed by recellularization have been demonstrated for a variety of tissues, including trachea,1,2 esophagus, 3 bladder,4,5 blood vessel,6–8 skin, 9 and cartilage. 10 However, only some ex vivo engineered structural tissues, for example, cartilage, 10 bladder, 4 and skin 11 but not functional organs, for example, lungs, hearts, or livers, have already been clinically used to treat patients.
Liver engineering has been emerging as a research hot spot around the world owing to the increasing demand of transplantable grafts for patients who need liver transplantation. However, researchers mainly study ex vivo liver engineering.12–17 Most of the transplantation studies used acellular or repopulated scaffolds for heterotopic transplantation to assess biocompatibility in the respectively selected functional aspects.18–22 However, neither biliary duct (BD) nor hepatic artery (HA) was orthotopically anastomosized to the recipient. The maximally reported observation time was limited to 72 h only.23,24 By far, orthotopic transplantation of an ex vivo repopulated full liver graft has not yet been reported. Long-term function and transplantation of engineered organs are still a vision. Therefore, an alternative methodology for studying liver engineering ex vivo is required. 25
Besides ex vivo liver engineering, in vivo liver engineering may represent a promising strategy to study hepatic repopulation under physiological conditions. The advantages of in vivo partial liver engineering compared with ex vivo liver engineering are as follows: First, in contrast to ex vivo perfusion with artificial culture medium, the in vivo repopulated partial liver scaffold can receive physiological blood perfusion maintaining the organ at the physiological temperature, ensuring the needed amount of oxygen and growth factors. 25 Second, BD and HA are naturally preserved, in contrast to implantation of ex vivo engineered liver lobes without anastomosis of either BD or HA, as reported by other authors.20,23,26 Last and most importantly, the remaining normal liver lobes maintain hepatic function, allowing long-term survival. 25 Pan et al. 27 tried in vivo decellularization and recellularization of the right inferior lobe in rats. However, all experimental animals were sacrificed after only 6 h of intraoperative observation time in their trial. They claimed that the short lifespan of the animals may be due to the injury caused by the detergent used. 27 Postoperative survival has not yet been reported till date.
Before in vivo liver lobe engineering, survival after in vivo perfusion decellularization of a selected liver lobe is a prerequisite. Three main challenges need to be addressed: (1) Owing to the complicated intrahepatic vascular anatomy, the first challenge is to properly isolate the selected liver lobe and generate a fluid circuit bypass only through the isolated lobe, compromising portal perfusion or venous drainage of the nonselected liver lobes. (2) Since the maximal operation time for an in vivo liver lobe perfusion should not exceed 5 h, 25 the second challenge is to identify a time-efficient in vivo decellularization protocol not exceeding 2 h. Doing so is the prerequisite for later reseeding and cell settlement, which might take another 2 h, leading to a total procedure time of about 5 h for liver engineering. (3) To prevent intra-abdominal corrosive injury by the detergent, the third challenge is to cover all other organs and tissues and drain the waste fluid without any contamination of the abdominal cavity.
Therefore, to establish survival after in vivo liver lobe perfusion decellularization, three critical subgoals need to be accomplished: One is to achieve perfusion of the targeted liver lobe without blocking the vena cava and the main portal vein (PV) for a long period. In our previous study, we already accomplished this goal. 25 Second is to limit the decellularization time to 2 h. Third is to prevent the animal from chemical injury owing to detergent contamination during in vivo decellularization.
To limit the decellularization duration, identifying a proper protocol for in vivo decellularization that allows maintaining scaffold structure and preserving matrix proteins is critical. Detergents frequently used for ex vivo liver decellularization include Triton X-100, sodium dodecyl sulfate (SDS), or Triton combined with SDS.12–18,24,28–30 The concentration of the Triton X-100 solution used for organ perfusion ranges from 0.5% up to 3% and the SDS solution ranges from 0.01% to 1%.15,20,31–35 Similarly, the decellularization time also ranges from hours up to several weeks.14,19,34,35,36,37 The flow rate employed in the protocols ranges from 1 to 200 mL/min, depending on the species.15,16,20,38–40 In our previous study on ex vivo liver decellularization in rodents, we used 1% SDS followed by 1% Triton as detergents for ex vivo liver lobe decellularization in mice and obtained an intact extracellular matrix (ECM) within only 3 h of the perfusion period. 21 To minimize the in vivo decellularization duration to not >2 h, here we tried to compare three decellularization protocols of using the combination of 1% SDS followed by 1% Triton X100, 1% Triton X100 only, and 1% SDS only, to identify the ideal in vivo partial liver lobe perfusion decellularization protocol in rats.
To prevent chemical damage during in vivo decellularization, looking for an efficient drainage method to prevent contamination of the abdominal organs with the detergent is also important. However, no report has been published about drainage optimization during in vivo decellularization. Preventing detergent from leakage into the abdominal cavity resulting in damaging other organs is rather challenging due to the difficulty of isolating the uneven surface of the abdominal cavity and other organs from the decellularized lobe. Therefore, here we also tried to create a novel isolation and sufficient drainage method for in vivo partial liver lobe decellularization.
In brief, in a previous study we achieved the establishment of the selected liver lobe perfusion technique. 25 We here further compared three in vivo liver lobe decellularization protocols and two drainage methods to identify the ideal partial liver decellularization protocol. The key steps for the procedure are illustrated in Figure 1.

Scheme of identification of an ideal protocol for survival model of in vivo partial liver lobe decellularization in rat liver. CT, computed tomography; EvG, Verhoeff-Van Gieson; H&E, hematoxylin and eosin; IHC, immunohistochemical; LLL, left lateral lobe; SEM, scanning electron microscopy. Color images are available online.
Materials and Methods
Animals
In total, 43 male Lewis rats (aged at 11–13 weeks) were used (Table 1). All protocols were approved by The Thüringer Landesamt für Verbraucherschutz, Thuringia, Germany (Reg. No: UKJ-17-031) and conform to European guidelines on Care and Use of Laboratory Animals.
Rats Used for Establishment of In Vivo Partial Liver Lobe Decellularization
CT, computed tomography; LLL, left lateral lobe; SDS, sodium dodecyl sulfate; SEM, scanning electron microscopy.
Experimental design
The experiment was performed in three steps: (1) Small modifications of the selective perfusion technique to adjust it for in vivo decellularization (n = 3). (2) Identification of optimal protocol for in vivo selective liver lobe decellularization and characterization of the scaffold quality (n = 25). (3) Prevention of contamination to abdominal cavity caused by the detergent (n = 12) and histological assessment after postoperative 12 h for confirmation of short-term physiological perfusion (n = 3).
Modification of selective perfusion technique to make it suitable for in vivo decellularization
Before decellularization, the rats (n = 3) underwent a surgical circuit bypass only through the left lateral lobe (LLL) based on small modifications of the perfusion technique previously reported. 25
In contrast to the previous study, where a suture ligation was used, here the left PV was blocked with micro-clamps (Fig. 2A). This facilitated the insertion of the 24G needle-free catheter as a fluid inlet. Using a second clamp, the left HA and the left BD as well as the left median PV, the left median HA, and the left median BD were blocked. To speed up the procedure, we created the outlet (Fig. 2B) in the left lateral hepatic vein (HV) by performing a small 1-mm-long incision instead of using a catheter. Doing so facilitated the placement of the PVDC film and the dry gauze needed to protect the abdominal organs from the corrosive detergent solution during later in vivo liver lobe decellularization. At the same time, detergent leaking from the surface of the organ could be absorbed. As a next step, selective perfusion of the LLL was started by using 15 mL of heparinized saline (40 U/mL) at a flow rate of 1 mL/min. Success of selective perfusion was judged based on the selective color change of LLL from fresh red to faint yellow as well as on a representative histological assessment, as reported earlier.

Comparison of three detergents for in vivo perfusion decellularization
To identify the optimal protocol for in vivo perfusion decellularization of the targeted LLL, we designed three experimental groups (n = 6/group) for histological work-up. After heparin perfusion of the lobes using the modified perfusion technique, we compared perfusion of 1% SDS for 1 h followed by 1 h of 1% Triton with perfusion of either 2 h of only 1% Triton X or 2 h of only 1% SDS, respectively.
Detergents were applied by using a peristaltic pump (Harvard Apparatus 70P, USA) (Fig. 3A), at a flow rate of 1.4 mL/min, 4 s interval, 1.8 mL/min for 2 h. The abdominal cavity was protected from the contaminating detergent by covering all organs with polyvinylidene chloride (PVDC) film (Fig. 3B). Outflowing waste perfused fluid was drained by using dry gauze (Fig. 3C).
