
Abstract
Considerable research is being undertaken to develop novel biomaterials-based approaches for surgical reconstruction of bone defects. This extends to three-dimensional (3D) printed materials that provide stable, structural, and functional support in vivo. However, few preclinical models can simulate in vivo human biological conditions for clinically relevant testing. In this study we describe a novel ovine model that allows evaluation of in vivo osteogenesis via contact with bone and/or periosteum interfaced with printed polymer bioreactors loaded with biomaterial bone substitutes. The infraspinous scapular region of 14 Dorset cross sheep was exposed. Vascularized periosteum was elevated either attached to the infraspinatus muscle or separately. In both cases, the periosteum was supplied by the periosteal branch of the circumflex scapular vessels. In eight sheep, a 3D printed 4-chambered polyetheretherketone bioreactor was wrapped circumferentially in vascularized periosteum. In 6 sheep, 12 double-sided 3D printed 2-chambered polyetherketone bioreactors were secured to the underlying bone allowing direct contact with the bone on one side and periosteum on the other. Our model enabled simultaneous testing of up to 24 (12 double-sided) 10 × 10 × 5 mm bioreactors per scapula in the flat contact approach or a single 40 × 10 mm four-chambered bioreactor per scapula using the periosteal wrap. De novo bone growth was evaluated using histological and radiological analysis. Of importance, the experimental model was well tolerated by the animals and provides a versatile approach for comparing the osteogenic potential of cambium on the bone surface and elevated with periosteum. Furthermore, the periosteal flaps were sufficiently large for encasing bioreactors containing biomaterial bone substitutes for applications such as segmental mandibular reconstruction.
Impact statement
Adequately powered preclinical testing is needed to determine the capacity of biomaterials to support osseointegration, osteoinduction, and osteoconduction. Our novel sheep model uses advanced 3D printed polymer bioreactors and the inherent osteogenic properties of periosteum to assist de novo bone growth in vivo. Leveraging the large surface area of the infraspinous region of the scapula, periosteum can be surgically raised and wrapped circumferentially around the printed bioreactors or provide dual contact with periosteum and underlying native bone simultaneously. Finally, the versatile model of osteogenesis allows many bioreactors to be implanted while minimizing the number of animals required for experimentation.
Introduction
Biomaterials-guided bone regeneration (BGBR) is of increasing interest to surgeons and engineers aiming to heal critical-sized skeletal defects. Three-dimensional (3D) printed materials can provide mechanical strength during defect healing with optimized pore geometries and chemical stimulation of osteogenesis. 1 BGBR is already being used clinically in the reconstruction of small bone defects such as alveolar ridge augmentation in dentistry. 2 However, translation of this technology to critical-sized defects, that is, those which cannot naturally heal, has been incumbered by a lack of materials with coincident biocompatibility and mechanical strength, the need for expensive exogenous growth factors, such as recombinant bone morphogenic protein,3,4 and clinically relevant models for evaluation. Nonetheless, BGBR holds great potential as a method to replace autologous bone grafts and osseous free flaps (the current gold standard for large maxillomandibular defects), which can be highly morbid, expensive, and inaccessible to many.5–10
Material scientists continue to develop novel polymer-, ceramic-, and metal-based implants for bone repair.11–13 However, before such implants can be translated to patients, they must undergo appropriate preclinical testing, including in large animal models. The models should replicate the defect site and native tissue response, ideally without requiring exogenous growth factors 14 or follow-up surgery for implant adjustment or removal.
Osteoinduction, osteoconduction, and osseointegration underpin BGBR. 15 Osteoinduction occurs to help bone heal and remodel following injury whereby mesenchymal stem cells are triggered by local chemical and mechanical messengers to promote fracture healing. 16 Furthermore, osteoinduction can be facilitated by periosteum, which harbors a significant bone progenitor cell population. 17 For this reason, periosteal flaps are used clinically to help repair necrotic mandibular bone. 18 However, the osteogenic potential of periosteum can differ between anatomical sites and decreases with age. 19 That is to say, the proliferation and differentiation of osteoblasts is greater in younger animals compared with older ones.
In biomaterials science, osteoconduction refers to the complex processes involved in bone formation on the surface of an implant including the proliferation of supporting cells.20,21 Adequate blood supply is a prerequisite for osteoconduction and depends on the properties of material used, such as structure and surface topology. Investigating this osteoconductive capacity is the focus of much research in biomaterial science and a relevant application for the ovine model presented in this article. Osseointegration refers to the direct contact of living bone on an implant surface for biomechanical anchorage. 22 Histologically, a completely osseointegrated implant will not demonstrate any fibrous tissue growth at the bone-implant interface, 20 and is a necessary requirement for maxillomandibular endosteal implants to sustain mechanical loading over many years.
