
Abstract
Three-dimensional (3D) bioprinting is an emerging tissue engineering technology, already with several remarkable accomplishments and with more promises to fulfill. Besides the enduring goal of making tissues for implantation, it could also become an essential tool in the worldwide trend to replace animal experimentation with improved in vitro models for disease mechanism studies, or with new high-throughput pharmacological and toxicology assays. All these require the speed, reproducibility, and standardization that bioprinting could easily provide. However, originating from additive manufacturing with its top-down approach of “filling” a virtual volume with a semifluid (hydrogel) material, the finer internal anatomic structure of the tissues, as well as vascularization and innervation, has remained difficult to implement. Thus, the next frontier in bioprinting is the generation of more anatomically realistic models, needed for ascending to the functionality of living tissues. In this study, I discuss the conceptual and practical barriers still hampering the attainment of this goal and suggest solutions to overcome them. In this regard, I introduce two workflows that combine existing methods in new operational sequences: (1) bioprinting guided by images of histological sections assembled in 3D constructs and (2) bioprinting of bidimensional vascular patterns implemented among stackable cellular layers. While more sophisticated methods to capture the tissue structure in 3D constructs certainly exist, I contend that extrusion bioprinting may still offer a simple, practical, and affordable option.
Impact statement
Paucity of anatomic structural details is one of the limitations of three-dimensional bioprinting toward fulfilling its potential for tissue engineering, drug testing, and toxicological assays. The origins of this problem can be tracked back to derivation of bioprinting from inorganic additive manufacturing, making it more adept to render the shapes of the objects than their content. As solutions, I suggest two simple workflows that can be implemented by most current bioprinters, based on the import into the construct design of anatomically realistic structural information. If more largely adopted, these and similar approaches may significantly improve the applicability of bioprinted constructs.
State of the Field
After almost two decades of progress that started with a courageous idea, 1 three-dimensional (3D) bioprinting has become one of the most promising biofabrication tools for tissue engineering. 2 It already generated numerous “proofs of concept,” mostly for in vitro applications.3,4 However, bioprinting is still perceived as underdelivering on its basic promise: namely, to produce realistic tissue models not only for experimentation and drug testing but also for implantation.5–7 A recent critical assessment of the field did not find the clinical translation of bioprinting possible for several additional years, if not decades. 8 This situation is explained, in part, by the difficulty to integrate bioprinted constructs in the current health care paradigm, which could not yet accommodate many other tissue-engineered constructs either. 9
However, the main issues are related to the very concept of “bioprinting,” and with the way this has been implemented thus far. In a way, bioprinting still bears the imprint of its origin, namely its derivation from the “additive manufacturing” of inorganic materials (plastics, resins, ceramics, metals etc.). In this method, the structure of the object is generally uniform, and what defines its properties is the volume and shape. To date, the main computer-assisted design (CAD) approach to make printable models remained image thresholding (segmentation), followed by isosurface extraction, and the generation of “stereolithography” (
Thus, in the additive manufacturing workflow used in bioprinting so far, the construct is seen as a volume that is filled with what it is meant to contain. 11 However, the biological tissues and organs are fundamentally different: they develop organically from inside out, in well-controlled stages of cell differentiation. This process leads to structures with optimal distances between cells, permitting a rich intercellular communication by direct or mediated through extracellular matrix contact, by diffusive paracrine signaling, or by exosomes. In bioprinting, this cell proximity is largely absent or hampered by the substantial amounts of crosslinked hydrogels needed for generation of a stable shape. 12
To address this issue, the pioneers of bioprinting envisioned alternative robotic methods to generate 3D constructs made from cells only.13,14 A “scaffold-free” bioprinting approach was thus proposed, and later implemented in several embodiments. One of the commercial instruments uses cell spheroids, brought and temporarily maintained in contact in a microneedles array, in a technique known as the “Kenzan” method. 15 In a “hybrid” version, the spheroids are temporarily embedded in supportive hydrogels, 16 as in two other well-known commercial technologies.17,18 In all these cases, the construct shapes are predesigned on the controlling computers. The details are limited, as it is often the case. by the method's resolution, which, in this study, is either that of one spheroid (compacted 19 or manipulated in place individually 15 ) or that of the preformed rings 20 or “honeycomb”-like building blocks. 21 In practice, this resolution is slightly better when taking into consideration the predictable self-assembling of the cells within spheroids in cell layers, 22 or bundles. 23 Thus, in this technology, the cellular structures are determined, in large part, by the ability of the cells to self-assemble, with the contribution of both biophysical (energy minimization during spheroid fusion 24 ) and purely biological (intrinsic cellular dynamics such as moving, division, and/or cell death 25 ) factors.