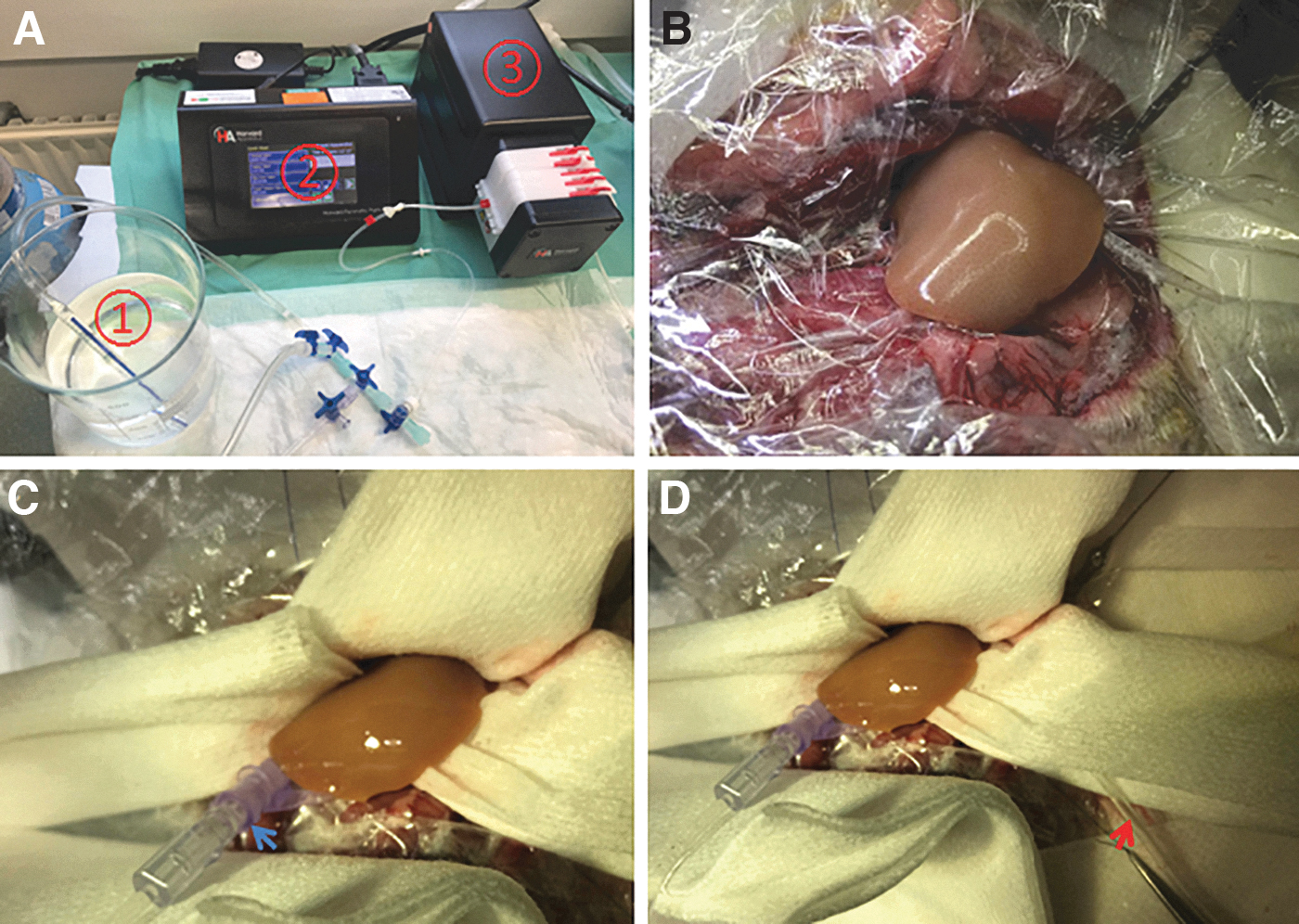
Intraoperative images showing perfusion system, isolation, and drainage for in vivo perfusion decellularization. Experimental setup with detergent solution
Immediately after in vivo perfusion decellularization, rats were sacrificed for assessment of decellularization efficiency based on macroscopic appearance of the liver lobe, histological assessment, and DNA content.
The most efficient decellularization protocol was used for further characterization of scaffold quality. Integrity of the portal vascular tree was examined by using an injection of blue silicone rubber compound via the left PV followed by micro-computed tomography (μCT) scanning (n = 3 scaffolds, and additional one normal as control). Integrity of the matrix structure of vascular and biliary tree and the sinusoidal network was assessed by histomorphology. The ultrastructure was visualized by using scanning electron microscopy (SEM) (n = 2 scaffolds, and additional one normal as control). Preservation of matrix proteins (elastin, fibronectin, laminin, and collagen IV) was assessed based on immunohistochemical (IHC) staining.
Comparison of two drainage methods to eliminate waste fluid during in vivo perfusion decellularization
To prevent the abdominal organs from direct contact with the detergent leading to corrosive injury, we further designed another two groups (n = 6/group) based on two different drainage methods: PVDC film + dry gauze and PVDC film + dry gauze + aspiration tube. For the first group, the drainage method of using PVDC film + dry gauze was performed as described in the first experiment. For the second group, an aspiration tube (Fig. 3D) was placed close to the base of the LLL for further drainage. After having put everything in place, the lobe was decellularized by using the most efficient decellularization protocol determined earlier. Constant liver perfusion was achieved by the Harvard peristaltic pump at the same flow rate and duration as mentioned earlier. Detergent leakage, drainage efficiency, and especially 1-week survival rate were taken as indicators of the optimal drainage method for in vivo perfusion decellularization.
Physiological blood reperfusion of the decellularized scaffold in vivo
After in vivo perfusion decellularization of the LLL with the optimal detergent, the decellularized scaffold was flushed with 0.9% sodium chloride solution at a flow rate of 5 mL/min for 10 min to remove most of the residual SDS from the ∼3-mL scaffold. The incisions of the left PV and left lateral HV were closed with 11-0 prolene sutures. All micro-clamps were taken off the vessels to allow physiological blood reperfusion of the decellularized lobe. Macroscopic change of the color of the scaffold from transparent to bright red was taken as an indicator to confirm the success of in vivo physiological reperfusion. The abdominal cavity was washed with 50 mL warm 0.9% sodium chloride solution to remove any possible contaminating SDS leaking from the liver lobe during decellularization. After closing the abdominal cavity, all rats in both groups were allowed to recover from anesthesia. Buprenorphine was administered subcutaneously in a dose of 0.05 mg/kg twice per day, so as to relieve postoperative pain. Totally, six rats per drainage group were used for 1-week survival analysis. With the most efficient drainage method determined from the two groups mentioned earlier, histological assessment at 12 h postoperatively was performed to confirm the physiological reperfusion of the decellularized scaffolds (additional three rats).
Histological staining
Liver sections of 3-μm thickness were cut after formalin fixation and paraffin embedding. Sections were stained with histochemical dyes for hematoxylin and eosin (H&E) staining. The stained sections were scanned at ×40 magnification with the scanner NanoZoomer 2.0 HT by using the software NDP scan (Hamamatsu, Japan).
Verhoeff-Van Gieson staining
Histological sections were dewaxed at 59°C in a warming cabinet for 30 min and then dehydrated through a descending alcohol series including xylol and alcohol (100%, 96%, and 70%). The sections were rinsed with distilled water three times, followed by incubation with resorcinafuchsin (00088663; Hollborn&Söhne) for 120 min. Afterward, they were rinsed with 96% alcohol until no more color clouds were left, and again briefly washed with distilled water three times. Mayer's hematoxylin (T865.3; Roth) was applied to stain the sections for 30 min. After being washed with distilled water three times, the sections were further stained with Van Gieson (Ch.-B.:0219; Apotheke) They were again washed with distilled water, dehydrated through an ascending alcohol series including alcohol (70%, 96%, and 100%) and xylol, and finally coverslipped. The stained sections were scanned in the same way as described earlier (Nuclei, black brown; Cytoplasm, light brown; Collagen, red).
