
Abstract
Purpose:
There is still a lack of effective treatments for cartilage damage. Cartilage tissue engineering could be a promising treatment method. Human umbilical cord Wharton's jelly (HUCWJ) and hydrogels have received wide attention as a scaffold for tissue engineering. They have not been widely used in clinical studies as their effectiveness and safety are still controversial. This study systematically compared the ability of these two biological tissue engineering materials to carry chondrocytes to repair cartilage injury in vivo.
Methods:
Chondrocytes were cocultured with HUCWJ or hydrogel for in vivo transplantation. The treatments comprised the HUCWJ+cell, hydrogel+cell, and blank groups. A rabbit model with articular cartilage defect in the knee joint area was established. The defective knee cartilage of different rabbit groups was treated for 3 and 6 months. The efficacy of the various treatments on articular cartilage injury was evaluated by immunohistochemistry and biochemical indices.
Results:
We found that the HUCWJ+cell and hydrogel+cell groups promoted cartilage repair compared with the blank group, which had no repair effect. The treatment efficacy of each group at 6 months was significantly better than that at 3 months. HUCWJ showed accelerated cartilage repair ability than the hydrogel.
Conclusion:
This study showed that HUCWJ is useful in cartilage tissue engineering to enhance the efficacy of chondrocyte-based cartilage repair, providing new insights for regenerative medicine.
Impact statement
Human umbilical cord Wharton's jelly (HUCWJ) and hydrogel are the suitable extracellular matrix for cartilage tissue engineering. This study assessed the capacity of HUCWJ- and hydrogel-loaded chondrocytes to repair cartilage injury in vivo. The data demonstrate that both HUCWJ and hydrogel effectively facilitated cartilage repair, and the repair effects of HUCWJ were significantly better compared with hydrogel, therefore providing a potential candidate for clinical practice of cartilage regeneration therapy.
Introduction
Degenerative lesions and trauma are the major causes of articular cartilage injury.1,2 With this global population aging, the number of articular cartilage damage has increased sharply. If articular cartilage damage is not timely and effectively treated, it will lead to osteoarthritis (OA) and other diseases, which cause great physical pain and financial pressure on patients. 3 This idea is the consensus of experts and is a global problem. Implementing effective treatments in the early stage of articular cartilage injury is crucial to prevent its continued development and reduce the incidence of OA. 4 With the development of science and technology, the improvement of biological tissue engineering materials, related treatment technology, and various methods such as autologous or allogeneic chondrocartilage transplantation have made great progress. 5
Recently, the construction of functional tissue-engineered cartilage to treat cartilage injury has attracted extensive interest.6,7 An acellular extracellular matrix (ECM) has attracted extensive attention because it can preserve bioactive proteins and provide a biomimetic microenvironment for cell attachment, proliferation, and redifferentiation. 8 Extensive in vitro studies have shown the potential of human umbilical cord Wharton's jelly (HUCWJ) in the therapy of cartilage regeneration medicine.9–13 The human umbilical cord contains a gelatinous ECM called HUCWJ, 14 which is similar in composition to the cartilage ECM and comprises large amounts of collagen, hyaluronic acid (HA), and sulfate proteoglycans. In addition, it is rich in growth factors, such as insulin-like growth factor I and transforming growth factor-β, which facilitate the cellular biosynthesis of collagen and glycosaminoglycan (GAG) and promote chondrogenesis. 15 HUCWJ scaffolds prepared by freeze-drying possess uniformly interconnected pore structures with favorable sizes.
The use of HUCWJ scaffold could avoid the uneven distribution of chondrocytes used for the treatment of articular cartilage defects due to the influence of gravity, thus improving the uniform regeneration ability of cartilage. 9 Moreover, human umbilical cords are abundant, easily accessible, and usually discarded as medical waste. Therefore, there will be no ethical barriers to using it. Although HUCWJ presents many advantages as an excellent biomaterial alternative to tissue-engineered cartilage, its therapeutic effect on cartilage regeneration in vivo remains to be investigated.
Hydrogels are hydrophilic polymers composed of 3D mesh scaffolds, which are cheap, easy to make, and environmentally friendly materials. Researchers have synthesized injectable hydrogel formed by glycol chitosan (GCS) and dibenzaldehyde functionalized-polyethylene glycol (DF-PEG), that is, GCS/DF-PEG hydrogel. 16 Due to the dynamic balance between the Schiff base bond and the reactant, GCS/DF-PEG hydrogels display good injectability and self-healing ability and are sensitive to many biochemical stimuli, such as pH, amino acids, and vitamin B6 derivatives. Injectable hydrogels can be gelatinized and injected in situ at the defect site, which offers the advantage of simple operation and minimally invasive injection methods to simplify complex implantation procedures. 17 Their high water content has similar properties to natural extracellular cartilage and is considered a very suitable ECM for tissue engineering. 18 In addition, chitosan can be digested by enzymes such as papain, causing hydrogel degradation. Various cells have been successfully encapsulated in hydrogels, suggesting their potential application value in biomedicine. 16
In previous studies, HUCWJ has been used to generate tissue-engineered cartilage scaffolds in cellular experiments. The HUCWJ scaffold displayed uniformly interconnected pore structures, favorable compressive modulus, water uptake ratio, ECM components' (collagen and GAG) content, and cytocompatibility. 9 The physical properties and cytocompatibility of the GCS/DF-PEG scaffold for the treatment of articular cartilage defects were also studied. The mechanical elastic modulus increased while the cell proliferative ability decreased with the DF-PEG concentration. Overall, 1.5% GCS/4% DF-PEG hydrogel showed feasible porous structure, elastic modulus, degradation rate, and biocompatibility. 19
In the current study, HUCWJ and hydrogel were used as graft scaffolds equipped with rabbit autologous articular chondrocytes to systematically study their ability for cartilage injury repair at the in vivo level. Moreover, the feasibility of HUCWJ and hydrogel loaded with chondrocytes to repair cartilage defects was compared. The results of this study will provide valuable information on the safety and efficacy of HUCWJ and hydrogel combined with chondrocytes in the treatment of cartilage injury, bringing new treatment options for the clinical practice of cartilage regeneration therapy.
Methods
Preparation of the hydrogel
The hydrogel was prepared as described before. 19 Briefly, GCS powder and DF-PEG powder were dissolved by stirring in water to prepare a 1.5% and 4% (mass/vol) concentration and sterilized by filtration with a 0.22 μm filter membrane. A certain volume of sterile GCS solution and an equal volume of sterile DF-PEG solution were mixed to form the GCS/DF-PEG hydrogel.