Regarding the hydrogel-based bioprinting of in vitro models for mechanism discovery, drug testing, or toxicological assessment, these have been reviewed elsewhere. 26 I will add only that scaffold-free bioprinted (mainly spheroid based) assays have also been developed to test the effects of cardioactive and other drugs. 27 Moreover, the hybrid bioprinting 16 has been applied for drug testing in models of liver28,29 and intestine, 30 or for modeling tumor growth. 31
The more widespread hydrogel-based bioprinting methods have conceivably attempted to capture details of the inner structures of tissues, but these were limited mostly to larger voids such as heart chambers or the coronary vessels. 32 A reason for this preference is that tissue perfusion is not only the cornerstone of successful tissue engineering but also one of the unsolved problems of the field. To fill this gap, NASA launched an ongoing “Vascular Tissue Challenge,” 33 which enlists bioprinting besides other methods hoped to produce the needed progress in this area.
Much of the effort in construct vascularization was directed so far to create perfusable channels inside the constructs by using sacrificial materials, either solid34,35 or viscous, 36 endowed at best with an endothelial layer. Self-standing vascular tubes with more anatomically accurate structure (i.e., containing two layers of vascular cells) have been also created by coaxial bioprinting, in some instances using vascular extracellular matrix, 37 but an anatomically realistic branching pattern was usually ignored. Thus, there is a good opportunity for innovation in this area, with some promising precedents particularly by using the direct-write (“bioplotting”) bioprinting approach,38–40 but this remained an underdeveloped technology so far.
In the paradigm of “scaffold-dependent” bioprinting, other meritorious efforts have been made to capture the inner structure of tissues and organs from medical images using truly 3D (“voxel-by-voxel”), rather than “layer-by-layer” approaches. However, few of those have cellular-level resolution, and currently, the most considered approach capable to produce such “voxelated materials” remains inkjet-based 3D printing. 41 Recently, it was reported the fabrication of voxelated soft matter using a high-frequency, multimaterial, and multinozzle printing method, in which the composition, function, and structure of the materials are programmed at individual voxel level. 42 Still, this technology is restricted to expert laboratories, and with applicability demonstrated for only a few selected materials.41,42
Proposed Solutions
3D reconstruction of histological sections
In this study, I suggest a simpler, more accessible solution to the problem of incorporating natural cellular patterns within bioprinted constructs: instead of designing the construct's volume and then virtually sectioning it in layers for printing, to directly use the images obtained from anatomic sections of actual tissues to instruct a high-resolution in-plane printing of stacked layers. The advantage of this approach would be that in these images is already captured a wealth of structural information, which can be first transferred into “2.5-dimensional” (or 2.5D) models, 43 by giving them a finite thickness, and then combining them in stacks by the common “layer-by-layer” printing in equivalent 3D volumes that would represent the original tissues.
