
Abstract
For end-stage lung disease, lung transplantation remains the only treatment but is limited by the availability of organs. Production of bioengineered lungs via recellularization is an alternative but is hindered by inadequate repopulation. We present a cell delivery method via the generation of negative pressure. Decellularized lungs were seeded with human bronchial epithelial cells using gravity-based perfusion or negative pressure (via air removal). After delivery, lungs were maintained in static conditions for 18 h, and cell surface coverage was qualitatively assessed using histology and analyzed by subjective scoring and an image analysis software. Negative pressure seeded lungs had higher cell surface coverage area, and this effect was maintained following 5 days of culture. Enhanced coverage via negative pressure cell delivery was also observed when vasculature seeded with endothelial cells. Our findings show that negative pressure cell delivery is a superior approach for the recellularization of the bioengineered lung.
Impact statement
New strategies are required to overcome the shortage of organ donors for lung transplantation. Recellularization of acellular biological scaffolds is an exciting potential alternative. Adequate recellularization, however, remains a significant challenge. This proof of concept study describes a novel cell delivery approach, which further enhances the recellularization of decellularized lungs. Organs seeded and cultured with this method possess higher cell surface coverage and number compared to those seeded via traditional gravity-based perfusion approaches.
Introduction
Lung disease is one of the leading causes of death in the world. 1 Currently, lung transplantation is the only viable therapeutic option for end-stage lung disease but remains limited by the availability of transplantable lungs 2 and is associated with mortality and complications. 3 One alternative solution that has currently been investigated is the use of tissue engineering approaches to generate bioengineered lungs through the process of decellularization and recellularization. In this process, all cells are removed from the lungs while the extracellular matrix is maintained, resulting in an acellular biologically active scaffold with intact structure and mechanical integrity. 4 Ultimately, decellularized scaffolds would be repopulated with recipient-derived cells and “made to order” or, using universal donor cells, used as an “off-the-shelf” source of transplantable lungs, thus avoiding graft rejection. 5
While there has been significant progress in the optimization of decellularization protocols for lung scaffolds, 6 recellularization remains a significant challenge, and adequate repopulation of the scaffold is not yet achieved. There are a number of cell-intrinsic factors such as appropriate cell types and complex culture requirements limiting the reepithelialization of acellular lung scaffolds.7–9 The initial delivery of cells to the scaffold is a fundamental step that may warrant reevaluation, given the persisting challenges in cell delivery. 10
Typically, gravity-based perfusion is the most commonly used approach for seeding epithelial cells.11–13 However, this cell-seeding method results in an inhomogeneous distribution of cells and inadequate coverage, which could be, in part, due to low cell suspension flow rates.10,14 In addition, gravity perfusion cell seeding occurs via positive pressure, which is in contrast with the lung's intrinsic negative pressure mechanism.
Herein, we propose a cell-seeding system mimicking inhalation via a negative pressure mechanism driven by the difference in the pressure gradient between the lung and the surrounding environment resulting in the expansion of the airways. Our system allows for controlled high cell suspension flow rates and results in significantly higher scaffold cell coverage in comparison to the standard gravity-based perfusion system. Importantly, the effect was maintained after a prolonged culture period, thus resulting in better overall recellularization. Moreover, proof-of-concept studies evaluating the use of negative pressure for recellularization of the vasculature also resulted in higher cell surface coverage.
Methods
All experimental work was conducted as per protocols approved by the Toronto General Hospital Research Institute ethical review board. To generate the negative pressure, a commercial syringe pump “NE-4000 programmable 2 channel syringe pump” (New Era) was used. Mice were used as the experimental animal model and euthanized by CO2. Lungs were harvested and cannulated at the trachea and pulmonary artery (PA). Decellularization was completed over 3 days via enzymatic and chemical treatment with reagents, including triton X100, sodium deoxycholate (SDC), sodium chloride, DNase, and phosphate buffer sulfate. Details pertaining to surgery and decellularization are discussed in the experimental design section.
Human bronchial epithelial cells were delivered to the lungs intratracheally using gravity-based perfusion and negative pressure cells seeding method at different rates of air removal (200, 50, and 12.5 mL). Following 18 h of static period, the samples were fixed in formalin for further analysis. Additional lungs were seeded with gravity-based perfusion and negative pressure cell seeding (NPCS) at an air removal rate (ARR) of 50 mL/min. After 18 h of static period, seeded lungs were transferred to a perfusion bioreactor for 5 days for long-term assessment. Finally, the effect of NPCS on endothelialization was assessed. A set of lungs were seeded intravascularly with mice endothelial cells using gravity-based perfusion and NPCS at ARR of 50 mL/min. After 18 h of static period, these lungs were fixed for further analysis.