Preparation of HUCWJ
The HUCWJ was prepared by decellularization and conventional freeze-drying process for fabricating scaffolds, as described before.9,20 Briefly, the human umbilical cord was immersed in an aqueous acid electrolyte oxide solution (EOW, pH = 2.5) for 10 min and repeated three times for umbilical cord decellularization. The umbilical cord was cut open with scissors under aseptic conditions. The vascular and adventitial tissue were dissected with forceps, rinsed with sterile water, soaked in 3% hydrogen peroxide for 30 min, and then rinsed with phosphate-buffered saline. The tissue was crushed in a Jianyang chef machine. Then 2 × volume of precooled sterile ultrapure water was added at a low temperature (4°C), and the tissue was ground for 10 min. The process was repeated three times.
Precooled sterile ultrapure water was added to a glue solution (glue:water = 1:10) and mixed thoroughly. The Wharton's glue homogenate was frozen in the −20°C refrigerator and then thawed at room temperature. After three or four times of freezing and thawing, the cell membrane was finally broken. The freeze-thawed homogenate was centrifuged (2000 rpm, 20 min). Cell digestion solution (1% Triton X-100, 0.25% trypsin, 1 mM Tris-HCL pH = 7.0) was added to the supernatant and placed at 4°C for 24 h. The solution was centrifuged at 3000 rpm for 20 min. DNase and RNase were added to the supernatant and digested at 37°C for 12 h. The supernatant was centrifuged at 4°C (speed = 6000 rpm, 15–20 min) to remove cell fragments, nucleic acids, and other residual substances in the colloid. The pH of the colloid solution was adjusted to 7.0. After washing and precipitation (4°C, 12 h), the upper liquid was centrifuged at high speed at low temperature (speed = 10,000 rpm, 40 min). The supernatant was discarded, and the prepared nano-scale Wharton's glue was carefully collected.
Cell culture
Before the experiment, the rabbits were subjected to fasting and water deprivation for more than 6 h. After anesthesia and surgical operation, the joint was fully exposed. The cartilage tissue was carefully scraped with a knife and placed into a container with the culture medium. D-hank's solution was used to wash off the blood stains attached to the surface of the tissue, and the cartilage tissue was cut into fragments of about 1 × 3 mm pieces. Then 0.2% collagenase type II was added, and the tissue was placed in an incubator at 37°C and digested for about 1 h with stirring. Digestion was complete when no obvious tissue block was observed, and the solution became cloudy. The digestion was terminated by centrifugation (1500 rpm, 5 min) to remove the collagenase type II. The cell precipitates were washed with D-hank's solution and cell culture medium, respectively, to fully remove collagenase type II. The cell suspension was placed in cell culture flasks and incubated with 5% CO2 at 37°C.
After 12–16 h of culture and when 70% or more cells adhered to the wall, D-hank's balance buffer was used to wash and remove impurities and nonadherent cells. The culturing of the cells was continued, and the culture solution was changed every 2 days. When the confluence rate of the primary cells reached about 80%, the cells were subcultured and digested with 0.25% trypsin for about 3–5 min. When the cells became round and bright, serum medium was added immediately to terminate the trypsin digestion. The cells were evenly divided into two new culture flasks at a ratio of 1:2.
Preparation of cell-laden HUCWJ
Primary articular chondrocytes within three generations were digested with 0.25% trypsin, and the cell density was adjusted to 1 × 107 cells/mL. Sterile 1 mm (thick) × 4 mm (diameter) HUCWJ scaffolds were placed in a cell culture dish. The cell suspension was slowly and evenly added to the orientated scaffold material until the scaffold material was evenly and fully soaked with liquid. Each scaffold required 20 μL of cell suspension (containing 2 × 105 cells). The scaffolds and cell suspension were placed in a conventional cell incubator for about 4 h to allow the cells to adhere to the scaffolds. After that, 2 mL of cell culture medium (Dulbecco's modified Eagle's medium containing 10% fetal bovine serum [FBS]) was slowly added to the culture plate and incubated. The liquid was changed every 2 days and observed under the microscope daily.
Preparation of cell-laden hydrogel
GCS solution at 3% mass concentration and DF-PEG solution at 4% mass concentration were prepared by solubilization in a cell medium containing 10% FBS. The suspension of articular chondrocytes within three generations was prepared at a concentration of 1 × 107 cells/mL. The 3% GCS solution was mixed with the cell suspension in a 1:1 ratio. Exactly 150 μL of 1.5% GCS-cell suspension (5 × 106 cells/mL) was mixed with 4% DF-PEG solution at a ratio of 1:1, then added to a 48-well plate and left to stand for 2 h to solidify into gelatin. Exactly 300 μL of cell culture medium was added to each well and cultured in a cell culture incubator (37°C, 5% CO2). The culture medium was changed every 2 days. The general morphology of chondrocytes in the hydrogel was observed under a microscope.
Implantation of the complex for cartilage regeneration
The animal experiment was approved by the Animal Ethics and Welfare Committee of Longgang District People's Hospital of Shenzhen (Shenzhen, China) and was performed according to the guidelines of Biomedical and Animal Ethics Committee. Thirty adults, healthy New Zealand white rabbits weighing 2.5–3.0 kg were purchased from the Medical Laboratory Animal Center of the PLA General Hospital. The thirty rabbits were randomly divided into three groups, with 10 knees (bilateral knees) in each group. The repair effect was evaluated at 3 and 6 months after surgery. The animals were anesthetized by intramuscular injection of 0.5 mL/kg ketamine and imbrium II (1:1V/V) and were placed with the abdomen facing the operating table after general anesthesia. The knee joint was straightened, and an incision of about 2 cm was made ∼1.0 cm inside the patella. The patella was dislocated laterally, and the trochlear groove of the patella was exposed by bending the knee. A full-thickness cartilage defect of ∼1.2 mm depth was made in the trochlear groove. The cartilage debris was removed with a curette to smooth the damaged area.
The 3-day in vitro cultured cell–scaffold complex was transplanted to the site of joint injury so that the plane's height into the complex was the same as that of the adjacent cartilage. Then the patella was repositioned, and the joint capsule, muscle layer, fascia layer, and skin were sutured sequentially and disinfected with iodophor and alcohol. When the animals awakened, they were placed in a cage and fed. After the surgery, 800,000 U/day penicillin was injected intramuscularly for 3 days to prevent infection.
Observation of joint tissue morphology
The gross assessment included the level of repair of the injured edge and the status of the injured cartilage surface, the transparency of the new cartilage, and the degree of filling in the defect. From a score of 0–8, the higher the score, the better the repair state (Table 1).
Scoring Criteria for Cartilage Repair
Histological evaluation of cartilage repair
Fresh specimens were fixed in 4% paraformaldehyde solution and then decalcified with 10% ethylenediaminetetraacetic acid decalcification solution. This solution was changed every fourth day. After decalcification, the samples were dehydrated in an alcohol gradient series. The specimen was embedded in paraffin wax and sectioned with a thickness of 5 μm. The sections were stained with hematoxylin-eosin (HE), Toluidine Blue, Safranin “O” chemical staining, and type II collagen staining. The staining results were used to judge the histological status changes of cartilage repair.
