
Abstract
Experimental analyses of knee joint contractures have traditionally utilized a 6-month rabbit model as the gold standard. However, this model is time-intensive and costly. The purpose of this study was to develop an abbreviated rabbit model of knee contractures and compare it to the well-established longer model. Twenty female New Zealand White rabbits were divided into two equal groups and prospectively studied to assess knee passive extension angles (PEA), contracture angles (CA), and terminal posterior capsular stiffness. Experimental knees were immobilized for either 4 weeks (n = 10) with an 8-week remobilization period in the abbreviated model (i.e., 3 months) or for 8 weeks (n = 10) with a 16-week remobilization period in the standard model (i.e., 6 months). PEAs were assessed at remobilization and several time points using differing vertical forces. At sacrifice, terminal biomechanical data were collected to assess posterior capsular stiffness. Analysis of PEAs in live animals at each torque value and time point demonstrated increased PEAs and decreased CAs in the 3-month abbreviated model as compared to the 6-month standard model. At sacrifice, biomechanical analysis demonstrated that the posterior capsules of the 3-month experimental limbs were significantly more stiff than the contralateral limb (2.4 vs. 0.05 Ncm/°, p < 0.0001), but significantly less stiff compared to the 6-month experimental limbs (2.4 vs. 4.7 Ncm/°, p < 0.0001). Our study suggests that the 6-month standard rabbit knee model of arthrofibrosis should continue to be used in the laboratory assessment of arthrofibrosis. However, the abbreviated model may be beneficial under selected experimental conditions.
Impact Statement
Orthopedic animal models, especially rabbit models of knee stiffness, are crucial for testing therapeutic efficacy due to their similarity to human knee joints. The standard 6-month rabbit model is time- and cost-intensive. To address this, a 3-month model was developed, yielding comparable results in live passive extension at various vertical forces. However, it showed significantly less stiff posterior capsule stiffness than the 6-month model. This study presents a viable, shortened model for measuring live passive knee extension, offering a more efficient option for therapeutic efficacy research in live specimens.
Introduction
Joint contractures and their negative sequelae following synovial joint trauma have been described since the time of Hippocrates. 1 Joint contractures decrease an affected joint’s natural range of motion, often resulting in pain, loss of function, decreased dexterity, and cosmetic deformities.2,3 In the upper extremity, joint contractures limit activities of daily living such as transferring, feeding, hygiene, toileting, and self-dressing.4,5 In the lower extremity, joint contractures alter gait kinematics, increase energy expenditure during ambulation, and limit exercise capacity, with significant ramifications on the cardiopulmonary system.6–9 Despite modern postinjury regimens, improved surgical techniques, and early, regimented physical therapy, the prevention and treatment of joint contractures continue to pose a problem for contemporary orthopedic surgery. 10
Given the life-altering sequelae of a joint contracture, the development of a robust animal model for the study of the disease process and novel therapeutics is paramount. While animal models utilizing mice, rats, and canines have been described in the literature, rabbit models of joint contracture are commonly utilized.11–20 Rabbit models are advantageous in studies of joint contracture given the larger hind limb size in comparison to rodents, which allows for ease of identification of joint structures and allows for a myriad of different treatment modalities to be studied. Rabbit knee joints are also more similar to human knee joint anatomy, except for a smaller patella with respect to other structures. 21 Unfortunately, the cost of rabbit models is significantly higher than that of rodent models. 22 In addition, current rabbit models of joint contractures require a prolonged period to establish contracture, and experimental timelines often total 6 months, which is both time- and cost-intensive.16,17,19,20
The time-intensive and costly nature of current joint contracture rabbit models limits their more widespread use and adoption in mechanistic and therapeutic orthopedic studies. The development of a shortened model of rabbit joint contracture would increase access to this model and promote studies regarding the mechanisms of joint contracture and potential therapeutic interventions. Therefore, the purpose of this study was to develop an abbreviated rabbit model of knee contractures and compare it to the well-accepted standard model to determine whether equivalent knee stiffness could be achieved.