Experiment
Experimental design
Lung surgery and decellularization
All the animal works were approved and done in accordance with established protocols by the Institutional Animal Care and Use Committee of the University Health Network. These studies used 14–16 weeks of C57BL/6 male mice (Jackson Laboratory, Bar Harbor, ME). After euthanasia, the chest cavity was opened, and blood was flushed via injection of phosphate-buffered saline (PBS) (Thermo Fisher Scientific, San Diego, CA) through the right ventricle. PA and Trachea were cannulated, and the heart-lung block was extracted and stored in a solution of PBS and 1% antibiotic-antimycotic (Thermo Fisher Scientific) at 4°C. The decellularization protocol was completed as previously described.15,16
In brief, the extracted heart-lung block was stored in distilled water (dH20) at 4°C for 1 h followed by perfusion of airways and vasculature with dH20. Samples were then stored in 0.1% Triton X100 solution at 4°C overnight. This was followed by another wash with dH20 and stored in 2% SDC solution at 4° for 24 h. Samples were then washed with dH20 and stored in sodium chloride (NaCl) solution at room temperature (RT) for 1 h followed by another round of dH20 and storage in DNase (Thermo Fisher Scientific) solution at RT for another hour. After this step, airways and vasculature were washed by PBS and decellularized lung stored in PBS and 1% antibiotic-antimycotic solution (Thermo Fisher Scientific) at 4°C.
Cell culture
In this study, human bronchial epithelial (BEAS2B) cells (ATCC, Manassas, VA) were used for the repopulation of lung scaffold airways. For the repopulation of lung scaffold vasculature, mouse endothelial cells (C166) (ATCC) were used. Beas2b and mC-166 cells were cultured in 89% high-glucose content Dulbecco's modified Eagle's medium (DMEM) (Thermo Fisher Scientific) containing 10% fetal bovine serum (Thermo Fisher Scientific), and 1% antibiotic-antimycotic (Thermo Fisher Scientific). Cells were stored in a standard incubator (95% air and 5% CO2 at 37°C). Every 2 to 3 days, the cell culture media was changed, and cells were passaged once they reached confluency (1 × per week). Before seeding, Beas2b and mC-166 cells were trypsinized, counted using Vi-CELL™ Cell Viability Analyzer (Beckman Coulter Life Sciences, Indianapolis). Five million mC-166 cells and 2.5 million Beas2b were resuspended in 20 and 1.5 mL of cell culture media, respectively.
Gravity perfusion cell seeding setup for reepithelialization and reendothelialization
Gravity perfusion seeding (Gr) was performed as previously described.13,17 For reepithelialization, the cell suspension was elevated to the height of 1 m in reference to the decellularized lung and connected to the tracheal inlet via a tube (ID = 3.1 mm; Cole-Parmer, CA). This height elevation resulted in a pressure gradient of 80 mmHg between the cell suspension reservoir and the seeding chamber, providing the required driving force to push the cells into the decellularized lung airways. For reendothelialization, the same procedure was followed; however, the inlet was connected to the PA (Fig. 1G).

NPCS system facilitates higher lung expansion and cell suspension flow rates for lung reepithelialization.
NPCS system setup for reepithelialization
The NPCS system consisted of a syringe pump, a sealed primary chamber (500 mL) containing the decellularized lung suspended in air with two inlets and a secondary reservoir (50 mL) for the cell suspension open to the atmosphere. One of the inlet tubes (ID = 3.1 mm) connected the primary chamber to a syringe pump was responsible for generating the vacuum. The second inlet tube was connected the tracheal cannula to the cell suspension reservoir. The cell suspension was maintained at an equal height (8 cm) to that of the decellularized lung to ensure that there is no hydrostatic pressure gradient between the cell suspension and the decellularized lung. To generate the vacuum, the syringe pump was programmed to withdraw air from the primary chamber, causing the lung to expand, drawing fluid from the secondary reservoir into the trachea and airways themselves. The pump was programmed to withdraw air (up to 60 mL total) at rates of 200, 50, or 12.5 mL/min.
NPCS system setup for reendothelialization
The NPCS system consisted of a syringe pump, a sealed primary chamber (500 mL) containing the decellularized lung suspended in air with two inlets and a secondary reservoir (50 mL) for the cell suspension open to the atmosphere. One of the inlet tubes (‘ID = 3.1 mm) connected the primary chamber to a syringe pump was responsible for generating the vacuum. The second inlet tube was connected the PA cannula to the cell suspension reservoir. The cell suspension was maintained at an equal height (8 cm) to that of the decellularized lung to ensure there is no hydrostatic pressure gradient between the cell suspension and the decellularized lung. To generate the vacuum, the syringe pump was programmed to withdraw air from the primary chamber, causing the lung to expand, drawing fluid from the secondary reservoir into the PA and lungs. The pump was programmed to withdraw air (up to 60 mL total) at rate of 100 mL/min.