In the virtual space, 3D tissue shapes are routinely reconstructed from serial sections. 44 For example, an alveolar sac with its feeding bronchiole and the associated arteriole, venule, and capillaries was reconstructed in 3D from human lung serial sections. 45 Of note, to perform this reconstruction accurately, it is important to pay attention to the sections' images and their assemblage to be authentic, that is, not only structurally preserved (not teared, folded etc.) but also to follow the sequence in which they were cut from the tissue, which could be easily lost during processing. To verify the accuracy of this operation, it is practical to track continuous structures such as the blood vessels or bronchioles and nerves, across the stack of sections. 46
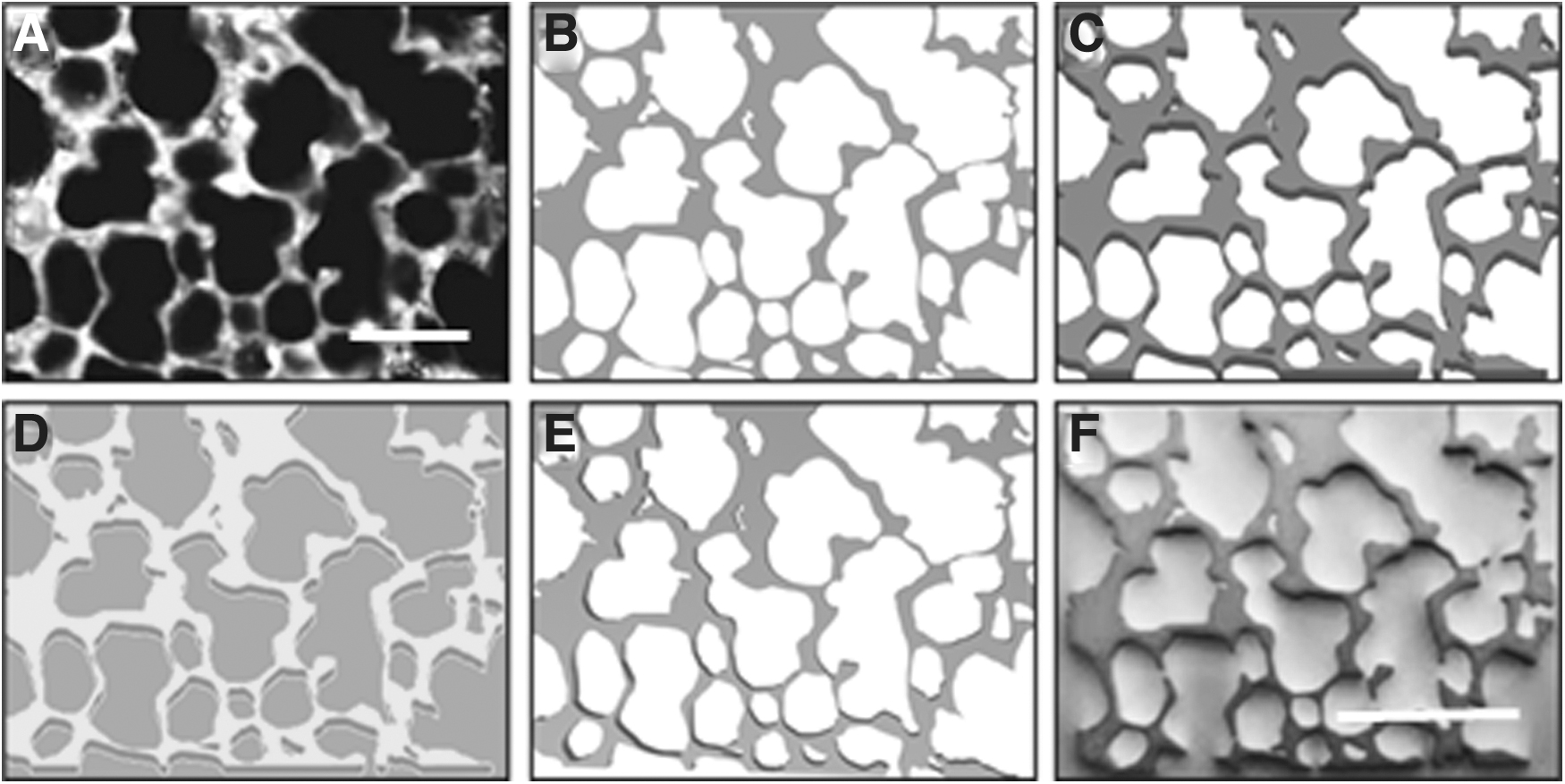
I will illustrate this workflow with two examples of lung tissue, which has a complex microanatomy (of note, for the design of an alveolus, the most realistic bioprinted model so far employed a generic de novo construct, rather than actual lung structural information 47 ). The images can be obtained either from regular histology sections as in Fig. 1 or from confocal fluorescent images (Fig. 2).
