
Abstract
The ongoing coronavirus disease 2019 (COVID-19) pandemic highlights the importance of developing point-of-care (POC) antibody tests for monitoring the COVID-19 immune response upon viral infection or following vaccination, which requires three key aspects to achieve optimal monitoring, including three-dimensional (3D)-printed POC devices, mobile health (mHealth), and noninvasive sampling. As a critical tissue engineering concept, additive manufacturing (AM, also known as 3D printing) enables accurate control over the dimensional and architectural features of the devices. mHealth refers to the use of portable digital devices, such as smartphones, tablet computers, and fitness and medical wearables, to support health, which facilitates contact tracing, and telehealth consultations during the pandemic. Compared with invasive biosample (blood), saliva is of great importance in the spread and surveillance of COVID-19 as a noninvasive diagnostic method for virus detection and immune status monitoring. However, investigations into 3D-printed POC antibody test and mHealth using noninvasive saliva are relatively limited. Further exploration of 3D-printed antibody POC tests and mHealth applications to monitor antibody production for either disease onset or immune response following vaccination is warranted. This review briefly describes the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus and immune response after infection and vaccination, then discusses current widely used binding antibody tests using blood samples and enzyme-linked immunosorbent assays on two-dimensional microplates before focusing upon emerging POC technological platforms, such as field-effect transistor biosensors, lateral flow assay, microfluidics, and AM for fabricating immunoassays, and the possibility of their combination with mHealth. This review proposes that noninvasive biofluid sampling combined with 3D POC antibody tests and mHealth technologies is a promising and novel approach for POC detection and surveillance of SARS-CoV-2 immune response. Furthermore, as key concepts in dentistry, the application of 3D printing and mHealth was also included to facilitate the appreciation of cutting edge techniques in regenerative dentistry. This review highlights the potential of 3D printing and mHealth in both COVID-19 immunity monitoring and regenerative dentistry.
Impact statement
This review summarizes current research progress of combining three-dimensional (3D) printing and mobile health (mHealth) to develop point-of-care antibody tests to detect salivary COVID-19 (coronavirus disease 2019) immunity, as well in regenerative dentistry. This scoping review will advance the understanding of commercial use of 3D printing and mHealth and provide more insights for preparedness for future pandemics.
Color images are available online.
Introduction
Coronavirus disease 2019 (COVID-19), caused by a novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus, 1 has posed major challenges worldwide. It is evident that SARS-CoV-2 infection and vaccines for COVID-19 can trigger an innate and adaptive immune response resulting in immunoglobulin (Ig) antibody production2,3 detectable in various biofluids, such as plasma,4–7 saliva,8,9 urine, 10 and gingival crevicular fluid (GCF).11,12 IgM and IgA are considered indicators of early-stage infection, whereas IgG is an indicator of current or prior infection. 13 It is of considerable importance to develop reliable antibody detection tests against SARS-CoV-2 for either infected populations or trace immune responses after vaccination. Neutralizing and binding antibody tests are two common tests to detect humoral antibodies against the SARS-CoV-2 virus, where neutralizing antibodies block the entry of a pathogen into a cell, whereas binding antibodies reflect the presence of a pathogen in the body. 14
Most currently available binding antibody tests are two-dimensional (2D) platforms (i.e., microplates) using blood samples requiring invasive and resource-intensive sampling. 14 Given the high demand for testing, “off-the-shelf” point-of-care (POC) antibody tests with high sensitivity and specificity using noninvasive biofluids (e.g., saliva) are needed to assess and monitor immune response in the general community. According to International Standard ISO 22870, point-of-care testing (POCT) is defined as “medical testing that is performed near or at the site of a patient with the result leading to a possible change in the care of the patient.” Developing POC antibody tests are essential to monitoring immunity for the general community.
Emerging material and manufacturing technologies that can be harnessed to develop novel approaches to accurate monitoring of COVID-19 disease status and immunity are discussed below. In the context of the COVID-19 pandemic, various POC platforms have been developed to deliver care near the patient, such as lateral flow assay (LFA), 15 microfluidic devices, and electrochemical biosensors (reviewed in Ref. 16 ). Application of developing technology such as additive manufacturing (AM) has shown promise in the design and fabrication of personal protective equipment, ventilators, nasopharyngeal swab test devices, customized masks, and even emergency dwellings (reviewed in Refs.17–20 ).
AM, also known as 3D printing, is an advancing tissue engineering technology in which a product derived from a high-resolution computer-aided design (CAD) model is “printed” layer by layer by technologies, such as fused deposition modeling (FDM), melt electrospinning, melt electrowritting (MEW), or bioprinting. 21 FDM is a 3D printing method that extrudes layers of molten thermoplastic onto a stationary collector plate and is compatible with a variety of polymers (polylactic acid [PLA]) and polymer composites.22,23 MEW is another high-resolution AM method to produce tunable fibers and porosity of 3D structures in micro- or nanoscale range using a moving collector to facilitate direct writing using gold standard poly(ɛ-caprolactone) (PCL) polymer.24–26
The AM technique is utilized for multiple industrial applications, including implantable tissue-engineered constructs and biomedical applications such as personalized external medical devices and instruments to combat COVID-19 pandemic.27–29 In terms of using AM in COVID-19 antibody detection, our recent research developed a salivary SARS-CoV-2 antibody detection platform using S1-receptor-binding domain (RBD) protein-immobilized 3D PCL scaffolds. 30 Compellingly, this technology has paved the way to advance 2D assay systems toward development of 3D testing platforms with improved sensitivity, efficacy, and cost-effectiveness offering novel POC options.
Mobile Health (mHealth) is an emerging health concept that uses mobile devices and related technologies in health care to diagnose, track, and control infectious diseases (i.e., Ebola and COVID-19).31–33 The mHealth market was valued at $11.5 billion in 2014 and is expected to rise to $316.8 billion by 2027, indicating its increased interest despite regulations and security challenges related to patients' personal information. During the COVID-19 pandemic, mobile phone-based applications (apps), automated text messaging, wearable devices, and mobile telehealth are common applications to improve the efficiency of health systems. The application of mHealth facilitates site monitoring, fast screening, patient monitoring, information sharing, education, and treatment in response to COVID-19 outbreak.34–38 During the pandemic, for example, mHealth apps monitoring a patient's vital signs remotely can instantly send and receive real-time information across multiple providers and platforms, without direct contact.
Other than AM and mHealth technologies, clinical biosampling, particularly noninvasive oral biofluids (i.e., saliva), is another critical aspect of immunity monitoring. Saliva is an attractive diagnostic method for the detection of SARS-CoV-2 due to its low cost, noninvasive, and easy to access, containing a variety of biomolecules such as extracellular vesicles, 39 DNA, RNA, proinflammatory cytokines, SAS-CoV-2 antibodies, 12 viruses, and metabolites.40,41 A variety of salivary local and systemic biomarkers have been revealed to be associated with various diseases while saliva is a “foe” during COVID-19 pandemic by spreading the virus via aerosols and droplets during dental aerosol-generating procedures.42–44 Therefore, saliva samples can be used as a powerful tool for detection and screening of SARS-CoV-2 virus and antibodies.