Calculation of cell suspension flow rates
A digital clock was used to record the time required for the cell suspension to travel from the container to the PA. The clock was started when cells entered the PA inlet tube and stopped at the instant when the entire cell suspension passed from the inlet to the lung. The flow rate was calculated by dividing the cell suspension volume (1.5 mL, for reepithelialization and 20 mL for reendothelialization) by the measured time.
Vascular perfusion and culture phase for repopulation of lung scaffold airways
After seeding, the NP50 and Gr groups were allowed 18 h of static culture to facilitate initial adhesion. Seeded lungs were then transferred to a perfusion bioreactor. Vascular perfusion through the PA was initiated to provide means of nutrient delivery and waste removal. Perfusion was achieved by a Masterflex L/S Precision Modular Drivers with Bench Top Controller and at the rate of 1.5 mL/min for 5 days. During the culture phase, bioreactors were placed in a standard incubator (95% air and 5% CO2 at 37°C), and cell culture media was changed every other day.
Histology and fluorescence staining
A 10% formalin solution was injected intratracheally into the sample and stored at RT overnight. Samples were then transferred into 70% ethanol solution and processed using the Excelsior ES Tissue Processor (Thermo Fisher Scientific). Processed samples were embedded in paraffin blocks. Three or four 5 μm whole lung sections were prepared for each lung. Sections were then stained by hematoxylin and eosin (H&E) and 4′,6-diamidino-2-phenylindole (DAPI) using established protocols in the laboratory. H&E slides were prepared according to established protocols 18 and achieved by deparaffinization, followed by incubation in hematoxylin (3 min) and eosin (1 min). Nuclear staining was achieved by deparaffinization followed by incubation with 2 mg/mL DAPI (Sigma, Ronkonkoma, NY) for 5 min. Slides were covered using a standard coverslip and scanned using the Aperio slide scanner (Leica Biosystems).
Image analysis of histology sections
The scanned images were processed with HALO™ software (Indica Labs, Albuquerque, NM). The output of this software is a colorized image, which demonstrates the global distribution of cells on the scaffold as well as the quantified surface coverage area occupied by cells and scaffold. For each whole lung section, five examples of cells and scaffolds were introduced to the software manually. A classifier was set at a resolution of 1.04 μm/pixel and a minimum object size of 20 μm.
2
The cell surface and scaffold area were used in the formula shown below to obtain cell surface coverage percentage:
The obtained value then normalized to surface coverage percentage for native lung and reported.
Histology semiquantitative image analysis
The same set of images analyzed by HALO were randomized and given to five observers who were asked to score the H&E images based on surface coverage on a scale of 1 (0–10% coverage) to 7 (60–70%+). Observer values were tabulated and averaged.
Real-time polymerase chain reaction for repopulation of lung scaffold airways
To estimate the relative cell number in recellularized lungs, sixteen 10-μm thick sections were taken randomly from paraffin blocks and pooled for genomic DNA extraction using QIAamp DNA FFPE Tissue Kit (Qiagen; CA) as per the manufacturer's protocol. Real-time polymerase chain reaction was performed on gDNA to detect levels of human Glyceraldehyde-3-Phosphate Dehydrogenase (GAPDH F-CTGGGCTACACTGAGCACC, R-AAGTGGTCGTTGAGGGCAATG, Primerbank ID 378404907c3) in mouse lung scaffold using PowerUp SYBR Green Master Mix (Thermo Fisher Scientific, Waltham, MA). The values were normalized to tissue section surface area.
Statistical analysis
To determine statistical significance in the measured cell suspension flow rates, and cell surface coverage at 18 h, a one-way analysis of variance with Dunnett's post hoc analysis was done. For the statistical significance of cell surface coverage and gene expression analysis at 5 days after cell seeding, a paired Student's t-test was used. Any p-value <0.05 was considered statistically significant.
Experimental Results
NPCS system results in a more significant expansion of lung scaffolds and higher cell suspension flow rates
The gravity-based perfusion and NPCS system were set up as described in detail in the Methods section and represented schematically in Figure 1G and H. In gravity-based perfusion cell seeding, cells are forced through the scaffold via the generated hydrostatic pressure differential between the cell suspension and main reservoir. In contrast, NPCS resulted in the cells being drawn into the scaffold via the pressure gradient generated between the cell suspension and the main reservoir.
Native mouse lungs were decellularized as previously described. 16 Decellularization was confirmed morphologically (Fig. 1B), by H&E (Fig. 1D) and nuclear staining with DAPI (Fig. 1F), which showed no cells in the scaffold in contrast to native lungs, which show clearly defined cells in the airways and parenchyma (Fig. 1A, C, and E). In both systems, 2.5 × 106 BEAS2B cells were delivered to decellularized scaffolds via the trachea and lungs were morphologically evaluated during cell seeding. The morphological evaluation showed that the volumetric expansion of the lung scaffolds seeded via negative pressure was significantly more than those seeded by gravity-based perfusion (Fig. 1I, J).