Methods
Ethical treatment of animals
All animals were treated ethically in this study. Our Institutional Animal Care and Use Committee (IACUC#: A6201-21) prospectively reviewed and approved all procedures performed. New Zealand skeletally mature white rabbits (Charlies Rivers Laboratories, MA, USA) were utilized in this study. The rabbits were approximately 2.5 to 3.5 kg in weight and were allowed free cage range and water and food ad libitum. No animal suffered a surgical, perioperative, or postoperative complication. Before terminal biomechanics, rabbits were sacrificed with intravenous Fatal-Plus (100 mg/kg; Vortech Pharmaceuticals Ltd., Dearborn, Michigan, USA). This study followed the guidelines stated in the Animals in Research: Reporting in vivo Experiments (ARRIVE) guidelines.
Experimental design
Twenty mature female New Zealand White rabbits aged approximately 10 months were evenly divided into two experimental groups. Group 1 (abbreviated model, 3-month) was immobilized for 4 weeks and remobilized for 8 weeks. Group 2 (standard model, 6-month) was immobilized for 8 weeks and remobilized for 16 weeks.
Surgical knee joint immobilization
We have previously published on the surgical immobilization and remobilization procedures for the standard rabbit model of arthrofibrosis.16,23–26 Briefly, operative sedation was achieved with weight-based ketamine (35 mg/kg; Zoetis, NJ, USA), xylazine (5 mg/kg; Akorn Animal Health, IL, USA), and continuous flow isoflurane (1–3% mg/kg; Piramal, KY, USA). Cefazolin (22 mg/kg; Institutional Pharmacy) and Buprenorphine ER (0.18 mg/kg; Institutional Pharmacy) were used for infection prophylaxis and analgesia, respectively. The right leg of each rabbit was shaved, and each animal was intubated and placed supine on the operative table. Operative limbs were prepped and draped in the usual surgical fashion. Operative knees were fully flexed, and an approximately 2 cm midline incision was made over the center of the knee joint using a 10 blade (Bard-Parker, NJ, USA). Blunt dissection was used to remove the soft tissues overlaying the synovial joint capsule. A lateral arthrotomy was made and carried down to bone. The patella was subluxated medially. All soft tissues interposed between the femoral condyles were removed, and the cruciate ligaments were severed using a 15 blade (Bard-Parker) and dental pick. The posterior capsule was traumatically disrupted by hyperextending the knee to −45°. Subsequently, bilateral femoral cortical defects were made proximal to the articular cartilage using a 3 mm drill to simulate the marrow elements introduced at the time of trauma or surgical intervention. The patella was restored to its anatomical position. The knee was fully flexed once more, and an anteromedial incision approximately 2 cm in length was made over the anterior tibia using a 10 blade. A steel Kirschner wire (Stryker; Kalamazoo, MI, USA) with a single trocar point and half-threaded to support a nut was introduced from the anterior tibial crest 1 cm distal to the tibial tubercle using a 1.6 mm drill. An approximately 2 cm incision was made over the lateral femur, and blunt dissection was used to expose the femur, and a freer elevator was used to strip the periosteum. The tibial Kirschner wire was advanced lateral to the femur and visualized through this incision. The sharp Kirschner wire tip was clipped and subsequently bent to form a hook. The hooked end of the Kirschner wire was passed over the femur from lateral to medial to avoid any interruption of the medial neurovascular bundle. The Kirschner wire was secured to the tibia using a nut with the knee in ≥160° of flexion. All incisions were irrigated with normal saline. The arthrotomy was closed using 4-0 Vicryl (Ethicon, NJ, USA) in a running fashion, and the skin incisions were closed using 4-0 Monocryl (Ethicon) in a running fashion.