As for the immune response to viral infection or following vaccination, it is necessary for health care departments and individuals to monitor real-time antibody levels to guide future vaccine booster protocol in line with the seemingly long-term health challenge posed by the COVID-19 pandemic. In 2020, the World Health Organization (WHO) recommended not using POC immunodiagnostic tests for patient care, rather encouraging the continuation of work to establish their usefulness in disease surveillance and epidemiological research.
However, the concept of combining 3D-printed testing (POC) devices with mHealth in the management of COVID-19 immunity presents a logical approach to the acquisition of real-time data tracking both positivities in those who have contracted the SARS-CoV-2 virus (diagnostic) and identifying local infection rates and trends in a population (surveillance), obtained from self-testing individuals. Present knowledge around this is limited.
The current literature focuses extensively on the application of POC diagnostic devices to detect SARS-CoV-2 antigens and COVID-19 treatment; however, the importance of POC antibody tests and mHealth has not been sufficiently explored in relation to detecting immune responses against the SARS-CoV-2 virus. The present review highlights recent advances in the application of additively manufactured devices and mHealth to effectively monitor humoral immune response against SARS-CoV-2. The combination of additive-manufactured 3D antibody tests and mHealth may offer great promise in monitoring an individual's and community's immunity status and evaluating the effectiveness of vaccines.
SARS-CoV-2 Virus and Adaptive Immune Response upon Viral Infection or Vaccination
COVID-19 disease transmission via aerosols and droplets has resulted in rapid spread to more than 200 countries leading to a global pandemic.43,45,46 It is well known that SARS-CoV-2 is a positive-sense, single-stranded enveloped RNA virus with a diameter of 60–140 nm and a length of ∼30,000 nucleotides, 47 containing four structural proteins, including spike (S) protein, nucleocapsid (N) protein, envelope (E) protein, and membrane (M) protein (Fig. 1a). 48 The M and E proteins are necessary for virus assembly, whereas the S protein is critical for the virus to infect host cells.

The structure of SARS-CoV-2 virus and the COVID-19 immunity.
The S protein, with a size of 180 kDa, contains a highly conserved C-terminal S2 subunit and a less conserved N-terminal S1 subunit that mediates receptor binding and cell membrane fusion. 49 The S1 subunit comprises an N-terminal domain and a RBD 50 specifically recognizing receptor angiotensin-converting enzyme 2 (ACE2) on the host epithelial cell membrane (on the oral mucosa or lung). 51 It is noted that the S2 subunit mainly plays a role in the fusion of cell and virus membranes, facilitating SARS-CoV-2 access to human cells, whereas the S1 subunit exhibits greater variations. 52 Therefore, the spike (S) protein, especially the S1 subunit, has become a common target for COVID-19 vaccine research to minimize cross-reaction with other coronaviruses.
During the COVID-19 pandemic, the SARS-CoV-2 virus has been constantly evolving and mutating. 53 As of May 2022, the WHO identified the Omicron variants (Fig. 1b) as variants of concern (VOC) since they have been shown to significantly increase infectivity and reduce vaccine effectiveness, 53 where S protein mutations increase infectivity and transmissibility and facilitate the virus to evade vaccine-induced immunity. Previously, the WHO identified the Alpha, Beta, Gamma, Delta, and Omicron variants as VOC. The Lambda and Mu variants are variants of interest that are predicted to pose risks to global health. It is of considerable importance to understand how the host immune response occurs upon infection and vaccination; this will be reviewed in the following sections.
Extensive host immune responses are stimulated upon SARS-CoV-2 infection after recognition of virus surface epitope, eliciting innate and adaptive immune responses with a hyperinflammatory cytokine storm in some severe COVID-19 cases. 47 Increasing research demonstrates a general adaptive immune response toward SARS-CoV-2 viral infection or vaccination by activating specific B and T cells to generate Ig antibodies (Fig. 1c). 54 Taken together, upon infection by SARS-CoV-2 virus, host innate and adaptive immune response systems are activated to generate proinflammatory cytokines/chemokines and eventually produce Ig antibodies to protect the host from being reinfected. It thus may be useful to use antibody testing to determine whether an individual has a prior infection, especially for antibodies against the N protein.
The serological assay can identify patients who have developed an immune response upon viral infection or following vaccination at varied time periods (Fig. 1d) by detecting viral antigens in the blood. 55 There are three isotype antibodies, IgG, IgM, and IgA, that are the targets of serological testing. Studies have shown that IgM antibody is the earliest antibody and the antibody response peaks within 1 week of the patient's illness. 54 IgA and IgG antibodies are produced a few days after the appearance of IgM antibodies and reach a peak in 2–3 weeks after viral infection. 56 The IgG antibody has a neutralizing effect and can persist in the human body for several months. 57 Besides viral infection, vaccines can generate Ig antibodies by mostly targeting the S protein as an immunogen to prevent the interaction between the S protein and the ACE2 receptor.
For instance, the BNT62b1 Biotech Pfizer vaccine can effectively boost immune response, with a 91- to 368-fold increase in IgG levels 21 days after the first dose of mRNA vaccine (30 μg), with antibody levels peaking 35 days after vaccination. 58 The second dose of Pfizer mRNA vaccine further increased antibody levels, with a 1.3-fold increase in IgA levels and a second peak on day 28. 58 IgA levels subsequently decreased but were still 15 times higher than before the vaccine was administered. 58 Thus, detecting these antibodies is important to trace host adaptive immune response for both viral infection and post-vaccination, which has limited studies in the field.
Current and Developing Antibody Test Platforms with a Focus on 3D-Printed POC Devices
Following vaccination or disease onset, antibody tests can monitor antibody generation for diagnosis of suspicious cases with negative viral RNA test, past-COVID-19 infection, or immune response surveillance assessment post-vaccination. As previously reviewed, 14 antibody neutralization assays and binding antibody tests are the common antibody assays used to determine different aspects of the adaptive immune response. The neutralizing antibody test and the binding antibody test differ in that the neutralizing antibody binds to a specific part of the pathogen and prevents it from entering the cell, whereas the binding antibody binds specifically to the pathogen but does not interfere with its infectivity. 14
Although antibody tests can use specific antigens, antibodies raised against different proteins may cross-react and may not provide sufficient information about the existence of antigen-specific antibodies. Thus, antibody tests need to reveal a good performance with high specificity and sensitivity. There is no WHO international standard to evaluate antibody response; 59 it is challenging to state whether either neutralization or binding antibody tests is a better candidate. The current review will focus on developed or currently developing tests (listed in Table 1), such as enzyme-linked immunosorbent assay (ELISA), field-effect transistor (FET), and LFA and novel state-of-art technology (3D printing) to manufacture binding antibody tests.