In contrast to gravity-based perfusion, our NPCS system allows for control over the cell suspension flow rate by changing the ARR. Gravity-based perfusion cell suspension flow rates were significantly lower than those achieved using the NPCS system. NPCS allows for modulation of cell suspension flow rates over the range of 0 to ∼20 mL/min (Fig. 1K).
NPCS results in greater airway cell surface coverage after 18 h of static culture
To determine if higher ARR results in better scaffold cell surface coverage, we evaluated cells seeded via 12.5, 50, and 200 mL of air per minute. These were compared to gravity-seeded lungs. Decellularized lungs were seeded with BEAS2B cells using either gravity-based perfusion (n = 4) or NPCS (described in detail in the methods section) at the selected air removal rates (n = 4 for each group). After seeding, seeded cells were subject to 18 h of static culture to allow adhesion to the decellularized scaffold. Qualitative assessment of histology showed cells distributed in the lung scaffolds using both methods of cell delivery (Fig. 2A–D) and with higher cell surface coverage in the scaffolds seeded using the NPCS system. These observations were confirmed using nuclear staining (Fig. 2E–H).
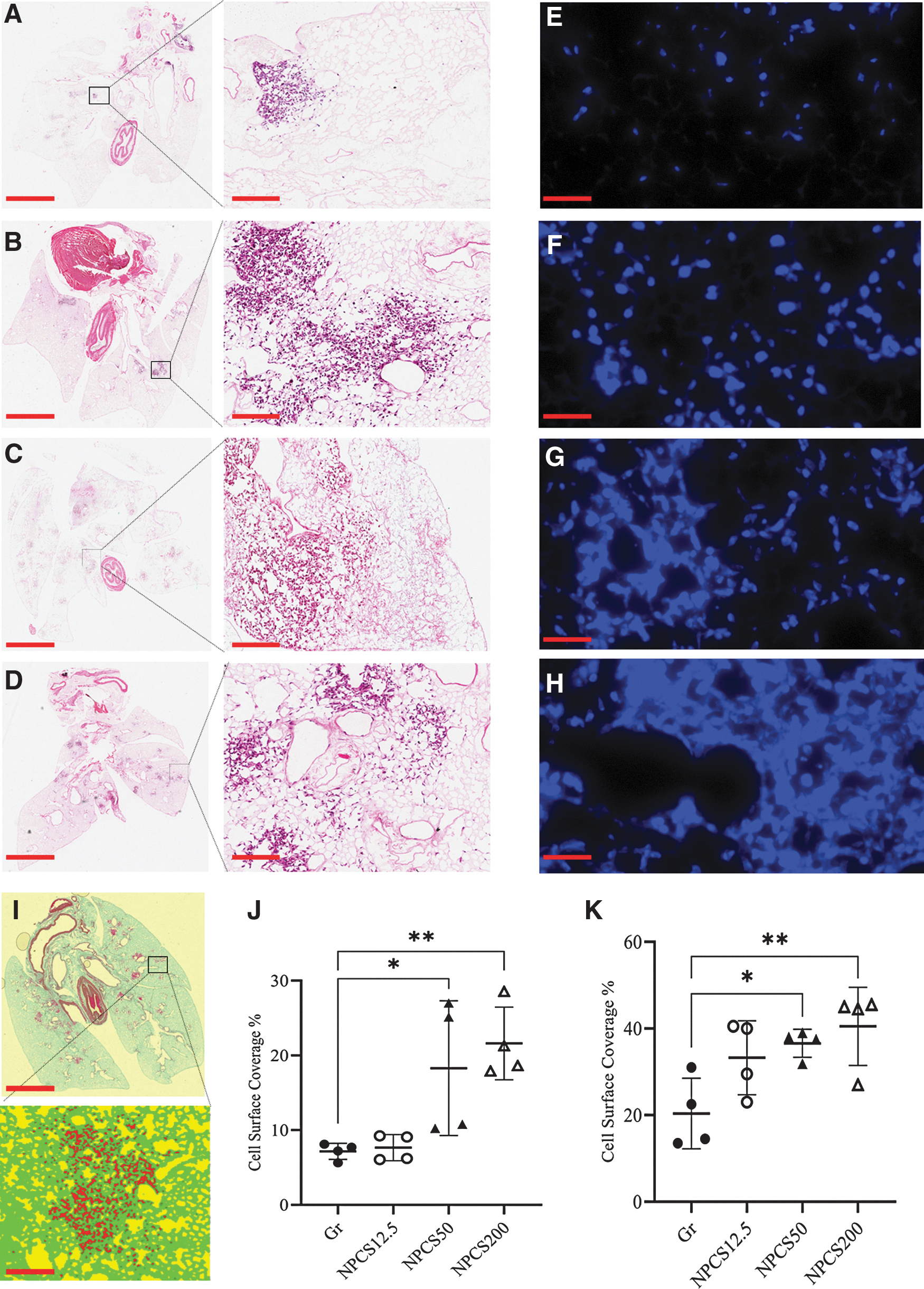
NPCS results in enhanced cell surface coverage after 18 h of static period. Whole lung H&E-stained samples of lungs seeded via
To quantify cell surface coverage, two approaches were used, the HALO image analysis platform and a semiquantitative scoring by blinded observers. Both quantification approaches showed that air removal rates of 50 and 200 mL/min resulted in significantly higher cell surface coverage (Fig. 2J–K). Taken together, our results suggest that NPCS, particularly at the higher cell suspension flow rates of 9.82 ± 0.20 and 19.42 ± 1.33 mL/min, results in better coverage than that achieved using gravity-based cell perfusion (0.93 ± 0.05 mL/min) at 18 h after cell delivery. The time required to inject the cell suspension was 13.4 ± 0.4, 9.2 ± 0.2, and 4.6 ± 0.3 s for NPCS and ARR of 12.5, 50, and 200 mL/min, respectively; and 96 ± 4.9 s for gravity-based perfusion.
