
Abstract
Decellularized porcine pericardium has many applications in the cardiovascular field for its excellent properties. The peritoneum is a single-layer bio-dialysis membrane with many similarities and differences in physical characteristics, biochemical composition, and structure to the pericardium. The limited available literature suggests that, similar to the pericardium, the peritoneum has good application potential in the field of cardiovascular substitute materials. This research focused on comparing the differences between decellularized peritoneum and decellularized pericardium in microstructure, biochemical composition, mechanical properties, hemocompatibility, in vitro enzymatic degradation, in vitro calcification, cytocompatibility, and other vital indicators. The peritoneum was consistent with pericardium in terms of fibrous structure, hemocompatibility, in vitro calcification, and cytocompatibility. The peritoneal elastic fiber content (219 μg/mg) was significantly higher than that of the pericardium (66 μg/mg), resulting in two to three times higher maximum load (21.1 N) and burst pressure (1309 mmHg), and better performance than the pericardium in terms of in vitro resistance to enzymatic degradation. In the cardiovascular field, decellularized peritoneum can be used as vascular substitute material.
Impact statement
There are many similarities between the embryonic origin and morphological structure of the porcine peritoneum and the porcine pericardium, but little research has been done on the use of the porcine peritoneum as a biomaterial. In this compared research, we showed that porcine peritoneum had better resistance to enzymatic degradation, better stretching, and more suitable burst pressure for being used as vascular substitute material. This research is the first to describe the structural composition of porcine peritoneum and its advantageous properties as a cardiovascular material.
Introduction
Decellularized matrix materials have been studied, and applied to the preparation of artificial vessels, including carotid arteries, mesenteric veins, and ureters. 1 And some other membranous decellularized matrixes have also been studied and widely used in cardiovascular field, including small intestine submucosa, 2 amnion, 3 peritoneum, 4 and pericardium. 5 When being used as cardiovascular materials, the two most important functional property requirements are (1) the ability to support the adhesion and proliferation of vascular endothelial cell, and to form an endothelial cell layer; and (2) matched mechanical properties, including bursting pressure and elastic modulus. The small intestine submucosa and amniotic cannot be used as artificial vascular replacement materials alone due to their poor mechanical properties, thus only the peritoneum and pericardium have the potential to be used as full-layer replacement vessels.
The porcine pericardium is a promising biomaterial for its low antigenicity, high biocompatibility, and proper biodegradability, and is often used to construct heart valve, vascular patch, dura mater, and bone-guided regenerative collagen membrane. 6 Whereas the peritoneum is a thin biomembrane adjacent to the inner surface of the abdominal wall and has the same embryological origin as the pericardium, consisting of a single layer of mesothelial cells and a sparse connective tissue layer beneath them. The peritoneum is also a semipermeable membrane with numerous blood capillaries distributed in a reticular pattern, which serves as a lubricant and protector of abdominal organ motility, and also has physiological functions, such as leaching, leakage, and secretion. In terms of physiological structure, peritoneum is mainly composed of mesothelial cells, smooth muscle cells, and fibroblasts similar to the cellular composition of the pericardium.7,8
For each 20 kg donor porcine, 800 cm2 of high-quality regular peritoneum can be obtained, whereas only 70 cm2 of high-quality regular pericardium can be obtained. The clinical research on peritoneum mainly focused on dialysis functions. However, in the field of biomaterials, peritoneum is occasionally used as dural grafts, 9 artificial skin, 10 cardiovascular field, 4 and so on. A few exploratory researches in which the peritoneum is also used as a vascular patch indicate its potential for cardiovascular applications. Therefore, to explore the potential of peritoneum for applying in artificial vessel, we compared the differences between decellularized pericardium and decellularized peritoneum when they were used as cardiovascular material materials in microstructure, biochemical composition, mechanical properties, hemocompatibility, in vitro enzymatic degradation, in vitro calcification, cytocompatibility, in vivo degradation rate, and other vital indicators.
Materials and Methods
The decellularization of peritoneum and pericardium
Fresh peritonea were placed in 1% Triton X-100/PBS solution after removing the adherent fat and shaken at 4°C (120 rpm) for 3 h. Subsequently, they were transferred to 0.5% sodium dodecyl sulfate (SDS)/phosphate buffer solution (PBS), and also shaken at 4°C for 3 h (120 rpm). The samples were washed three times with PBS.
The decellularization procedure of pericardium is the same as peritoneum, except that the treatment times of pericardium by 1% Triton X-100/PBS and 0.5% SDS/PBS are 1 and 2 h, respectively.
Characterization of sample surface
Samples were dried at the critical point after gradient dehydration and observed using a field emission scanning electron microscope (SEM, Carl Zeiss, Oberkochen, Germany) after sputtering with gold. The water contact angle (WCA) of sample was measured by a contact angle goniometer (SL200KS, Boston, MA, USA).
Histological observation of samples
Fresh and decellularized samples were fixed in 4% paraformaldehyde for 24 h, and stained with hematoxylin-eosin (HE), Masson, and Verhoeff's Van Gieson (EVG) to observe the morphology of collagen and elastic fibers, respectively.