Digitalized images were used for the morphological analysis. First, we checked the H&E images from the scaffolds subjected to different decellularization protocols for the presence of remaining liver cells or cellular debris (nuclei, purple/black). Second, structural integrity (collagen, pink) was also assessed based on the H&E staining of scaffolds obtained after 1% SDS-only decellularization. We identified the key features of the hepatic acinus such as the portal field with the PV, HA, and the BD as well as the central vein (CV) based on the appearance of the matrix structure (collagen, pink). We then assessed the integrity of the sinusoidal matrix structure based on the continuity of the network. We further judged the optimal decellularization protocol based on Verhoeff-Van Gieson staining (EvG staining).
IHC staining
To further assess matrix proteins of the scaffold, immunostaining was performed. Briefly, sample tissues were fixed in 4% formaldehyde and then embedded with paraffin. Liver sections were cut into 3-μm thickness. A panel of primary rabbit antibodies were used for immunostaining: Anti-collagen IV (ab6586, 1:500; abcam), Anti-fibronectin (ab2413, 1:200; abcam), Anti-elastin (ab21610, 1:100; abcam), and Anti-laminin (ab11575, 1:1000; abcam). After three washes with Tris-buffered saline with Polysorbate 20 (TBST), the samples were stained according to the manual of EnVision® + System-HRP Labeled Polymer Anti-Rabbit (K4011; Dako). Thereafter, the sample was counterstained with hematoxylin for 7 min, and it was then rinsed with tap water for 10 min. After dehydration with ethanol (70%, 96%, and 100%) and xylol in sequence, the samples were mounted with mounting medium (41-4011; Medite) before imaging.
Preservation of the main ECM proteins in the portal field and the sinusoidal network was assessed by comparing IHC images from normal and decellularized liver samples.
Silicon rubber compound staining
To visualize the integrity and patency of the portal vascular tree, 0.5-mL blue silicone rubber injection contrast agent (MV120; MICROFIL®, USA) was administered via the left PV in normal and decellularized LLLs. About 20 min after injection, the compound polymerized. Integrity of the portal tree of the scaffold was judged based on the continuous contrasting of vascular tree as well as on the detection of intrahepatic leakage.
μCT scanning
The scaffold injected with silicone rubber compound was explanted and stored in formalin solution at 4° for more than 48 h for fixation. For μCT scanning of the scaffold, the liver sample was taken out of the fixation solution and placed onto a μCT bed. Then, the bed with scaffold was put into the μCT machine. A high-resolution μCT (SkyScan1272; Bruker, Billerica, MA) acquired 940 projections with 2688 × 4032 pixels with 3186 ms exposure time, with a total duration of 8 h. The X-ray tube was operated at voltage 60 kV and current 0.166 mA with an aluminum filter of 0.25-mm thickness. After scanning, a volumetric stack with voxel size 6.6 μm was constructed by filtered backprojection. The images were used for three-dimensional (3D) reconstruction of the portal tree by using the software IMALYTICS Preclinical 2.0. 41
To assess the structural integrity of the portal tree, we determined the continuity of the vascular tree after 3D reconstruction and the level of branching.
Scanning electron microscopy
To evaluate the 3D ultrastructure of the decellularized scaffold, SEM was conducted. A normal and a decellularized LLL were subjected to perfusion fixation with 20 mL of a mixture of 4% paraformaldehyde, 2.5% glutaraldehyde, and 0.1 M cacodylate buffer (pH 7.4). After perfusion, the LLL was excised and placed into the fixative for 24 h at room temperature. Afterward, the samples were washed three times for 10 min each with cacodylate buffer and dehydrated in ascending ethanol concentrations (30%, 50%, 70%, 90%, and 100%) for 10 min each. Subsequently, the samples were critical-point dried by using liquid carbon dioxide and sputter coated with gold (thickness ∼4 nm) by using an SCD005 sputter coater (BAL-TEC; Liechtenstein) to avoid surface charging. Finally, the specimens were investigated with a field emission SEM LEO-1530 Gemini (Carl Zeiss NTS GmbH, Oberkochen, Germany).
Images were taken at different magnifications. Similar to the histological investigation, we focused on determining the integrity of the ultrastructure of the matrix in the portal triad and of the CV. We also assessed the integrity of the ultrastructure of the sinusoidal matrix network.
DNA quantification
To further assess the complete removal of cells in the decellularized scaffold, DNA quantification was carried out. DNA was extracted from a small piece (up to 25 mg) of excised normal liver and the decellularized scaffolds by using QIAamp DNA Mini Kit (QIAGEN) according to the instruction of the QIAamp DNA Mini and Blood Mini Handbook (2016; QIAGEN). DNA concentration was measured by Spectrophotometry using a Nanodrop1000.
Statistical analysis
All results are presented as mean ± standard deviation. Statistical comparisons were made through the use of a Student's t-test performed within SPSS Statistics 25. Statistical significance was determined to be p < 0.05.
Results
Selective perfusion of the left lateral lobe using the modified method
After perfusion of the LLL with heparinized saline, the lobe did gradually change color from red to faint yellow (Fig. 4A, B), indicating that the blood in the portal system of the lobe was completely washed out. However, as reported earlier, clamping of the left lateral PV caused ischemia of the left median lobe (Fig. 4B). The histological assessment of the lobe further confirmed that no blood cells were visible in the PV branches and CVs, compared with a native liver lobe (Fig. 4C–F). This indicates that the modified in vivo circuit bypass also enabled the selective perfusion of the LLL without causing any further damage.

Confirmation of successful selective perfusion of LLL by using the modified perfusion technique.
Identification of the optimal decellularization protocol for in vivo perfusion decellularization
Using 1% Triton X100 followed by 1% SDS within 2 h resulted in incomplete removal of the cellular components of the liver lobe, as indicated by nontranslucent areas of different sizes (Fig. 5A–D). Histology revealed large areas of cell-free parenchyma interspersed with islands of remaining cells, confirming the incomplete decellularization result (Fig. 6B). Correspondingly, the DNA concentration after random sampling of the liver was as high as 1366.92 ± 500.89 ng/mg (n = 6/6, wet tissue), which is about 50% of the normal liver (3091.31 ± 192.89 ng/mg, n = 6/6) (p < 0.0001).
