
Abstract
The characterization of diffusion through biological tissues has played an important role in fundamental medical research and product development. Understanding the diffusion phenomena allows for the identification of new concepts in fundamental science, evolving medical knowledge and improving future standards and protocols. To illustrate, the structure of cortical bone changes upon the onset of osteoporosis, altering the limited porous compartment through which nutrients and essential signaling molecules travel to bone cells. Estrogen hormone replacement therapy (HRT) is one of the gold standard treatments to attempt to mitigate the effects that this structural change exerts in menopausal osteoporosis patients; however, HRT effectiveness is often variable in these patients, likely due to variability in bone structure and physiology, and thus transport rates. Scientists have studied diffusion in cortical bone tissue for decades. Current methodological standards include fluorescence recovery after photobleaching and computed tomography finite element analysis. Both techniques limit areas of tissue to microscale (1–100 μm2) analysis—only examining a few osteocytes within the structure at a time—and adopt assumptions that oversimplify in vivo tissue structure and transport phenomena. Also, the range of diffusion tracers is limited by the sensitivities of the analytical equipment, typically requiring tracer concentrations in the micromolar range.
Herein is described a novel device for directly assessing the diffusion coefficient of 3H-estradiol at 37°C in macroscale osteonal bone specimens (1.4 cm2)—assessing a much larger portion of the total tissue than previously reported—while using radioisotope tracers for much higher sensitivity, thus achieving physiologically relevant estradiol concentrations. The current diffusion chamber device represents a cost-effective and validated method to mitigate these shortcomings. The device provides long-term diffusion data through macroscale (greater than 1 mm2) tissue areas, presenting a more physiologically accurate way to assess cortical bone diffusion. The device can assess solute diffusion through other tissues or materials and may easily be scaled up to run multiple diffusion experiments simultaneously.
Impact statement
The diffusion chamber device represents a cost-effective and validated method to assess solute diffusion through solid materials. Specifically, it demonstrates that this novel device provides long-term diffusion data through macroscale tissue samples at nanomolar concentrations, presenting a precise way to address the effects of tissue structures on diffusion. This device can be applied to other tissues or engineered materials, offering a methodology that is easily scaled up to allow simultaneous assessment of multiple material samples.
Introduction
Understanding the transport rates of small molecules critical to bone maintenance is important for the design and dosing of these pharmaceutical agents and for understanding possibly variable outcomes in animal and clinical studies. Osteocytes, the cells responsible for maintaining bone homeostasis through regulation of osteoblasts and osteoclasts, 1 are embedded into cavities called lacunae that are interconnected through channels called canaliculi.1,2 Based on this interconnectivity, the lacunar-canalicular system (LCS) is defined as the major communication network and tortuous transport pathway between neighboring osteocytes. Cylindrically arranged cortical bone tissue layers containing embedded osteocytes comprise an osteon.
At the center of each osteon is a small blood vessel surrounded by supporting extracellular matrix. When osteons are oriented parallel with the long axis of a bone, their central channel with blood vessel is referred to as Haversian canals, while the central blood vessel within osteons oriented perpendicular to the long axis is referred to as Volkmann's canals. 3 Altogether, the Haversian–Volkmann's-LCS (HVLCS) comprises the porous compartment of osteonal bone.1,2
Interstitial fluids containing important biomolecules have been shown to transport through the HVLCS by convective pressures from blood perfusion and locomotion-associated cyclic bending.2,4–6 Solute transport through the HVLCS occurs along the long axis of the bone and radially from the endosteum and periosteum. Due to the low radial porosity and connectivity of osteonal bone, convective pressures primarily facilitate axial solute transport and their effects diminish at positions that are radially distant from the central canal of an osteon.7,8 This indicates that diffusion may be the primary transport mechanism in more radially distant areas from the central canal within an osteon, especially in patients with limited mobility. For this reason, radial solute diffusion in osteonal bone defines the focus of this study.
Estradiol is the clinically approved estrogen for hormone replacement therapy (HRT) and perimenopausal patients undergoing HRT treatment can exhibit varying degrees of effectiveness at mitigating bone loss in patients throughout various stages of menopause.7,9 In healthy bone tissue, in vivo serum concentrations of estradiol range between 300 and 800 pM. 10 Estrogen ERα and ERβ receptor signaling mediates osteocyte-dependent regulation of bone forming (e.g., osteoblasts) and bone resorbing (e.g., osteoclasts) surface cells.1,11–13 Since osteoclasts can resorb cortical bone at a much faster rate than osteoblasts can form it, disruption of osteocyte estrogen signaling in perimenopause manifests as progressive bone loss, disrupting structural homeostasis.1,14,15
Transport of estradiol throughout osteonal bone tissue is dependent on the microstructure and macrostructure of the HVLCS; however, the rate and mechanisms of estradiol transport within osteonal bone have not been reported to date. Our interest is to directly measure the radial diffusion coefficient of estradiol at 37°C across a section of canine osteonal bone, at dimensions of several hundred microns, between osteons connected through a porous HVLCS microstructure.
Sodium fluorescein (NaFluor) and coumestrol were tested initially as the solutes of interest due to their fluorescent detectability and similar molecular size to estradiol. The transport of NaFluor in bone tissue has been investigated previously.4,16–18 Coumestrol is a phytoestrogen with fluorescent properties that binds to human estrogen receptors, 19 which is another reason it was selected.