The content of DNA, collagen, elastin, and cytokines in samples
0.5 g lyophilized tissue samples were placed in sterile microcentrifuge tubes (1.5 mL). The DNA was isolated from tissue-samples using blood/cell/tissue genomic DNA extraction kit (DP304; Qiagen). The DNA concentration was measured by a spectrophotometer (Thermo Spectronic; Biomate 3, Rochester, NY, USA) at 280 nm and total DNA content was calculated according to the DNA concentration.
One gram lyophilized tissue samples were added into 9 mL PBS solution and homogenized thoroughly using a tissue homogenizer. Subsequently, the prepared samples were centrifuged at 5000 rpm for 5 min. The supernatant was collected, and the content of collagen, elastin, and cytokines in supernatant was, respectively, assayed according to the enzyme-linked immunosorbent assay for porcine collagen (JN21515; Jining Shiye), porcine elastin (JN21464; Jining Shiye), porcine vascular endothelial growth factor (JN21626; Jining Shiye), porcine transforming growth factor β (JN21642; Jining Shiye) by an enzyme standardization instrument at 450 nm.
Uniaxial tensile test
Samples were cut into a rectangular strip with a length of 40 mm and a width of 10 mm. Their accurate thickness was measured using a micrometer. The biomechanical test of each sample was operated on Instron material testing machine (Instron Co., USA) at an extension rate of 7 mm/min. The ultimate tensile strain and the ultimate tensile stress were recorded before failure. The ultimate elastic modulus was determined from the stress–strain curves.
In vitro enzyme degradation and in vivo degradation test
In vitro enzyme degradation
All samples were immersed into 1.5 mL Collagenase I/PBS (Elastin enzyme/PBS) solutions (25 U/mL) and incubated at 37℃ with constant shaking. Then, transferred into 10 mM ethylene diamine tetraacetic acid (EDTA) to terminate enzymatic hydrolysis at every interval point (0.5, 1, 3, 6, 12, 24, 48, and 72 h), respectively. Samples before and after degradation were lyophilized. The degradation rate or weight loss percentage (ΔW%) was calculated by the following formula:
11
W0 represented the sample's weight before degradation. Wt represented the sample's weight after degradation.
In vivo degradation test
Sprague Dawley rats were purchased from Experimental and Research Animal Institute, Sichuan University. All animals were anesthetized using 1–2% isoflurane by inhalation. After anesthesia, two subcutaneous pouches were created in the abdomen of each animal. Sterilized decellularized peritoneum and decellularized pericardium (n = 4) by Co60 irradiation were implanted into the subcutaneous. All materials were thoroughly rinsed in 0.9% NaCl before implantation. After recovery from anesthesia, all animals were returned to the animal facilities and fed a standard rat diet. Animals were sacrificed after 30, 60, and 90 days, respectively. After sacrifice, each implantation material was harvested from animals and fixed in 4% formaldehyde for HE staining analysis.
Hemocompatibility measurement
Hemolytic test
The sample was cut into the shape of a square with 1 × 1 cm and placed flat in a 12-well plate. And then equal amounts of RBCs suspension were added to each well and incubated at 37°C for 3 h. After incubation, all supernate was centrifuged at 10,016 g for 3 min, and 100 μL supernatant of each group was transferred to a 96-well plate. Their absorbance of released hemoglobin was tested using a spectrophotometer at 540 nm. The hemolysis rate (%) was calculated as follows:

Platelet adhesion test
Fresh whole blood of healthy rabbits was centrifuged at 1000 rpm for 10 min for platelet-rich plasma (PRP). After samples had been preimmersed in PBS and equilibrated at 37°C for 1 h, PBS was removed. Two hundred microliters PRP was dropped on surfaces of samples to ensure complete immersion. Then, they were cultured at 37°C for another 1 h. These samples were gently washed with PBS to remove non-adherent platelets, and then were fixed with 2.5% glutaric dialdehyde (GA)/PBS solution at 4°C for 8 h. Finally, the prepared samples were gradient dehydrated by ethanol (50%, 70%, 90%, 95%, and 100% in turn) for 10 min, respectively. The morphology and aggregation situation of attached platelets were observed by SEM.
β-TG determination
One milliliter PRP was added to the surface of 1 cm2 sample placed on a 24-well plate. And then this sample was incubated for 1 h at 37°C. The supernatant was collected for β--thromboglobulin (β-TG) measurement. The β-TG content was quantified according to the Rabbit β-TG Elisa kit instructions (JN21708; Jining Shiye).
Calcification assay in vitro and in vivo
The samples were cut into 1 × 1 cm slices and lyophilized. After that, they were sterilized by Co60 irradiation and soaked in 10 mL simulated body fluid (SBF) in a sterile environment, and then slightly uniformly oscillated at 37°C for 30, 60, and 90 days. The SBF was changed per week. When reaching the preset time point (30, 60, and 90 days), the sample was thoroughly washed three times with ultrapure water. SEM and energy dispersive spectroscopy (EDS) elemental analyses were conducted to observe the calcification of samples. The samples were fixed in 4% formalin for 3 days, and then were stained with Von kossa staining to observe calcium nodules on the surface of samples. The tested samples were homogenized using a homogenizer and then digested with acid until the samples were completely dissolved. After dissolution, their absorbances were measured at 660 nm. The amount of Ca in samples was obtained from their absorbances according to the instructions of the calcium assay kit (Arsenic Azo III method).