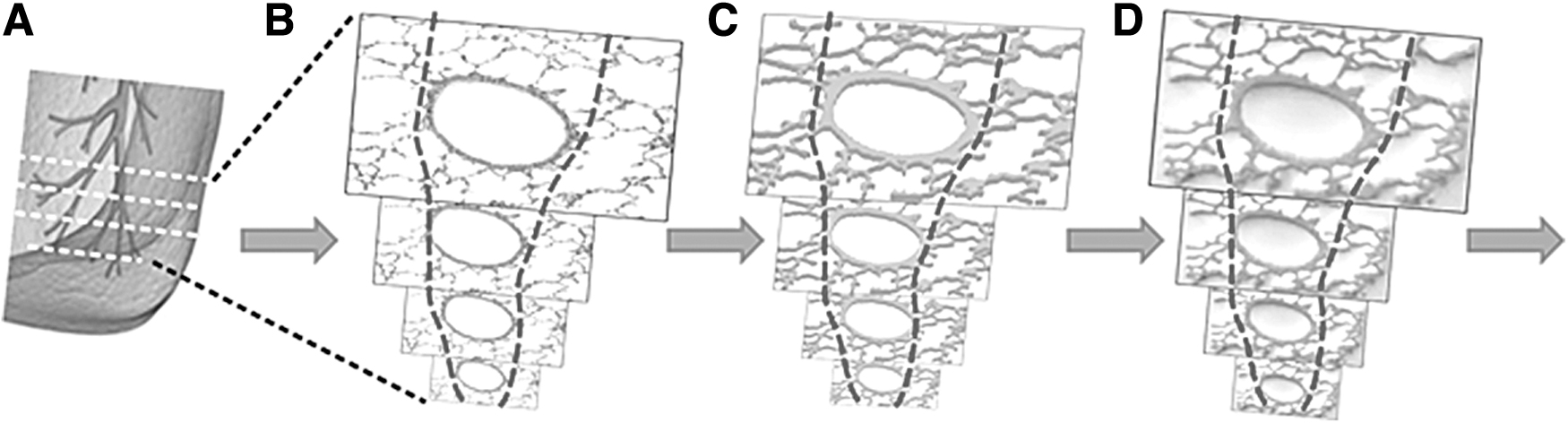
Conceptual workflow for reconstitution by 3D (bio)printing of a tissue fragment from histological section images.
Proposed sequence of image processing steps that lead to a printable object.
The procedure starts with the transformation of section images in their black-and-white equivalents (if not already so, as the fluorescent image in Fig. 2A), followed by image segmentation (Fig. 2B). Then, this image will be converted from pixels into voxels of predetermined size, and thus, the 2D image becomes a virtual “2.5D” object (Fig. 2C). Importantly, this step could be used as the virtual 3D template of the actual section (either fixed or alive) it derives from, which does have a finite thickness. In particular, living sections (“slices”) of lung,
48
liver,
49
brain,
50
and other origins are remarkably versatile for in vitro experimentation, and also for in silico modeling (suggested in Fig. 2D). Next, the voxelated 2.5D (or “pseudo-3D”) volume of the section with its specific structure could be processed as customarily done for 3D printing, to generate an
Among the additional technical considerations and limitations of this approach, one is that the original serial stack may contain too many sections. If so, this would require a selection of the minimum number of successive images, which together would still maintain enough of the original structural information. 54 Equally important is that the 2.5D conversion of each section making it printable will also make the interlayer spaces uniform on the z axis of the initial microscopic image, which is equivalent to a loss of resolution (“coarsening”). This could be particularly consequential for structures with a significant curvature on the scale length of intersection distance, such as lung alveoli. In that case, a virtual “repairing” of the image, by re-rounding of the inadvertently flatted details, might be necessary and possible, using computer-assisted modeling. Moreover, this proposed methodology does not by itself guarantee a cell-level resolution, which depends on the available hardware and software; it only makes it possible with adequate tools. In fact, the resolution of the currently available methods imposes one of the most significant limitations to the implementation of anatomic details into bioprinted constructs (Table 1).
Limits Imposed on Section-Based Approach by the Resolution of Current Bioprinting Methods
Also, it is worth noting is that when making the sections, there is always some tissue loss. Combined with the additional correction steps during 3D conversion, in the resulting construct admittedly, there will be missing details of the original tissue. Thus, what is obtained will likely be only a close model of the original, rather than an actual copy, but still sufficient for many applications. How large the difference is can be quantitatively determined either by resectioning and image analysis or assessed by microcomputed tomography or other noninvasive methods.