However, fluorophore tracers only allow for evaluation of one tracer per experimental solution, as the emission and excitation spectrums of the two tested molecules coincide, not allowing for simultaneous detectability. 3 H-estradiol was then chosen for detailed investigation, based on its clinical relevance described above, and because the use of radioisotopes allows highly sensitive detection at the low concentrations present in vivo. 14 C-sucrose was chosen as a control molecule because it is of similar size to estradiol, but is polar, its diffusivity in aqueous solutions has been well characterized, and differences between the photon energies emitted by decay of the two radioisotopes are separable, allowing for both molecules to be simultaneously evaluated in a dual-label radioisotope solution.
Several techniques have been used to evaluate solute transport in cortical bone: fluorescence recovery after photobleaching (FRAP), computed tomography image-based three-dimensional (3D) modeling, a tracer immersion method, and prior diffusion chamber experiments. FRAP focuses on transport within a single lacuna utilizing two-photon confocal microscopy,4,5,18,20 and is not appropriate for assessing diffusion rates at macroscale dimensions (greater that 1 mm2). 3D tomography-based finite element modeling has been used for macroscale assessment of solute diffusion in cortical bone through the creation of 3D models based on microscopy images, which undergo computer simulations to estimate solute diffusion rates.17,21–25
These models rely on simplifications, such as disregarding extracellular matrix and cellular components in the canaliculi, or interpreting bone as a homogenous material. The tracer immersion method was developed for testing larger bone specimens 16 ; however, the requirement for fluorescent tracers limits the usefulness of this method. The techniques described above utilize fluorophore concentrations that are orders of magnitude larger than estradiol concentrations in vivo, and many use bone specimens lack osteons (e.g., rodents), a key structural trait for solute diffusion in human bone, 26 diminishing clinical relevance.
Our laboratory has reported results using a classical diffusion system where the donor and receiver chambers are constructed of glass, surrounding a bone specimen held within micron filter holders modified to fit into each chamber. 16 This device had a large footprint due to the requirement for temperature control using a cumbersome external water bath, which rendered it difficult to scale up the number of bone diffusion trials that can be simultaneously conducted. In addition, silicone grease was necessary for sealing the system, which potentially provides a transport route for nonpolar solutes and could lead to flawed experimental results.
The limitations of the previous systems created the need for a small device whose materials do not adsorb polar and nonpolar solutes and can be reliably operated over a 14-day experimental timeframe. The size of the device needed to be minimized and its components simplified for cost effectiveness, and improved manufacturability and scalability. The device must also be able to employ a reproducible method for fixing bone specimens in place during operation. For clinical relevance, sub-nanomolar concentrations must be detectable. Solution volumes must be minimized to reduce the use of radioactive tracers and to ensure measurable concentration changes in both chambers. The diffusion system presented herein satisfies all these design constraints, constituting a simplified design through readily available components and 3D printed parts.
Materials and Method
Bone specimen fabrication
Radial bone samples were prepared from the diaphysis of the tibia from 2- to 5-year-old dogs that were sourced from the Cleveland Clinic as remains from unrelated experiments. The dog legs were preserved in a −20°C freezer until removed for dissection. After removing soft tissues and the epiphysis and metaphysis portions (Fig. 1a), the diaphysis was sectioned into 1.2-cm rings along its long axis before cutting each of the rings into three flat planes (Fig. 1b–d), each of ∼2.0 mm thickness, utilizing a saline-lubricated bone band saw (Mar-Med Inc., Cleveland, OH). The bone planes were placed into custom silicone cylinder molds (2.54 cm in diameter) periosteal face down, before filling the molds with red polymethylmethacrylate (PMMA) dental resin (DentsPly Sirona, Charlotte, NC) and curing for 24 h (Fig. 1e).

Radial canine bone sample processing for diffusion experiments. Once isolated, the diaphysis of the long bone
The periosteal surface of the bone was shaved off (Fig. 1f) due to its impermeable nature 16 by removing the top 100 μm of tissue using a Leica SP1600 diamond blade microtome (Leica, Wetzlar, Germany). From here, two to three 400 μm thick bone specimens were cut from each embedded bone section using the microtome (Fig. 1g). Each bone specimen was carefully removed from surrounding PMMA to prevent nonpolar molecular adsorption, and the sample was stored at 4°C in 3 mL of potassium-free phosphate-buffered saline (PBS) solution (7.2 pH; all dry salts from Sigma Aldrich, Burlington, MA) containing 0.05% (w/v) sodium azide (Sigma Aldrich) as a preservative.