The subcutaneously implanted samples in the 30th day, 60th day, and 90th day were harvested and stained with Von kossa staining to observe calcium nodules on the surface of sample.
Cytocompatibility test
After human vascular endothelial cells (HVEC) and L929 cells were separately inoculated on sterilized samples (1 × 1 cm) in 24-well culture plates at a density of 1 × 105 cells/mL for 30 min, 400 μL DMEM high sugar medium (with 10% fetal bovine serum [FBS]) was added into each well and cultured for a predetermined period. The culture mediums were changed every 2 days. CCK8 (Cell Counting Kit-8; Beyotime) assays were, respectively, performed on days 1, 3, and 5 to evaluate the cell proliferation. The cell live/dead fluorescent staining assay (Calcein AM; Beyotime) was performed on day 2 to study the adhesion and viability of cells on the surfaces of samples.
Results and Analysis
The structure of decellularized pericardium and decellularized peritoneum
Both freshly isolated porcine pericardium and fresh porcine peritoneum were translucent films with some elasticity, and the former was thinner than the latter. After decellularization and freeze–drying, the peritoneum became a white sheet with dry weight of 9.10 mg/cm2. In comparison, the pericardium appeared a translucent sheet with dry weight of 4.90 mg/cm2 and presented a softer texture. As an additional comparison, the density of commonly used A4 paper is 7.4 mg/cm2. The surface WCA of peritoneum and pericardium ranged from 40° to 50° with no significant difference between them, indicating that peritoneum and pericardium were moderately hydrophilic.
The intact total framework and porous microstructure in decellularized peritoneum and pericardium were all well preserved. However, the porous microstructure in decellularized peritoneum appeared more extensive, which could provide a better microenvironment for cell adhesion and growth. The fiber diameter of the decellularized peritoneum was larger than that of the decellularized pericardium, and the fiber breakage of pericardium was more pronounced after decellularization using the same method (Fig. 1).

Characterization of decellularized peritoneum and decellularized pericardium.
Histological observation of samples
HE, Masson, and EVG staining results showed that the peritoneal tissue structure was clearly stratified, with an inner layer of mesothelial cells, a middle layer of collagen fibers and elastic fibers, and an outer layer connective tissue. The pericardium was composed of a plasma membrane layer, a fibrous layer, and a connective tissue layer, but the stratification was not as obvious as that of the peritoneum. The pericardial collagen fibers are wavy, and their elastic fibers are thin and less abundant. 12 Small-diameter natural arteries are clearly stratified into an intimal layer, an elastic fiber layer, and a connective tissue layer, and about 500 μm thick, whereas the thicknesses of peritoneal tissue, porcine pericardium, and bovine pericardium 13 are, respectively, about 400–500, 260, and 250–500 μm.
Physically, the mesothelial cell layer and the elastic fiber layer of the peritoneum could act as the intimal layer and the elastic fiber layer of natural arteries, respectively. The pericardium is not suitable for acting as arteries with high-flow and high-pressure due to its small thickness and poor elastic fiber content. In contrast, the peritoneum is more suitable for acting as arterial vascular substitute than the pericardium (Fig. 2).

HE, Masson, EVG staining of peritoneum, pericardium, and native artery (dashed lines indicate structural layering). EVG, Verhoeff's Van Gieson; HE, hematoxylin-eosin.
The content of DNA, collagen, elastin, and cytokines in samples
Residual cellular components in biologically derived samples could lead to severe host immune responses after sample implantation. Although the U.S. Federal Drug Administration does not regulate the limits for DNA in biologically derived samples currently, 14 the common minimal standard for decellularized native tissues is <50 ng/mg. However, there are also some research reports in the world, which the biologically derived tissues containing high residual DNA levels (>50 ng/mg) present better repair efficacy after clinical use. 15 The DNA contents in some decellularized tissues (including porcine decellularized esophageal mucosa, porcine decellularized meniscus, porcine decellularized liver, porcine decellularized kidney, porcine decellularized brain tissue, and porcine decellularized aorta) are, respectively, 48, 19.54, 18, 22, 40.2, and 286 ng/mg.
To summarize the international reports, the following three elements need to be satisfied for setting the immunogenicity removal criteria:16,17 (1) DNA residue <50 ng/mg dry weight material; (2) no cell nuclear components were seen in samples underwent standard histological staining; and (3) residual DNA fragment length <200 bp. There was no significant difference in DNA content between the same mass of decellularized peritoneum and decellularized pericardium (38 and 36 ng/mg, respectively), which was inextricably linked to their similar tissue composition. The peritoneum was mainly composed of peritoneal mesothelial cells, smooth muscle cells, and fibroblasts. The pericardium was composed of pericardial mesothelial cells, smooth muscle cells, and fibroblasts. Therefore, for peritoneum and pericardium, the similar tissue composition resulted in a similar amount of DNA per unit mass of decellularized tissue.