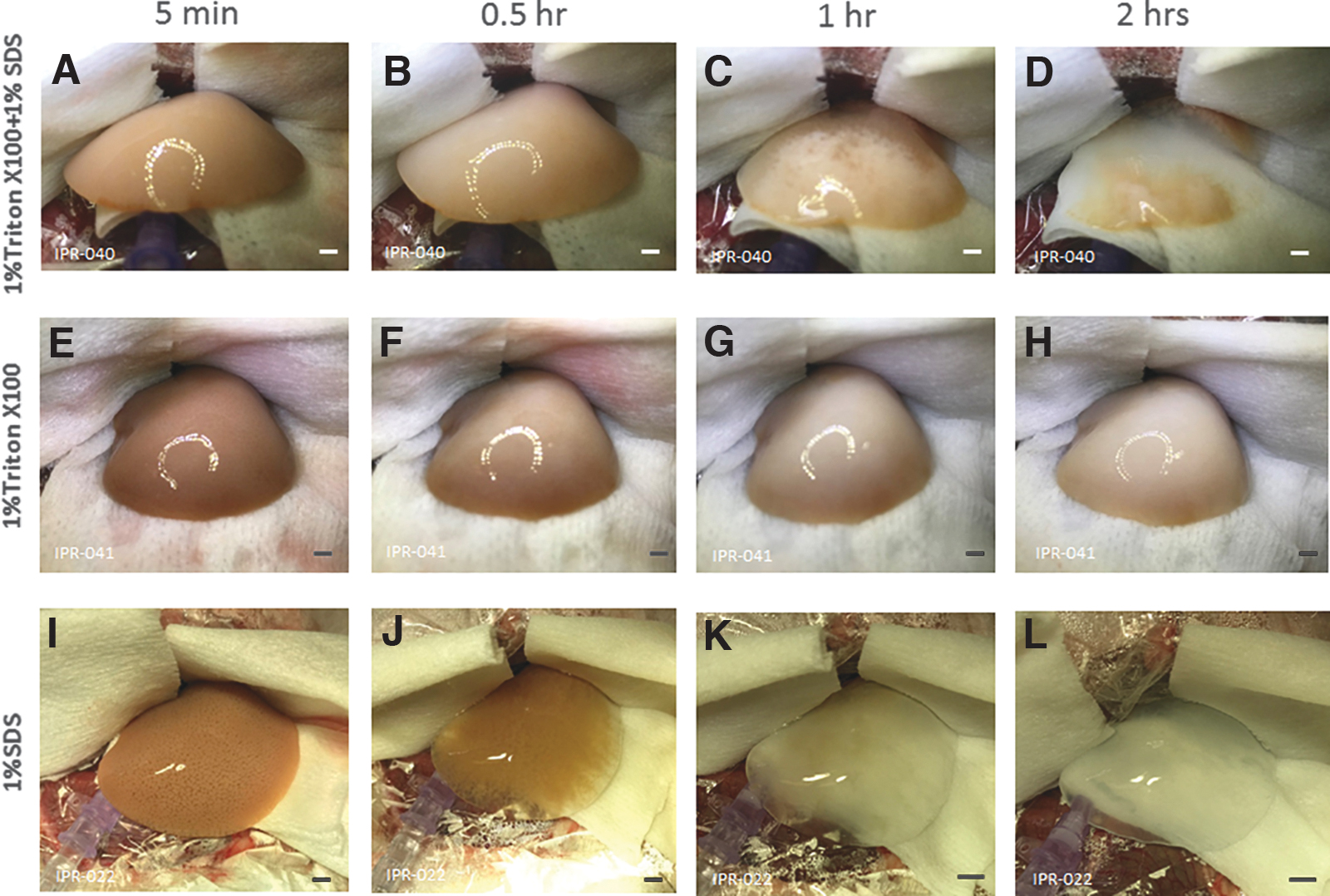
Intraoperative images showing in vivo decellularization of the LLL. Time sequence from 5 min to 2 h using 1% Triton X100 followed by 1% SDS, resulting in incomplete decellularization of the lobe
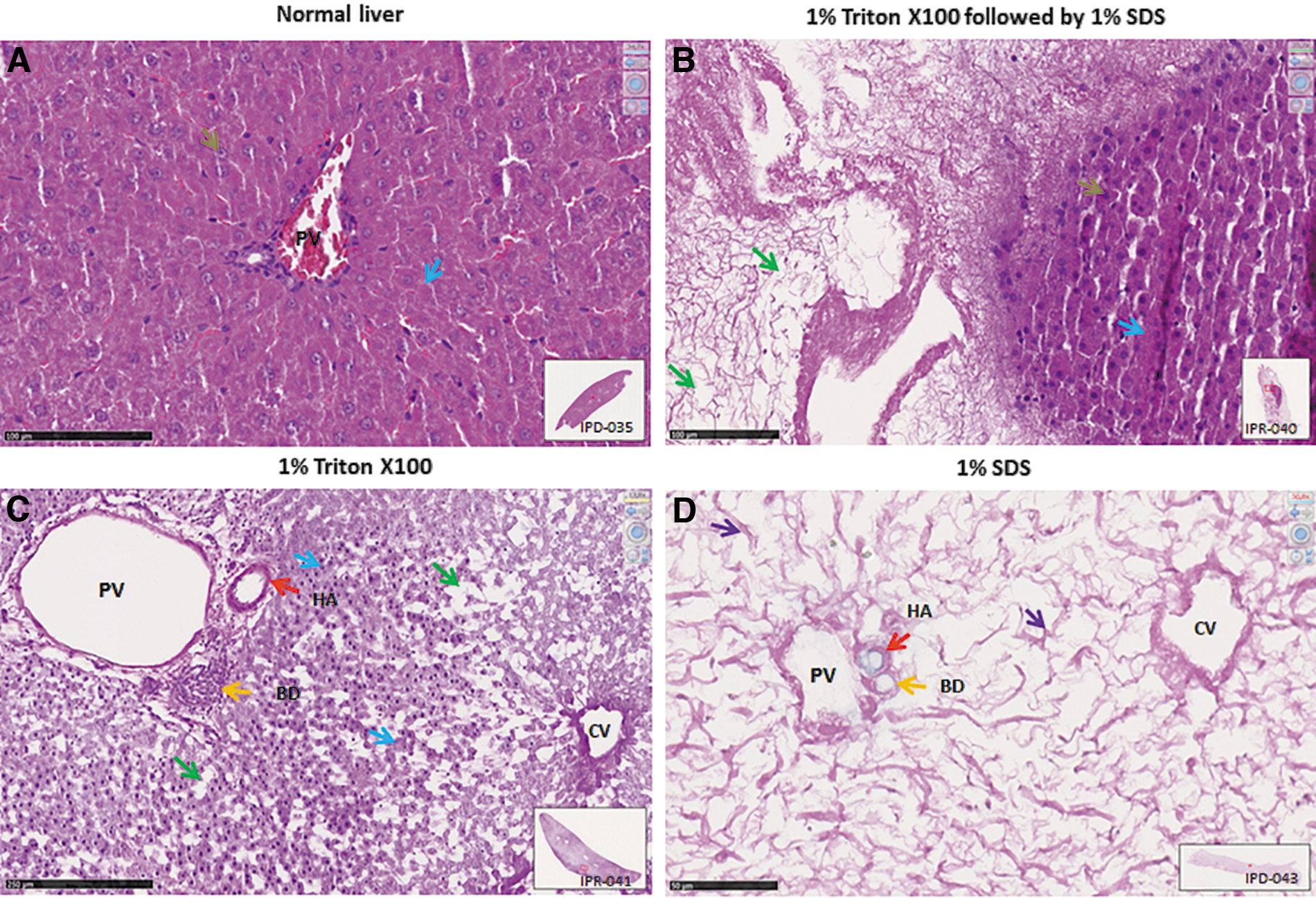
Histological assessment (H&E) of scaffolds comparing three in vivo decellularization protocols.
Perfusion with 1% Triton X100 alone did not result in decellularization but caused a smooth change in color from faint yellow to a nontranslucent white appearance of the LLL within 2 h (Fig. 5E–H). Similarly, histology showed that hepatic parenchyma was not removed. However, detergent perfusion caused the loss of nuclear stain in the majority of the liver cells, suggesting at least severe damage or death of the cells. Interestingly, a small rim of seemingly vital cells was seen in the vicinity of the portal field. In between the hepatic chords, large empty spaces became visible, suggesting the removal of at least some hepatocytes (Fig. 6C). These finding were confirmed by the DNA-concentration measurement revealing slightly lower levels (2614.94 ± 547.73 ng/mg, n = 6/6) (p = 0.16 > 0.01) than in the normal liver.
In contrast, perfusion with 1% SDS alone gradually cleared the liver from all cellular components within 2 h, as indicated by the translucent appearance (Fig. 5I–L). No areas with remaining cells or cellular debris were detected in any of the histological sections (Fig. 6D). Correspondingly, the remnant DNA concentration was as low as 57.40 ± 11.71 ng/mg, which represents <2% of the DNA concentration of the normal liver lobe (p < 0.00001) (Fig. 7).
