
Abstract
Suboptimal nerve end alignment achieved with conventional nerve repair techniques may contribute to poor clinical outcomes. In this study, we introduce Nerve Tape®, a novel nerve repair device that integrates flexible columns of Nitinol microhooks within a biologic backing to entubulate, align, and secure approximated nerve ends. This study compares the repair strength of Nerve Tape with that of conventional microsuture repairs. Thirty small (2 mm) and 30 large (7 mm) diameter human cadaveric nerves were transected and repaired utilizing Nerve Tape or appropriate microsuture technique. Biomechanical testing was performed using a horizontal tensile tester. The repaired nerves were loaded until failure at a distraction rate of 40 mm/min, and the maximum failure load was determined. In the small nerve groups, the load-to-failure for Nerve Tape repairs (2.33 ± 0.66 N) was significantly higher than for suture repairs (1.22 ± 0.52 N; p < 0.05). In the large nerve groups, no significant difference in load-to-failure was found between Nerve Tape (7.45 ± 2.66 N) and suture repairs (5.82 ± 1.59 N: p = 0.12). Suture repairs tended to fail by rupture, whereas Nerve Tape failures resulted from microhook pullout. Nerve Tape is a novel nerve coaptation device that provides mechanical repair strength equal or greater to clinically relevant microsuture repairs.
Impact statement
Peripheral nerve injuries are common and result in devastating functional outcomes. Despite being the established standard of care, microsurgical suture repair is often inconsistent and functional outcomes are suboptimal, leaving long-term deficits. In this study, we have designed a novel nerve coaptation device, Nerve Tape, to provide a simple sutureless solution. Through biomechanical testing, we show that the holding strength of Nerve Tape repairs is comparable with that of microsuture repairs. This study represents one step in establishing Nerve Tape's ease of use and efficacy in peripheral nerve repair.
Introduction
Peripheral nerve lacerations are common and can result in pain, paresthesia, and focal paralysis. The current standard of care, whenever a direct coaptation can be achieved, is microsuture neurorrhaphy. Despite well-established and accepted principles of suture repair, nerve regeneration is inconsistent and often suboptimal, resulting in persistent, often profound, functional deficits.1–5
Most efforts to enhance clinical recovery after peripheral nerve surgery have focused on physiological obstacles such as poor axonal regeneration. Microsuture neurorrhaphy, the current standard of care for nerve coaptation, requires specialized training and outcomes are often suboptimal. Experimental models have shown that repair quality depends significantly on surgeon experience 6 and 40% of suture-approximated nerve ends were judged technically fair or poor based on gross fascicular malalignment in cadaver nerves.7,8 In addition, regardless of technical expertise, suture material-related foreign-body reactions have been associated with axon-inhibiting intraneural fibrosis.9–15
Not surprisingly, a substantial number of surgeons utilize alternative repair techniques such as fibrin glue or connector-assisted repairs. 16 A fibrin glue-assisted nerve repair involves the simultaneous application of commercially available components of the clotting cascade around approximated nerve stumps. The components mix to form a bloodless clot that can maintain nerve end approximation. Although maintaining precise nerve end alignment when applying the fibrin glue can be challenging, catastrophic repair rupture is the most commonly referenced concern.17–21 Connector-assisted repairs by contrast entubulate and improve nerve coaptation alignment as demonstrated in a cadaveric study. 7 This technique, however, still necessitates microsuture placement and in clinical settings can be technically challenging and time consuming.
Our group has developed a sutureless nerve repair device that combines the efficiency and convenience of fibrin glue with the effectiveness and mechanical integrity of a conduit-assisted nerve repair. Nerve Tape® consists of flexible columns of microscale hooks embedded within a thin flexible biologic backing (Fig. 1). The microhooks are nominally 400–550 μm in height and fabricated from the super elastic alloy Nitinol to prevent metal crimping that could impinge or compress the underlying nerve tissue. The microhooks have been optimized to mechanically engage the outer epineurium without damaging the internal nerve fascicles.