Sheep have similar skeletal anatomy to humans, display comparable bone turnover rates when older, and can be housed easier than most other large animals. 23 Although previous ovine models have been used to cover small bone implants using rib periosteum, this is difficult to translate in humans because of the small surface area available.3,24 More recently, the tibial corticoperiosteal flap has been used with a bone scaffold, but the cortical portion of the flap is not malleable and therefore is less suited to irregular-shaped defects encountered in maxillofacial surgery. 1 Here, we describe the use of periosteum from the infraspinous region of the scapula in older sheep for assessing bone substitutes in vivo that are contained within advanced 3D printed polymer bioreactors and without exogenous growth factors. Two novel periosteal flap designs are presented for wrapping or flat contact with the bioreactors.
Methods
Ethics approval was obtained from The University of Sydney Animal Research Ethics Committee (2020/1817 & 2021/2004).
Cadaveric study
Three thoracic limbs from skeletally mature Dorset cross sheep (Ovis aries) cadavers were examined to define the anatomical boundaries and blood supply to the infraspinous region of the scapula. The sheep scapula has the same bony landmarks as the human scapula as given in Figure 1, with the addition of a large cartilaginous border that extends across its length dorsally and caudally. The infraspinatus muscle arises from the infraspinous fossa and scapular spine, inserting onto the greater tubercle of the humerus. The teres major muscle arises from the caudal angle of the scapula and inserts into the greater tubercle of the humerus. 25 Periosteum in this region can be separated from the underlying cortical bone with relative ease in younger sheep but is more challenging when older (Fig. 2). It is also more difficult to elevate closer to the glenoid fossa, where it tends to fragment. Blood supply is via branches of the subscapular artery, predominantly through the circumflex scapular artery, which supplies perforating branches to the border of the scapula and muscular branches to teres major and infraspinatus.
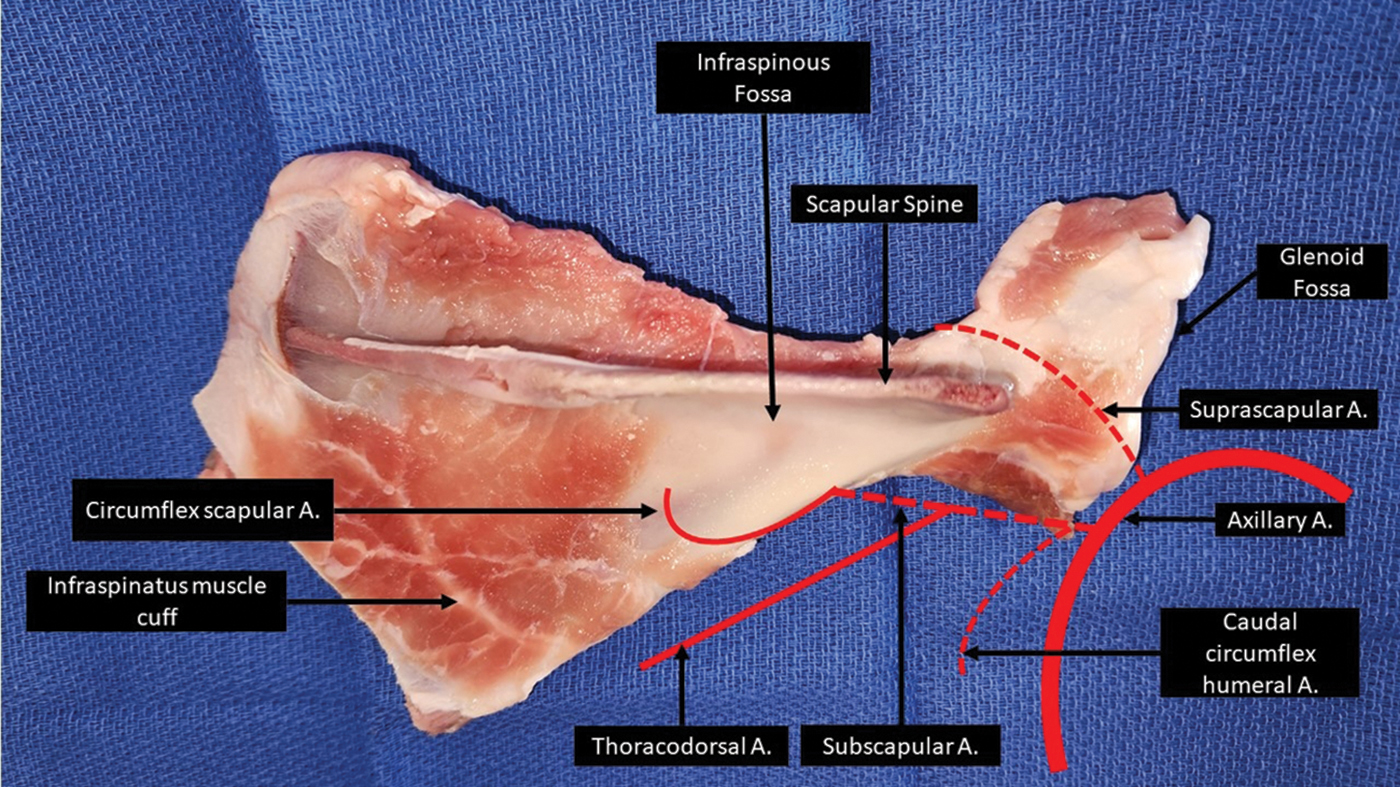
Lateral view of a right sheep scapula labeled with bony landmarks and arterial blood supply superimposed (red). Color images are available online.