The histologic grading index includes several aspects: cellular composition and heterochromatic cartilage repair area, the flatness of tissue surface after repair injury, the thickness of healthy cartilage, the degree of integration of new tissue, and healthy cartilage contact site. The score ranges from 0 to 14 points, with a lower score indicating better repair ability and a better state after repair (Table 2).
Reference Standard for Evaluation of Wakitani Score Histology
Quantitative GAG detection of newly generated tissues
Three joints of each group were observed and measured at 3 and 6 months after the operation. The tissue in the repair area of the joint was removed using an ophthalmic trephine (4 mm in diameter) and a small bladed knife. The tissue was placed in an eppendorf tube, and the cartilage was cut into pieces with ophthalmic scissors (trumps). At the same time, three healthy cartilage tissues of similar size were obtained as controls. The fresh cartilage tissue was immediately freeze dried for 3 days. The weight of the completely dried cartilage tissue was weighed and called “dry weight.” A sample of about 1 mg dry weight was lysed with 1 mL of tissue lysate for 1 to 3 days. The impurities were removed by centrifugation (10,000 rpm, 10 min). Exactly 3 mL dimethyl methylene blue color solution was added to 100 μL of the supernatant, mixed, and then run on the machine. The absorbance value of each sample was converted into GAG content according to a standard curve and expressed as GAG/dry weight.
Determination of hydroxyproline in repair tissues
Hydroxyproline concentration is determined by the reaction of oxidized hydroxyproline with 4-(dimethylamino)benzaldehyde, which results in a colorimetric (560 nm) product proportional to the hydroxyproline present. The linear range of detection for this assay is between 0.2 and 1.0 μg.
Biochemical detection of repair tissues
Three fresh specimens were collected from each group. The base and sides of the femoral condyle were polished, and the bottom was glued to the cell culture dish, exposing the surface of the new tissue on top. The samples were fixed on the BOSE5100 mechanical measuring machine, and the surface of the regenerated tissue was perpendicular to the vector direction of the biomechanical loading force. The maximum pressure of 20 N was applied, and the pressure depth was set at 0.3 mm at a speed of 0.001 mm/s. The load–displacement curve was detected using a 1.5 mm Kirschner wire probe. The linear formula and its slope are obtained by aiming at the linear part of the load–displacement curve. The stiffness of the tissue (k = P/δ) is obtained where P represents the force on the tissue surface, and δ represents the deformation coefficient of the regenerated tissue under compression.
Statistical analysis
Statistical analysis was performed with SPSS 17.0 statistical software, and data within groups are presented as
Results
Observation of joint tissue morphology
Three months after surgery, the surface of the injured site in the blank group was significantly lower than the surface of the surrounding healthy cartilage and showed a pitted appearance. No obvious repair trace was observed on the injured site. Even if there was a little regenerated tissue, the surface was uneven, did not form an effective filling, the degree of integration with normal tissue was poor, and there was still a large area of defect (Figs. 1A and 2A). After the sixth month of surgery, there was a small amount of defective surface in the center of the regeneration site without tissue filling, with an uneven surface and poor fusion (Figs. 1B and 2B). However, the defect area and depth were reduced compared with that at 3 months (Figs. 1B and 2B).
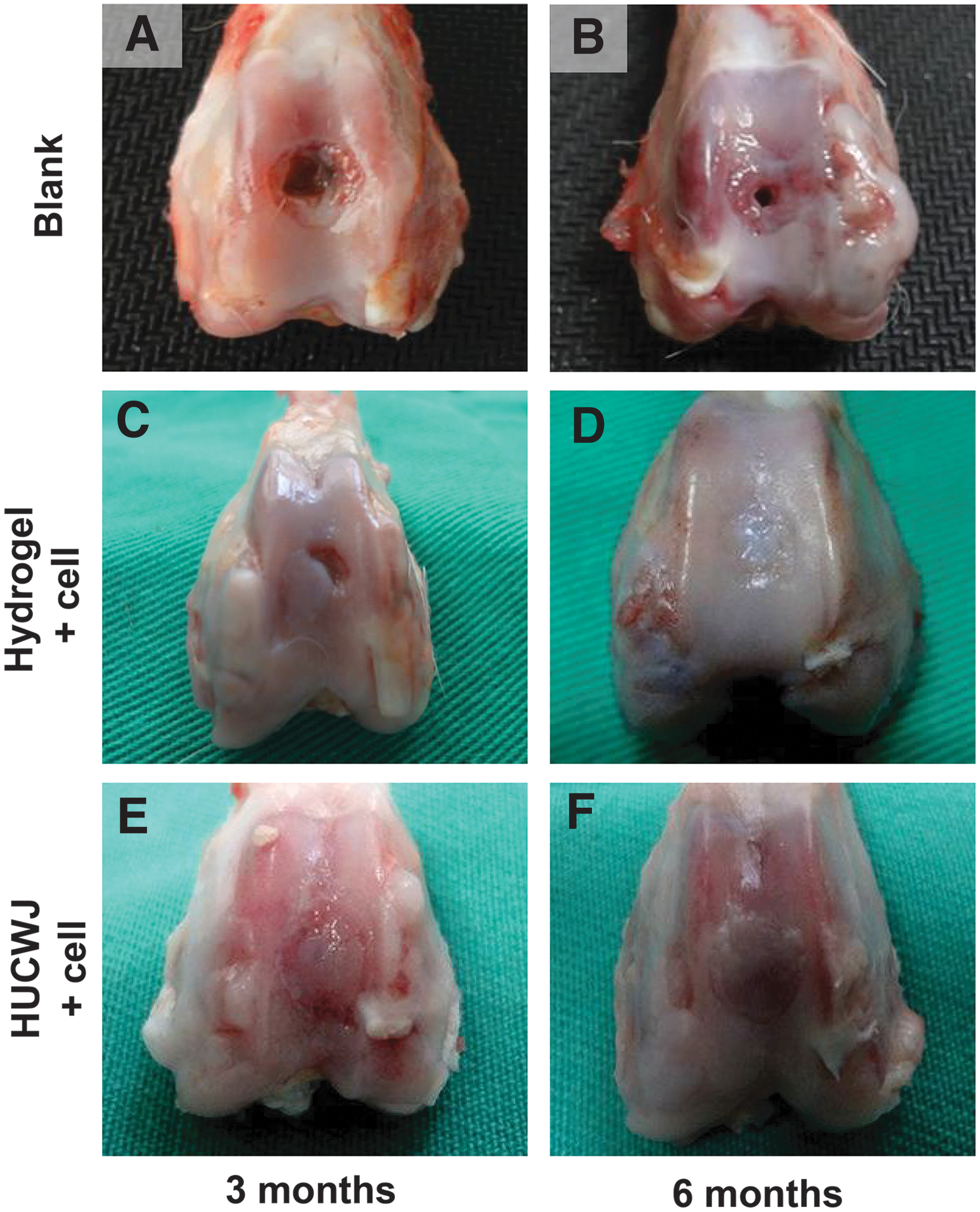
Cartilage repair status after the surgery at 3 and 6 months.