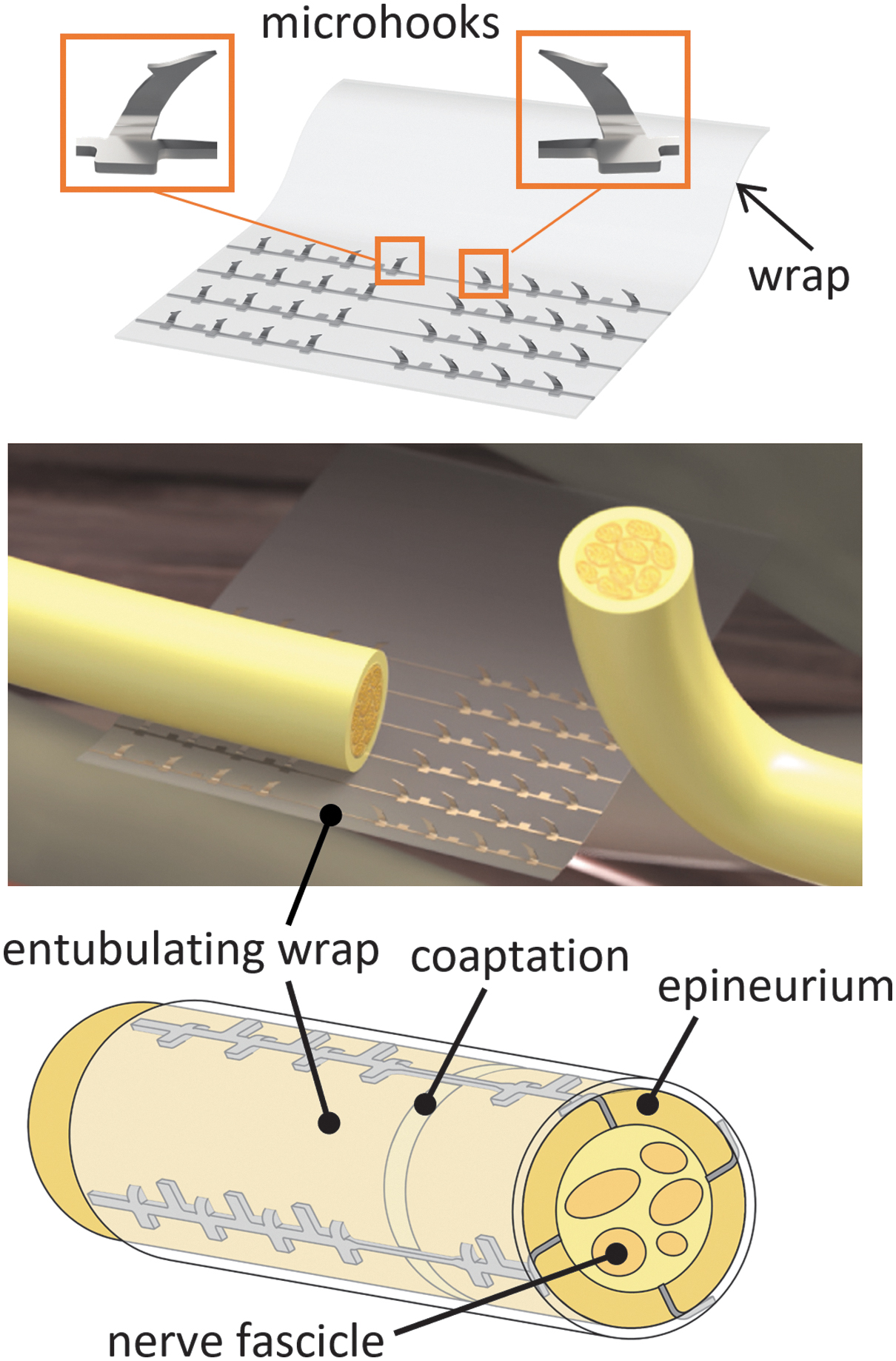
Nerve Tape consists of opposing Nitinol microhooks embedded in a biocompatible SIS backing. Nerve stumps are placed on the microhooks that engage the outer epineurium. The device is then wrapped around the approximated nerve ends to allow additional microhook engagement and to achieve a secure entubulated nerve repair. SIS, small intestinal submucosa.
Each Nitinol column consists of two sides of opposing microhooks arranged to ensure multiple grab points to secure and approximate nerve ends. The columns are sandwiched between thin layers of porcine small intestinal submucosa (SIS) laminated into a robust but flexible backing substrate. An extra leaf of SIS material (without microhooks) allows complete entubulation and self-closure, thanks to the self-adherent nature of the SIS. Various sizes of Nerve Tape have been designed to optimally fit around the circumference of a range of nerve diameters (2–7 mm) by varying the microhook quantity, spacing, and height as well as SIS laminate length and width.