Surgical knee joint remobilization
After a period of immobilization, a second surgical procedure was performed to remobilize the right limb by removing the Kirschner wire. After anesthetization and preparation of the right lower extremity as described above, an approximately 1 cm incision was made over the anteromedial tibia using a 10-blade. Blunt dissection was carried down onto the previously implanted hardware. A rongeur was utilized to clear the hardware of any callus and soft tissue formation overlying the implanted hardware. The previously implanted nut was loosened from the threaded Kirschner wire. Subsequently, an approximately 2 cm incision was made over the lateral thigh in line with the femur. Blunt dissection was carried down onto the implanted hardware and lateral femur. A rongeur and curette were utilized to clear any callus, heterotopic ossification, and soft tissue that formed over the hardware in the interim. A freer elevator and needle driver were utilized to unhook the Kirschner wire from the femur while avoiding injury to medial neurovascular structures. The Kirschner wire was removed from the femoral wound after being unhooked. The femoral and tibial wounds were irrigated with normal saline. Each incision was closed utilizing 4-0 Monocryl (Ethicon) in a running fashion.
Live passive extension angle measurements
Radiological passive extension angle (PEA) measurements were performed with our previously published validated dynamic load cell device and protocol.16,20,23,24 Briefly, vertical forces were applied to the limb as the rabbit lay supine, and radiographs were taken at each respective force value. To calculate the passive extension angle, lines were drawn from the center of the hip joint along the posterior cortex of the femur and transecting the long axis of the tibia, meeting at the center of rotation of the knee joint (Fig. 1). For 3-month experimental limbs, PEAs in live animals were measured at remobilization, 1 week, 4 weeks, and 8 weeks, and for 6-month experimental limbs at remobilization, 2 weeks, 8 weeks, and 16 weeks at forces of 20, 30, 40, and 50 Ncm. The difference between 3-month and 6-month PEAs was calculated.

Sample radiographical measurement of live knee joint passive extension angle (PEA), utilizing the center of the hip and knee joint and long axis of the tibia to determine the angle of the joint at different force values.
Live animal flexion contracture angles
Contracture angles were calculated by taking the difference between 160°—the normal range of motion of the rabbit knee—and the mean live animal PEAs at each force value, as previously described. 16 The difference between 3-month and 6-month contractures was calculated.
Terminal biomechanical posterior capsule stiffness measurements
Sacrificed rabbits had their experimental and contralateral limbs harvested. To measure isolated posterior capsule stiffness, all soft tissue attachments to the femur and tibia were removed, leaving only the synovial joint capsule. Steel rods were cemented (Stryker, Warsaw, IN, USA) in the tibial and femoral canals and subsequently mounted on a dedicated torque sensor (Transducer Techniques, CA, USA) device to measure capsular stiffness at a rate of 1°/s. Incremental PEAs and torques were graphed using MatLab 2016a (Mathworks, Natick, MA, USA), and a line tangential to the exponential curve segment determined endpoint capsular stiffness.
Statistical analysis
Analyses between 3-month and contralateral limbs and 3-month and 6-month limbs were directly compared using the Mann–Whitney U test. All statistical analyses and figure generation utilized GraphPad Prism 9.3.1 (GraphPad Software, Boston, MA, USA). All data and figures are represented or tabulated as mean ± standard deviation (SD). A significant difference was considered p < 0.05.
Experiment
Live animal passive extension angle measurements
Live animal PEAs for both 3-month and 6-month experimental limbs were significantly stiffer than the respective contralateral limbs at the end of each of their experimental timelines and at all force values (Fig. 2). The 6-month experimental limbs continued to be stiff through their remobilization period for all timepoints and force values. Similarly, 3-month experimental limbs showed a similar trend, though the 3-month limbs were less stiff compared to 6-month limbs (Fig. 3). Mean PEAs are tabulated in Table 1. In a direct comparison of 3-month and 6-month experimental limbs at 8 weeks, 6-month limbs were significantly stiffer at all force values (Fig. 4).