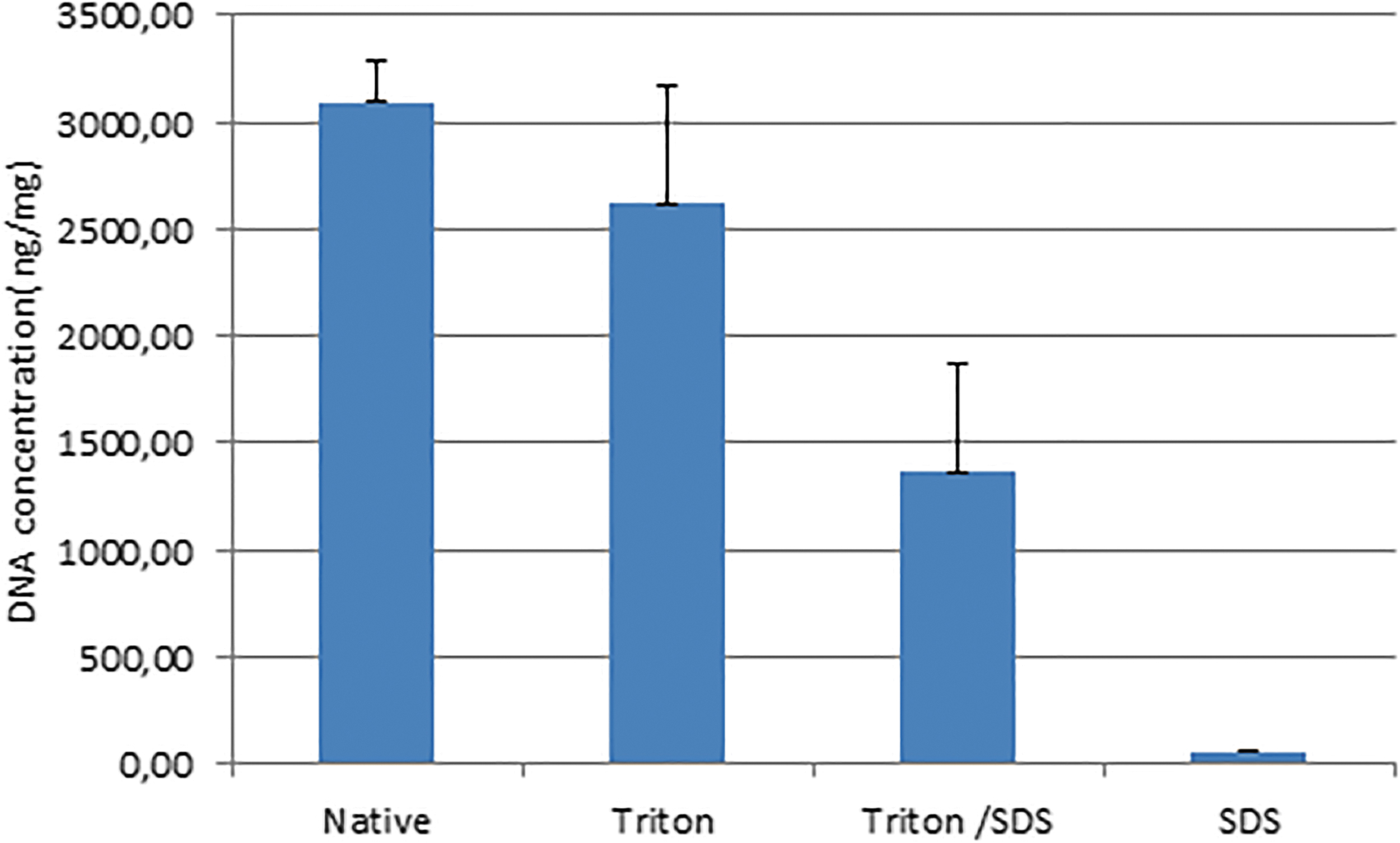
Molecular assessment of the decellularized scaffolds. DNA quantification of the decellularized liver scaffolds among the three groups of Triton X100 only, Triton X100 followed by SDS, and SDS only, in comparison with that of the native liver lobe. Color images are available online.
Taken together, these findings suggest that in vivo decellularization with 1% SDS only for 2 h is very effective compared with the other two protocols and was, therefore, used in the subsequent experiments.
Characterization of the scaffolds generated with the optimal decellularization protocol (1% SDS)
First, we characterized the vascular tree of the scaffold generated with the optimal decellularization protocol based on macroscopic evaluation. The vascular trees including the PV tree system and HV system (Fig. 8A) are macroscopically visible in the translucent matrix. The blue silicon rubber compound solution injected through the left PV appeared as expected inside the portal vascular network. On injection, it gradually moved from the lobar portal vein (PV) vessels to smaller venules, indicating the integrity of the portal vascular structure (Fig. 8B). Since injection was stopped when the blue compound reached the finest branches of the portal vascular tree, the hepatic venous tree appeared white in the otherwise translucent scaffold (Fig. 8B).
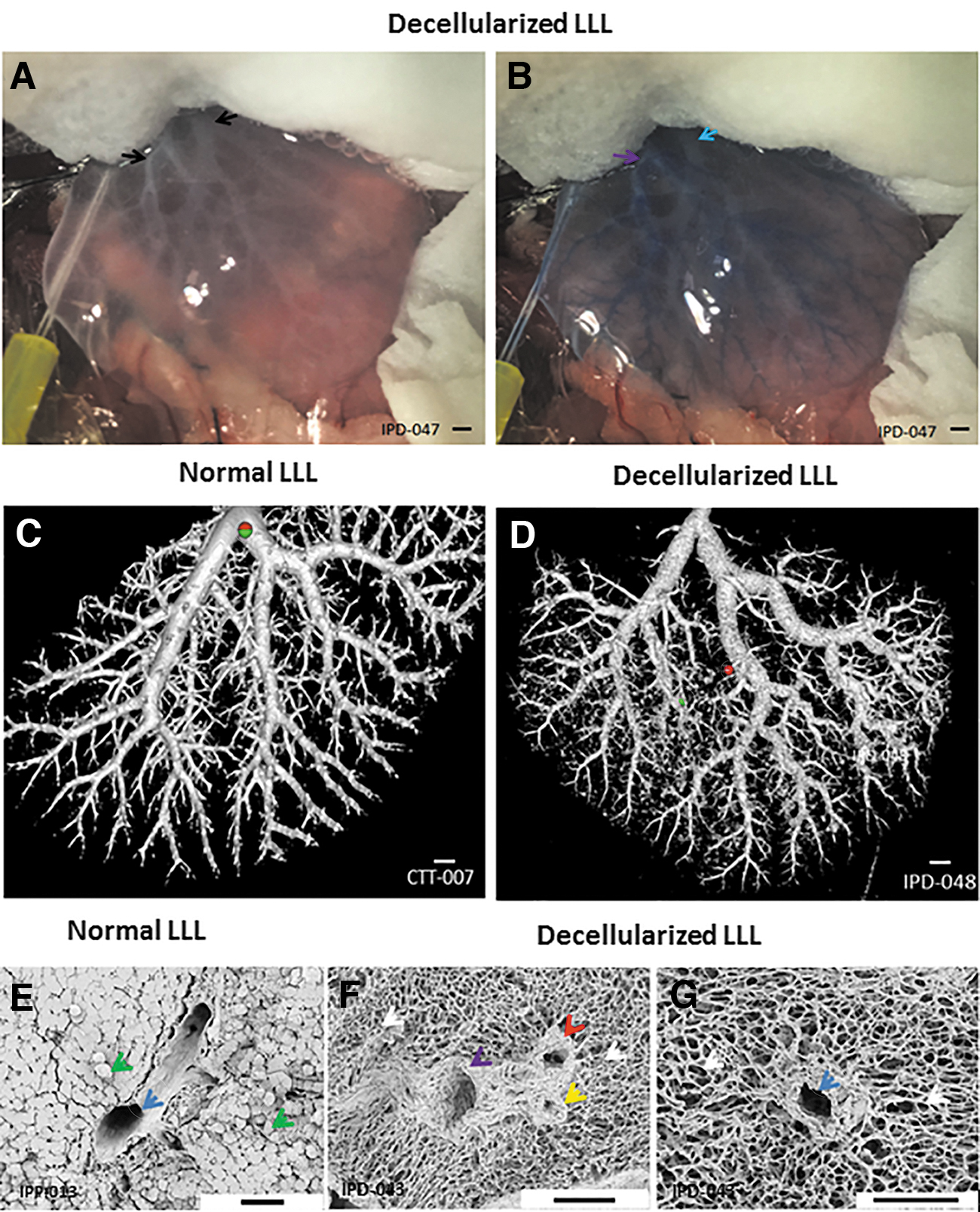
Characterization of structural architecture of the LLL scaffold.
We further visualized the portal vascular tree in three dimensions by μCT scanning and 3D reconstruction. Computed tomography (CT) scanning confirmed that the continuity of portal vascular tree was clearly visible on 3D reconstruction. Furthermore, the large-sized lobar portal vessels up to the fourth to fifth order (Fig. 8D) remained intact, which is comparable to the normal LLL.
Second, histological staining of the scaffold showed key features of the hepatic acinus. Portal fields could be clearly identified based on the remaining matrix structure of PV, HA, and BD. CVs appeared as single vascular matrix structures. In addition, the decellularized hepatic lobules appeared as a dense network of sinusoidal structures resembling a spider net (Fig. 6D). These findings suggest that hepatic microarchitecture was morphologically preserved after in vivo decellularization of the selected liver lobe.
Third, the SEM images revealed the integrity of the ultra-structure of the matrix including the PV, HA, BD (Fig. 8F), and the CV (Fig. 8G). We observed the continuous sinusoidal matrix network in the parenchyma of the scaffold (Fig. 8F, G). These findings show the integrity of the ultravascular structure in the decellularized liver scaffold, compared with the native liver lobe.
As the fourth and last step, using a staining panel consisting of histochemical and IHC methods, the protein components of the scaffold were assessed.