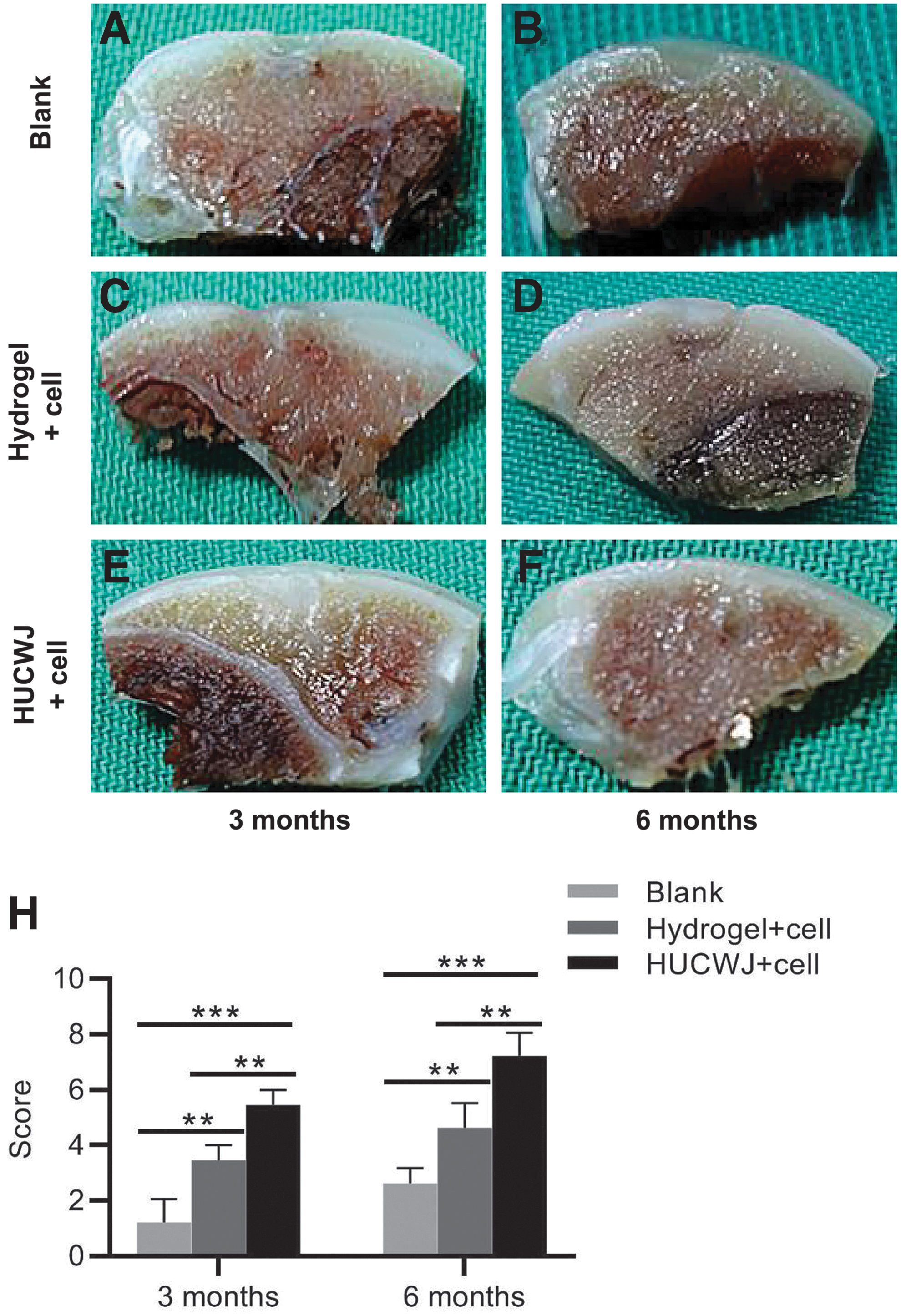
Joint profile view at 3 and 6 months after the operation.
Most of the defect area in the hydrogel compound autologous chondrocyte group was filled 3 months after surgery, and the repair effect was significantly better than that in the blank group at the same time point. Although the surface was not smooth, there were unfilled areas in the center or edge, and the repair area was white, yellow, and opaque (Fig. 1C). The profile observation showed ladder depressions in the junction area, and the degree of fusion was poor (Fig. 2C). After 6 months, the overall repair level of the repaired area was better than that after 3 months. The surface of the repaired area was flat and smooth, and the regenerated tissue was fused with the surrounding healthy cartilage. However, incomplete cracks and injuries were still observed in the center of the damaged and repaired area (Fig. 1D). Six months after the operation, the repaired tissue showed that the new tissue could fill the damaged site, and the tissue smoothness and continuity were much better than those at 3 months. However, the surface of the repaired area remained uneven to a certain extent and included some cracks and injuries (Fig. 2D).
Three months after surgery, the Wharton's plastic stent group's cartilage was filled with a large amount of tissue that appeared smooth, transparent, and flat. No obvious boundary existed between the new tissue and the adjacent healthy cartilage. The new and old cartilage levels were the same, with the new tissue appearing transparent (Fig. 1E) with many hyaline cartilage cells. The regenerated tissue was relatively flat, smooth, and continuous. The damaged area was filled, the degree of fusion of the damaged junction was relatively high, and the newly restored area was transparent (Fig. 2E).
Six months after the surgery, the appearance of the new and damaged cartilage was very similar to the adjacent healthy cartilage. It was transparent and flat with a smooth surface. The injury was fully populated with a new organization; the new cartilage surface was smooth and continuous, with good fusion with the adjacent normal cartilage (Fig. 1F). The tissue profile observation showed that the injured site was filled; the regenerated repair tissue was well integrated with the adjacent healthy cartilage. The regenerated cartilage's transparency, smoothness, and color were indistinguishable from the adjacent healthy tissue (Fig. 2F).
Significant differences in cartilage repair levels were found between each group at the same time point (3 and 6 months). The repair effect of the HUCWJ+cell group was the best, followed by the autologous chondrocytes+hydrogel group. The repair effect of both groups was significantly better compared with the blank control group. The repair effect of the cartilage injury after 6 months was better than that after 3 months for each treatment group (Fig. 2H).