To perform repair with Nerve Tape (Fig. 2), the device is first placed on the tissue bed between nerve stumps with the Nitinol columns parallel to the longitudinal axis of the nerve being repaired. Each nerve stump is placed on the center row of opposing microhook columns in slight overlap, taking care to line up and match fascicular patterns. A slight back tug on each nerve trunk while applying a gentle downward pressure induces microhook engagement, resulting in well-approximated nerve ends. The device is then wrapped around the opposing nerve ends to passively engage the remaining microhooks while entubulating the repair to splint and direct any wayward fascicles into precise secure alignment.
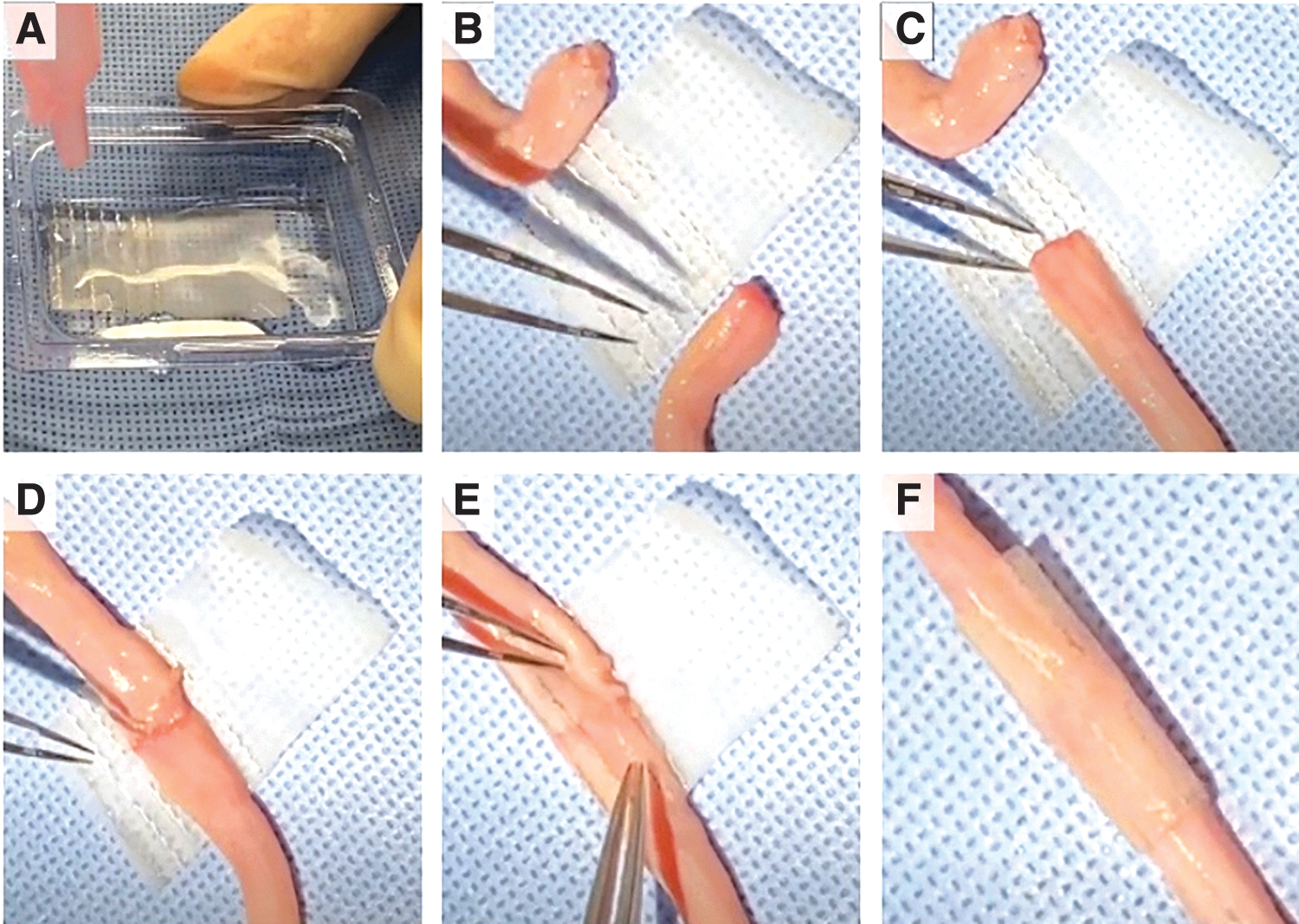
Application of 7 mm Nerve Tape.