The benefits of generating such bioprinted models could be multiple. For example, realistic 3D lung models for in vitro experimentation are in high demand and short supply during the Covid-19 pandemic. The most complex models currently available are either “pseudo-3D” models55,56 or the “precision-cut lung slices” (PCLS). 57 The former consists of flat layers of epithelial and endothelial cells, possibly containing fibroblasts and/or macrophages. In this category is the commercial EpiAlveolar system, used for the study of the effects of particulate pollutants 55 and the molecular inducers of pulmonary fibrosis. 56 Alternatively, for the same and a variety of other investigations, such as in vitro alveologenesis, 57 PCLS could be used, which are thin living sections from human lung. However, these “pseudo-3D” systems either lack the true alveolar organization, which completely changes the diffusion of molecules and the contribution of the bronchiolar and capillary system, or the cell composition and their local arrangements (as in PCLS, which are inherently cut from nonidentical segments of the organ) cannot be standardized, and thus would compromise the interwell reproducibility expected from high-throughput assays for drug discovery. Therefore, an anatomically realistic 3D bioprinted model as proposed in this study, realized with living cells and maintained in optimized conditions, could advance the fields of drug testing and of toxicology.
3D assembling of cellular layers
Another tissue engineering method to generate 3D constructs by stacking layers is based on “cell sheet” technology. 58 In this approach, cells are cultivated to confluency on a temperature-sensitive gel (“thermogel”) and then detached as continuous cell layers and either directly used in a myriad of applications or further stacked to make thicker cell blocks. 59 However, due to the lack of vascularization, these stacked constructs will suffer from hypoxia, if more than three cell sheets are overlayed. 60 Therefore, it was proposed to incorporate bioprinted hydrogel layers containing preformed, perfusable endothelium-covered vascular channels between the cell sheets. 61 However, the degree of anatomic realism of these channels was minimal, depriving the constructs of the benefits of naturally optimal fluid distribution. 62
As a solution, I suggest that bidimensional (and eventually 3D) vascular structural information can be directly transferred to the bioprinted constructs from anatomic images by direct-write printing, as schematically illustrated in Fig. 3. This approach is similar to the recently described “Bioprinting-Assisted Tissue Emergence” (BATE) method, which uses stem cells at very high densities to spontaneously self-organize within appropriate hydrogels, while being spatially distributed in linear patterns. 63 In this way, the stem cells that would otherwise develop relatively randomly in organoids are constrained to condense and organize according to the 3D printing-imposed geometry. An analogous method has been proposed for vascular cell organization in the limited confines of gelatin “lines,”38–40 but apparently, no attempt to extract realistic vascular patterns from medical images and to return them to a bioprinted construct has been yet made. Instead, this approach has been considered when transferring a cerebral microvascular pattern by image-assisted laser control combined with laser-assisted hydrogel degradation, leading to generation of perfusable microfluidic channels with dimensions and spatial geometry of the original microvascular network. 64 This work and its larger context were expertly discussed in a follow-up overview. 65