Diffusion system design and assembly
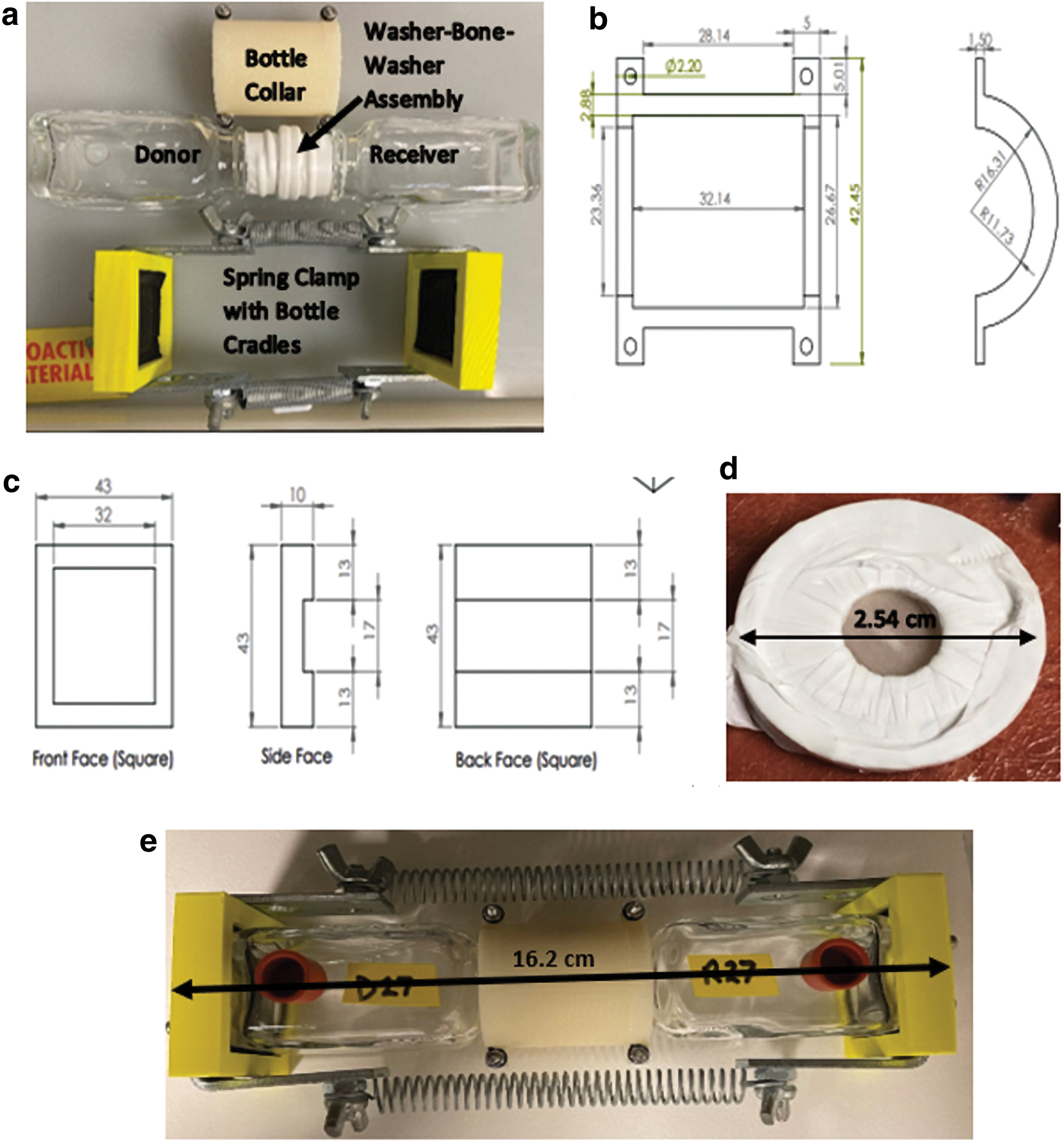
Diffusion chamber system parts and general assembly layout are shown in Figure 2a and the component list in Table 1. All parts listed—except the 3D printed parts and polytetrafluoroethylene (PTFE) washers—were sourced from local hardware stores. PTFE washers were wrapped with PTFE tape through their center around their entire circumference before sandwiching a bone specimen between them (Fig. 2d). Wrapping with PTFE tape provides an elastic surface to improve the seal at the interface of the solid PTFE washer and glass bottle neck, preventing leaking. The washer-bone-washer assembly was then wrapped tightly with PTFE tape around the circumference to seal the gap between the two washers. The chamber bottle necks were also wrapped with PTFE tape to ensure a firm seal (Fig. 2a).
Major components of the diffusion system.
Component List For a Complete Diffusion System
There are a total of 41 components, summing to a total fabrication cost of about $65 for each chamber. Bolded parts are utilized to build the chamber spring clamp, which provides the sealing compression required to establish a closed diffusion system.
The washer-bone-washer assembly was positioned between the donor and chamber bottles and aligned in place with the two bottle neck collar pieces (Fig. 2b), which were fastened together with M2 nuts and bolts with the periosteal-facing bone surface oriented toward the receiver chamber bottle. After ensuring chamber bottle alignment, padded bottle cradles (Fig. 2c)—with attached spring clamps—were attached to the bottom of each chamber bottle, providing the compression to seal the complete system (Fig. 2e).
Experimental solutions and concentration analysis
For material adsorption and leak testing, the 90 nM coumestrol solution in PBS was prepared by serial dilutions of a 90 μM stock in absolute ethanol. The 90 nM NaFluor solution in PBS was prepared by serial dilutions of a 90 μM NaFluor stock in distilled water. Fluorophore concentrations in experimental samples were measured using a spectrofluorometer (BioTek Synergy H1) by means of standard concentration curves. Excitation and emission wavelengths for coumestrol (λex = 355 nm, λem = 420 nm) and NaFluor (λex = 488 nm, λem = 525 nm) were provided from the vendor labels of both dry reagents (Sigma Aldrich).
Dual-label donor solutions were prepared in 133 mL batches, providing enough for four 33 mL donor chambers. Approximately 8.5 μL of 3 H-estradiol in ethanol 11.4 μM stock (Perkin Elmer, Waltham, MA) and 4.5 μL of 14 C-sucrose (polar control) in water 229 μM stock (Perkin Elmer) were added to 133 mL of PBS using separate 10 μL gas-tight Hamilton syringes and mixed to yield a donor solution containing ∼0.73 nM 3 H-estradiol and 7.74 nM 14 C-sucrose. Stock concentrations were calculated from the specific activities provided from the vendor, given as 88 Ci/mmol for 3 H-estradiol and 435 mCi/mmol for 14 C-sucrose.