Histological observation
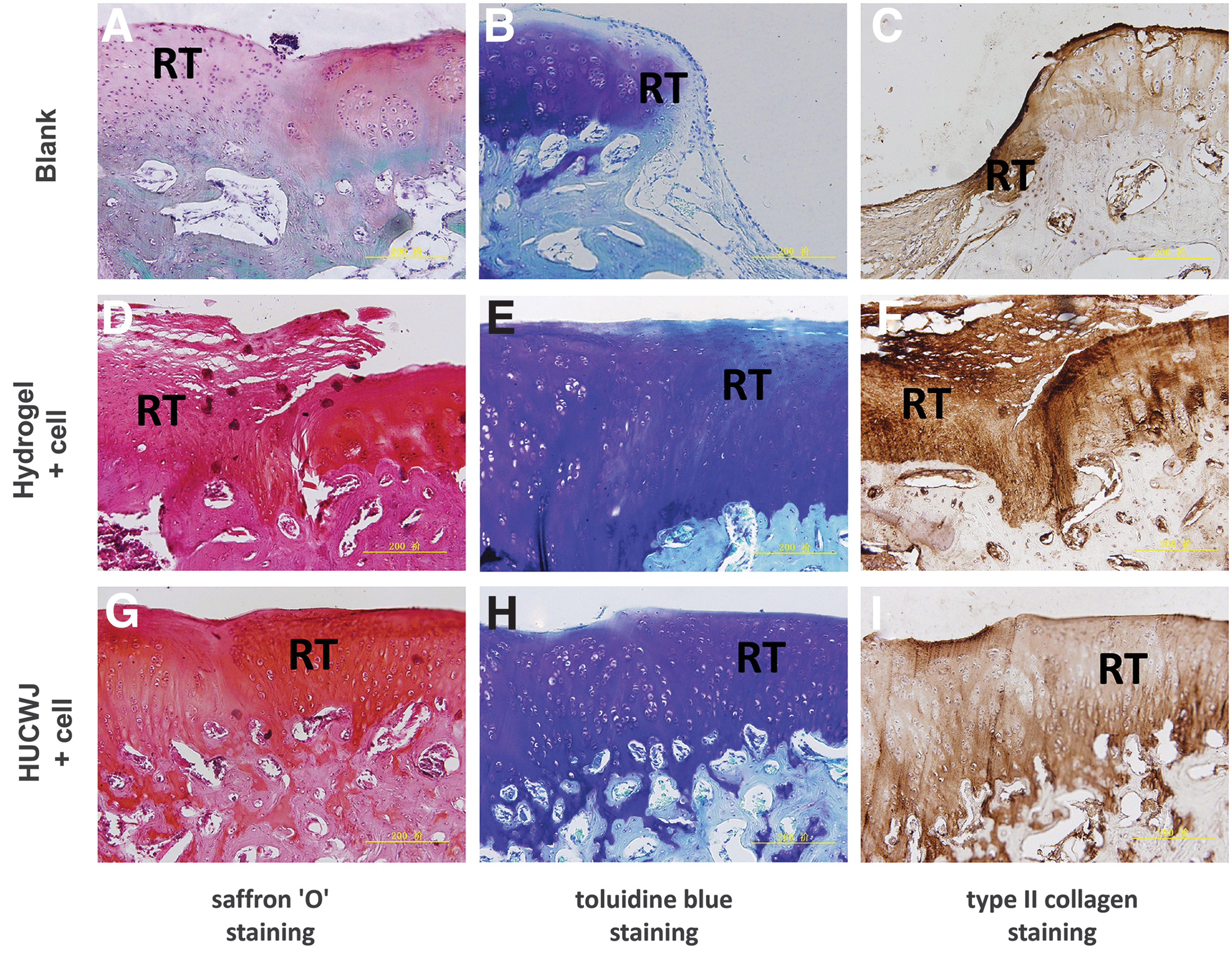
In the third month after the operation, the injured site in the blank control group showed nonstained tissues after HE (Fig. 3A), Oil Red O (Fig. 4A), Toluidine Blue (Fig. 4B), and collagen type II staining (Fig. 4C). In the sixth month after the operation, a thinner new cartilage appeared with a central depression and a small number of new cartilage cells. The rest were fibrous tissue cells. HE (Fig. 3B), Safranin “O” (Fig. 5A), Toluidine Blue (Fig. 5B), and collagen type II staining (Fig. 5C) showed little metachromatic organization with poor alignment.
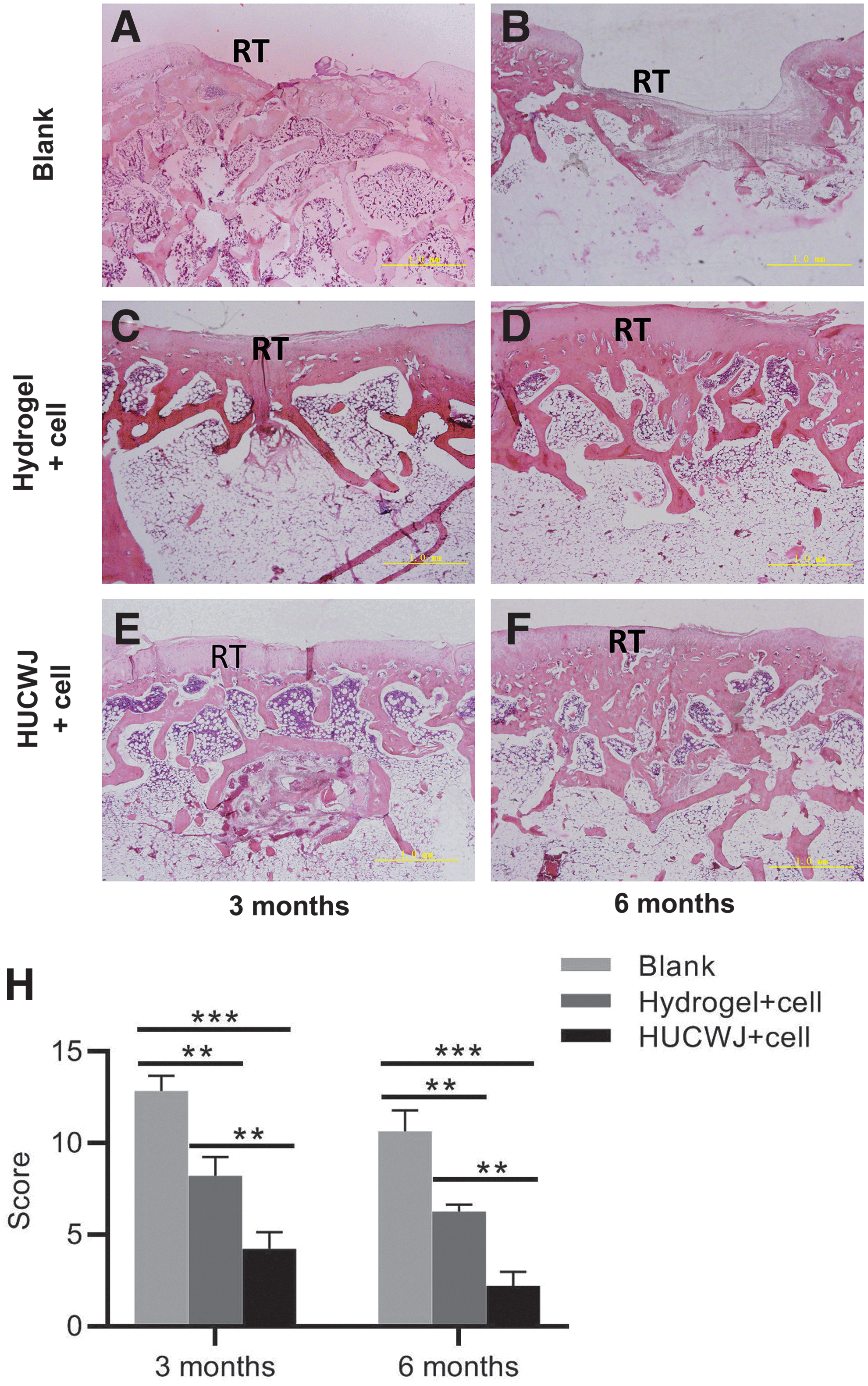
HE staining of repair site at 3 and 6 months after operation.