Extracellular matrix (ECM) retention is the central goal of decellularization. Collagen, fibronectin, and laminin are important components of the ECM, which are essential proteins for stabilizing the mechanical structure of the ECM and are decisive proteins for cell survival, development, migration, and proliferation, thus servicing as the basic skeletal structure for tissue engineering scaffolds. 18 The total collagen content in fresh peritoneum, decellularized peritoneum, fresh pericardium, and decellularized pericardium was, respectively, 441.1, 415.0, 401.3, and 389.0 μg/mg, and there were no significant differences among groups. However, the elastin content (219 μg/mg) and the vascular endothelial growth factor (VEGF) content (30 pg/g) in peritoneum were about 2.8–3.3 times of pericardium.
This difference is closely related to the similarities and differences in the structure and physiological functions between two tissues. Peritoneum is rich in capillaries and has a much larger store of vascular endothelial cells than the pericardium, 19 resulting in a higher VEGF content in the peritoneum. β-thromboglobulin (β-TG) has been attracting a lot of research work as a bifunctional growth factor. It normally presents in an inactive form stored in the ECM. 20 When inflammation occurs in the organism, TGF-β is activated and is involved in tissue repair and immune system regulation, regulating cell growth, differentiation, matrix production, and apoptosis. Before decellularization, TGF-β levels in the peritoneum and pericardium are comparable. After decellularization, the TGF-β content of peritoneum did not change significantly, whereas the TGF-β content of pericardium decreased significantly. The results indicated that the peritoneum and pericardium retained the vast essential collagen, elastin, and some growth factors after decellularization treatment (Fig. 3).
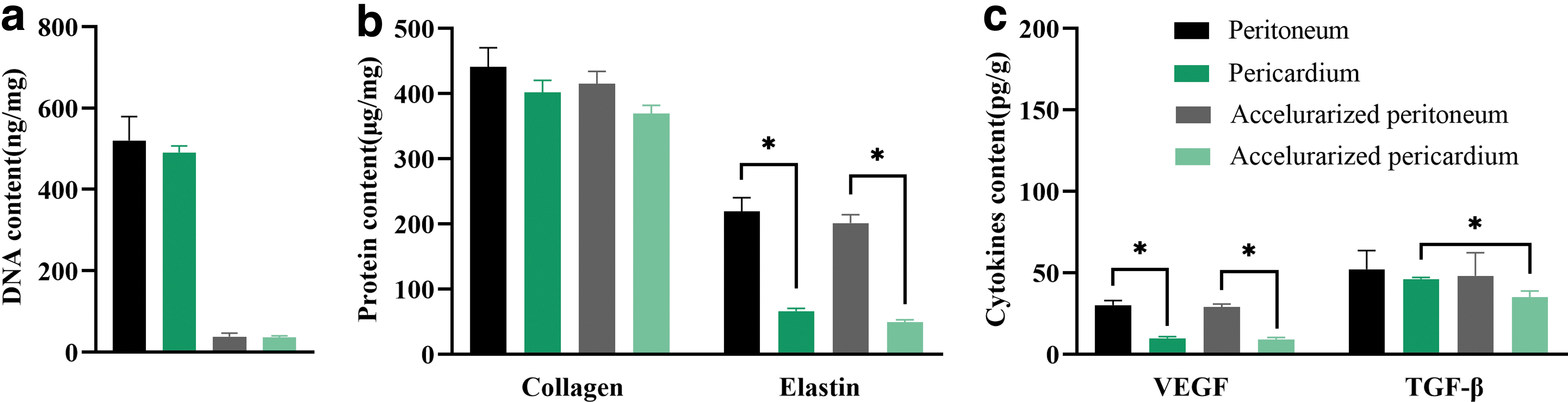
The content of residual DNA
Mechanical properties
Adequate mechanical properties are a fundamental requirement for cardiovascular materials, especially when used in small diameter vascular grafts and artificial heart valves.21,22 In uniaxial tensile mechanical tests, the maximum load (21.10 N) and maximum tensile stress (5.65 MPa) of the peritoneum were significantly greater than those of the pericardium (maximum load for 6.27 N, maximum tensile stress for 4.03 MPa). However, there was no significant difference in modulus of elasticity between them (11.21 and 10.63 MPa, respectively). This indicated that the peritoneal tissue could withstand greater tensile and rupture strengths than the pericardium when they were used as vascular substitute materials, that is, it could withstand greater bursting pressure.
The burst pressure of a material is proportional to its yield stress and thickness. 21 The burst pressure of the peritoneum and the pericardium is about 1300 and 412 mmHg, respectively. The burst pressure of the decellularized peritoneum is significantly greater than that of the pericardium and is close to small-diameter natural vessels. The decellularized pericardium is not suitable for being used as a vascular substitute material and is more suitable for being used as valvular tissue, 22 whereas the decellularized peritoneum have the potential to be used as vascular substitute material (Fig. 4).

Uniaxial tensile mechanical (from left to right, maximum load, tensile stress at maximum load, E-modulus, burst pressure, respectively).