To account for the half-life of 3 H (12.2 y), estradiol stock volumes used to fabricate donor solutions were adjusted biannually. This adjustment was not necessary for 14 C due to its extremely long half-life (5,730 y). Due their specific activities, the donor solution concentration of sucrose was roughly 10-fold greater compared with estradiol to ensure adequate sucrose detectability in the solution throughout the experiment.
Radioisotope concentrations were measured daily in both chambers to construct their concentration curves over the experimental timeframe in an LS6500 liquid scintillation counter (Beckman Coulter, Brea, CA), which reports the counts per minute (CPM) in three energy windows from each sample vial. 3 H and 14 C emit beta particles of different energy spectra, 27 allowing their CPM to be separated from the total reported CPM using the CPM values in the three counting windows. Some 14 C beta electrons emitted overlap into the 3 H spectrum, which are separated from the 3 H counts by a measured spillover correction factor calculated with standards (1.54 here).
CPM was converted to disintegrations per minute (DPM) by dividing CPM by the measured counting efficiencies of each radioisotope (0.5 for 3 H and 0.99 for 14 C). 27 DPM were converted to mols by converting DPM to μCi (2.22 × 106 DPM/μCi) and then dividing by the provided specific activities. Concentrations were then calculated by dividing the mols of each radioisotope by the aliquot volume.
Material adsorption testing
Various materials for fabricating the diffusion chamber system were tested for solute adsorption to ensure quantitative recovery. Coatings of epoxy, silicone, and polyurethane were applied to 3D printed disks (1ʺ diameter, 0.5 mm thickness) constructed from a proprietary plastic called RGD720 (Stratasys, Eden Prairie, MN). Two disks from each coating group were placed into separate 50 mL Pyrex glass beakers containing 10 mL of 90 nM coumestrol in PBS. Three 200 μL aliquots were taken from each beaker at t = 0 and analyzed in a Synergy H1 spectrofluorometer (BioTek, Winooski, VT) in 96-well plates before sealing the beakers with TiterTops (Diversified Biotech Inc., Boston, MA) and placing them on stir plates under medium convection at room temperature. Triplicate aliquots were taken every 24 hours thereafter up to 96 hours, which were assayed immediately after collection.
Adsorption experiments were also conducted using empty 35 mL glass chamber bottles (Wheaton, Staffordshire, United Kingdom) and custom polytetrafluoroethylene (PTFE) washers (Fluoroplastics Inc., Philadelphia, PA) in the chamber glass bottles, with coumestrol solution (90 nM), NaFluor solution (90 nM), and dual-label solutions containing both 0.76 nM 3 H-estradiol and 7.65 nM 14 C-sucrose in PBS. Two 50 μL aliquots were taken at t = 0 from each sample, and every 24 h thereafter until 96 h. Recovery was calculated from the sum of the number of moles of solute measured in each aliquot and from the final solution concentration at 96 h, relative to the number of moles of solute present in the initial solution.
Coumestrol, NaFluor, 3 H-estradiol, and 14 C-sucrose were assessed for adsorption into the proprietary plastic, various coating materials, glass, and PTFE as described in the previous paragraph. All coating materials (epoxy, silicone, and polyethylene), and the 3D printed proprietary plastic itself, showed substantial adsorption of coumestrol (Fig. 3a) and were eliminated from consideration. Adsorption of all compounds on glass and PTFE was minimal (Fig. 3b).

Recovery of fluorescent and radioisotope tracers after 96 h of exposure to various materials.
Diffusion system leak testing
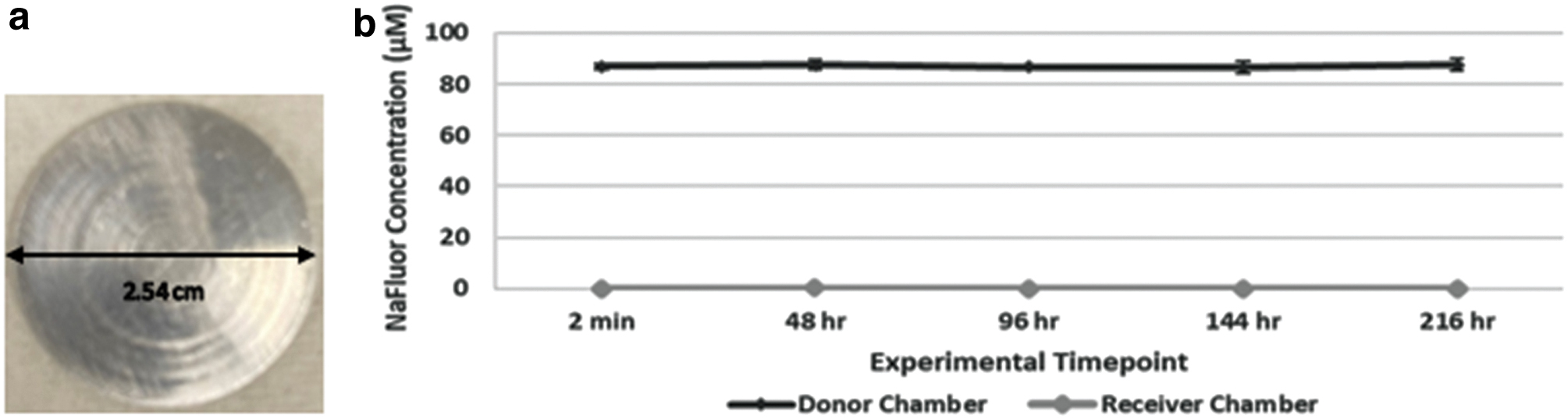
Internal leaking between donor and receiver chambers of the diffusion system was assessed using a solid aluminum disk of 400 μm thickness in place of the bone sample. The donor chamber was filled with 32 mL of 90 μM NaFluor in PBS solution and the receiver chamber with 32 mL of PBS. Three 200 μL aliquots were removed from both donor and receiver chambers every 24 h for 9 days, and NaFluor concentrations were measured using a spectrofluorometer. External leaking of chamber solutions out of the device was evaluated by measuring the liquid volume recovered from both chambers at the end of the experiment, including the sum of all aliquot volumes. The spring constant was assessed by hanging a 250 g weight from the springs on a bimonthly basis and recording the resulting deformation. These results showed no change in the spring constant value, ensuring consistent sealing.