Selected Key Studies of Point-of-Care Antibody Test Platforms
“—” indicates that results are not applicable or unstated.
3D, three-dimensional; AuNP-LF, colloidal gold nanoparticle-based lateral flow assay; COVID-19, coronavirus disease 2019; ED, electrodeposition; ELISA, enzyme-linked immunosorbent assay; FDM, fused deposition modeling; FET, field-effect transistor; g-FET, graphene field-effect transistors; IFA, immunofluorescence assay; LNPs, lanthanide-doped polystyrene nanoparticles; LOD, limit of detection; PDMS, polydimethylsiloxane; POC, point-of-care; RBD, receptor binding domain; rGO, reduced graphene oxide; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; TBC, triblock copolymer.
ELISA is a gold standard immunoassay that uses whole blood or other biofluids to perform the antibody test on a microplate or microbeads platform. An FET is a transistor in which the voltage on one terminal (the gate) creates a field that allows or disallows conduction between the other two terminals (the source and drain). 60 LFA is a POC device that can detect Ig antibodies in fingerstick whole blood by providing semiquantitative results, consisting of four essential parts in a cassette: the sample pad, conjugate pad, nitrocellulose membrane, and absorption pad.15,61,62
As an emerging field, 3D printing and polymer science have arisen in response to the COVID-19 pandemic, particularly for antibody test development. Selected 3D platforms using either 3D printing or microfluidics technologies to enable on-demand solutions for novel antibody test development will be discussed in this review. However, it is necessary to understand the foundation of a successful antibody test, such as clinical samples and antibody testing challenges, which are highlighted in the following section.
Clinical sampling for anti-SARS-CoV-2 antibody detection
Due to the high sensitivity of serological testing, blood (plasma, serum) is extensively used for SARS-COV-2 antibody testing in patients. 63 However, blood collection is invasive, requires a pathologist or nurse, and with increased health risk potential for patients and collectors. Noninvasive body fluids, such as saliva, are an alternative source for antibody tests being easy to access and relatively safe. Patient saliva samples can be used as a method for COVID-19 Ig isotype antibody detection, achieving 84.2% sensitivity and 100% specificity in COVID-positive patients.64,65 Self-collected saliva by spitting has been authorized by the Food Drug Administration (FDA) Emergency Use in the Yale School of Public Health using the SalivaDirect™ test, and saliva home tests have been manufactured for patients; this can significantly reduce the risk for frontline health care workers.
Moreover, a small number of studies have shown that IgG antibodies against the spike protein are detected in saliva after BNT162b2 vaccination.9,12,66,67 However, it is worth noting that antibody concentrations in saliva are ∼500 times lower than that in plasma. 66 More recently, breast milk was reported as a potential sample type for the detection of SARS-CoV-2 antibodies. Studies have shown that high levels of IgA antibodies against SARS-CoV-2 can be detected in the breast milk of mothers infected with the coronavirus. 68 Studies using other noninvasive biofluids such as tears, 69 urine, 10 and GCF11,12 are advancing the COVID serological test field. While these noninvasive fluids might not require trained medical professionals to collect samples, with relatively lower analytes than that in plasma, continuing studies using plasma or blood samples are necessary to validate the viability of noninvasive samples.
Current available ELISA assays for Ig detection
At present, ELISA is the gold standard for SARS-COV-2 immunoglobulin IgA, IgM, and IgG detection using 2D microwell or microbeads platforms by indirect ELISA, direct ELISA, or sandwich ELISA (Fig. 2a). 14
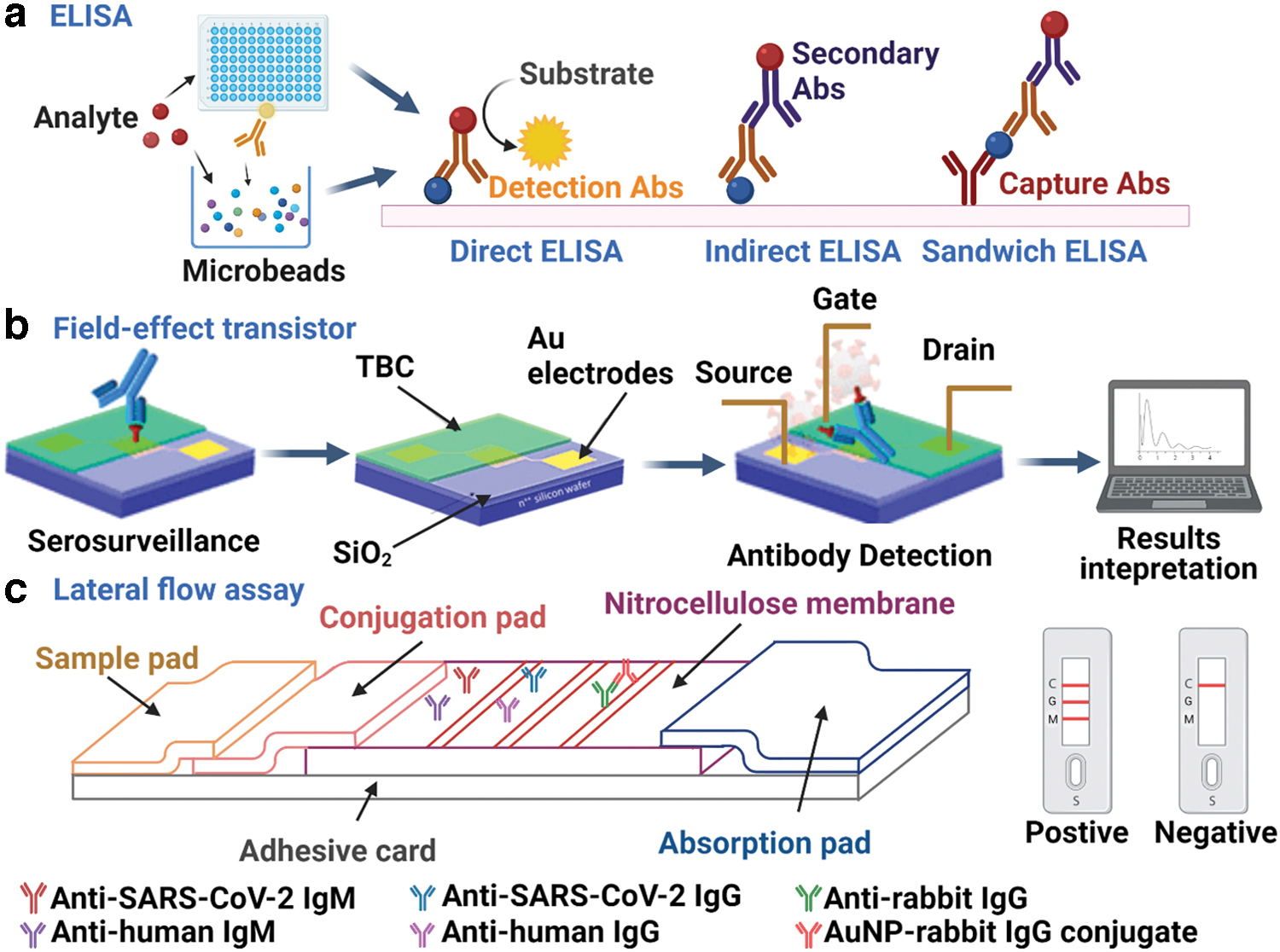
Representative antibody binding tests to detect COVID-19 antibody production, such as
Indirect ELISA is a two-step ELISA that involves the binding of the primary antibody to a specific antigen that is coated on a microwell and the binding of the secondary antibody to the primary antibody. 70 Indirect ELISA is highly sensitive but may result in nonspecific signaling due to the risk of cross-reaction of secondary antibodies. 70 Experiments confirm that the indirect ELISA detection of SARS-CoV-2 S1 has a specificity of 97.8%, reproducibly and accurately. 71 Examples of commercial indirect ELISA kits for COVID include CD Creative Diagnostics DEIASL019 SARS-CoV-2 IgG ELISA Kit, Canvax COVID-19 Human IgG Indirect ELISA Kit (EL0074), and RayBiotech IEQ-CoVS1RBD-IgG-DBS.