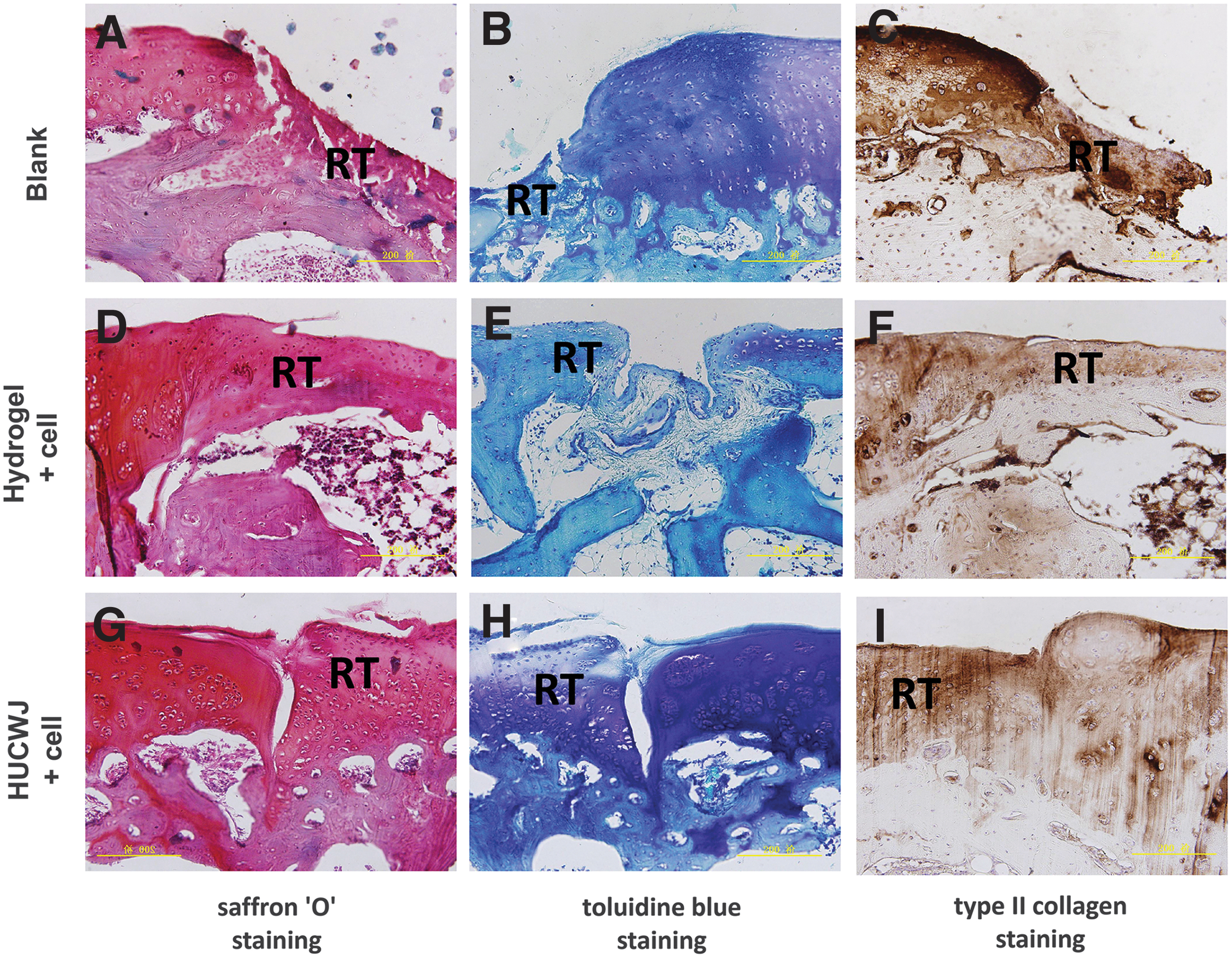
Staining for junction and restoration areas of repair site at 3 months after operation.
Staining for junction and restoration areas of repair site at 6 months after operation.