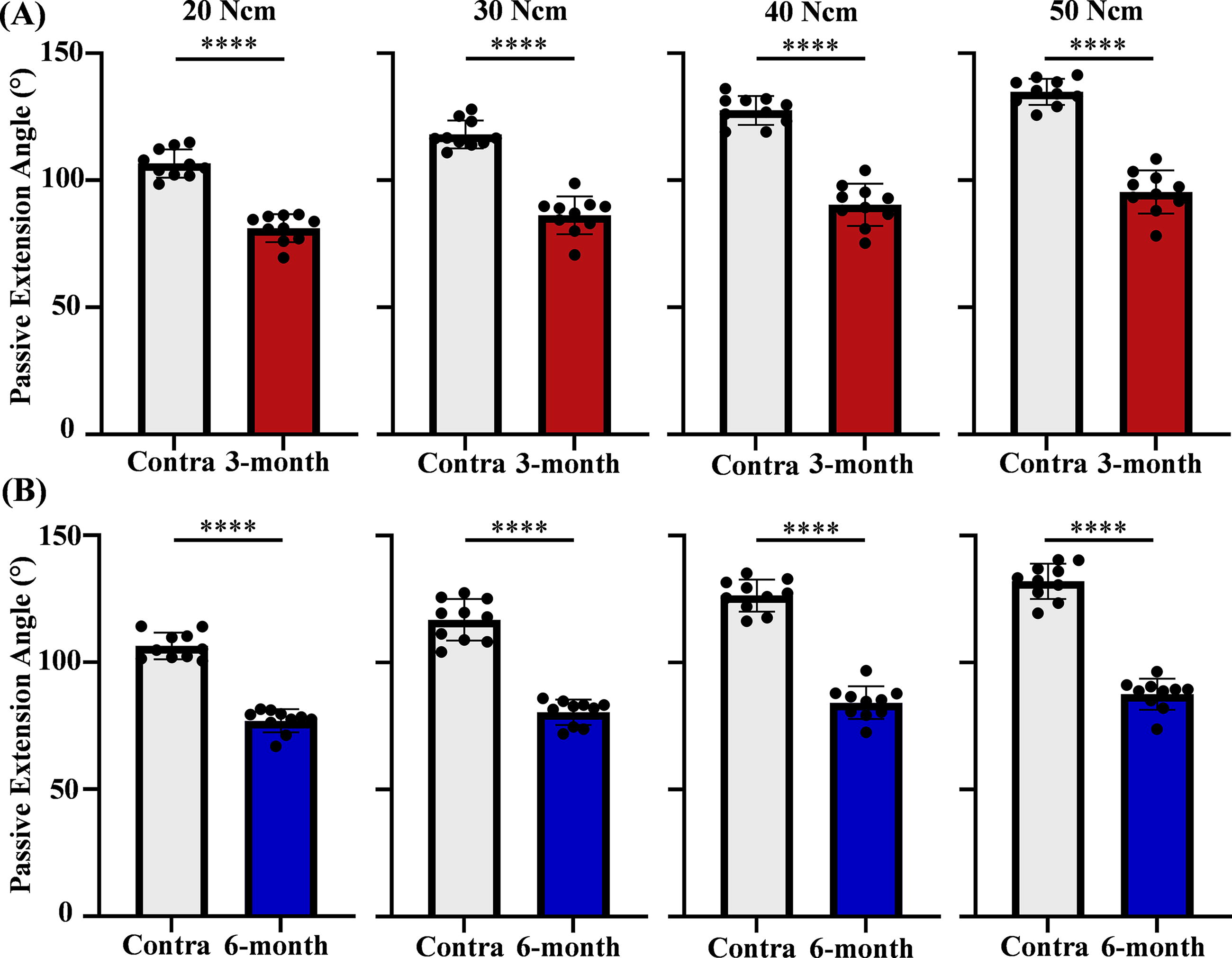
Live passive extension angles (PEAs) for 3-month and 6-month experimental limbs at the end of their experimental timelines.