Using the EVG staining, we observed strong red signals (collagen) in the portal field (Fig. 9A, B) and around the CV (Fig. 9C, D) of the scaffold, similar as in the native liver. Compared with the portal field, the staining intensity in the sinusoidal matrix network was much weaker, indicative of the different collagen content in the structures. In the scaffold, we neither observed any black nuclear signals nor observed any yellowish cytoplasmic stain, indicating the removal of cells or cell remnants. As expected, we saw only a faint dark purple signal in the HA of the native liver but not clearly in the scaffold.
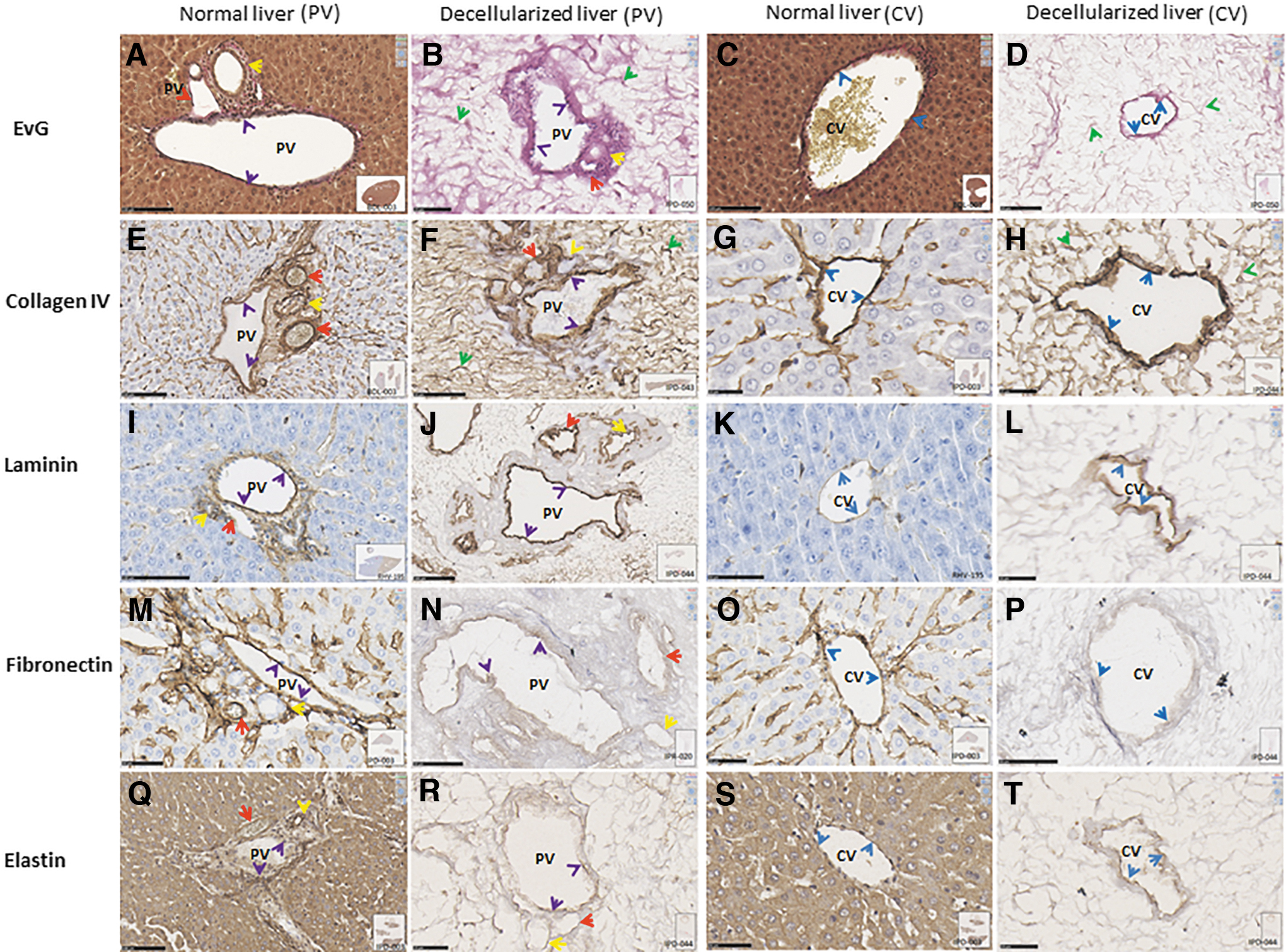
EvG staining and IHC assessment of the decellularized scaffold demonstrating the preservation of key extracellular matrix proteins in the portal field as well as the CV. In normal liver and decellularized liver scaffold and lobe, EvG staining showing red collagen
This was further confirmed by the Collagen IV staining. We observed an over-all stronger signal in both the native liver and the decellularized scaffold. The strong signal in the portal field, especially in the basal membranes, facilitated the identification and differentiation of the three key structures PV, HA, and BD (Fig. 9E, F). Due to the strong staining of the basal membrane also the CV (Fig. 9G, H) could be detected easily. Further, the strong staining of the sinusoidal network can be taken as an indicator of the preservation of the sinusoidal matrix.
The IHC signal for Laminin, usually expressed in the basal membrane of vessels and to a much lesser extent also in the sinusoids, was strong in the portal field (Fig. 9I, J) and in the CV (Fig. 9K, L). In contrast, the signal was rather weak in the sinusoidal network, also reflecting the preservation of the physiological distribution of the ECM protein.
Fibronectin is one of the most abundant proteins in the perisinusoidal space surrounding the periportal and CV regions. 42 We observed a strong signal in the portal field (Fig. 9M, N) and around the CV (Fig. 9O, P) of the native liver, which was less pronounced in the scaffold. Similarly, we observed a slightly weaker signal in the sinusoidal matrix of the scaffold compared with the native liver. This gives rise to the speculation that the detergent might have affected the fibronectin content of the scaffold.
Elastin is mainly expressed in the vasculature of normal liver, as indicated by strong brown signals, but less in the sinusoids, as visualized by light brown signals (Fig. 9Q, S). In the LLL scaffold, strong signal intensity was seen in the portal field (Fig. 9R) and in the CV (Fig. 9T), which is similar to the pattern observed in the normal liver. Similarly, the staining intensity was much fainter in the sinusoidal network, suggesting preservation of this ECM protein as well.
Identification of the optimal organ protection during in vivo decellularization (1% SDS)
During in vivo perfusion decellularization, waste fluid emerged not only from the incision hole in the left lateral HV but also from the surface of the liver (Fig. 10), in total about 200 mL within the 2-h procedure. To protect the abdominal cavity and all organs completely from this volume, placement of the PVDC film covered by gauzes was insufficient to absorb and drain this large amount of corrosive waste fluid. Animals subjected to this procedure died within 48 h (n = 5/6) and just only one (n = 1/6) survived for less than 1 week. Only after placing an additional suction tube between the gauze layers, complete prevention of contamination was achieved. All animals (n = 6/6) subjected to the drainage method of PVDC film + dry gauze + suction tube tolerated the procedure well, as indicated by the survival rate of 100% after the 7 days of observation time. In contrast, in the group of rats subjected to the simple procedure (no suction tube), only 16.7% (1/6) reached the end of the observation period, as shown in the Kaplan–Meier curve (Fig. 11). None of the rats subjected to the combination of PVDC film + dry gauze + suction tube suffered from any severe postoperative complications. The maximal body weight loss during the first 7 postoperative days was <20% and occurred on postoperative days 2–3, and with a fast recovery thereafter (Fig. 12). This observation suggests that the procedure was well tolerated and that it did not experience severe toxic SDS-related side effects.