For clinical utility, Nerve Tape is designed to be technically easy to apply, maintain stable and well-aligned coaptations, be effective in supporting nerve regeneration, and not cause excessive nerve tissue damage while distributing the tension of the repair along the microhook rows. This biomechanical study focuses on testing the mechanical holding strength across the coaptation in comparison with the clinical gold standard of microsuture repairs. We hypothesized that Nerve Tape would match or exceed the repair strength achieved with microsutures.
Materials and Methods
Microhook column fabrication
Microhook columns were manufactured in three steps: (1) laser micromachining of Nitinol sheet material into 2D patterns, (2) shape-setting the microhooks to 90°, and (3) surface treatment for corrosion resistance. Laser patterning of Nitinol: Individual microhook columns were precision machined from Nitinol sheet stock using a femtosecond laser to remove material with minimal thermal input due to its ultrashort laser pulses.
The cold-ablation process of the femtosecond laser minimizes the risk of inducing heat-affected zones, which may impair the maximum attainable strain and fatigue life. Shape-setting microhook columns: Custom shape-setting fixtures were manually loaded and heat-treated to permanently set the microhooks into their three-dimensional conformation, 90° out of plane. Proper thermal conditioning without negative impact to the austenite finish (Af) transition temperature was confirmed through differential scanning calorimetry. Finished shape-set microhooks were inspected using a vision system for compliance to dimensional specification.
Lamination of microhooks in SIS
Microhook columns were placed in a parallel configuration between multiple layers of SIS. The microhooks were penetrated through the SIS substrate. The layers of SIS were laminated using a vacuum drying process as previously described 22 to permanently trap the Nitinol components within the SIS matrix.
Nerve tape specifications
Two sizes of Nerve Tape were utilized in this study (Fig. 3) to evaluate repairs of both small and large diameter nerves. The “small” devices, designed to fit a nerve of ∼2 mm diameter, contain four parallel columns of microhooks spaced 1.5 mm apart. Each column consists of eight microhooks arranged in opposing groups of four, separated by a 2 mm empty space (the central coaptation zone). The “large” devices, designed to fit a ∼7 mm diameter nerve, contain eight parallel columns of microhooks spaced 2.7 mm apart. Each column consists of 10 microhooks arranged in opposing groups of five, separated by a 4 mm central coaptation zone. By design, the microhooks nominally protrude from the SIS substrate by ∼400 μm and ∼550 μm, respectively, for the small and large devices. The SIS material was produced by Cook Biotech, Inc., and was analogous to commercially available products manufactured by Cook Biotech and sold as Axoguard Nerve Protector®.
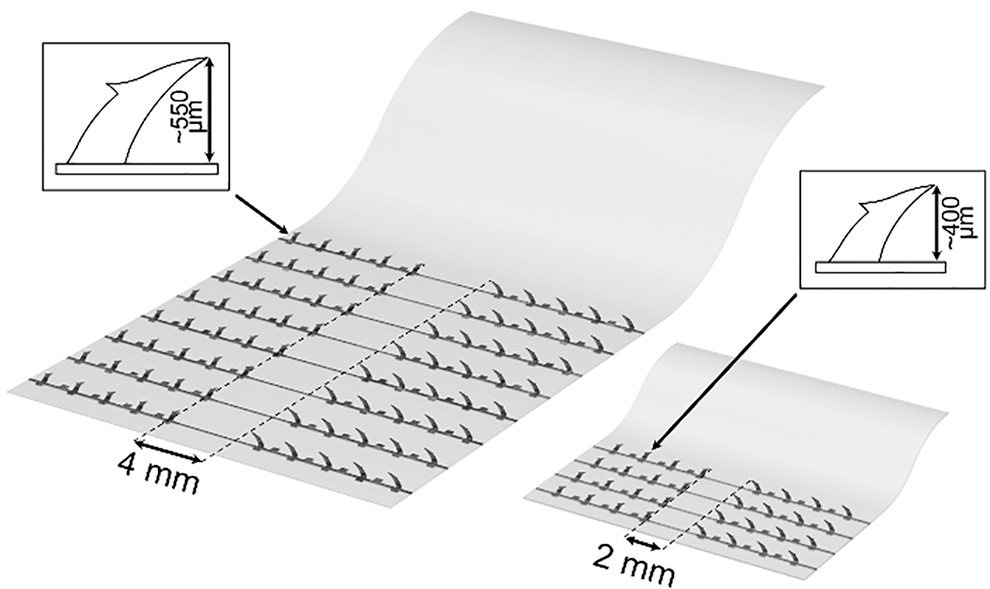
Small (fits 2 mm nerve) and large (fits 7 mm nerve) Nerve Tape devices tested in this study.