Anti-enzymatic degradation in vitro and in vivo
Collagen and elastin are the major structural proteins in mammals, and they provide mechanical support, strength, and elasticity for various organs and tissues. 23 Both peritoneum and pericardium are rich in collagen and elastin. In vitro enzymatic degradation experiments could provide insight into the contents of collagen and elastin in different tissues, and their ability to resist enzymatic digestion. 24 The degradation rate of collagen I, collagen IV, and elastin within the pericardium was higher than that within peritoneum at all time points. The differences were more significant at 24, 48, and 72 h. Histological staining of samples after enzymatic degradation showed that the collagen fibers and elastic fibers in pericardium were broken more severely compared with peritoneum (Fig. 5).

Anti-enzymatic degradation in vitro results.
At 30th day of subcutaneous implantation, the peritoneum and pericardium did not present significant degradation. At 60th day, the morphology of peritoneum changed, and its degradation was visible, whereas the degradation of the pericardium was more obvious, and the degradation products caused a significant inflammatory reaction. At 90th day, the peritoneum morphology was still visible, but it had degraded into flakes, whereas the pericardium was completely degraded, and almost no degradation products were visible (Fig. 6a). The results observed by HE staining were consistent with the anatomical findings (Fig. 6b). At 30th day, the complete structure of the peritoneum and pericardium could be observed.

Decellularized peritoneum and decellularized pericardium subcutaneous implantation for 90 days.
At 60th and 90th days, the peritoneum still retained its basic structure. But the pericardium was severely degraded, with significant breakage of collagen fibers and a more severe inflammatory response caused by degradation products. From subcutaneous implantation results, pericardium degraded completely within 90 days, whereas the peritoneum presented significantly slower degradation than the pericardium. Both in vitro enzymatic degradation and in vivo degradation experiments showed that the peritoneum was more resistant to degradation than the pericardium and had a good durability during application.