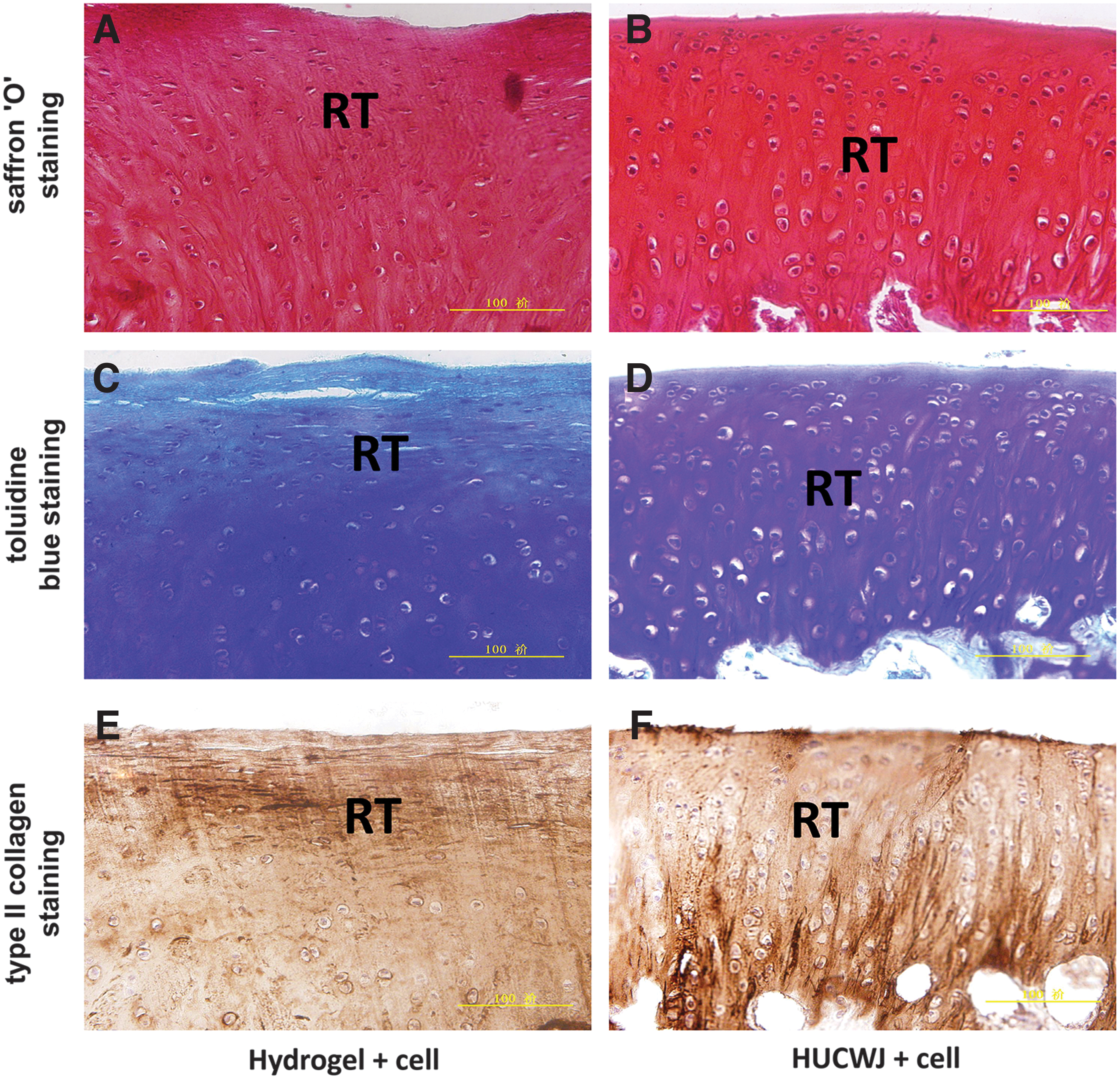
In the hydrogel autologous chondrocyte group, HE (Fig. 3C), Safranin “O” (Figs. 4D and 6A), Toluidine Blue (Figs. 4E and 6C), and collagen type II staining (Figs. 4F and 6E) showed that the regenerated tissue was filled with many fibrochondrocytes 3 months after the operation. Six months after surgery, the new cartilage was thinner than the normal cartilage, and the HE staining showed that the matrix signal was weak (Fig. 3D). Most of the regenerated tissue was composed of fibrochondrocytes, and only a few hyaline chondrocytes existed at the junction of the adjacent healthy cartilage (Figs. 5D–F, 7A, 7C, and 7E).

Staining for repair area at 3 months after operation.
Staining for repair area at 6 months after operation.
In the stent group + cartilage cells, the new tissue was only 50% as thick as the adjacent healthy cartilage after 3 months. The regenerated cartilage's surface was transparent with many hyaline cartilage cells. HE staining showed that the matrix was metachromatic deep, and the repair and transition area was aligned with the adjacent normal cartilage (Fig. 3E). The deep chondrocytes of the new tissue were columnar and not ossified (Figs. 4G–I, 6B, 6D, and 6F). At 6 months after the operation, the cartilage surface of newly generated tissue was smooth, and the thickness was not enough (Fig. 3F, HE staining). There were hyaline cartilage cells, which are significantly metachromatic in the repair area. The chondrocytes were columnar, with a few chondrocytes in the marginal zone. The weak color showed subchondral ossification (Figs. 5G–I, 7B, 7D, and 7F).
Statistical analysis showed that there were significant differences between groups at the same time point. The cartilage repair effect of the HUCWJ group was better compared with the hydrogel group, and the repair effect of the two groups was significantly better compared with the blank control group. At the same time, it can be seen that the repair effect of cartilage injury after 6 months is better than that after 3 months with the same treatment (Fig. 4H).
Analysis of GAG content in newly generated tissue from the damaged site
The GAG content in the HUCWJ and hydrogel group at 3 and 6 months after the operation accounted for 57.0%, 29.6%, 80.9%, and 44.7% of normal cartilage tissue, respectively. Comparing the GAG content in the new cartilage tissue of each group showed that the repair effect of the cartilage defect in the HUCWJ group was better than that in the hydrogel group at the same repair time. The longer the repair time, the better the repair effect (Fig. 8A).

Assessment of biochemical indices in newly generated cartilage tissue at 3 and 6 months after surgery.
Quantitative assessment of hydroxyproline in newly generated cartilage tissue
The hydroxyproline content in the new cartilage of the stent and the hydrogel groups at 3 and 6 months after the operation were measured. The results showed that they accounted for 58.8%, 45.85%, 79.08%, and 55.3% of the normal cartilage tissue. The statistical analysis showed that the hydroxyproline content of each group was significantly different under the same repair time. The treatment effect of the HUCWJ group on cartilage defect regeneration is better compared with the hydrogel group. Under the same treatment, the longer the repair time, the more similar the hydroxyproline content in the newly repaired tissue to that of normal cartilage (Fig. 8B).
Biomechanical evaluation of cartilage defect after repair
The tissue stiffness evaluation of the repair site showed that the stiffness of the HUCWJ and the hydrogel+chondrocyte groups at 3 and 6 months after surgery could reach 45.7%, 25.3%, 69.8%, and 35.1% of the stiffness of the healthy cartilage, respectively. Statistical analysis showed that there were significant differences among groups at the same time point. At the same repair period, the tissue stiffness of the HUCWJ+cell group was higher compared with the hydrogel+cell group. The longer the repair time in the same treatment, the better the biomechanics of the new cartilage and the closer it is to the normal cartilage tissue (Fig. 8C).