Biomechanical study
Sixty fresh-frozen human cadaveric nerves, either 1.5–2 mm (small) or 6.5– 8 mm (large) diameter were purchased from a human tissue processing company (AxoGen, Inc., Alachua, FL). Specimens were tailored to 4.5 cm (for small diameter nerves) or ∼5 cm (for larger diameter nerves) in length for consistency. Before testing, the length and diameter for each specimen was measured using a calibrated caliper (Model 500-195-30; Mitutoyo, Kanagawa, Japan). Under a surgical microscope (Leica M850, Wetzlar, Germany), the nerves were transected at the midpoint using a fresh scalpel and immediately repaired with either sutures or appropriately sized Nerve Tape device as indicated by a preprocedure randomization table.
For the small nerve suture repair, four 9–0 nylon monofilament sutures (AROSuture; AROSurgical Instruments Corporation, Newport Beach, CA) were placed through the epineurium evenly spaced around the circumference of the nerve. For the large nerve suture repair, similar epineurial repairs were done using eight stitches of 8–0 nylon monofilament sutures (AROSuture), with the goal of technically achieving a clinically proper well-aligned repair. Nerve Tape repairs were achieved using 2 and 7 mm Nerve Tape devices as described earlier (Fig. 2). Frequent irrigation with saline improved SIS flexibility and facilitated wrapping.
Immediately after repair, the coapted nerves were positioned for biomechanical testing onto a custom horizontal tensile tester stage consisting of metal clamps (G1062; Mark-10 Corp., Copiague, NY), a force gauge (Model M5–5, 25 N full scale, ±0.025 N accuracy; Mark-10 Corp.), and a motorized actuator (Series 613; Mark-10 Corp.) (Fig. 4). Approximately 5 mm of the free nerve ends were secured within the clamps. The actuator speed was set so that the two clamps would separate at an extension rate of 40 mm/min. Axial forces were measured by the force transducer at 7000 Hz. Repair failure was defined as total loss of repair tension. The nerve specimens were moistened with saline irrigation throughout testing. Maximum force to failure values were compared using unpaired Student's t-test, with a value of p < 0.05 considered to be statistically significant.
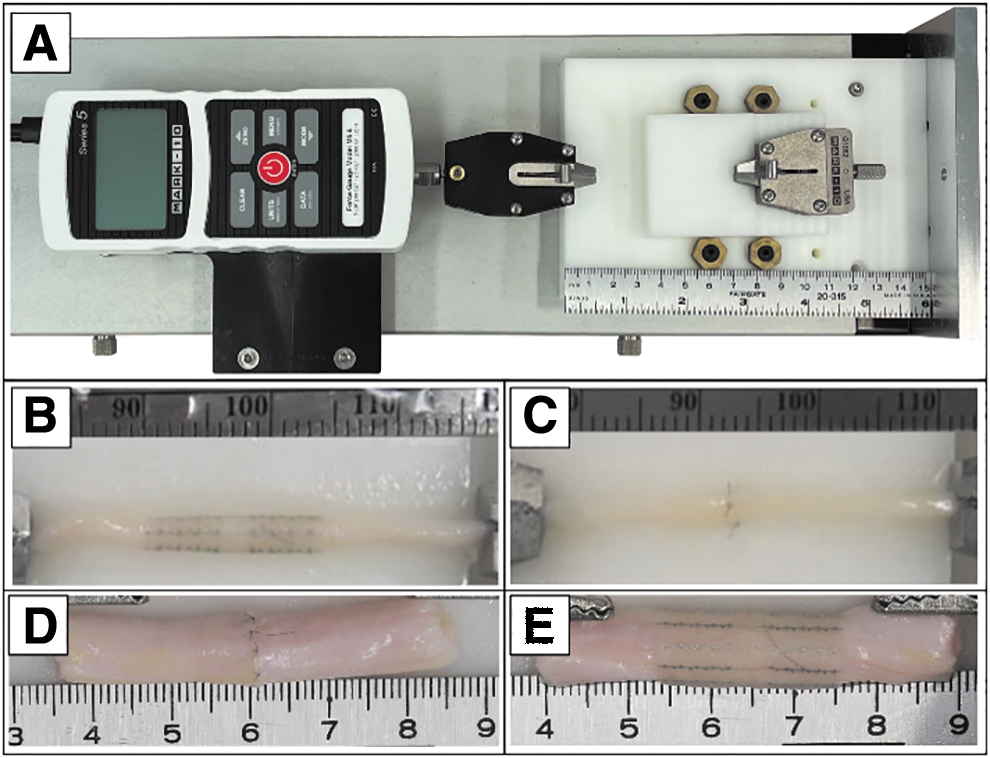
Testing.