Leak testing with the aluminum test disk (Fig. 4a) showed that NaFluor concentration remained constant in the donor chamber and nondetectible in the receiver chamber over nine days (Fig. 4b), indicating little to no internal leaking or material adsorption. No evidence of NaFluor outside of the system and 100% recovery of the initial liquid volume from each chamber were observed, confirming absence of external leaking. These outcomes were likely the result of the high compression force (338 N) of the springs and the wrapping of the bottle necks and washers with PTFE tape, which compensated for the inelastic nature of the glass and PTFE washer.
NaFluor concentration profiles using aluminum test disk in place of bone samples. To perform the leak test, a solid aluminum disk
Calculation of solute partition coefficients
Measurement of the partition coefficients (
Three bone samples were used for each dual-label solute concentration, with
3
H-estradiol and
14
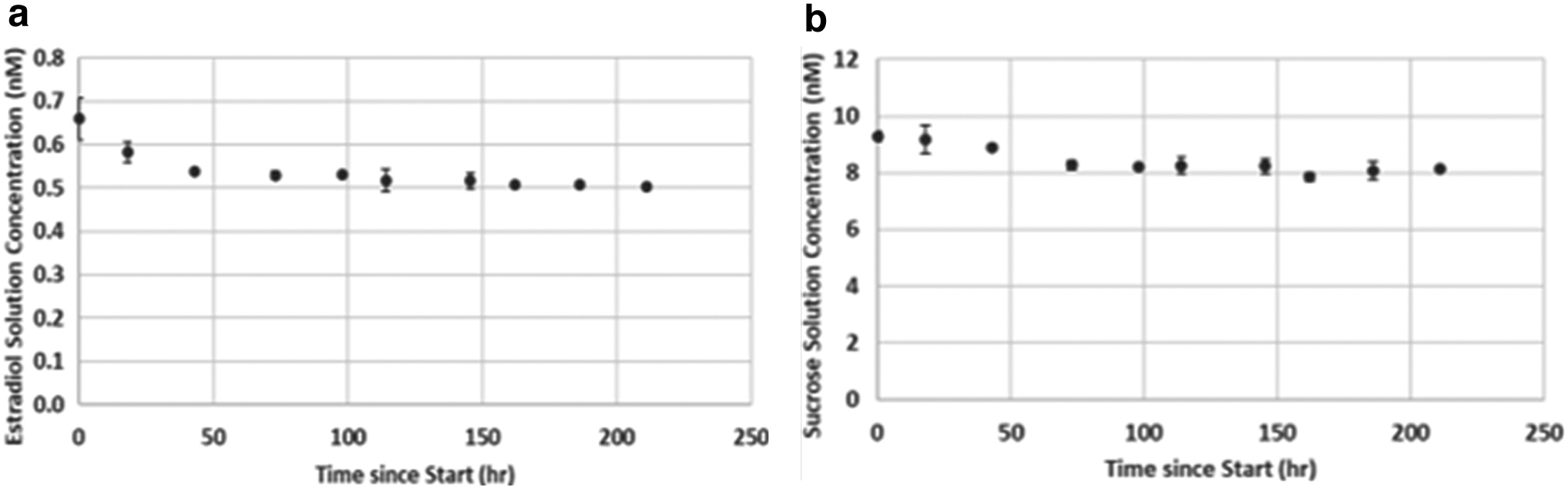
C-sucrose being simultaneously assessed in each solution. Duplicate 50 μL aliquots were taken daily for 9 days, with the average of the concentrations from days 7 to 9 taken as the solution equilibrium concentration, Seq. Equilibrium was confirmed when the three final concentrations were within 5% of their mean for both solutes. The bone equilibrium concentration, Beq, was calculated from
The partition coefficient (φ) was then calculated from
28
Analysis of variance (ANOVA) comparisons were done between the partition coefficients of all tested starting concentrations within both experimental solutes to determine dependence on starting concentration for estradiol and sucrose (e.g., 0.5 × estradiol vs. 1 × estradiol, etc.). Similarly, ANOVA tests were done between the partition coefficients of sucrose and estradiol at the same concentration multiplier group to determine dependence on the solute type at given multiplier concentrations (e.g., 1 × estradiol vs. 1 × sucrose, etc.). Partition coefficients from the two lowest concentrations were then used to calculate the mean values utilized in the diffusion system governing equation, and data were analyzed using paired t-tests.