NPCS system results in greater airway cell surface coverage and cell number after 5 days of culture
We next evaluated if the initial increase in cell surface coverage is maintained after a more extended period of culture by assessing the recellularization of lungs over a 5-day culture period. For these and subsequent experiments, we used ARR of 50 mL/min as this ARR had a significantly higher cell surface coverage compared to gravity-based perfusion and there was no significant difference in cell suspension coverage when compared to the ARR of 200 mL/min. In addition, achievement of the ARR 200 mL/min was logistically more challenging to set up. For these studies, cells were seeded using either gravity-based perfusion (n = 3) or NPCS at an ARR of 50 mL/min (n = 3), and after an 18 h static period, were cultured under vascular perfusion for 5 days. At the end of the 5-day culture period (Supplementary Fig. S1), lungs were processed and analyzed as those of the 18-h static culture experiments.
Qualitative histological evaluation of recellularized lungs in the NP-seeded lungs (three sections per lung) showed that cells are distributed in the scaffold with cells observed in the distal (Fig. 3C), proximal (Fig. 3E), and pleural regions (Fig. 3G). In particular, scaffolds seeded via NPCS showed dense coverage of the pleural region and complete coverage in proximal airways. Cell surface coverage was consistent across all lungs in the NP-seeded group. While the distribution of the cells in the gravity-based perfusion group was similar in that cells could also be found in the distal (Fig. 3D), proximal (Fig. 3F) and pleural regions (Fig. 3I), there was considerably higher inconsistency in the distribution of the cells across the lungs in this group.
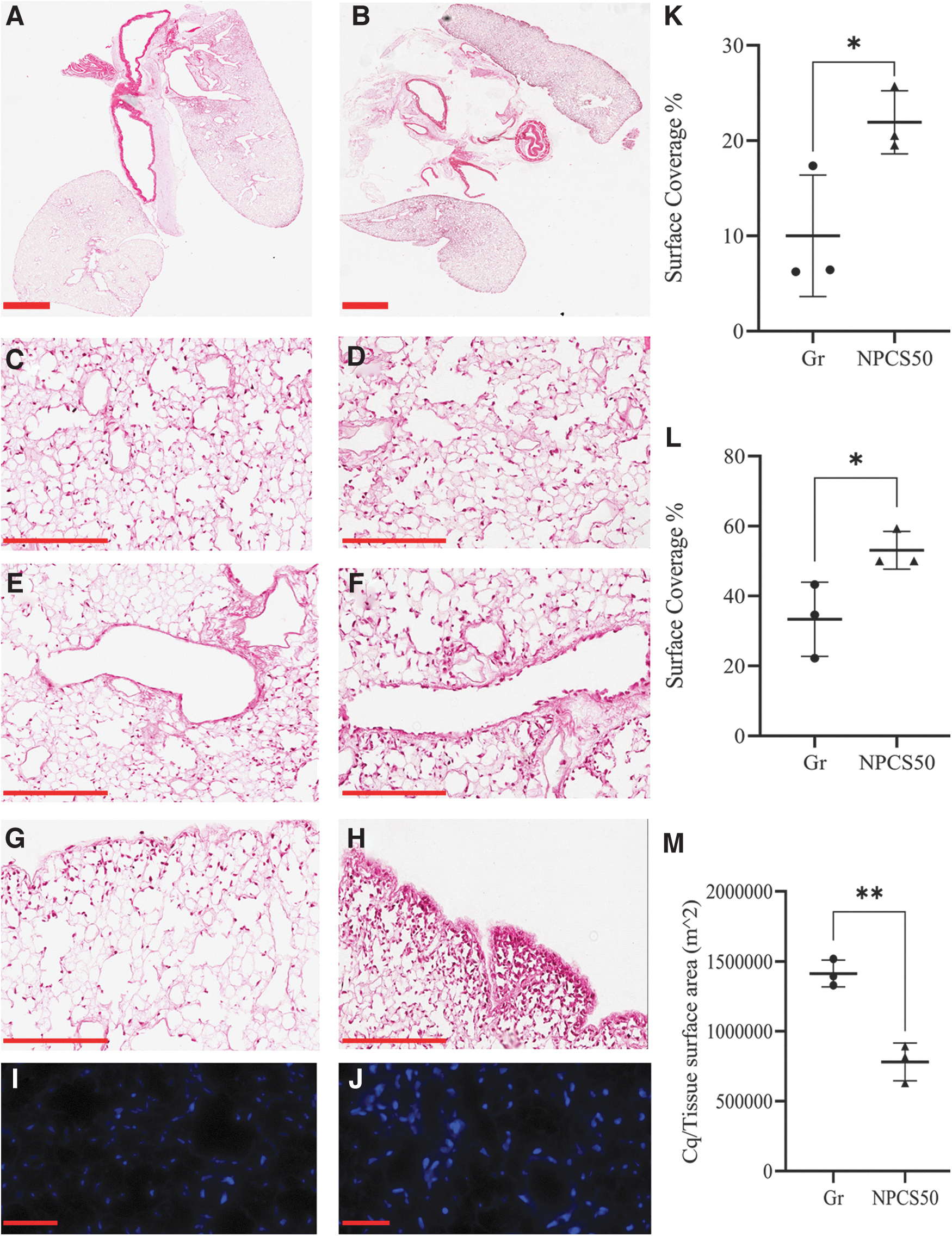
NPCS enhances the reepithelialization process after 5 days of culture. Negative pressure (50 mL/min air removal rate) versus gravity perfusion cell seeding after 5 days of culture. Whole lung slices stained with H&E of lung scaffolds seeded with