Results
Small cadaveric nerves were measured to be 1.8 ± 0.2 (Nerve Tape group) and 1.9 ± 0.3 mm in diameter (suture repair group). The larger nerves were 7.0 ± 0.9 and 6.5 ± 0.9 mm in diameter for the Nerve Tape and suture group, respectively.
For smaller nerves, a significantly higher maximum load to failure was recorded for Nerve Tape (2.33 ± 0.66 N) compared with suture repairs (1.22 ± 0.52 N; p < 0.05) (Fig. 5). For larger nerves, the average Nerve Tape repair strength (7.45 ± 2.66 N) was higher but not statistically different from suture repairs (5.82 ± 1.59 N; p = 0.12) (Fig. 5). Post-testing inspection suggested that suture repairs failed by rupture, whereas in Nerve Tape, repairs failed by microhooks pulling free from the epineurium. For both repair techniques, there was no visible damage to any internal fascicles.

Maximum tensile strength of Nerve Tape versus microsuture repair.
Discussion
Recognizing deficiencies in contemporary nerve repair strategies, Nerve Tape was envisioned and developed to improve nerve repair efficiency, consistency (especially across variable surgical skill sets), and efficacy. Although microsuture neurorrhaphy is considered the gold standard, many surgeons are dissatisfied with this technique, which is time consuming (resource expensive) and requires a high degree of surgical skill. 16 Although fibrin glue can avoid some of the technical challenges associated with microsuture repair, catastrophic failure remains a concern, and the application of fibrin glue does not improve fascicular alignment.
Although Whitlock et al. concluded that novice and expert microsurgeons achieved similar results after rodent nerve repairs performed with fibrin glue, the described technique in their article interposed an additional 5 mm nerve graft, even though the injury consisted of an acute sharp laceration (which would typically be repaired directly without a graft). 6 A likely explanation for this deviation from standard treatment is that even physiological tension present in an end-to-end repair must have impeded fibrin glue-based coaptation, at least when performed by a less experienced surgeon. Multiple other small animal studies have reported one or more repair failures in their fibrin glue groups.17–21
Entubulation of the repair with either a preformed tube slid across the coaptation or a biocompatible sheet wrapped around the coaptation have been described to improve regeneration. 23 Although most animal and clinical studies fail to demonstrate improved functional recovery, reduced pain at the repair site is a consistent finding often attributed to reduced axonal escape. 24 The entubulating sheet does seem to splint and direct wayward fascicles and increase the chances of a “technically good” or “excellent” repair, as demonstrated in a cadaver study performed by the senior author. 7 However, conventional wraps and conduits both still require microsuture technique along with its drawbacks. By incorporating shallow penetrating microhooks for mechanical fixation, Nerve Tape can uniquely offer the benefits of entubulation without requiring use of microsutures.
Many materials were considered for both the microhook fabrication and the substrate. SIS was chosen for its flexibility, resilience, and pro-regenerative properties. SIS is approved by the US Food and Drug Administration (FDA) for a spectrum of clinical applications including nerve surgery, and previous studies demonstrate revascularization and remodeling of SIS material wrapped around rabbit sciatic nerves. A mild inflammatory response dissipated with SIS incorporation into the mesoneurial layer and did not affect nerve function. 25
Nitinol is an alloy of nickel and titanium widely used in medical devices because of its biocompatibility and unique mechanical properties.26,27 Nitinol behaves “super elastically,” does not easily crimp, and returns to its original shape even after application of strains up to 10%. 26 The composite SIS-Nitinol construct exhibits excellent mechanical and handling properties. The Nitinol columns provide axial strength across the repair site, but each column is isolated to “float” within the SIS, allowing for easy wrapping and contouring of the device to the nerve surface.