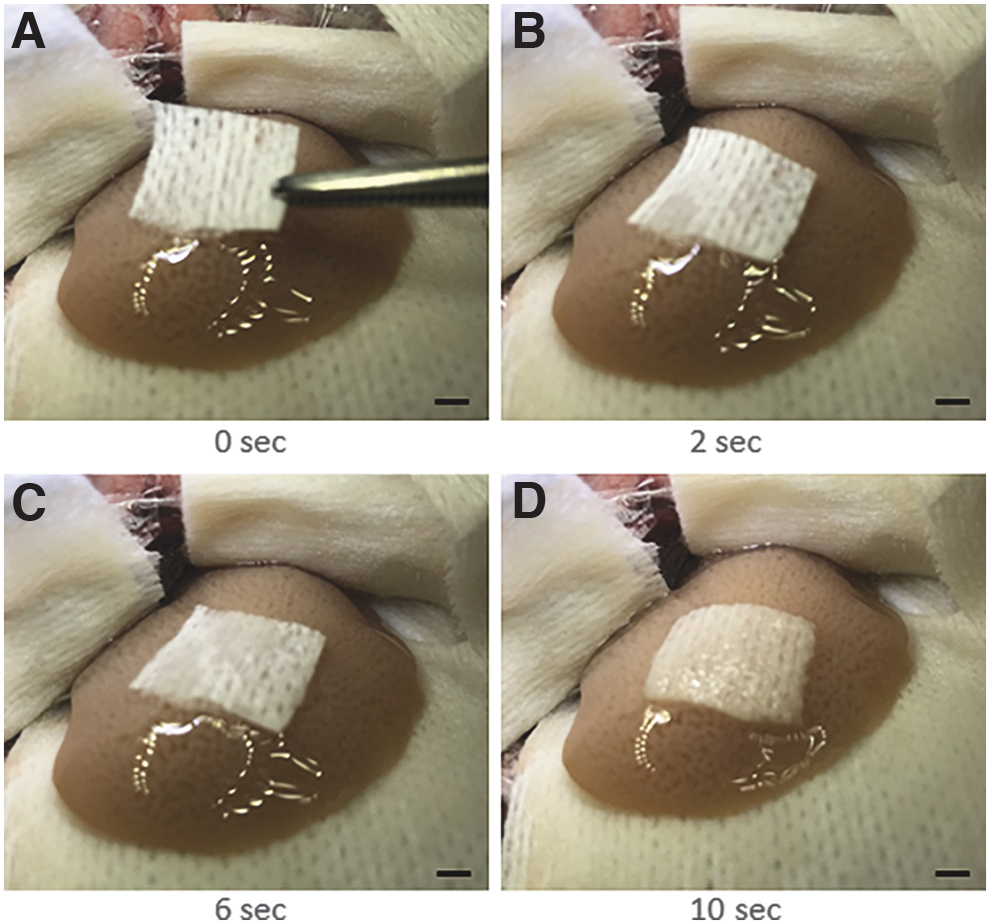
Intraoperative images showing waste perfusate emerging from the whole surface of the LLL during perfusion decellularizaton in vivo. A small square piece of dry gauze placed on the surface of the LLL turning from dry to wet within seconds
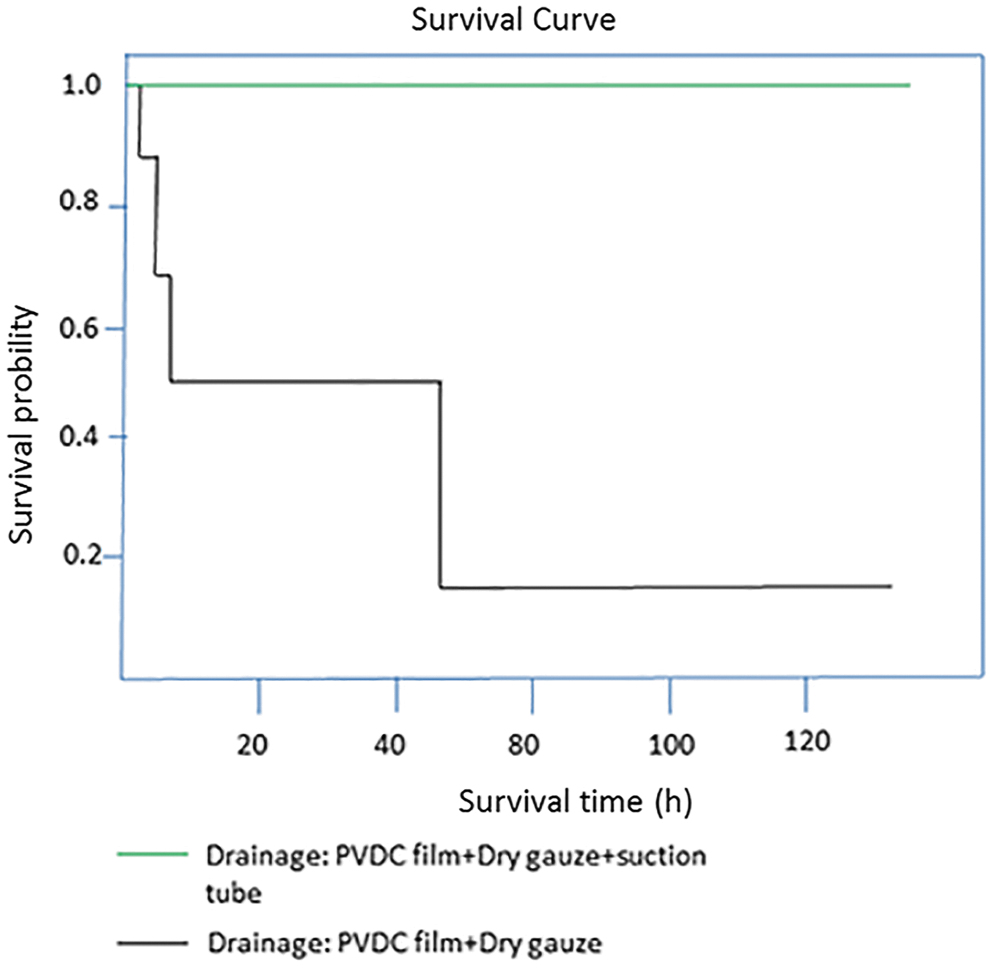
Survival rate of the rats between two different drainage methods. Kaplan–Meier survival curve of the rats that were subjected to the efficient drainage method of PVDC film + dry gauze + suction tube and those that were subjected to the less efficient drainage method (PVDC film + dry gauze) during the procedure of in vivo decellularization. Color images are available online.

Postoperative body weight. A postoperative first-week observation of body weight of the rats subjected to the drainage method of PVDC film + dry gauze + suction tube. Color images are available online.
Physiological reperfusion of the decellularized scaffold in vivo
After closing the incision on the left PV and the left lateral HV and reopening the blocked left PV, artery, and BD to the left lateral scaffold, the color of the scaffold changed back from translucent (Fig. 13A) into red (Fig. 13C), suggesting blood reperfusion of the scaffold.

Physiological reperfusion of LLL scaffold in vivo.
Histology obtained 12 h after reperfusion revealed large amounts of erythrocytes in PV, sinusoidal network, and CV, although distributed very inhomogeneously throughout the section. In all three animals we also found blood clots in large intralobar vessels, leading to a partial blockade of the vessel (Fig. 13D, E). Further, in one of the three animals we observed an alteration of erythrocytes and formation of hemoglobin crystals in some areas of the section (Fig. 13F).
Discussion
In this study, for the first time, we demonstrate long-time survival after in vivo liver lobe decellularization and physiological reperfusion in rats. Further, our technique resulted in remarkable scaffold quality.
Decellularization time
In comparison to the first report of in vivo decellularization by Pan et al., 27 our procedure took longer with 2 h compared with 1 h reported by them. This might be related to the size of the targeted liver lobe, with the LLL being fivefold the size of the right superior liver lobe, according to the rat liver volume measurement reported by Madrahimov et al. 43 Nevertheless, completing the operation, including laparotomy, decellularization, and closure, within 3 h still allows using up to 90 min for reseeding the organ in vivo to keep the total time below 5 h. Our previous study investigating in vivo perfusion of the LLL revealed that an operation time of <5 h was still tolerated by the animals. However, when prolonging the time to 5 h or more, the rats developed transient diarrhea and bloody ocular discharge. 25 In contrast, Pan needed about 2 h for in vivo decellularization and reseeding, but sacrificed the rats intraoperatively after additional 6 h of observation without even attempting to assess the survival rate and time.
Using 1% SDS for in vivo liver lobe decellularization resulted in a complete removal of cells in the targeted liver lobe within 2 h, which is even more time-efficient than using Triton X100 alone or the sequential application of Triton X and SDS in our study. In addition, loss and destruction of matrix protein might be related to the exposure time to the harsh detergents, as shown in detail for porcine aorta by Guler et al. 44 Therefore, it is critical to reduce the exposure time for the sake of preserving more matrix proteins. Using only 2 h of 1% SDS perfusion for in vivo decellularization is substantially shorter compared with the duration of ex vivo decellularization ranging from hours to days or even weeks reported by other authors mentioned earlier. The reason that we could shorten the decellularization time may be due to an extensive heparin saline flush of the live lobe before decellularization. Using heparin did not only help to prevent disseminated intravascular coagulation but also dissolved small thrombi formed in the vessel after clamping. Such microthrombi causing obstruction may hinder the flow of the detergent into the liver lobe and slow down the process of decellularization.