Sheep scapula dissection with the periosteum reflected with attached infraspinatus muscle from the underlying bone. Note that the periosteum fragments closer to the glenoid fossa (right of figure). Color images are available online.
Concept development
To utilize the osteogenic properties of periosteum within the bioreactor, two surgical approaches were used. In the first approach (Group A), printed polyetheretherketone (PEEK) bioreactors were wrapped circumferentially in vascularized periosteum, with the whole external surface of the bioreactor contents in contact with cambium as given in Figure 3A. This maximized the surface area of the bioreactor–periosteum interface. However, the second approach (Group B) allowed the model to compare osteogenesis of the polyetherketone (PEK) bioreactor through contact with periosteum and bone simultaneously. Figure 3D demonstrates how the separation of two chambers arranged in a “H-shape” accommodates dual contact for simultaneous testing.
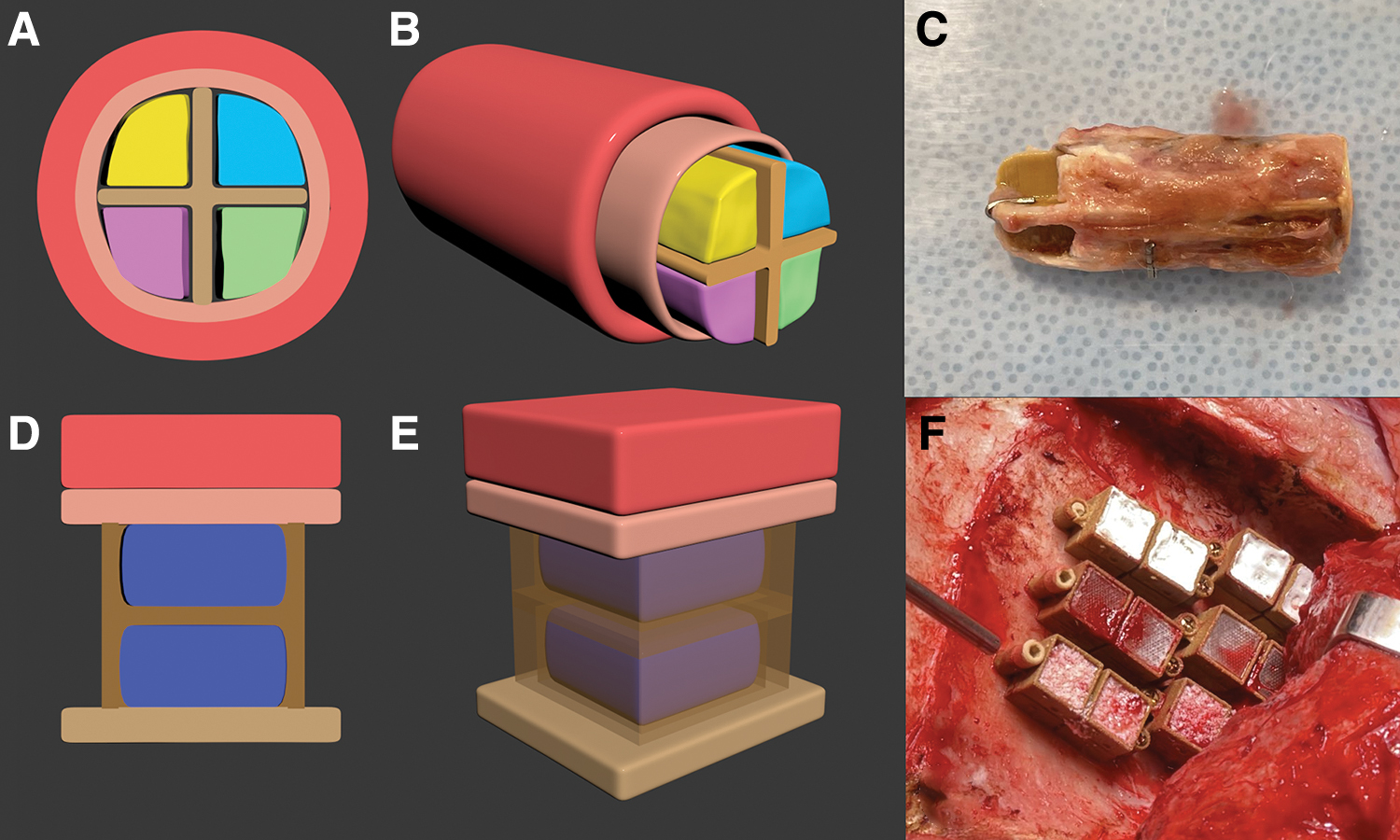
Two bioreactor designs were used in the ovine models.