Direct ELISA is used to measure the antigen directly to the ELISA plate and then detects the antigen using conjugate antibodies. 70 Compared with other ELISA types, direct ELISA is faster but less sensitive and has a higher reaction to background noise. 70 Examples of current commercial direct ELISA kits for COVID include Mybiosource COVID-19 Spike Protein S1 IgG Coronavirus ELISA Kit and LifeSpan Biosciences Human SARS-CoV-2 Spike IgM (Direct ELISA) ELISA Kit.
The sandwich ELISA is used to coat the capture antibody on the ELISA plate, with the antigen sandwiched between the capture antibody and the detection antibody. 70 Sandwich ELISA has the characteristics of high sensitivity and high specificity, but there may be a cross-reaction between the capture and detection antibodies. 70 Chen et al reported that the precision of measuring 10 COVID-19-positive sera using sandwich ELISA is 3.0–4.4%. 72 Examples of commercial sandwich ELISA kits for COVID include CD Creative Diagnostics DEIA2020 SARS-CoV-2 Antigen ELISA Kit and GeneTex SARS-CoV-2 Nucleocapsid Protein Sandwich ELISA Kit.
Multiplex microbeads-based immunoassays detect COVID-19 antibodies in test fluid (blood, plasma, serum) by utilizing microbeads covalently coupled with SARS-COV-2 S protein, spike protein RBD, or nucleocapsid.73–76 The diagnostic time of multiplex immunoassay is usually between 12 min and 2.5 h.74,75 Compared with ELISA and PCR, the sensitivity and specificity of microsphere immunoassays are 95–97% and 99–100%, respectively. 74 Cameron et al noted that microsphere immunoassays have higher sensitivity at an earlier time point after infection (<5 days from symptom onset). 73 Weiss et al reported that only 5–10 ng antigen is used for each test, which uses 20 times less antigen than that required by ELISA and can perform thousands of tests on antigen-coated beads in 1 day. 75 In addition, SARS-COV-2 does not cross-react with other diseases during microbead immunoassay, and interfering substances do not cause the system to produce inaccurate results.73,76
In general, ELISA has the advantages of high sensitivity and high specificity, but its limitation is that it is time-consuming (>4 h) and not suitable for high-throughput screening and analysis. 70 Importantly, the sensitivity and specificity of ELISA assays largely rely on the antigen/antibody choice; different commercial ELISA kits showed a range of 50–100% of sensitivity and 80–100% of specificity. 77 It is worth noting that ELISA is a 2D platform detection technique; advanced materials and 3D printing platforms (discussed more below) offer novel approaches to improved and efficient methods for SARS-CoV-2 antibody detection.
FET and LFA for SARS-CoV-2 immune response
The FET-based detection platform is a three-terminal (source, gate, and drain) active device using an electric field to control the current flow in a semiconductor, used for COVID-19 serological detection with advantages of high sensitivity, real-time measurement, and less analyte required (Fig. 2b).78–80 Such three-terminal FET devices enable the straightforward amplification and fine-tuning of measured electrical signals by controlling the applied voltage on the gate electrode. Graphene, a two-dimensional sheet of hexagonal carbon atoms, is used in a variety of sensing platforms due to its high conductivity and carrier mobility. 78 Graphene-based FET sensors can be used to detect SARS-COV-2 antibodies in serum and human nasopharyngeal swabs. 78 According to Kang et al, the average diagnosis time of COVID-19 by a graphene-based FET sensor was about 5.3 min, with the shortest time of 2 min. 81
On the contrary, Ditte et al reported that a biosensor based on an FET could rapidly detect SARS-COV-2 within 20 min using a mobile device. 82 The limit of detection (LOD) for FET is 10–18 M and the lowest LOD value of SARS-CoV-2 antibody biorecognition events occurring in graphene surface was 150 μL antibody in 100 μL full serum. 81 Seo et al showed that the LOD value of the FET biosensor (1 fg/mL of SARS-COV-2 spike protein) was much lower than that of ELISA, and there was no cross-reaction between the COVID-19 FET sensor and MERS-CoV spike protein. 78 In addition, the COVID-19 FET sensor can detect SARS-COV-2 without the preprocessing of samples. 78
Of note, the biosensor developed by Ditte et al adsorbs the SARS-CoV-2 RBD receptor and S1 antibodies to the stretchable poly-diketo-pyrrolopyrrole-thienothiophene (PDPP-TT) triblock copolymer surface that is conjugated semiconductors flanked by two soft elastic polydimethylsiloxane (PDMS) segments. 82 The antigen/polymer layer is then used for selective binding to target S1 antibody (or RBD) and detects biometric effects through electronic transduction. The average LOD of OFET biosensor was 0.36 fg/mL. RBD sensing has a narrower dynamic range (10 pg/mL–1 μg/mL), and its sensitivity is better at high concentrations. 82
LFA is a simple method for the detection of target substances in liquid samples (similar to a pregnancy test), where antibodies are used to recognize antigens, proteins, or hormones by using a sandwich LFA. 61 In an LFA device (Fig. 2c), the sample is applied on a sample pad before flowing to a conjugation pad with gold nanoparticles conjugate and antibodies, which allow the formation of antibodies and conjugation labels complex. After the interaction, the antibody along with the target migrates toward a detection zone on LFAs consisting of another set of antibodies that react to the target molecules bonded to the antibodies present in the previous zones. The lines appearing at different intensities can be interpreted visually or via a dedicated mobile reader. Huang et al coupled colloidal gold nanoparticles (AuNPs) with anti-human IgM antibody that was then fixed on the conjugate pad of AuNP-LF test strip (consisting of a sample pad, conjugate pad, nitrocellulose membrane, and absorption pad). 61
After the serum sample was added, IgM was bound by the gold conjugate, and the Au-NP-IgM complex was then captured by SARS-CoV-2 NP via capillary action at the analysis membrane. 61 The gathered gold particles produced visible red lines indicating positive detection. 61 LFA diagnosis usually takes 15–20 min and requires only 10–20 μL of serum per test.61,83–85 Conklin et al 83 and Huang et al 61 showed that LFA had no cross-reaction with other viruses during the detection of SARS-COV-2, with a sensitivity of 100% and specificity of 93.3–100%.