Concentration profiles from the partition coefficient experiments reach equilibrium within 7 days (Fig. 5), which is confirmed with the concentrations from days 8 and 9. Estradiol and sucrose partition coefficients are shown for the entire range of solute concentrations, 0.5 × –400 × the donor chamber concentrations (Fig. 6). The partition coefficients of estradiol versus sucrose at a given concentration multiplier (e.g., 0.5 × sucrose vs. 0.5 × estradiol) group are significantly different (Fig. 6, p < 0.001; ANOVA); however, values within a given radioisotope group (e.g., 0.5 × sucrose vs. 1.0 × sucrose) are independent of starting concentration (Fig. 6, p > 0.05; ANOVA).
Concentration profiles of partition coefficient solutions at low concentrations of estradiol and sucrose. The data illustrate the concentration profiles of the partition coefficient solution for
3
H-estradiol
Although partition coefficients are shown to be independent of starting concentration, only the partition coefficient measurements within range of diffusion chamber solution concentrations (0.5 and 1 × donor solution values: 0.37 nM estradiol/3.9 nM sucrose and 0.73 nM estradiol/7.7 nM sucrose, respectively; Fig. 6, boxes) were averaged to calculate values shown in Figure 7 and used in Eq. 5. This was because previous work suggests that starting concentration influences the value of partition coefficients of other polar tracers 29 and including values derived from concentrations outside the scope of the diffusion system experiments would not improve the accuracy. Figure 7 shows the partition coefficient of estradiol was 42% higher compared with sucrose (44 vs. 31, p = 0.025).

Partition coefficient versus starting solute concentration, mean ± SD. Error bars represent the standard deviation of measurements from three bone specimens per starting concentration (error bars too small to be visible in some cases). Boxes illustrate the 0.5 × and 1 × concentrations for both estradiol and sucrose used to calculate partition coefficients in Figure 7. Color images are available online.
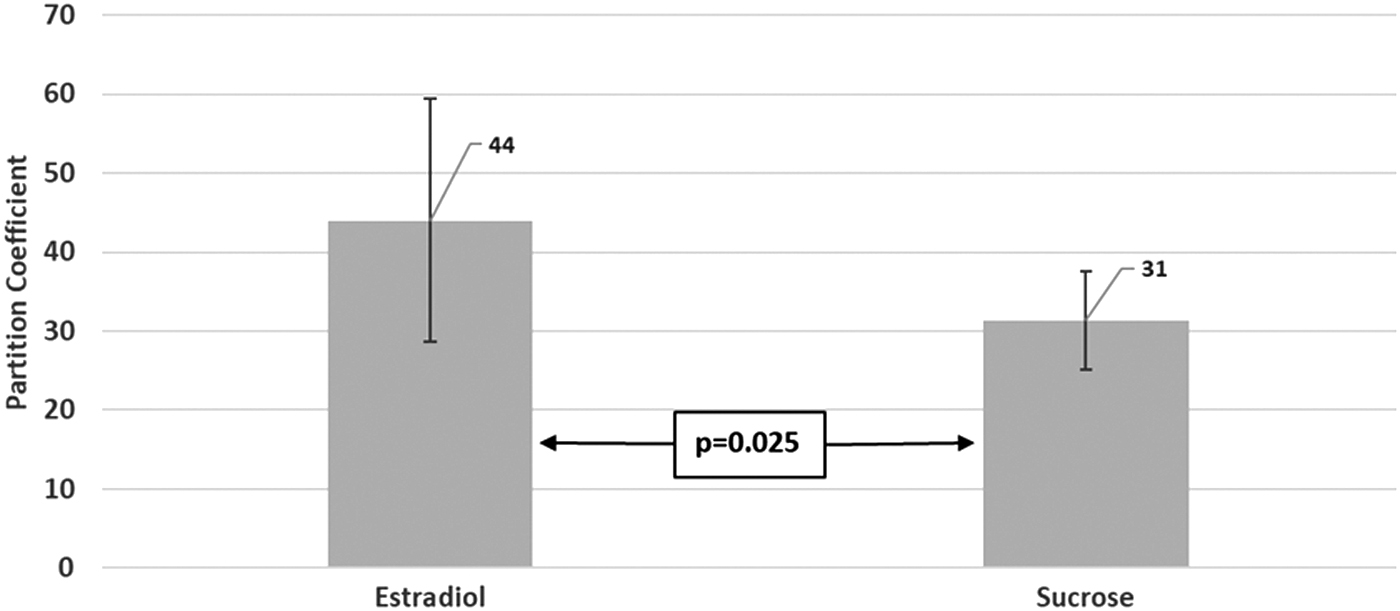
Partition coefficients used in diffusion coefficient calculations. The mean ± SD of the measurements from starting concentrations of 0.37 and 0.73 nM for estradiol and 3.9 and 7.7 nM for sucrose are shown here, for an n = 6 per group. These concentrations represent the expected range of concentrations within the diffusion system. Statistical analysis indicates a significant difference in partition coefficients of the two solutes (paired comparison, p = 0.025).
Experiment
Experimental design
The diffusivities of 3 H-estradiol and 14 C-sucrose were measured simultaneously through a single tibia bone sample in triplicate measurements to verify device repeatability. Immediately after assembly of the bone sample in the diffusion system and addition of the donor solution (0.76 nM 3 H-estradiol and 7.65 nM 14 C-sucrose in PBS) and receiver solution (PBS), two 50 μL aliquots were taken from each chamber, and daily thereafter, for the next 13 days. Each duplicate aliquot was pipetted into a 4 mL liquid scintillation vial (Perkin Elmer), followed by the addition of 2.5 mL of Ecolite+ liquid scintillation cocktail (MP Biomedicals, Santa Ana, CA). The vial was then sealed and vortexed for 10 s, and immediately counted for 10 min in the LS6500 liquid scintillation counter.