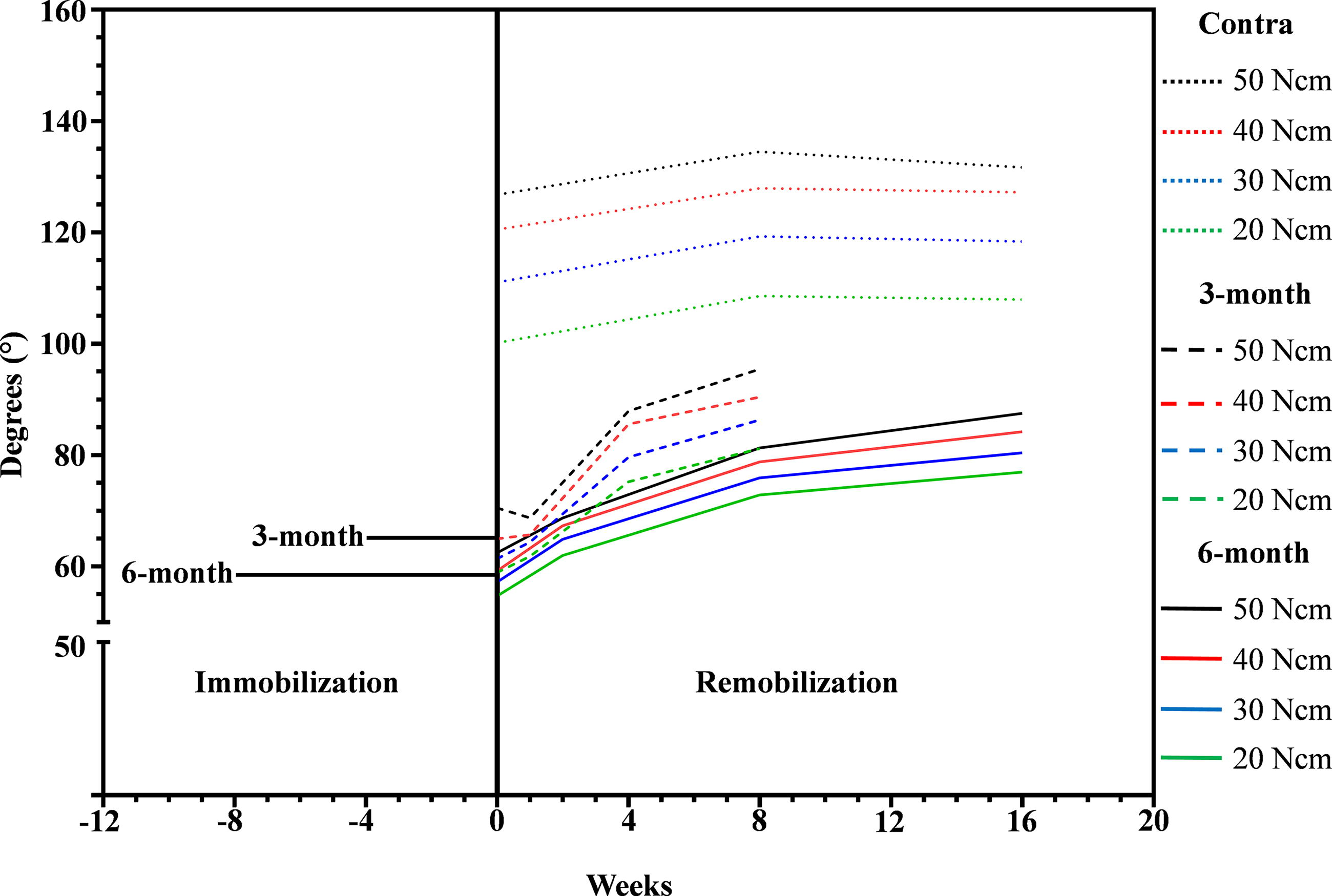
Live passive extension angles (PEAs) for 3-month and 6-month experimental limbs measured at 0, 1, 4, and 8 weeks for 3-month and 0, 2, 8, and 16 weeks for 6-month after remobilization surgery. Contralateral (Contra) limbs were measured at 0, 8, and 16 weeks after remobilization to confirm knee stiffness.