LFA tests satisfy the assured criteria established by the WHO, with approved commercial (Wondfo SARS-CoV-2 Antibody Test) or laboratory LFA tests. The advantage of LFA technology is that a small volume of various body fluids can be used for detection, and the technology is low in production cost and easy to use. However, variability and antibody cross-reactivity between batches, sensitivity limitations, and the fact that its analysis results are qualitative or semiquantitative remain challenges for the LFA test in terms of accurate diagnosis.
Additively manufactured devices for antibody tests
A novel AM approach with potential in combating the COVID-19 pandemic is the use of 3D printing and polymer science to design complex devices with a high surface area that can be modified to incorporate sensitive molecules for COVID-19 antibody detection, such as 3D-printed POC chips and 3D microfluidic devices. A POC chip is a simple medical diagnostic device allowing rapid and reliable results that can be used outside of a laboratory setting. A microfluidic chip is a set of microchannels etched or molded into a material (glass, silicon, or polymer such as PDMS). The microchannels forming the microfluidic chip are connected to achieve the desired features (mix, pump, sort, or control the biochemical environment). The outcomes would be cost-effective, sensitive, and customizable detection devices. Following this approach, eight works using 3D-printed POC chips (Fig. 3a

Representative 3D-printed POC chip
Mortelmans's team developed a 3D device for rapid and multiplex detection of IgG and IgM antibodies in convalescent human serum and further detection of anti-spiking SARS-CoV-2 and anti-influenza A hemagglutinin antibodies simultaneously. 86 The device is a 3D polymethylmethacrylate (PMMA) nanofluidic particle sorter that incorporates passive capillary microfluidic elements to control fluid flow, thereby eliminating the need for an external loading mechanism. Nanofluidic devices fix the particles from multiparticle mixtures by size in nanochannels to generate distinct trapping lines for size sorting and size determination. The SARS-CoV-2s-RBD was coated on beads and combined with an on-bead serological immunoassay to detect SARS-CoV-2 and influenza A antibodies.
The device concentrates and captures S-RBD-functionalized beads in IgG SARS-CoV-2 serological assays and detects anti-S-RBD and anti-hemagglutinin antibodies in samples by different bead sizes. During the evaluation of the SARS-CoV-2 IgG antibody immunoassay, the fluorescent signal LOD of the captured beads was analyzed at 0.8 nM, achieving subnanomolar detection limits for different analytes. The 3D nanofluidic device can quickly and efficiently complete serological detection, and the sample volume can complete multiple detections of various antibody types with only 4 μL. In future applications, a single chip could detect more than 100 antibodies and use in conjunction with a smartphone.
Ali et al 87 developed an N protein-based 3D biosensor for rapid quantification of SARS-CoV-2 antibodies via electrochemical transduction. The sensor is composed of a set of 3D micro-length-scale electrode structures fabricated by aerosol jet 3D printing, including an array of gold nanoparticle micropillars coated with reduced graphene oxide (rGO) nanosheets and N protein. The micropillar array realizes N protein coverage onto the 3D microsurface through an intermediate layer. The counter, reference electrode, and micropillar array are integrated into the PDMS-based microfluidic channel and form an electrochemical cell. The electrochemical transduction detects the antibody of N protein through the antibody–antigen interaction on the surface of the micropillar. (The detailed mechanism is written below in Ali et al, 2021.) Using AJ-printed 3D sensors, the N protein was found to be highly immunogenic compared with the S protein and fully expressed after infection.
The 3D sensor detection (LOD 13 fm) is 20-fold higher sensitive than the 2D sensor (LOD 2.5 pm) in terms of N-antibody, and its analytical sensitivity reaches 100 fm. More importantly, ∼94% of the impedance signal during the detection of N protein antibodies by the 3D sensor were reached within 8 s, and the detection was completed within 10–12 s. In addition, the 3D biosensor can be regenerated at least 10 times to reduce costs, providing a powerful tool for rapid screening of SARS-CoV-2 antibodies after infection or vaccination.
Muñoz's team developed a novel 3D-printed COVID-19 electrochemical immunosensor with high sensitivity. 88 FDM was applied to print non-porous pendulum-shaped electrodes using conductive graphene-based nanocomposite fillers dispersed in an insulating PLA polymer matrix (G/PLA). Surface treatment was applied to eliminate the PLA and expose the graphene-based electrode, followed by electrochemical activation. SARS-CoV-2 S1-RBD recombinant protein was covalently immobilized on the surface of a 3D-printed (FDM) graphene/PLA nanocomposite electrode, and [Fe (CN)6]3-/4- was used as a redox probe to detect the electronic output of different concentrations of antigen through the change of the electrode's charge transfer resistance.