Hemocompatibility
For the blood-contacting material, the hemocompatibility is one of the most important basic criteria of vascular substitute materials to measure whether they could be used as cardiovascular materials. 25 Hemolysis refers to the rupture of cell membranes when red blood cells are damaged. The hemolysis tests of the samples showed that the hemolysis rates of decellularized pericardium and decellularized peritoneum were both <5.0%, which met the safety standards of blood contact materials (the international standard ISO 10993-4: 2017(E), <5%), and indicated the good blood safety of these two materials. 26
Thrombosis, which is mainly attributed to platelet activation and adhesion, is the most potentially disastrous consequence of blood-contacting vascular substitute materials. 27 As shown in Figure 7, some spreading irreversible adhesion platelets were observed on decellularized peritoneum, whereas more firm reversible adhesion platelets were observed on decellularized pericardium. 28 However, the results of β-TG, which is accepted as a sensitive marker of platelet activation in vivo, 29 showed that the β-TG level released from the platelets in decellularized pericardium was similar to decellularized peritoneum, indicating that these two materials had comparable platelet activation capacity.
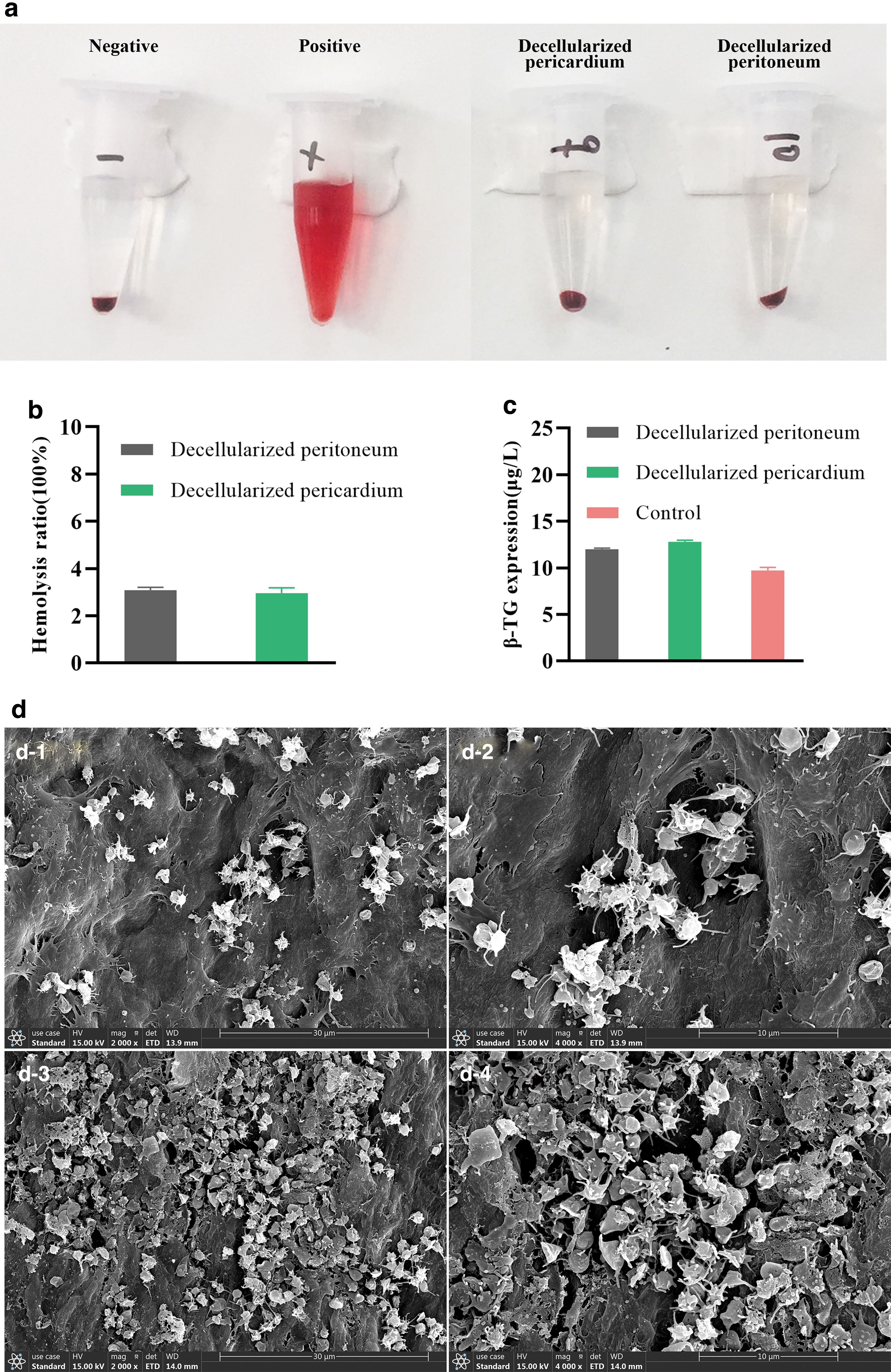
Hemocompatibility of decellularized peritoneum and decellularized pericardium.
Resistance to calcification in vitro and in vivo
Generally, serious calcification processes, which is the enrichment and deposition of insoluble inorganic salts in implanted arteries, may cause the failure of vascular transplantation. Once this occurs, it induces the occurrence of blood clots and inflammatory reaction. 30 Therefore, it is important for vascular substitute materials to have good resistance to calcification. From SEM (Fig. 8a) and Von kossa staining (Fig. 8b) pictures, both the sizes of calcium deposits on the pericardium and peritoneum were increasing with elapse of experiment time (during the 90 days test period), but the shapes of these two calcium deposits are different.
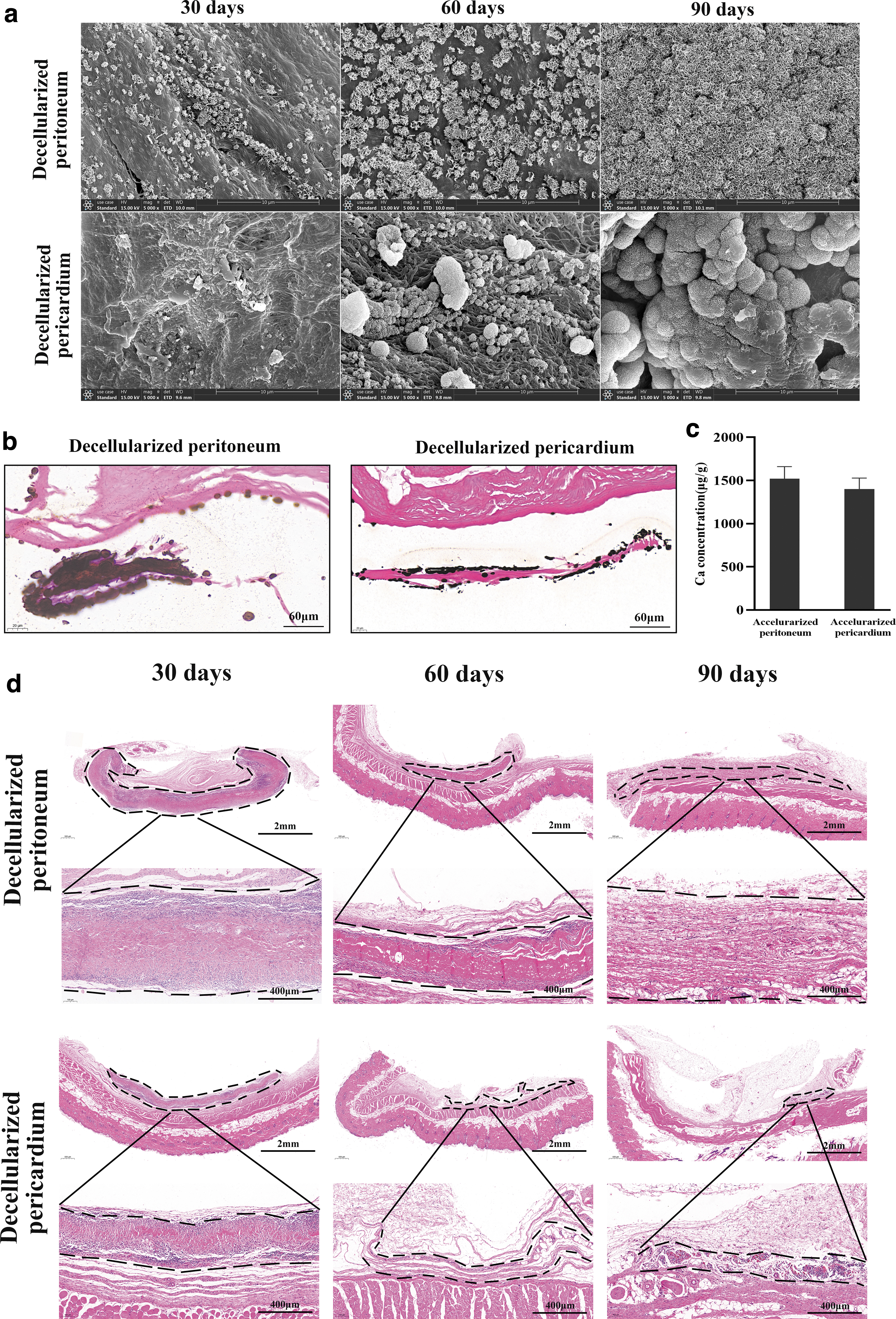
In vitro and in vivo calcification of decellularized peritoneum and decellularized pericardium.