Microhook height was determined through a series of handling experiments to achieve stable and secure tissue hold while minimizing tissue damage. The microhooks are intended to penetrate the outer epineurium and intraneural connective tissue (inner epineurium) without penetrating through the perineurium into the fascicles and vital axons. Thickness of this connective tissue varies across different nerves, within the same nerve, and between individuals. Several investigators have demonstrated that connective tissue comprises 30–75% of the total nerve cross-sectional area.28–30
High-resolution sonography of normal ulnar nerves revealed an average epineurial thickness of 0.49 mm. 31 Microhook lengths have been adjusted based on nerve size. The bending design of the microhooks protruding from the substrate limits the actual penetration depth. In addition, the perineurium around fascicles is quite tough32,33 and the loose inner epineurium allows fascicles to shift away from the microneedles. Fascicular glide between the perineurium (lining of the fascicles) and the inner epineurium is independent of the glide between the Nerve Tape and the outer epineurial surface, 34 further reducing the likelihood of inadvertent penetration into fascicles.
The optimal nerve repair strength is not known, but several authors have opined that if more than one or two microsutures are necessary to maintain coaptation, then there is too much tension and nerve regeneration could be compromised.35,36 Some tension relief and enhanced distribution of tension due to the multiple microhook grab points inherent to Nerve Tape would be expected and may offer some theoretical advantage for nerve regeneration based on small animal data. 11 Others have questioned the utility of such a strict tension phobia.37–39 Regardless, comparable holding strength to conventional microsuture repairs seemed like an appropriate design target. This biomechanical study indicates that this goal was achieved, and that Nerve Tape can provide adequate holding strength for clinical translation.
Repair strength can be measured in vivo using small animal models or ex vivo using animal nerves or human cadaver nerves. Nerve specimens were obtained from a human tissue processing facility to improve consistency in sizing and quality, although, as with any biological tissue, some variability persisted as evidenced by the small deviations from the mean diameters. Our goal was to compare Nerve Tape with clinically relevant microsuture repairs. Suture repairs using four 9–0 sutures in a 1.5–2 mm diameter nerve and eight 8–0 sutures in a 6.5–8 mm diameter nerve were deemed appropriate, based on widely accepted clinical principle, and as judged by the senior author, an experienced clinical peripheral nerve surgeon.
Although there are obviously many nerve sizes that were not assessed, testing at the relative ends of the spectrum of commonly treated nerve sizes would offer meaningful and clinically relevant data. The current Nerve Tape sizes in development would not be applicable to submillimeter nerve repairs or extremely large nerve trunks such as the sciatic nerve. In addition, although 40 mm/min is a relatively standard extension rate for this type of comparative biomechanical testing, faster or slower rates could affect either the modes of failure or the absolute failure strengths. In a clinical scenario, although higher tensile forces could conceivably create an unintended gap between the nerve stumps, the repair would still remain entubulated and protected. Multiple clinical studies have shown that even for large diameter nerves, small gaps between entubulated nerve stumps does not compromise functional recovery.40,41
Conclusion
In conclusion, the mechanical holding strength achieved with our novel Nerve Tape coaptation device was at least equivalent to clinically relevant conventional microsuture repairs for small (1.5–2 mm) and large (6.5–8 mm) diameter nerves. Although this study did not assess the clinical efficacy or safety of Nerve Tape, ongoing in vivo studies will provide further data regarding future clinical application of Nerve Tape.
Authors' Contributions
G.S.B., M.S., I.P.C., and J.E.I. designed and performed experiments. G.S.B. and M.S. analyzed data. G.S.B. wrote the original draft and M.S., I.P.C. and J.E.I. edited the article. I.P.C. and J.E.I. wrote the grant that supported this study.
Footnotes
Data Availability
Part of the data included in this article can be shared upon request.
Disclosure Statement
Geetanjali S. Bendale reports no conflict of interest. Maximillian Sonntag and Isaac P. Clements report financial support was provided by BioCircuit Technologies. Jonathan E. Isaacs and Isaac P. Clements have patent “Devices and methods for repairing damage to a tissue” pending to Virginia Commonwealth University and BioCircuit Technologies, Inc. Jonathan Isaacs and VCU have a royalty agreement with BioCircuit Technologies.
Funding Information
This study was supported by an NIH 7R44NS097113-05 grant.