Fabrication of printed PEEK and PEK bioreactor scaffolds
PEEK bioreactor scaffolds were fabricated in-house as previously described 26 using an AON M2 (AON3D, Montreal, Canada) fused filament fabrication (FFF) 3D printer. The PEEK material was ThermaXTM PEEK filament (batch 49-122619-06JV; 3DXTech, Grand Rapids, MI). The bioreactors were printed with a 0.4 mm diameter hardened steel nozzle on a polyetherimide build plate with a raft of PEEK to prevent contamination of the bioreactors. The FFF PEEK bioreactor design depicted in Figure 3A was cross-shaped in cross-section dividing the 10 × 10 × 40 mm rectangular prism into four chambers, providing space for four separate biomaterial bone substitutes to be housed concurrently. Postprinting processing involved annealing to complete the crystallization process. Scaffolds were placed in a dry oven with the temperature steadily increased to 200°C before being held at this temperature for 2 h and then steadily returned to room temperature.
PEK bioreactor scaffolds were fabricated in-house using PEEK HP3 powder (EOS GmbH, Krailling, Germany) and an EOS P800 (EOS GmbH) high temperature selective laser sintering (SLS) 3D printer. After printing and cooldown, the scaffolds were removed from the powder cake of the finished print and blasted free of unsintered powder with dry ice using a ColdJet Microclean at 1.8 bar gauge pressure and a feed rate of 0.15 kg/min (ColdJet, Loveland, OH). The SLS PEK bioreactor design in Figure 3D was H shaped in cross-section with two chambers of 10 × 10 × 5 mm, providing separate zones for biological contact.
Experimental animals
Fourteen elderly Dorset cross sheep (12 female, 2 male, age 6–8 years) were obtained from the University of Sydney laboratory animal services and acclimatized to the study facility for at least 2 weeks. Animals were housed in a minimum of pairs to prevent distress in a temperature-controlled indoor facility with straw bedding and fed a diet of wheaten chaff and oaten hay.
Anesthesia
All animals received a complete physical examination by a specialist veterinarian before anesthesia. Sheep were premedicated intravenously (IV) with a combination of methadone (Troy Animal Care, Glendenning, Australia) 0.2 mg/kg and midazolam 0.4 mg/kg. Anesthesia was inducted with propofol (Propofol Lipuro, B. Braun, Melsungen, Germany) administered intravenously to facilitate orotracheal intubation. Anesthesia was maintained with 1–2% inspired isoflurane (Laser Animal Health) delivered in an air/oxygen mixture. Before surgery both fetlocks were shaved, and one 50 μg fentanyl patch (Sandoz, Basel, Switzerland) was applied to each leg (∼2 μg/kg total). Patches were secured using tape and a layer of Vetwrap to prevent dislodgement. Meloxicam (Troy Animal Care) 0.5 mg/kg was administered intravenously before moving the animal to the operating room.
Ketamine (Randlab, Chipping Norton, Australia) was administered at 20 μg/kg/min IV throughout the procedure following a loading dose of 0.5 mg/kg. Fluid therapy was provided with Hartmann's solution (Baxter, Deerfield, IL) at a rate of 5 mL/kg/h and morphine (DBL, Dhaka, Bangladesh) was administered at 0.2–0.5 mg/kg IV every 4 h or as deemed necessary throughout the procedure. All sheep were mechanically ventilated using volume-controlled ventilation with positive end expiratory pressure of 5 cm H2O to maintain normocapnia. Pulse oximetry, noninvasive blood pressure, capnography, temperature, and electrocardiogram were monitored continuously throughout the procedure and mean arterial pressure was maintained at 70 mmHg or above throughout the entire procedure in all sheep. Active warming was provided to all sheep throughout the procedure using Hot Dog and Cocoon warming systems.
Surgical site access
Animals were placed in sternal recumbency, incision sites shaved, sprayed with 10% povidone–iodine (Betadine, Stamford, CT) and draped. The scapula was palpated, and the borders and spine marked using a sterile pen. A 30 cm curvilinear incision was made by electrocautery along the spine of the scapula. Subcutaneous fat and cutaneous omobrachialis was divided, and the junction between latissimus dorsi and trapezius muscles was incised to gain access to the underlying infraspinatus muscle.
Periosteal wrap model (Group A)
Infraspinatus and teres major muscles were detached from the infraspinous fossa using electrocautery, preserving the vascular supply to the periosteum by leaving a 2 mm cuff of muscle attached to bone and preserving its insertion to the humerus. The periosteal branch of the circumflex scapular artery and vein were identified and isolated at the ventral border of the scapula overlying the insertion of the teres major muscle. A large cutaneous perforator was frequently observed, analogous to the parascapular artery in humans, which could be followed retrograde to identify the circumflex scapular vessels. The periosteum was incised at the cartilaginous portion of the scapular tip and stripped from the entire infraspinous fossa using a periosteal elevator, in the direction of the vascular pedicle. Care was taken not to compromise the vascular pedicle and to include the inner cambium layer with the periosteum. The periosteum was wrapped circumferentially around the cross-shaped PEEK scaffolds leaving access at the distal portion of the flap (Fig. 4F).

Surgical steps for implanting the Group A scapular periosteal wrap flap in sheep.