At the end of each trial, diffusion chambers were drained, residual solution volumes were recorded, and chambers were rinsed with 32 mL PBS for 10 min under medium convection before draining the rinse solution in preparation for the next trial. After the three diffusion trials concluded, the diffusion system was disassembled and cleaned with reverse osmosis purified water, and the bone specimen was stored at 4°C in fresh 0.05% sodium azide (w/v) PBS solution.
The governing equation for the diffusion system was derived from Fick's Law
28
and the mass balance on the solute in the receiver chamber
28
where J is solute flux; D is effective diffusivity;
Receiver chamber concentrations were converted to dimensionless concentrations (natural log equation term), which was plotted against time. The diffusivity was calculated from the slope (bold term) of the best-fit line. All calculations and statistical analyses were done in Excel. Paired t-test comparisons of the estrogen and sucrose diffusivities from the three independent trials were conducted to determine if values significantly differ between the nonpolar solute of interest and the polar control. The mass recovery from each diffusion system experiment was calculated as the sum of the moles of solute recovered (from all the donor and receiver chambers at the conclusion of the experiment, plus from all the aliquots taken) relative to the initial number of moles of solute added to the donor chamber.
Experimental Results
The solute recoveries reported from the diffusion chamber experiments account for the mass in both chamber solutions at the end of the trial and all sampling aliquots. The recoveries from the three diffusivity measurements of estradiol and sucrose were 94% ± 2% and 95% ± 10%, respectively, confirming conservation of mass. This is supported by full liquid volume recoveries from both chambers after all three trials. Solute concentration profiles in the donor and receiver chambers (Fig. 8a) were used to derive the dimensionless concentration curves (Fig. 8b) for calculating the diffusion coefficients. The linear fit of data in Figure 8b and the near complete conservation of mass corroborate the assumptions used in deriving Equation (5).
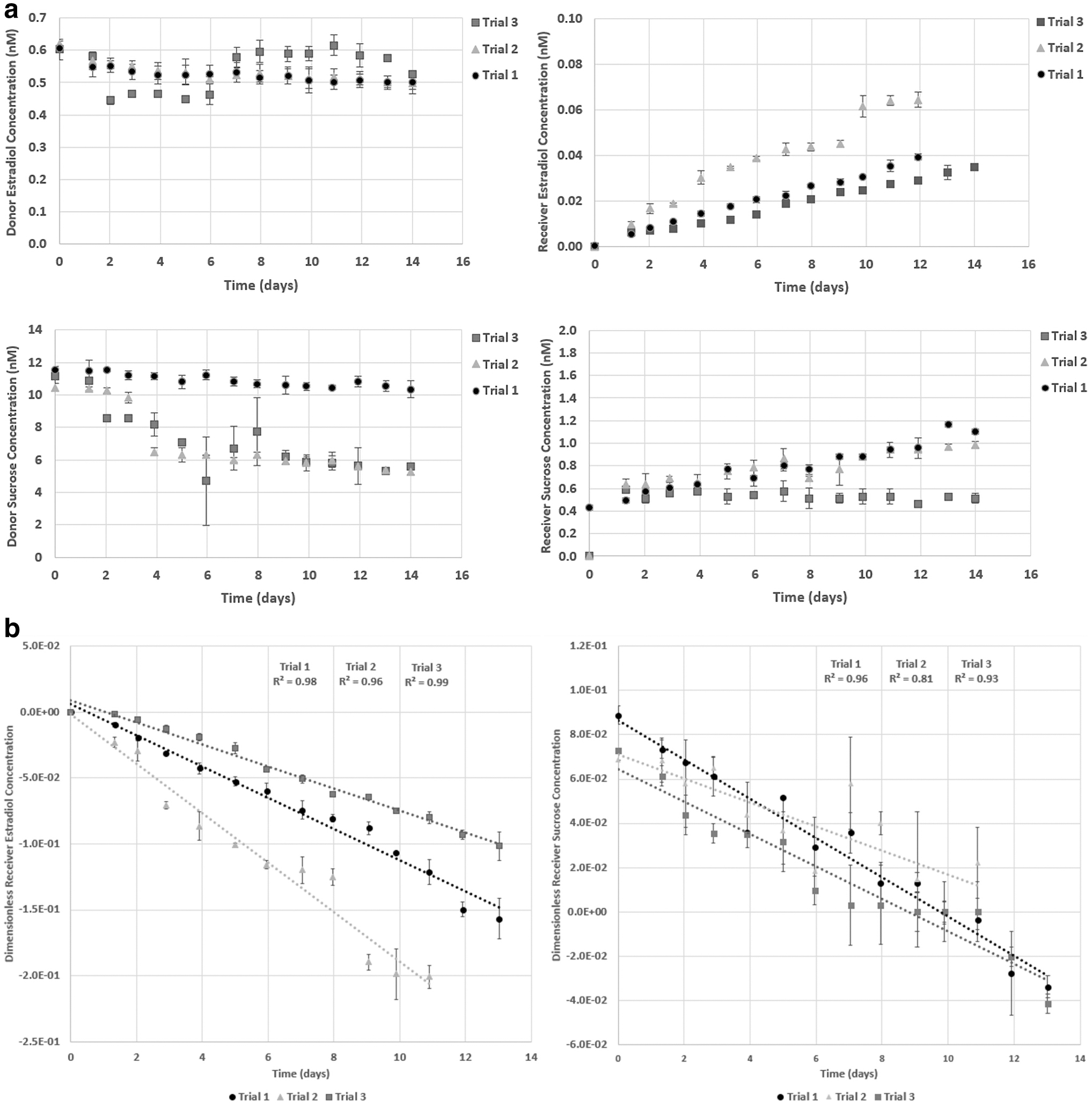
Repeated measurements of concentration profiles for a single bone specimen.