The combination of biomarkers and accessible antibodies promotes an insulating layer formatted on the electrode surface, which hinders the [Fe (CN)6]3-/4- redox reaction. The results of the electrical analysis demonstrated good sensitivity of the 3D-printed electrochemical immunosensor, with the antigen protein LOD being 0.5 ± 0.1 μg/mL. Monoclonal S1 antibody does not cross-react with nonspecific proteins and confirms the high specificity (97%) of monoclonal S1 antibody. Additionally, nonspecific proteins did not interfere with the 3D-printed immunosensor in experiments using a 100-fold diluted human serum sample. 88
Using another AM approach, Ali et al 89 manufactured an intricate biosensing platform using a 3D nano-printed electrode coated with rGO nanoflakes comprising immobilized SARS-CoV-2 S1 and RBD protein antigens. The electrode was manufactured with a highly precise process utilizing aerosol jet 3D printing to fabricate characteristic gold micro-columns (ø = 75 μm and height = 250 μm) with an increased total electrode surface area. The 10 × 10 gold micro-pillar electrodes were encapsulated within a replica-modeled PDMS housing unit. When the antibody enters the electrode surface, the antigen–antibody-specific binding causes a change in the circuit's impedance, which is then read by the smartphone platform. The platform is capable of detecting the presence of S1 and RBD antibodies in 5 μL of blood samples. 89
Experimental data showed that the 3DcC (3D-printed COVID-19 test chip) device could observe the change of impedance signal when the concentration of S1 antibody was 0.01 fm (4.2 Ω). 89 When the antibody concentration exceeds 10 × 10–9 M, the sensor shows a saturation impedance signal. 89 However, RBD sensors show different responses between 1 × 10–12–100 × 10–12 M and 100 × 10–12–20 × 10–9 M. This illustrates the high sensitivity of the biosensing platform. Detection time experiments showed that the impedance signal of S1 and RBD antibodies reached 93.2% and 92% of the saturation signal, respectively, in 11.5 s. The S1 and RBD antibodies were found not to have protein cross-reactivity. 89
It should be noted that a smartphone was used in this work. While maintaining control of the 3D-printed structure is challenging, this COVID test may represent a promising alternative for effective immune response monitoring with high sensitivity and specificity, although it does not provide comparatively low-cost and rapid prototyping as demonstrated by Muñoz and Pumera. The authors, however, have proposed that future designs could combine a multiplexed chip to enable the immobilization of several SARS-CoC-2 antibodies and thus provide detection of several past and emerging variants concurrently.
Other microfluidic devices present an alternative sensitive and specific method for the detection of antibodies (Fig. 3b).90–93 Glass, silicon, or polymer (PDMS) are the most common substrates to fabricate microfluidic devices as they are inexpensive and the creation of microchannels can be easily performed by embedding and molding techniques. Cognetti et al reported a silicon photonic sensor platform that combines a silicon nitride ring resonator-based detection with plastic micropillar microfluidics to detect viral antibodies. The sensitivity and specificity were 77.8% and 100%, respectively, and the diagnosis time was only 1–5 min. 90
Of note, Swank et al have developed a nano-immunoassay (NIA) that can analyze 1024 samples on a single microfluidic device. 91 The NIA had a 98% sensitivity and 100% specificity against 134 negative and 155 positive sera. The advantage of this method is that only 0.6 μL of serum sample can be detected and the reagent cost is 1000 times lower than traditional ELISA. 91 Lin et al established a portable microfluidic immunoassay system, which can quickly detect SARS-COV-2 antibodies within 15 min with a specificity of 100%. 92 Both patient serum and nasopharyngeal swab samples can be used in the system, and the data suggest that serum samples are more sensitive than nasopharyngeal swab samples. 92 Funari et al used a gold nanospike opto-microfluidic sensing platform to detect antibodies in <30 min. 93 The LOD is 0.5 pm, and the detection process is not interfered with other molecules. 93 These studies demonstrated that polymer-based 3D-printed chips and microfluidic devices may be effective alternative platforms for COVID-19 antibody response monitoring.
Summary and discussion of different antibody tests
The greatest challenge currently faced by all immunoassays is that no definitive results can be generated due to the performance of these serological assays showing diversity in clinical scenarios, as reviewed by Liu et al. 14 False-positive and false-negative detection hurdles in antibody immunoassays and usually represents a weakness in the sensitivity and specificity of the test. False negatives are mainly due to poor sensitivity of samples or low antibody levels, whereas false positives are usually due to antibody cross-reaction or contamination of sample reagents during collection and/or testing. 14 In the case of standard ELISA, uneven probe–protein coupling and background noise can lead to false-negative results. 14 However, limitations of false-positive and false-negative test results can be overcome by employing two independent tests that detect different antibodies or use different antigens or protocols. Detection platforms such as 3D-printed POC biosensors with high sensitivity and specificity can be used to reduce the frequency of false positives and false negatives.
Another limitation of antibody tests for the general community is the interpretation of the results (shown in Table 2), which may require a general practitioner to validate. In some cases, vaccinated participants may not develop antibodies, which makes antibody tests more difficult to be utilized. Moreover, antibody tests can detect prior infection (if the anti-N protein is positive) and vaccination history (if the anti-S protein is positive), whereas they cannot reflect a patient's current viral infection. As such, the antibody test is not an optimal tool for clinical diagnosis. Thus, antibody tests are not recommended by the WHO to assess for immunity to SARS-CoV-2 following COVID-19 vaccination. However, it is worth exploring to reach a highly sensitive antibody test for monitoring waning immunity for future vaccine boosts.
Interpretation of COVID-19 Antibody Tests
The development of high-performance platforms for rapid, sensitive, and specific testing remains the goal for combating COVID-19. As presented in Table 1, assay sensitivity and specificity range from 25% to 100%, and test detection time varies between 11.5 s to a few hours among the antibody detection strategies described above. Sampling volume among tests ranges from 0.6 to 100 μL indicating that all listed technologies have high sensitivity, requiring the least amount of blood samples. It is noted that all studies in Table 1 used either blood or nasal samples for antibody tests, with no attempts to use noninvasive fluids such as saliva—an important focus for future studies.
Another aspect of note is that it remains challenging to compare 3D and 2D platforms as no standardized antibody detection was used. However, 3D printing and polymer science may offer promising novel antibody test development with ultrasensitive detection limits and immediate detection (i.e., 13 fm within 10–12 s 86 ). While conventional ELISA requires at least 4 h to complete an assay, nanomaterials-based technologies for SARS-CoV-2 antibody detection are emerging with the development of biosensors and enhanced ELISA-based sysems,94,95 the employment of polymers—PLA, PMMA, PDMS, or PDPP-TT PSC81,82,86,88—to manufacture antibody tests, and novel 3D-printed POC tests that are reproducible, less costly, and easily modified to detect antigens and antibodies within seconds.88,89
Natural or synthetic polymers with different 3D printing techniques (e.g., MEW, bioprinting) can be validated in future studies to manufacture 3D antibody test platforms. Despite a relatively small number of studies, the potential for 3D printing material science-based technologies as an effective tool for immunity surveillance within the community is compelling.
To summarize selected reviewed POC antibody tests, the advantages, disadvantages, and commercial potential are listed in Table 3. In reported findings, 3D-printed POC devices show great promise compared with laboratory-based ELISA, with rapid antibody detection within 10 s. It is noted that normally two or three techniques are combined to improve sensitivity, specificity, and detection time; for instance, microfluidics and paper-based LFA can be combined to improve performance. Among five reviewed antibody tests, LFA and microfluidic-based devices have been commercialized by different companies, whereas FET biosensors and 3D-printed POC chips are newly established with great potential for commercialization.
Comparison of Reviewed COVID-19 Antibody Tests
Estimate cost is based on the approximate cost of the current COVID-19 commercial kits, excluding labor cost and other related consumables.
LFA, lateral flow assay.