Decellularized scaffold quality
Our work suggests that in vivo selective liver lobe decellularization did create a translucent liver matrix while preserving the integrity of the matrix structure. PV, HA, BD, and CV, as well as the ultrastructure of the matrix were confirmed by CT, histology, and SEM. The main matrix proteins including laminin, elastin, fibronectin, and collagen IV were preserved, as indicated by the presence of strong signals in IHC. Therefore, we could apparently identify and discriminate all vascular structures in the portal field and visualized the continuous sinusoidal network by using standard IHC staining. We provide the first data of a very detailed description of the fine structures of in vivo decellularized liver lobe scaffolds in contrast to other reports, which just claimed their structural integrity based on a global assessment.16,24,35,45
SDS contamination and toxicity
Since long-term survival is the prerequisite for establishing in vivo liver engineering successfully, this was the reason that we solved the drainage problem first before focusing on scaffold repopulation. Detergent waste fluid emerged not only from the incision in left lateral HV but also from the whole surface of the targeted liver lobe during the in vivo perfusion decellularization process. Therefore, the whole abdominal cavity and all abdominal organs were at risk of contamination with the detergent. Pan et al. 27 already identified the risk of contamination, but they only used a catheter placed in the outlet created in the inferior vena cava. This catheter can effectively drain a substantial amount of the waste fluid; however, it cannot prevent contamination with waste fluid emerging from the surface of the liver lobe undergoing decellularization.
We efficiently prevented the outflowing detergent waste fluid from contaminating nontargeted tissue and organs in the abdominal cavity by covering them with PVDC film. PVDC film is widely used for wrapping food,46,47 because it is insoluble in oil and organic solvents. It has a very low moisture regain and is impervious to mold and bacteria. PVDC seems to act as a remarkable barrier not only against water, oxygen, and aromas but also against base and acid solutions. Besides using the mechanical PVDC barrier, we efficiently drained the waste fluid by using dry gauze as well as an aspiration tube. Reduction of contamination by using an aspiration tube in addition to the PVDC film and dry gauze seemed to be most decisive for the survival of the animals.
Further, we not only perfused the decellularized scaffold with warm saline solution but also flushed the abdominal cavity with warm saline solution after decellularization to wash away the residual SDS.
Therefore, all these measures together enabled the long-term survival of the animals without experiencing severe toxic side effects. In addition, the maximal postoperative body weight loss never exceeded 20% and recovered from postoperative day 3 onward. Based on our observations, we concluded that using the combination of PVDC film + dry gauze + aspiration tube as drainage method together with a thorough perfusion of the scaffold and a wash of the scaffold and the abdominal cavity resulted in an efficient prevention of a potential contamination with residual SDS. Therefore, we did not go deeper in the exploration of the potential systemic toxic effects of the SDS.
Limitations
Despite anatomical and technical challenges, we successfully established a survival model of in vivo selective liver lobe decellularization in rats. However, there are also some limitations: First, since the left PV supplies the left lateral PV and the left lateral PV, transient ischemia of the left median lobe (only representing ∼15% of the whole liver in volume) is inevitable due to blockage of the left PV. Transient ischemia might induce some liver damage, but it does not put the animal at a vital risk.
Further, other rarely used detergents such as deoxyribonuclease,48,49 sodium lauryl ether sulfate, 48 and sodium deoxycholate, 50 possibly resulting in an even shorter time for in vivo decellularization, were not included in the comparison of the decellularization protocols.
Finally, the “naked” collagen of the scaffold can activate the extrinsic coagulation system on contact with blood uon reperfusion. Therefore, it is not surprising that we observed blood clots in the scaffold similar as also reported by others.23,26,27 This might explain the very inhomogeneous distribution of blood cells within the scaffold. Another interesting finding was the observation of altered swollen erythrocytes and the formation of crystals that were also distributed inhomogeneously throughout the scaffold. Both together, swollen erythrocytes potentially undergoing hemolysis and releasing hemoglobin in the direct neighborhood to crystals lead to the suspicion that hemoglobin crystals did form. Hemoglobin crystal formation was previously observed in the brain of rats with experimental intracerebral hemorrhage, 51 in lungs with pulmonary hemorrhage of varying etiologies,52–54 but also as a result of pressure injury to rat dentition. 55 In our case, hemoglobin crystal formation might be due to toxic injury because of minimal residual SDS trapped in the protein structure of the scaffold leading to hemolysis with subsequent release of hemoglobin. Assuming a volume of the LLL of ∼3 mL, we perfused the lobe with 50 mL saline solution, a 17-fold higher volume that should lead to substantial reduction of remaining SDS. However, it cannot be excluded that even low levels of SDS binding to the scaffold proteins might cause local hemolysis with subsequent crystal formation.
Further, it is highly likely that the loss of cells reduces the stability of the resulting scaffold, rendering the scaffold very prone to perfusion inhomogeneities. Inhomogeneous perfusion may result in an incomplete wash and a highly variable distribution of blood reperfusion, resulting in locally different levels of residual SDS as indicated by an inhomogeneous distribution of hemoglobin crystals.
Perspective
Both observations of clot formation and hemoglobin crystallization call for a kinetic observation of the reperfusion process over time to investigate the reperfusion quality of the scaffold and the effectivity of the wash-out procedure. For excluding any potential local and systemic toxicity of residual SDS, a number of tests could be performed at different observation time points during the first postoperative week, such as (1) a detailed histologic work-up of the scaffold to better understand the timing of blood clot and crystal formation; (2) blood count to detect any eventual hemolysis; (3) determination of local SDS-scaffold and systemic SDS-blood levels as direct evidence of SDS contamination, histology of other organs, for example, heart, lung, kidney, spleen, and undecellularized liver lobes; as well as (4) clinical chemistry including liver function and renal function to identify any organ-specific effect.
Since blood clots were observed in the blood reperfused scaffold, we believe that the next urgent problem to address is to prevent coagulation in the scaffold for ensuring in vivo physiological perfusion. It is highly unlikely that reseeding the scaffold with endothelial cells with a very short time for cell adherence is sufficient to prevent clotting. Recently, one interesting technique was suggested by Bruinsma et al. 56 for preventing coagulation when transplanting a repopulated liver scaffold. They reported applying a layer-by-layer heparin coating technique to a scaffold before reseeding the scaffold in vitro prevented coagulation.
Once anticoagulation in vivo is achieved, we will pursue in vivo liver reengineering by in vivo recellularization of the liver scaffold with hepatocytes and non-parenchymal cells, as done ex vivo by other authors.23,24,56–59
For fundamental research, the key benefit of in vivo partial liver decellularization is its potential for promoting the understanding of liver engineering by in vivo repopulation of a liver scaffold.
Clinical applicability is hampered by the difference in the lobar and vascular anatomy of the liver. The human liver represents one large organ that is separated by the underlying vasculature in a right and left lobe, but without being separated into two anatomically distinct lobes. Therefore, creating a bypass circuit is only possible after parenchymal transection as performed in the ALPPS procedure (Associating Liver Partition and Portal Vein Ligation for Staged Hepatectomy). 60 This is a therapeutic surgical procedure that is currently used to enhance resectability for otherwise unresectable liver tumors by ligating the PV from one liver lobe to promote regeneration of the other partitioned liver lobe. Therefore, in vivo selective lobe perfusion followed by decellularization would be feasible after parenchymal transection. In vivo selective liver lobe decellularization may be an alternative method of chemical resection for patients with diseased livers, for example, lobular liver cancer25,27 or various hepatic-based metabolic disorders. And then hepatic function could be restored through in vivo repopulation of the decellularized scaffold with healthy liver cells or stem cells. 27 In most hepatic metabolic disorders, recovery of only about 10% of the original enzyme activity is sufficient to ensure adequate metabolic control.61,62
Conclusions
Overall, despite technical and anatomic challenges, we provide the first data on having successfully established a survival model of in vivo partial liver decellularization in living rats, which represents groundwork toward in vivo organ engineering.
Footnotes
Disclosure Statement
Funding Information
This project is funded by the Chinese scholarship Council (Fund No.: CSC NO: 2017080801619). Special thanks go to Jens Geiling from the Institute of Anatomy I, Jena University Hospital for producing the schematic drawings of rat liver anatomy.