The calcium deposits on the peritoneum were smaller but more evenly distributed. The calcium deposits on the pericardium were larger and more densely distributed. The surface calcium content (Fig. 8c) of the decellularized peritoneum was 1521 ± 139 μg/g, which was slightly higher than that of the decellularized pericardium (1400 ± 128 μg/g). These two samples showed similar calcification in vitro. The numerous blood capillaries and the greater content of elastic fibers in the peritoneum might have contributed to this subtle difference. We also performed subcutaneous implantation of samples in rodents to study the material's resistance to calcification. The subcutaneously implanted samples in the 30th, 60th, and 90th days were harvested and stained with Von kossa staining to observe calcium nodules on the surface of sample. The Von kossa staining results (Fig. 8d) showed that there were no calcium nodules on the surfaces of all samples, indicating the good resistance of samples (peritoneum and pericardium) to calcification in vivo.
In vivo calcification after long-term transplantation of prosthetic valves and prosthetic vessels is a more common phenomenon, which should be avoided. Decellularized ECM can calcify in vivo due to the breakage and inflammation of collagen fibers and elastic fibers. 31 To address this disadvantage, we could fix the decellularized matrices by natural macromolecular cross-linking agent. On the one hand, it could improve the mechanical properties of ECM and reduce the exposure of broken elastic fibers due to some intermolecular cross-links formed between the free amino groups within ECM and the multiple functional groups on macromolecular cross-linking agent,30,32,33 thus leading to protecting ECM from enzymatic degradation, and inhibiting calcification of ECM. On the other hand, filling the fiber gap with macromolecules and reducing the binding sites of fibers to calcium and phosphorus ions is one of the mainstream methods to alleviate calcification of decellularized matrix at present. 33
Cytocompatibility
When the sample is used as a valve or vascular substitute material, mesothelial cells (or vascular endothelial cells) and fibroblasts should grow specifically on the inner and outer sides of the material. In this experiment, L929 and HVEC were inoculated on the surface of the sample. The cell live/dead fluorescent staining assay (Fig. 9) showed that L929 and HVEC well adhered, spread, and grew on the surface of sample during the 2 days culture time, with L929 cells in a spindle shape and HVEC cells in a characteristic irregular prismatic shape. Both cells showed good cell viability on the pericardial and peritoneal surfaces within 5 days culture time. The viability of cells on two samples was significantly >75% at all test time points and exceeded 100% at day 3 of culture. The results indicated that both samples could support the adhesion and spread of L929 and HVEC, even promote their proliferation to some extent.
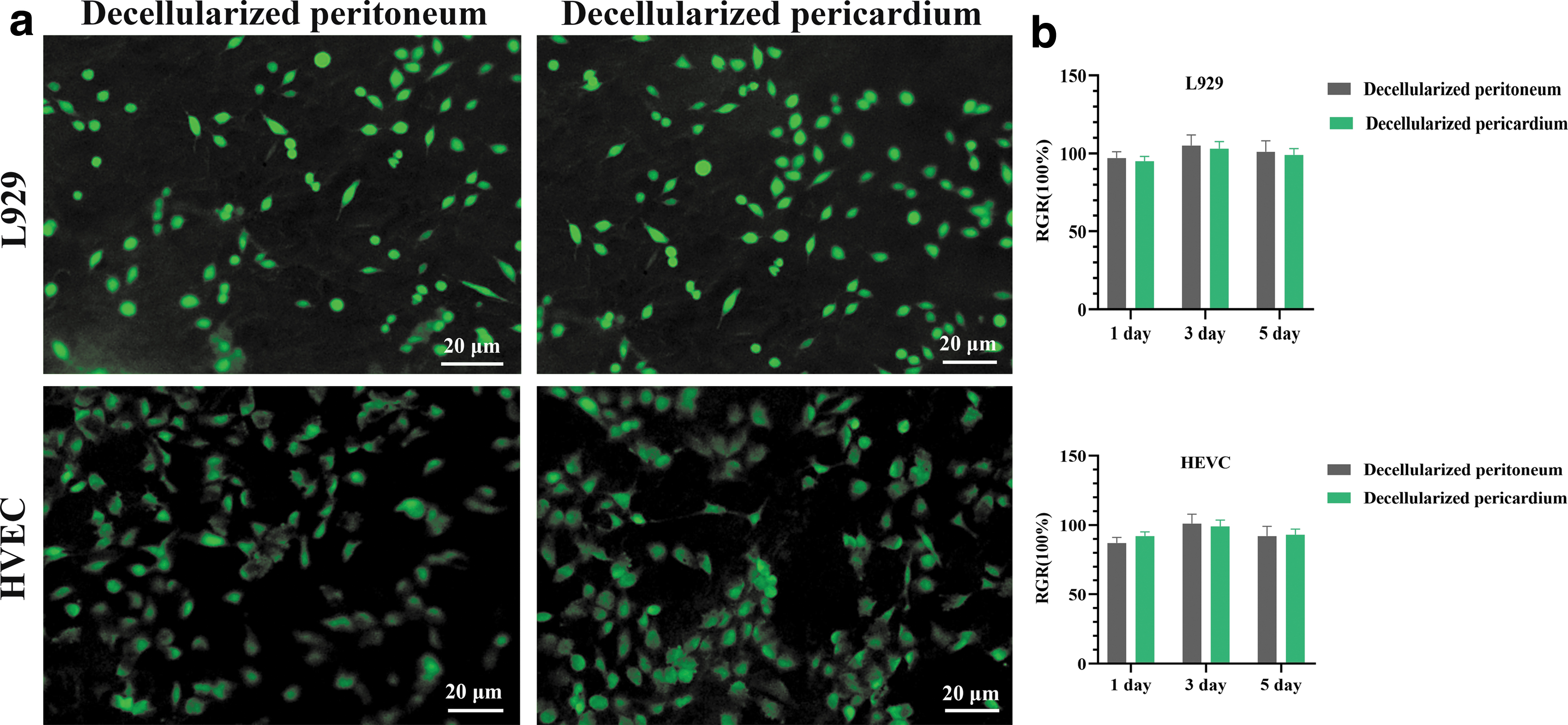
Cytocompatibility of decellularized peritoneum and decellularized pericardium.
Discussion