As for laboratory-based ELISA, assays are typically only performed by trained personnel of certified companies and require dedicated readout instruments to enable analysis, documentation, data sharing, and storage that limits its POC application. In terms of cost, it seems that 3D printing, LFA, and microfluidics POC may be cheaper than other techniques, which was evidenced by current LFA POC antibody tests on the market.
However, with digital technology advances and development of user-friendly interfaces and usability, smartphones are appealing portable devices to perform multiple analytical tasks with a critical sensor camera, offering high-resolution image capture, and allowing for the ready optical analysis of test strips to record results. Smartphone-associated applications (apps) have been utilized to detect Ebola and SARS-CoV-2 antibodies,31–33 with significantly enhanced accuracy for antibody detection. While only two 3D antibody platform studies herein employed smartphone technology,82,89 the precedent is set for its application as a powerful mobile tool for future immune response monitoring upon disease onset and following vaccinations. The next section highlights the application of mHealth technology in combating the COVID-19 pandemic.
Application of mHealth in COVID-19 Antibody Detection
mHealth provides researchers and health systems with the opportunity to capture and process data in real time and plays an important role in a comprehensive response to infectious disease outbreaks and complementing traditional public health measures.31,34 The use of Bluetooth-enabled smartphone apps to conduct COVID-19 contact tracking is a typical example of applying mHealth concept. 96 Recent systemic reviews conclude that the application of mHealth for COVID-19 management has been utilized for prevention, diagnosis, treatment, and protection via mobile-based apps, automated text messaging, wearable devices, telehealth, and machine learning-based digital epidemiological surveillance.34–38
The current review identified two studies that utilized mHealth in combination with binding antibody tests.82,89 Ali et al employed a smartphone-based user interface to enable readings of SARS-CoV-2 antibody detection from their aerosol-sprayed 3D nano-printed electrode platform. 89 Ditte et al proposed a wearable detection device based on an FET sensor. 82 Although in its infancy, in the context of the COVID-19 antibody response, there is an urgent need to adapt the monitoring, evaluation, and use of mHealth and digital technologies to transform and improve health care systems.
The Application of AM and mHealth in Regenerative Dentistry
Other than detecting COVID-19 immunity, AM (also named 3D printing) and mHealth have emerged as trending regenerative medicine approach in dentistry since craniofacial tissues are organized with unique complex 3D architectures.
Regenerative dentistry involves regenerating functional multicellular complexes that mimic naturally occurring craniofacial structures, and 3D printing technology has opened new horizons for regenerative medicine.97–99 3D printing can facilitate the construction of teeth and tooth supporting apparatus, and the manufacture of biocompatible polymeric implants for promoting dental pulp and tooth germ regeneration.100–102 For example, our research group and other researchers proposed additive-manufactured multiphasic polycaprolactone (PCL) scaffolds (to mimic alveolar bone and periodontal ligament compartments) to promote blood vessel formation and periodontal regeneration in preclinical animal models.103–106
In addition, 3D-printed PCL scaffold has proven to be in a clinical trial in fresh extraction sockets for normal bone healing, with better maintenance of ridge height after 6 months compared with extraction sockets without the scaffold. 107 Our research group also proposed custom-made 3D-printed PCL scaffolds after performing a patient defect scan and implant model creation using CAD. 108 As a new state-of-art 3D printing technique, 3D bioprinting of dental tissues has been proposed as an alternative approach that enables the customized printing of living cells and tissue structures in hydrogel bioink.109–113 The combination of regenerative dentistry and 3D printing can provide great potential in the field of dental regeneration.
However, utilizing mHealth concepts in dental applications (named mobile dentistry [mDentistry]) is relatively limited, although mDentistry can potentially facilitate population-wide oral disease prevention and early detection. mDentistry refers to using mobile devices (such as cell phones, tablets, and personal digital assistants) and wireless infrastructure in dental settings.114–116 Since there is limited research in the field, we speculate that the future of regenerative dentistry may be combining combing 3D printing and mDentistry, such as intraoral cameras, to achieve oral health screening, treatment planning, virtual examinations, and interactive oral health education on a broad population basis.
Conclusion and Future Perspectives
SARS-CoV-2 infection and COVID-19 vaccines trigger immunoglobulin antibody production for protection against viral infection. Antibody detection via various serological tests (Figs. 2 and 3) enables fast and high-throughput identification of active/past infections and host adaptive immunity after vaccinations. Additively manufactured 3D antibody binding platforms may provide increased performance in terms of sensitivity and specificity, with highly functionalized surfaces offering safe, rapid, and accurate immunoassays (Fig. 3). Coupling this emerging technology with mHealth features critical for monitoring an individual's immunity status and evaluating the effectiveness of vaccines is a compelling and necessary step forward.
Despite there currently being limited reports on 3D printing strategies and mHealth for POC antibody tests, available studies demonstrate sensitive and rapid (as short as 11.5 s) antibody detection, providing a significant advantage in the detection and containment of rapidly spreading pathogens. 3D printing is highly versatile and provides advantages of an adaptable design that can be digitally altered and enacted with a relatively minor lag time to the manufacturing floor compared with traditional modes of fabrication.
The 3D-printed immunosensor developed by Muñoz and Pumera proposes many advantages derived from its simplified manufacturing processes, such as cost-effectiveness, rapid prototyping, and the ability to tailor the immunosensor for a specific application. Updated CAD files can be instantly deployed and implemented into production lines globally with minimal expenditure of time and resources. Combined with the streamlined manufacturing steps required for its development and functionalization, AM presents an exciting future for at-point-of-use scenario-specific immunosensors for antigen tests.
Both designs from the Muñoz and Ali teams demonstrate an exciting development for rapid and sensitive COVID-19 antibody detection; however, although promising, the fundamental requirement for serological input does limit their overall efficacy and real-world application. The ever-changing COVID-19 situation, and an increased requirement for incorporating disease status testing into daily life, provide a greater need for immunosensors aimed at reducing or removing the invasive element with high sensitivity at low cost. Nevertheless, the development of 3D-printed immunosensors with high sensitivity utilizing noninvasive biological fluids, such as saliva, would represent a major development in the field and likely represent high commercial interest.
In addition to POC tests, additively manufactured structures (e.g., MEW PCL scaffolds) may provide an alternative option to detect antibody response with a variety of merits: (1) 3D scaffolds have tunable porosity and fiber diameters (ranging from nano- to micrometer scales), (2) MEW scaffolds possess higher surface area for a given footprint, which can be easily functionalized and immobilized with SARS-CoV-2 pathogen protein, and (3) generally the scaffolds are stable at room temperature and exhibit multiple features favorable for packaging and storage. So far, MEW has not been explored for COVID19 antibody detection, and its unique features that result in ordered 3D micrometric fibrous structures with a high surface area could be explored for more sensitive detection of humoral immune responses.