Four different biomaterials were combined with platelet-rich fibrin (PRF) and then inserted into the bioreactor: morselized autologous bone graft from the scapula, bovine xenograft (Bio-Oss®; Geistlich Pharma AG, Wolhusen, Switzerland), porcine xenograft (ZenGro®; Southern Implants, Irene, South Africa), and calcium phosphosilicate (NovaBone® Putty; Novabone, FL). An open-ended 1 mL syringe was used to pack the graft material inside the chambers, ensuring complete contact with periosteal cambium. The edges of the flap were sutured using 4-0 prolene (Ethicon, Inc., Raritan, NJ) in an interrupted manner, being careful to preserve the vascular pedicle.
Infraspinatus was reattached to the cartilaginous caudal border and bony spine with 1-0 Vicryl suture (Ethicon, Inc.) anchored through drilled holes where required. The bioreactor was placed between the infraspinatus and overlying latissimus dorsi muscle and secured in place with interrupted 2-0 Vicryl suture. Deep closure of the wound was achieved with 3-0 Vicryl suture in an interrupted manner. A wound soaker catheter was introduced subcutaneously, and skin was closed with continuous 3-0 Monocryl, and knots buried to prevent infection.
Periosteal-bone dual contact model (Group B)
Access to the infraspinatus was the same as Group A. The whole muscle belly was detached from the scapula spine and cartilaginous tip using electrocautery. Then the periosteum was raised using a sharp periosteal elevator with the infraspinatus and teres major muscles together leaving its blood supply via the ventral border and insertion to the humerus intact. Caution was taken not to compromise the vascular pedicle and to include the inner cambium layer with the periosteum and muscle.
After raising the musculoperiosteal flap, each bioreactor was secured to the scapular bone with two 2 × 11 mm titanium screws (KLS Martin, Mühlheim, Germany). The musculoperiosteal flap was then lowered onto the bioreactor, such that the cambium was in contact with the superficial surface (Fig. 5F). Infraspinatus was reattached to the cartilaginous caudal border and bony spine with 1-0 Vicryl suture anchored through drilled holes. Deep closure of the wound was achieved with 3-0 Vicryl suture in an interrupted manner. A wound soaker catheter was introduced subcutaneously, and skin was closed with continuous 3-0 Monocryl.

Surgical steps for implanting the Group B scapular periosteal dual-contact bioreactor in sheep.
Three graft materials were used separately for these chambers: bovine xenograft (Bio-Oss) mixed with PRF, polycaprolactone–gelatin methacryloyl (PCL-GelMA; Translational Research Initiative for Cell Engineering and Printing, Wollongong, Australia), and PCL-GelMA-tricalcium phosphate (PCL-GelMA-TCP; Bionnovation Biomedical, São Paulo, Brazil).
Animal recovery
At the end of the procedure, the wound soaker catheter was loaded with 1 mg/kg of bupivacaine (Pfizer, Tokyo, Japan) diluted 50:50 with 0.9% sodium chloride (Baxter, Deerfield, IL) to provide pain relief to the surgical site. Before recovery, sheep were weaned from mechanical ventilation and the mouth and oropharynx cleared as required. Animals were recovered in their home pens on a thick layer of straw. Continuous pulse oximetry monitoring as well as assessment of respiratory rate and effort were carried out throughout the recovery period with oxygen supplementation via face mask provided if oxygen saturation (SpO2) fell <90%. Continuous warming was provided using a Cocoon forced warm air system until sheep reached 39°C or until they were ambulatory. Following extubation, sheep were fitted with custom-made jackets that housed an elastomeric pump system. Animals were monitored for food intake as well as ambulation at least twice a day for the remainder of the study period.
Postoperative analgesia
Before leaving the sheep overnight a single dose of methadone 0.2 mg/kg was administered intravenously to continue provision of opioid analgesia until the fentanyl patches were estimated to have reached therapeutic plasma concentrations ∼12 h following application. Local anesthesia of 0.25% bupivacaine mixed with 300 μg of buprenorphine (Temgesic, Reckitt, Berkshire, United Kingdom) was delivered to the operative site via the wound soaker catheter twice daily. Pain was assessed using a combination of the sheep grimace scale as well as general behavioral signs of pain by a specialist veterinary anesthetist three times a day for the first 2 days, and then twice daily for up to 1 week following surgery.
Complications
Complications were graded according to the Clavien–Dindo Classification (2004) for surgical complications. 27
Sacrifice
Before killing sheep were premedicated as previously described and anesthesia was induced with propofol until loss of consciousness was achieved. Sheep were killed using a combination of pentobarbitone and potassium chloride administered IV. At the conclusion of the study (14 weeks) the bioreactors were explanted. A minimum of 5 mm of bone was left attached to the lower bioreactors.