For the use of artificial vessels, valves and patches for heart and vessel, alternatives are available from porcine, bovine, and equine sources, including (1) artificial vessels origin from umbilical vein, umbilical artery, and ureteral; (2) aortic valves, and mitral valves from porcine pericardium, bovine pericardium, and equine pericardium; and (3) bovine pericardium, equine pericardium, and porcine intestinal submucosal extracellular matrix-derived heart and vascular patches.34,35 Although these materials are not perfect substitutes, and all suffer from various complications, including infection, thrombosis, calcification, and endothelial hyperplasia pseudoaneurysm, these materials are biologically more active than synthetic materials.
In the field of valve replacement and cardiovascular patches, the pericardium is the main substitute material. The bovine pericardium is also commonly used valve material, but the immune response brought by α-Gal is one of the obstacles.36,37 α-Gal knockout porcine have industrially been produced for organ replacement. Therefore, the acute immune response brought by α-Gal is no longer a major consideration. 38 Within a period of time, the porcine pericardium has a greater advantage in overcoming the immune response problem. Although the peritoneum has been studied as an artificial dura, artificial skin, and vascular patch with good results, the physical and chemical structure of the peritoneum have not been well and systematically characterized as an indication of the good results obtained.
In this research, we investigated various properties of the porcine peritoneum in the direction of cardiovascular substitute materials. We used porcine pericardium as a control to compare the differences between them. Both porcine pericardium and porcine peritoneum are collagen-based membrane materials. However, the former has significantly lower elastin-content than the latter, which leads to differences in mechanical properties and in vitro enzymatic degradation properties. Porcine pericardium and porcine peritoneum have similar in vitro resistance to calcification. It has been reported that porcine pericardium has better in vitro resistance to calcification than bovine pericardium, so we could presume that porcine peritoneum also has better in vitro resistance to calcification than bovine pericardium.
The porcine pericardium is thin, about 150–200 μm, with a burst pressure of 412 mmHg. The thickness of porcine peritoneum is about 400–500 μm, with a burst pressure of 1309 mmHg. The burst pressure of the decellularized peritoneum is significantly greater than that of the pericardium and is close to small-diameter natural vessels.38,39 we hypothesize that porcine peritoneum can be used for reconstruction of vein and smaller diameter arteries. In conclusion, we summarized the advantages and disadvantages of the peritoneum and pericardium when they are used as cardiovascular materials, as shown in Table 1. In the future, we can use natural macromolecular cross-linking agent to fix porcine peritoneum, porcine pericardium, and bovine pericardium to obtain better mechanical property samples for their application in vascular grafts.
The Advantages and Disadvantages of the Peritoneum and Pericardium
Footnotes
Authors' Contributions
Experiment, analysis, and writing by X.P. Experiment and editing by C.C. and L.Y. Preparation and staining of pathological tissues by Y.L. Funding acquisition, review, and editing by X.Y. All the authors revised the article and approved it in the present form.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was financially supported by National Key Research and Development Program of China [Nos. 2016YFC1100900, 2016YFC1100901, 2016YFC1100903, and 2016YFC1100904]. The Key Research and Development Program of Sichuan Province (2020YFS0278).