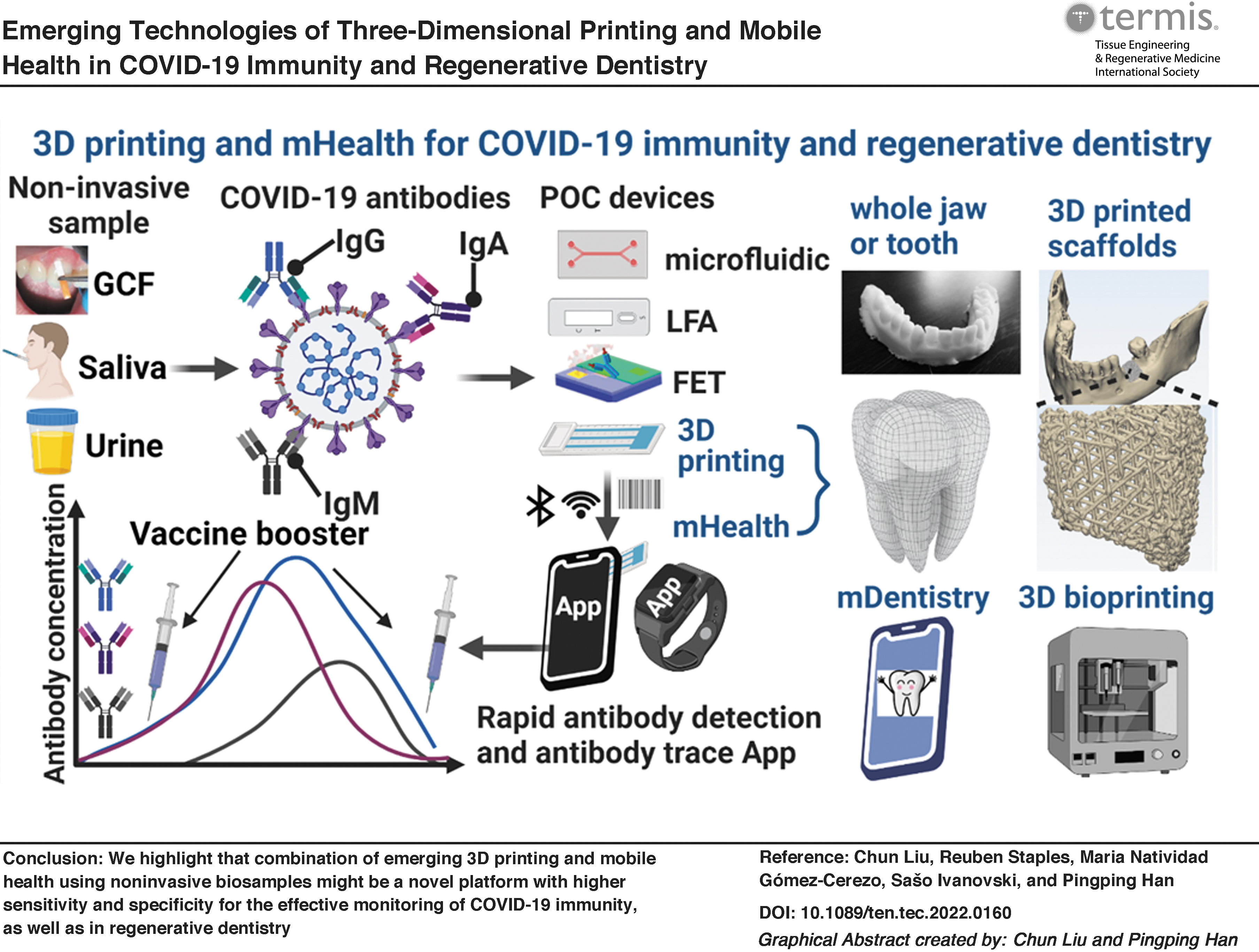
Notwithstanding the limited studies, we proposed a workflow of combining POC devices and mHealth using noninvasive samples for COVID-19 immunity monitoring (Fig. 4). First, noninvasive samples, such as saliva, GCF, and urine, are collected or self-collected to detect immunoglobulin levels (IgG, IgA, and IgM) using POC devices, for example, LFA devices, FET sensors, electrochemical sensors, microfluidic devices, and 3D-printed POC chips with specific barcodes. An individual's immunity results can be rapidly detected in a mobile or smart watch app to facilitate tracing real-time antibody levels.

Proposed workflow of utilizing POC devices and mHealth in noninvasive samples for COVID-19 antibodies detection, as well as in regenerative dentistry. Noninvasive samples such as GCF, saliva, and urine are collected for immunoglobulin (IgG, IgM, and IgA) detection via POC devices, such as LFA, electrochemical sensors, FET, and 3D-printed devices. Results from each assay can be rapidly detected and shared with a mobile phone or smart watch with an application via Bluetooth, Wi-Fi, and specific code. An individual or health department can decide to proceed with a vaccine booster when the traced antibody levels are at low concentrations. Representative examples of using 3D printing and mHealth in regenerative dentistry, such as regenerating whole jaw or tooth, using 3D-printed scaffold for alveolar bone defect, or using mDentistry and 3D bioprinting. GCF, gingival crevicular fluid; mDentistry, mobile dentistry; mHealth, mobile health. Color images are available online.
The tracing app can be monitored by individuals or the health care department. For example, for a vaccinated person, when the antibody concentration reaches a low level, the individual or the health care department can be administrated a vaccine booster. Due to the complexity of antibody tests and varied immune responses among individuals, any POC antibody test needs to be validated before being employed in a large population. Moreover, 3D printing and mDentistry are potential new approaches in regenerative dentistry, with examples of regenerating a whole jaw or tooth, using 3D-printed scaffold for alveolar bone defect, or using mDentistry and 3D bioprinting.
Ideally, multidisciplinary expertise and the emerging technologies of mHealth, wearable devices, and 3D bioprinting31,117–119 could be integrated to improve the performance (sensitivity, specificity, and accuracy) of antibody tests in the detection and monitoring of biological markers. Indeed, with increasing interest in using noninvasive biofluids and rapid POC tests, the combination of technological advancements in AM, biochemistry, materials and polymer science, chemistry, and medicine will facilitate the bench-to-chairside translation of devices critical for the effective management of SARS-CoV-2 infection and COVID-19. In this context, this review provides important insight into the development of 3D-printed antibody tests and the potential application of mHealth for the management of COVID-19. Further investigations on the combination of AM, mHealth, and other advanced technologies using noninvasive biofluids are required to tackle the COVID-19 pandemic with effective immune surveillance and epidemiological assessment at a population level.
Footnotes
Disclosure Statement
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. All authors gave their final approval and agreed to be accountable for all aspects of the work.
Funding Information
This project was supported by the Association for Dental Infection Control (ADIC), the Australasian Osseointegration Society Limited (AOS, Queensland Branch, Brisbane, Australia), and the Australian and New Zealand Academy of Periodontists (ANZAP, Sydney, Australia).