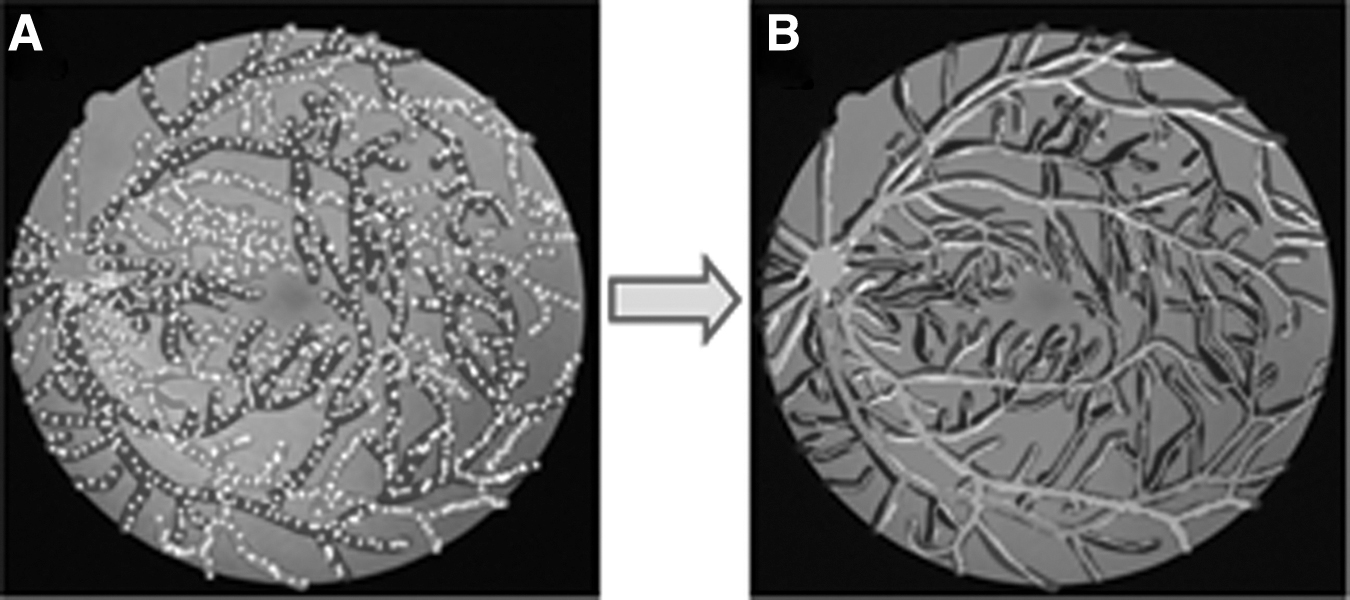
Diagram illustrating the proposed imaging-driven, direct-write printing of a retinal vascular pattern.
These methods leading to channel formation in hydrogel can organize only the vascular (and possibly the neural) systems, and less the nearby cells which—if present—will remain unconstrained in the bulk hydrogel. More additional control over this cell subpopulation can be obtained by direct-writing printing 66 of hydrogel “lines,” as mentioned. However, resolution of this method is still determined in combination, by the extrusion printhead, printing pressure and speed, and the wettability of the surface, as it is the case for extrusion bioprinting in general. 67
As a concrete example, a flat retinal vascular equivalent of human eye fundus could be quite straightforwardly achieved, by keeping track of the specific arteriolar vs. venular branching of the retinal vascular networks (Fig. 3A). After direct-write printing with an adequate hydrogel (e.g., a gelatin-fibrin mix 68 ) and further culture in appropriate growth factor-supplemented medium, the vascular cells are expected to self-organize within the confines of their gel lines that may contain other cells, such as pericytes or mesenchymal stroma cells, in vascular-like patterns 69 (Fig. 3B). The retinal vasculature has the benefit of representing large vascular beds with well-defined, single-access entrance and exit points for perfusion, but other vascular domains might be considered as well. These patterns could then secondarily be embedded in a supporting hydrogel layer and either used as such, or after maturation detached and placed between other cellular layers containing parenchymal cells, as described. 61
Comparatively, the assembly of preformed monolayers allows a much higher cellular density in “x-y” plane and could, at least in principle, provide a better resolution on “z” axis (commensurate with a cell height, which is of few tens of microns) than the direct “layer-by-layer-printing” with a hydrogel. Therefore, the combinatorial use of multiple experimental methods that are currently used in isolation may generate, in the near future, solutions to many of the current bottlenecks experienced in the application of bioprinting to tissue engineering.
Conclusion
In this succinct discussion, I addressed the need and possibilities for a next level of anatomical realism to endow the bioprinted constructs with more physiological properties. These are mainly (1) cellular-level tissue specificity of cell distribution and (2) incorporation in the constructs of self-assembled (micro)vascular patterns and similarly, of neural networks. A “layer-by-layer” design of the workflow would allow the integration in the construct's design of structural information contained in histological sections or in two-dimensional images of vasculature, both of which can be thereafter assembled by stacking in 3D constructs. More sophisticated approaches are nevertheless worthwhile and certainly pursued. However, these require more advanced hardware and different software than the ones currently accessible to the majority of laboratories, while the solutions proposed in this study could be readily implemented with the existing technology.
Footnotes
Acknowledgments
The author is grateful to Indiana Institute for Medical Research at Richard L. Roudebush VA Medical Center for support to the 3D Tissue Bioprinting Core Laboratory, to R. Cadle and D. Rogozea for help with CAD and 3D printing of the examples used for illustration, and to Dr. L. Moldovan for critical reading of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.