Tissue analysis
The materials were nondestructively imaged using a high-resolution microcomputed tomography (micro-CT) imaging (U-CT; MILabs) controlled by a MILabs workstation (Intel(R) Xeon(R) CPU E5-2690 V4 @2.60 GHz, 128G B RAM, 64-bit Operating System). Samples were scanned using an accurate scan mode with ultrafocus magnification and 20 μm resolution (55 kV tube voltage, 0.19 mA tube current, 75 ms exposure time, and 469 mGY dose estimation while being imaged 360° at 0.25 degree per step angle). Scanned image sequence were saved in .tif (Tag Image File) format (1536 × 1944 pixels, 16-bit depth, uncompressed resolution) and transferred to a postprocessing workstation (Intel(R) Core (TM) i5-2400 CPU @ 3.10 GHz, 4 GB RAM, and 32-bit operating system) for imaging reconstruction. The scan data of one sample was then reconstructed (total of 180 slices) using MILabs-Rec-10.16 software and exported to an imaging file in an NII (Neuroimaging Informatics Technology Initiative) format for further segmentation and analysis.
Specimens used for histology were fixed in 10% neutral-buffered formalin for at least 7 days. A diamond bone saw (Exakt Technologies, Inc., Oklahoma City, OK) was used to section the bioreactors into 5 mm slices, perpendicular to the long access. They were then transferred into tissue cassettes for acid decalcification overnight before processing using a Leica Peloris Tissue Processor (Leica Biosystems, Melbourne, Australia). The sections were embedded in paraffin on a TES Valida® Paraffin Embedding Centre (Medite GmbH, Wollenweberstr, Germany), sectioned at 4 μm thickness with a Leica RM2235 Rotary Microtome (Leica Biosystems, Melbourne, Australia), and mounted on glass slides for H&E staining with Sakura Tissue-Tek Prisma® Automated Slide Stainer (Sakura Fineteck USA, Inc.).
Experiment
Surgery was completed on 8 animals in Group A and 6 animals in Group B. The vascular supply to one Group A bioreactor (sheep 6) was found to be compromised at explantation; based on histological analysis ischemia was estimated to have occurred at week 6.
Analgesia
All sheep in Group A were deemed to need rescue analgesia on the first morning following surgery with moderate lameness being noted before administration of additional bupivacaine and buprenorphine. Therefore, the pain relief strategy was modified for Group B to replace the twice-daily wound-soaker administration in Group A with a continuous local infusion of bupivacaine 0.25% at a rate of 2 mL/h for 72 h postoperatively. Two sheep dislodged their elastomeric pumps and thus received additional loading doses of bupivacaine before recommencing bupivacaine infusions and no further analgesic interventions were required.
Complications
There were two Clavien–Dindo Grade IV complications, both unrelated to the surgical method, and the remaining complications were Grade I as shown in Table 1. A suspected hemorrhagic stroke caused one animal (Sheep 1) in Group A to not recover from anesthesia. This animal had a concurrent cranial procedure performed during the same operation and hence the stroke was deemed unrelated to the scapular surgery. The animal was killed after resuscitation efforts failed. One fatal aspiration also occurred in Group A (Sheep 2) following induction of anesthesia. This was discovered at the completion of the surgical procedure and the animal was killed immediately. Serous discharge drained directly from the surgical incision site of one animal (Sheep 3); however, this resolved spontaneously without intervention. Two animals in Group B (Sheep 11 and 12) had local infections at other surgical sites (mandibular and maxillary implants) unrelated to the procedure described, which resolved with antibiotic therapy before the date of killing. One animal was provided probiotic therapy during the experiment in response to soft stools (Sheep 13).
Complications Associated with Each Experimental Animal
Bioreactors in the vascularized wrap design (Group A) were exposed to periosteum only, whereas those in the flat contact design (Group B) were exposed to native bone on the deep surface and periosteum on the superficial surface.
Histological analysis
Histological examination of the bioreactors included evaluation of osteoid and bone formation in addition to cartilage formation, histiocytic and foreign body reaction, chronic inflammation (lymphocytic), and fibrosis. Each histological feature was assessed quantitatively from absent to diffusely present (scale of 0–3), as presented elsewhere. 28 In the cross-shaped bioreactor wrapped in periosteum, most osteoid production occurred at the edges of the bioreactor chambers adjacent to the periosteum. Fibrous tissue formed around all graft materials. Endochondral ossification was observed in the Bio-Oss and ZenGro chambers. The most substantial woven bone development occurred within chambers containing autologous bone graft (Fig. 6A).