The figures demonstrate the diffusion of estradiol and sucrose through osteonal bone tissue over a 14-day experimental timeframe. Slopes of data from Figure 8b, along with the partition coefficients in Figure 7, were used to calculate the radial diffusion coefficients for both solutes (Table 2). The data reveal that estradiol diffusivity is 4.4-fold greater compared with sucrose in devitalized osteonal bone (p = 0.03).
Mean Radial Diffusion Coefficients (± Standard Deviation) in Cortical Bone from Three Independent Trials of the Same Bone Specimen
These data verify the ability of the diffusion system to repeatably obtain the dimensionless concentration profiles required to calculate diffusivity. Statistical analysis indicates a significant difference in diffusivities of the two solutes (paired comparison, p = 0.03).
Discussion
Previous diffusion system designs 16 required expensive custom fabrication with long manufacturing times. The current design reduces costs to around $65 per unit—a fraction of prior systems—while confirming minimal adsorption of varying solutes into the chamber components (Fig. 2b) and the absence of both internal and external leaking (Fig. 4b). The small footprint and easy fabrication of the device enable larger scale studies—necessary to assess biologically diverse samples—to be run simultaneously. An additional benefit is that this device does not require full disassembly between repeated trials.
Although the original application assessed bone, the device can be utilized with virtually any porous biological tissue (cartilage, arterial membranes, etc.) or engineered material (fuel liners, industrial rubbers, artificial membranes, etc.), so long as they are rigid enough to be fixed between the washers at the center of the diffusion chamber. To our knowledge, there is no other validated and easily fabricated device available that provides all these benefits, which defines its novelty and significance to the field. There is currently no standard device in the market for this and most examples in medical literature involve crafting a custom apparatus specifically for the experiment, typically restricting broader applications.
This work provides empirical partition coefficients of estradiol and sucrose in osteonal bone—44 and 31, respectively—at physiological temperature and estradiol concentrations, which have not been previously reported. Differences observed between these values are likely because the lipophilic nature of estradiol favors partitioning into the lipid content within the porous compartment of cortical bone,,30 while hindering the sequestration of the polar control sucrose.
This is the first study to directly assess estradiol diffusion through osteonal bone. The use of radioisotope tracers allows the simultaneous assessment of estradiol and the polar control sucrose at physiologically relevant concentrations, allowing direct comparison of the diffusion behavior of two opposing chemistries. Data show that the diffusion coefficient of estradiol in osteonal bone is greater compared with sucrose, suggesting that HVLCS lipids may serve as a transport medium for nonpolar molecules in healthy bone. Comparisons with a much larger sample size that assess diffusion through the same specimen in native and delipidized tissue states could confirm this hypothesis.
A limitation of this experimental approach at present is the inability to utilize live tissue in assessment, neglecting active transport mechanisms in vivo. The model equations used in this study also assume no metabolism of the solute, requiring use of devitalized bone tissue. Future studies could be done to assess estrogen diffusion in living osteonal bone tissue; however, this would require a complete re-design of the diffusion system and harvesting protocol, as well as derivation of a more complicated mathematical model that includes solute metabolism and a limited experimental timeframe, likely less than a week.
Footnotes
Acknowledgments
The authors would like to recognize Dr. Caroline Androjna from the Cleveland Clinic (CCF) Lerner Research Institute in Cleveland, OH, for her help in developing the protocols for bone dissection and for serving as the project's administrative coordinator after the retirement of Dr. Ronald Midura.
The authors would also like to recognize Dr. Robert McLain from St. Vincent Charity Hospital in Cleveland, OH. He provided a great deal of insight into the medical significance of the project and helped to establish the research rationale in a manner than maximized clinical relevance.
Vincent Cimino—an aerospace engineer from Parker Hannifin—deserves acknowledgment from the authors for his work in optimizing the spring clamp for compressive sealing of the diffusion system. Consultation of his knowledge on closed liquid systems was a contributing factor to the final design.
Authors' Contributions
N.C.: conceptualization (equal split), data curation, formal analysis, funding acquisition (independent funding), investigation, methodology, software (Excel Analysis, ImageJ, SolidWorks), validation, visualization, writing—original draft, and writing—review and editing (Editing article).
J.M.B.: conceptualization (equal split), funding acquisition (departmental funding), project administration (principal investigator), resources (theoretical application, CSU training, and laboratory oversight), supervision (project advisor and scientific mentorship), and writing—review and editing (primary article review).
R.M.: conceptualization (equal split), funding acquisition (2-year funding from the Cleveland Clinic), project administration (principal investigator at Cleveland Clinic before retirement), resources (bone physiology expertise, radioisotope safety and usage, CCF training, and laboratory oversight), supervision (project co-advisor and scientific mentorship), and writing—review and editing (secondary article review).
Disclosure Statement
No competing financial interests exist.
Funding Information
Funding came from Cleveland Clinic Lerner Research Institute and from the Chemical and Biomedical Engineering Department at Cleveland State University (CSU). A fellowship from the Cellular and Molecular Medicine Specialization (CMMS) and the Graduate Student Research Award (GSRA), both through CSU, are also gratefully acknowledged.