Histology images also showed higher cell surface coverage in the negative pressure seeded lungs in comparison to the gravity-based perfusion seeded group (Fig. 3A, B). These results were confirmed by DAPI nuclear staining, which confirmed that the NP-seeded lungs had a higher number of cells in the scaffold after 5 days of culture (Fig. 3I, J). For quantification, whole lung sections were assessed using HALO image analysis (Fig. 3K) and observer-based image scoring (Fig. 3L), confirming a significantly higher percentage of cell surface coverage in the cultured lungs, which were seeded via NP. To confirm the image analysis, we measured human cellular DNA content and confirmed a significantly higher expression of human GAPDH in lungs seeded using NP (Fig. 3M). Our results confirm that the observed benefit of NPCS remains even after sustained perfusion culture, highlighting the importance of the cell delivery stage in lung recellularization.
NPCS results in greater vasculature cell surface coverage after 18 h of static culture
We performed proof-of-concept studies evaluating the effect of negative pressure for the repopulation of lung scaffold vasculature. In these set of experiments, we compared gravity-based perfusion systems (Fig. 4A) and an ARR of 100 mL/min for NPCS (Fig. 4B). Decellularized lungs were seeded with mC166 cells using NPCS (n = 3) and Gr (n = 3). After seeding, lung scaffolds were maintained in static conditions for 18 h to establish adhesion to the decellularized scaffold. To identify cells within the scaffolds, lungs were evaluated histologically and using DAPI nuclear staining. Qualitative assessment of the histology showed cells distributed in the lung scaffolds using both methods of cell delivery (Fig. 4C, D) and with higher cell surface coverage in the scaffolds seeded using the NPCS. These observations were confirmed using nuclear staining, showing cells deposited in the vasculature (Fig. 4E–F).