Discussion
Cartilage tissue engineering is a cutting-edge technology that has emerged recently, opening up a new field for treating cartilage injuries.17–19 As the core element of cartilage tissue engineering, the development and research of scaffold materials are gradually being optimized. The raw materials for scaffold preparation mainly include natural and synthetic polymer materials. Synthetic polymer materials include poly-glycolic acid and its copolymer, polylactic acid, etc. The advantages of these materials mainly include large-scale production, small structure, and artificially controllable material strength and degradation degree. However, these engineering materials generally showed poor biocompatibility and specific immunogenicity. The lack of a cell signal recognition system and poor adhesion with body cells are not conducive to the attachment and proliferation of chondrocytes on scaffolds prepared by such materials. The acidic nature of its degradation products can also hinder the growth and proliferation of implanted chondrocytes. 21 Another category of raw materials is natural biomaterials, mainly used in chondrocyte ECM, type I collagen, type II collagen, chitosan, HA, etc.
Its advantage lies in its good biocompatibility, which is conducive to the adhesion and proliferation of planted cells. 22 The synthesized scaffold can simulate the physiological microenvironment of chondrocyte growth. In addition, its degradation products are easily metabolized and cleared, with low toxicity and a low risk of inflammation. The neonatal umbilical cord is rich in GAGs and collagen, similar to the cartilage tissue composition. Therefore, Wharton's glue extracted from the umbilical cord is an ideal scaffold material for cartilage tissue engineering.
The overall observation of the repaired tissue in this study showed depressions in the blank injury area in the control group in the third month after the operation, and the shape of the injury site was similar to that during the surgery. At 6 months after surgery, there was a large area of unfilled tissue in the center of the injured area, and only a small amount of repaired cartilage tissue was still very different from the adjacent normal cartilage.
In the hydrogel combined with autologous chondrocyte group, most of the injured area had been filled in the third month after surgery, and the repair level of the newly generated cartilage tissue was higher compared with the control group during the same period. The freshly generated cartilage tissue in the repaired area was white and opaque. Compared with the third month after surgery, the overall level of the damaged repair area was significantly better. Specifically, the surface of the new tissue was relatively flat, but there were still incomplete cracks in the center of the damaged repair area, and the transparency of the tissue surface was not satisfactory. It is suggested that hydrogel combined with autologous chondrocytes has a certain repair ability, but this is not enough to completely repair the cartilage injury.
Three months after the surgery in the autologous chondrocytes' composite oriented stent group, the damaged area is filled, and the appearance of the new tissue is more transparent and smoother. The new tissue in the damaged region and the surrounding normal cartilage was fused with a blurred junction appearing smooth and continuous. The new repair cartilage seems transparent. At 6 months after the operation, the appearance and health of the new tissue in the damaged region are similar to normal cartilage. The cartilage was transparent and smooth, and the damaged area was fully populated with cells. The freshly repaired cartilage and the adjacent junction were continuous and smooth. The results were satisfactory, and the new deep cartilage had a columnar orientation. The structural regeneration of articular cartilage was observed. Perhaps the structural and functional properties of Wharton's glue promoted the direction of the chondrocytes and secretory matrix. Our research showed that the HUCWJ+cell group produced the best repair effect.
The biomechanical properties of cartilage tissue are reflected in the integrity of its biochemical composition, morphological structure, and tissue morphology.23–25 This is consistent with the physiological characteristics of cartilage tissue. It does not contain blood vessels, nerves, or lymph; its supporting units are mainly proteoglycans and type II collagen. 24 The high osmotic pressure of the proteoglycans causes a large amount of water to fill the cartilage tissue and produce liquid pressure, thus playing the role of resistance to stress. Proteoglycans fill cartilage with water-storage molecules, especially GAGs.26,27 The fluid pressure generated in the cartilage matrix can effectively maintain the stress exerted on it. The key to cartilage pressure is the content of GAG in cartilage. The interaction between the highly negatively charged cartilage proteoglycans and type II collagen provides the compressive and tensile strength of the tissue. The stiffness of cartilage is positively correlated with its GAG content.28–31 The higher the GAG content, the greater the stiffness and the stronger the antipressure effect.
Chondrocyte rupture caused by cartilage injury leads to the loss of GAG, decreasing cartilage stiffness, and weakening the antipressure effect. Our experimental results proved that the mechanical strength of the HUCWJ group was higher compared with the hydrogel group, and the mechanical strength of each group was positively correlated with the repair time. The mechanical strength of the newly repaired tissue was close to the overall change trend of GAG expression level in the tissue. The structure of the recently restored tissue of the HUCWJ+cell group showed orientation after 6 months, and the mechanical strength of the tissue was good and closest to the mechanical strength of normal cartilage tissue.
Other bioactive components, such as platelet-rich plasma (PRP) and platelet-rich fibrin (PRF), which are the concentration of autologous growth factors to stimulate tissue regeneration, have been wildly used in regenerative dentistry. Recently, PRP and PRF displayed therapeutic potential to support cartilage repair. Injectable PRF significantly increased chondrocyte proliferation and presented better cartilage regeneration ability than PRP in the defective knee of the rabbit model. 32 Leukocyte PRP (L-PRP) and leukocyte PRF (L-PRF) was proven to effectively enhance the healing of cartilage injuries in the dog knee. 33 L-PRP or L-PRF delivered with a HA scaffold effectively improved cartilage healing in the bovine model. L-PRF was not superior to L-PRP, as the L-PRP group had better collagen content, while L-PRF showed higher GAG production. 34 Many clinical studies have proven the obvious safety and efficacy of PRP and PRF in cartilage defects, although the evaluation criteria need to be standardized.35,36
PRP and PRF-based therapies have shown favorable results in the treatment of cartilage regeneration. However, how to combine PRP/PRF, chondrocytes and appropriate scaffolds to repair cartilage injury and their therapeutic effect remain to be investigated further.
Conclusion
In this study, we compared the ability of the HUCWJ and hydrogel-loaded chondrocytes to repair cartilage injury. The results showed that both had repair effects compared with the blank control group. The repair effect of the HUCWJ group was better compared with the hydrogel group. The therapeutic effect was significantly better at 6 than 3 months after the operation with the same treatment method.
Availability of Data
All data are available from the corresponding author on reasonable request.
Footnotes
Acknowledgments
The authors would like to thank Xinhang Yao for his suggestions and for providing some of the reagents. They would like to thank Editage for English language editing. They also thank Mrs. Lei Zhang for her assistance.
Authors' Contributions
J.Y., Q.G., and J.L. designed the experiments; J.Y., Y.Z., C.G., and X.L. performed the experiments; J.Y., X.J. and F.L. analyzed the data; H.Z., Y.H., and R.G. contributed to data interpretation and article revising; Q.G. and J.L. wrote the article. All authors read and approved the final article.
Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
This work was granted by the Shenzhen Municipal Natural Science Foundation of China (JCYJ20220530162206012).