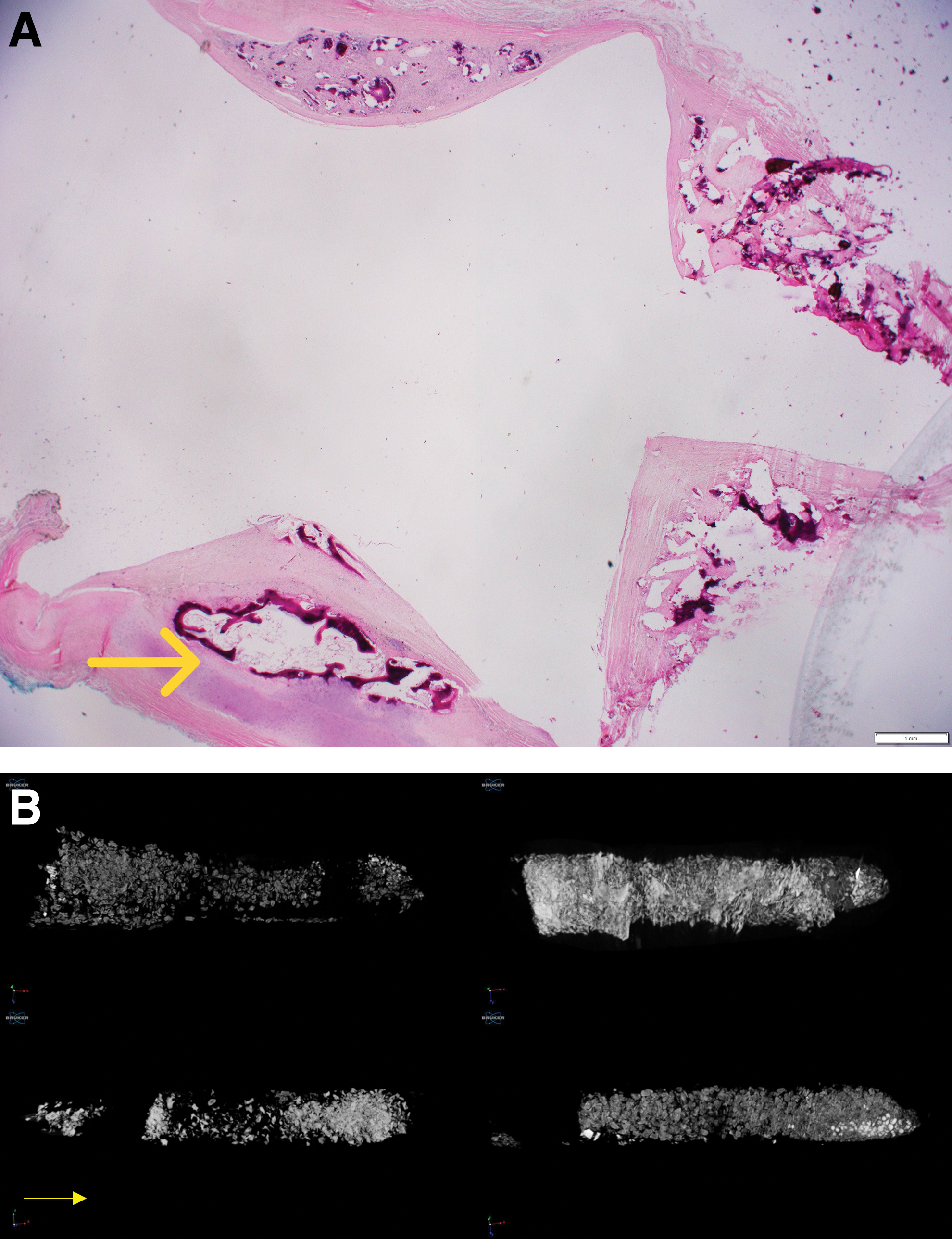
Representative results from 10-week timepoint for Group A periosteal wrap bioreactors.
In the H-shaped dual-contact bioreactors, new bone formation was observed in both the upper (periosteal contacting) and lower (bone contacting) chambers, but more was observed in the chambers contacting bone. Focal osteoid production was observed at the edge of the bioreactors containing GelMA (Fig. 7B) and more substantial osteoid was observed surrounding the implanted material in the bioreactors containing PCL-GelMA-TCP (Fig. 7C).

Representative results for Group B dual-contact bioreactors.
Micro-CT analysis
Radiological assessment of the graft material was achieved using volumetric analysis and bone mineral density. Across all timepoints the greatest mineral density was seen in Bio-Oss chambers; however, histological analysis demonstrated that most of the mineral content was not bone (Figs. 6B and 7D, E).
Discussion
The present protocol describes a novel approach that allows the use of vascularized periosteum to wrap implanted bioreactors (and other biomaterial constructs) circumferentially and permits concomitant contact of biomaterials with periosteum and cortical bone. The protocol differs from previous approaches in that it allows direct within-subject comparison of bone and periosteum contact, and in the ability to wrap large complex scaffolds that would be suitable for BGBR reconstruction of critical-sized bone defects such as those seen in segmental mandibulectomy.
Periosteum plays a significant role in bone growth, repair, and nutrient supply. Periosteum covers nearly every bone surface in the body, and is attached to the cortical surface by Sharpey's fibers. 29 Histologically, it can be divided into two layers. First, the superficial layer comprises a highly vascularized fibrous portion supplying nutrients to the bone and surrounding muscle, as well as a hypocellular fibroelastic portion. 30 It is this fibroelastic contribution that allows the periosteum to be surgically manipulated in our ovine model around bioreactors of any shape. Second, the deep inner cambial layer sits in contact with the bone cortex. The cambium harbors great osteogenic potential owing to its high concentration of osteoprogenitor cells imbedded within its collagen matrix along with a rich vascular and neural supply.19,29 It is likely that more exuberant bone growth would have been observed by using younger sheep; however, it is these older sheep that more closely replicate the adult human bone biology.