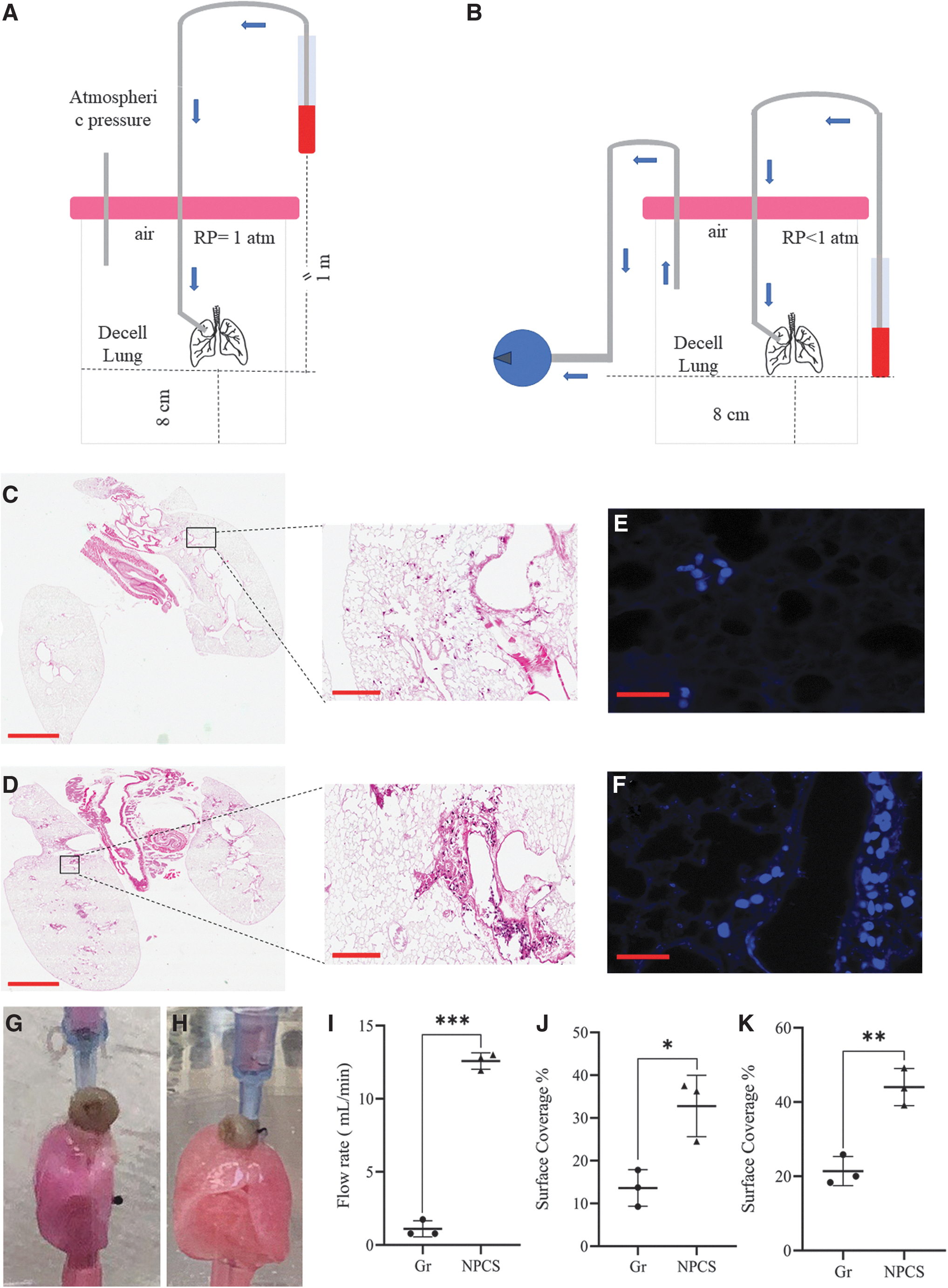
NPCS results in enhanced vascular cell surface coverage after 18 h static period: Schematic representation of
Morphological evaluation showed that the expansion of the lungs seeded via negative pressure was dramatically more significant than those seeded by gravity-based perfusion (Fig. 4G, H). The cell suspension flow rates generated using NPCS was 12.58 ± 0.56 mL/min, which was significantly higher when compared to gravity-based seeding and generated flow rate of 1.10 ± 0.55 mL/min (Fig. 4I). Both HALO image analysis (Fig. 4J) and semiquantitative scoring (Fig. 4K) quantification approaches showed that NPCS results in enhanced cell surface coverage. Taken together, our results suggest that NPCS results in better scaffold vascular coverage than that achieved via gravity-based seeding methods.
Discussion
While other stages of the recellularization process, such as the incorporation of different growth factors and mechanical cues similar to what might be seen in vivo, have been studied extensively, there has been very little focus on the initial delivery of the cells into decellularized lungs. The most common method for the delivery of cells into acellular lung scaffolds is via gravity-based perfusion. However, this method does not allow for precise control over cell delivery. Our observations suggest that this is attributed, in part, to the low and variable cell suspension flow rates, which are limited by the initial injection driving force (e.g., height elevation for gravity perfusion). There are intrinsic variables such as differences in airway compliance and method of cannulation that would always affect the cell suspension flow rates regardless of cell delivery method used. However, our results showed that the use of negative pressure during the cell seeding allows for control over and reproducible cell suspension flow rates. This initial step of cell delivery is particularly important as it is the only stage, in which the user can control the distribution of cells in the scaffold.
While culture techniques such as vascular perfusion or ventilation can partially enhance the distribution within a single lobe, their impacts are limited by the cell number initially retained in the scaffold. In this study, we used a negative pressure-based system (modelling inhalation) to seed cells in decellularized lung scaffolds. It was observed that the rate of vacuum generation via air removal directly correlated (R 2 = 0.9981, cell suspension flow rate = 0.0679*ARR [mL/min] ± 6.121) to cell suspension flow rates with higher rates of air removal resulting in higher cell suspension flow rates. Air removal rates of 50 and 200 mL/min resulted in significantly higher cell surface coverage of lungs in comparison to gravity-based cell seeding. Perfusion culture of lungs seeded with negative pressure at an ARR of 50 mL/min showed that the difference in cell surface coverage is maintained, thus confirming the importance of cell delivery.
We can only speculate as to the exact mechanisms, which result in improved cell delivery in the context of negative pressure cell delivery. First, the velocity of fluid flow is much higher in NP perfusion than in gravity-based perfusion. Such higher fluid flow rate can be correlated to higher cell surface coverage as Kim et al. have shown that high cell suspension flow rates result in further cell attachment using positive pressure-induced flow in native rat and pig lungs. 19 Fluid perfusion rate can be optimized to enhance cellular deposition, with reduced deposition seen in both high amd low flow states. 20 While the exact mechanism by which this increased flow rate is generated in the context of negative pressure is unclear, there are several possibilities. Expansion from outside the organ, via “pulling” of the remaining elastic fibrous structure of the scaffold clearly leads to decreased resistance of the perfused channels.
In addition, since the channels through which the cells are flowing are porous to the fluid media carrying the cells, the pressure differential applied externally in gravity-based perfusion may be dissipated as the fluid (but not the cells) leaks out at the first opportunity. Cells remaining in the vessel lumen may be increasingly compacted, further augmenting fluid egress across the wall of the proximal vessels, plugging the channels, and further reducing flow rate. Negative pressure, in contrast, may “pull” both fluid and cells farther into the vessels and avoid this proximal loss of carrier flow. If proven correct with additional studies, this explanation might help explain why other organs, never physiologically exposed to negative pressure, may benefit from negative pressure seeding.
Finally, resistance to deformation or expansion of the lung during gravity-based cell seeding can be primarily attributed to the compliance of the vascular and airway networks, which is further reduced by external pressure. Negative pressure cell delivery in both revascularization and reepithelialization is achieved by removing air from the main reservoir, thus decreasing the external forces on the vascular and airway networks. This decreases the overall resistance and results in expansion which facilitates cell suspension access to the distal sites. There have been several studies that used negative pressure to enhance the seeding of decellularized kidney scaffolds.21–24 To the best of our knowledge, this is the first protocol for seeding an acellularized lung using negative pressure.
Gravity-based perfusion is used in the majority of revascularization studies but is limited by low cell suspension flow rates. This, in combination with the high resistance of the vasculature, can limit the recruitment of the vascular network and the repopulation of smaller vessels.14,25 Calle et al. have shown recellularization using positive pressure flow (3 mL/min) in rat lung scaffolds. NPCS, by reduction of resistive external pressures and facilitating higher rates of cell suspension flow rates, can result in enhanced distribution of cells within the vascular network. Here, we suggest NPCS as an alternative that can considerably reduce the time required for cell delivery to the vasculature and result in enhanced distribution of the endothelial cells over the scaffold.
Our study is not without limitations. First, BEAS2b and mC-166 cells are cell lines, and further experiments need to be carried out to validate our NPCS method with primary lung epithelial and endothelial cells. While we expect to see similar findings with primary cells, the rate of air removal may need to be optimized for each cell type. The culture period was 5 days, a time point determined in preliminary studies, for sufficient growth of Beas-2b cells seeded at the selected concentration. Moreover, the rate of air removal was limited to the power of the syringe pump used. The maximum ARR achievable with this device was 200 mL/min. Herein, we present an alternative, improved approach for initial cell seeding of decellularized lung scaffolds, the benefits of which persist for 5 days in culture during the proliferation process. While we would speculate that there might be downstream effects on cell differentiation as well, these exciting and important questions beyond the scope of this proof of concept study.
Conclusion
In conclusion, by using a novel NPCS method, we were able to increase the cell surface coverage of the lung scaffold leading to enhanced reepithelialization epithelialization after a 5-day culture period. Moreover, NPCS during the reendothelialization phase can enhance the cell surface coverage in the vasculature. This proof of concept study demonstrates a clear advantage over traditional gravity-based cell-seeding protocols in the lung and can potentially be used in cell-seeding protocols of other organ systems. Finally, NPCS proved to be considerably faster and more efficient in distributing the cells in the decellularized scaffold in comparison to existing cell-seeding techniques. This may have significant benefits for clinical translation as seeding of larger preclinical models will require much higher cell numbers.
Footnotes
Acknowledgment
The authors thank Dr. David Romero for thoughtful editing of the article.
Authors' Contributions
M.A. performed experiments, analyzed data, wrote the article and designed the project. P.D. and D.T. assisted in performing experiments and analysis. T.K.W. and G.K. conceptualized and designed the project, supervised the work and contributed to writing the article. All authors reviewed the article.
Disclosure Statement
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
This research is part of the University of Toronto's Medicine by Design initiative, which receives funding from the Canada First Research Excellence Fund (CFREF; C1TPA-2016-18).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.