Clinically, vascularized periosteal flaps are well described as a surgical approach to optimize local bone healing. 31 Periosteal tissue is ideal for use in combination with a bioreactor, providing osteoinduction without the need for exogenous growth factors. 32 Of note, our group has recently investigated the use of scapular periosteal flaps in humans given the large osteogenic surface area, reliable pedicle, and low associated morbidity. 33 We also investigated the possibility of using an ex vivo perfusion bioreactor system to preserve the tissue viability of periosteum. 34
Several animal models have been used to assess bone scaffolds using periosteum as an osteogenic source. The majority utilize periosteum from the rib body as summarized in Table 2, and the most used animals included rats, dogs, pigs, and sheep.3,24,35 However, no previous studies have used the scapula as a donor site in animals. Previous techniques are limited by the small surface area of periosteum available for grafting. This challenge is overcome in our model by using periosteum from the broad infraspinous region of the scapula. Our model allowed for simultaneous testing of up to 24 (12 double-sided) 10 × 10 × 5 mm bioreactor chambers per scapula in the flat contact approach or a single 40 × 10 mm four-chambered bioreactor per scapula using the periosteal wrap. This is readily translatable to humans, with scapular periosteum from the infraspinous region having a mean thickness of 1.2 mm and dimension of 13.7 × 9.3 cm. 33
Different Preclinical Animal Models That Incorporate Periosteum for Assessing Bone Scaffolds In Vivo
Although sheep are comparable with humans in both size and physiology, several differences were observed during the surgical procedure and recovery. The absolute size of any scapula will be determined by the age and breed of the animal. In our experiments, Dorset cross sheep between the ages of 6–8 years were used. This allowed us to harvest a large periosteal flap; however, skeletally mature animals inherently have a lower osteogenic capacity compared with growing specimens. 17 In addition to the latissimus dorsi and trapezius muscles that overly the scapula in humans, sheep have an additional superficial muscle, the cutaneous omobrachialis, which runs over the lateral surface of the shoulder and extends to the caudal aspect of the scapula. 25 Differences in the skin and wool layers also make dressing the surgical site in sheep somewhat harder. Owing to the production of lanolin, sheep skin is too waxy for traditional adhesive dressings. As such, we opted to use a spray-on waterproof dressing following primary skin closure (OpSite Spray, Smith+Nephew, Watford, United Kingdom).
Initially we were concerned about the effect that surgery would have on the mobility of the sheep; however, the addition of a wound-soaker catheter provided excellent postoperative analgesia in nearly all the sheep implanted. The use of older sheep comes with increased operative risk, particularly in ruminants, as observed in this protocol where two sheep succumbed to complications including aspiration and stroke. Although it is important to maximize the utility of each experimental animal, it is important to carefully consider the effect that concurrent experiments may have on each other. In our experience, two sheep were unable to reach their planned date of killing resulting in a considerable waste of resources.
Conclusion
In this methods article we describe a novel model for assessing bone regeneration using periosteum and bone from a safely accessible and large surface area in the scapula. Our reproducible and standardized surgical technique optimizes the use of experimental animals allowing simultaneous testing of up to 24 bioreactor chambers per scapula in the flat contact approach or a single four-chambered bioreactor per scapula using the periosteal wrap. Following incubation of the bioreactors, various destructive and nondestructive analytical techniques can be used to determine the quality and quantity of bone formed.
Authors' Contribution
Y.A.G.: Writing—original draft, investigation. H.X.: Project administration, investigation, formal analysis. D.S.A.A.M.: Project administration, investigation, formal analysis. K.C.: Writing—review and editing, investigation, data curation. I.W.: Investigation, resources. C.B.: Writing—review and editing, investigation, resources. R.G.: Investigation, formal analysis. V.K.-Y.C.: Writing—review and editing, investigation, formal analysis. J.W.: Writing—review and editing, investigation. D.L.: Writing—review and editing, investigation. C.F.: Writing—review and editing, investigation. W.L.: Writing—review and editing, investigation. H.V.K.: Investigation. E.T.-C.: Writing—review and editing. D.R.M.: Writing—review and editing, resources. J.C.: Writing—review and editing, Resources. J.R.C.: Conceptualization, methodology, writing—review and editing, Investigation, Supervision. Y.A.G, H.X., and D.S.A.A.M. contributed equally to this article.
Footnotes
Acknowledgment
The authors acknowledge the facilities and the scientific and technical assistance at the Hybrid Theatre, Sydney Imaging, a Core Research Facility, University of Sydney.
Disclosure Statement
No competing financial interests exist.
Funding Information
The authors acknowledge the following sources of funding supporting this research:
The Cancer Institute New South Wales (CINSW 2020/2081), the National Health and Medical Research Council (NHMRC 2023/GNT2024602), Sydney Local Health District, The Lang Walker Family Foundation, the Australia and New Zealand Head and Neck Cancer Society, the Arto Hardy Family, and the Federal Government of Australia through the Sarcoma and Surgical Research Centre.