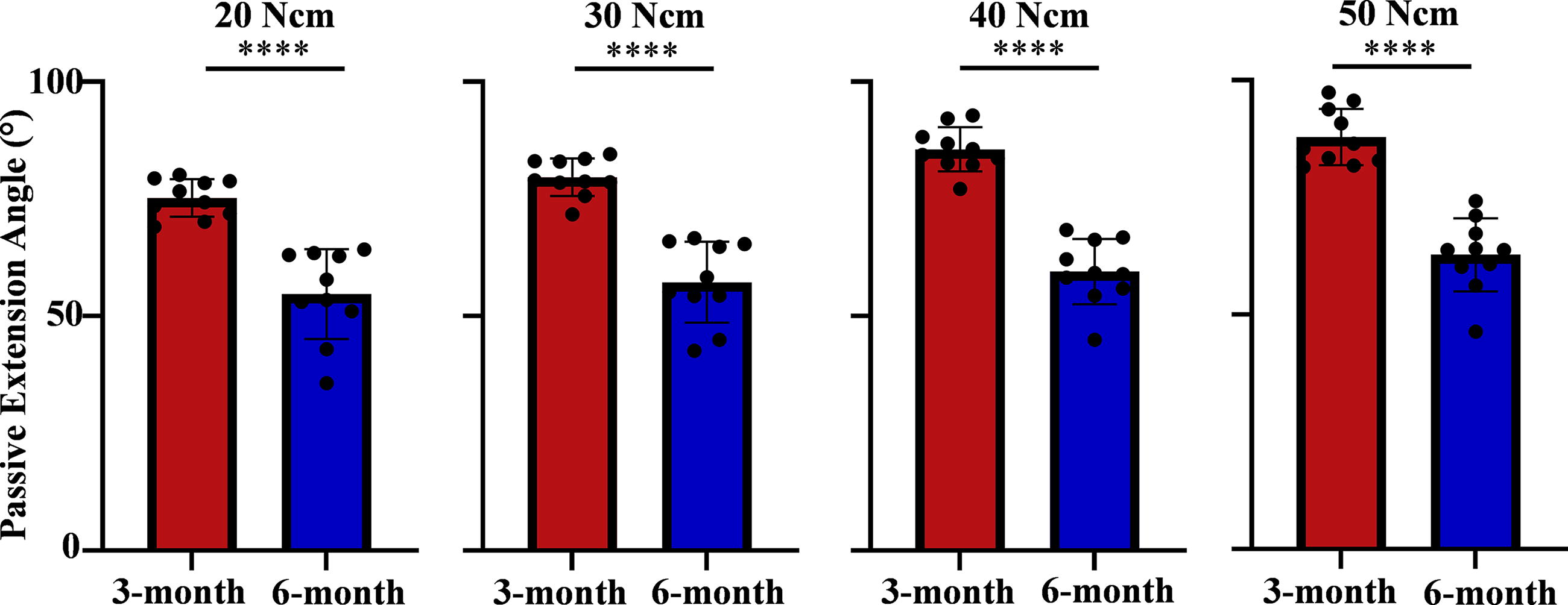
Live passive extension angles (PEAs) with direct comparison of 3-month and 6-month models at 8 weeks. A significant difference was considered p < 0.05, with **** equating to p < 0.0001.
Tabulated Mean Live Passive Extension Angles for Experimental Limbs at Forces of 20, 30, 40, and 50 Ncm
Live animal flexion contracture angles
Historically, contracture angles were used to describe joint stiffness in rabbit models of contracture. Therefore, live animal PEAs were transformed into contracture angles and are tabulated in Table 2 for reference.
Tabulated Mean Live Contracture Angles for Experimental Limbs at Forces of 20, 30, 40, and 50 Ncm
Terminal biomechanical posterior capsule stiffness measurements
Terminal PEAs and capsular stiffness for 3-month and 6-month were significantly stiffer than their respective contralaterals (Fig. 5). Direct comparison between 3 months and 6 months terminal PEAs and capsular stiffness showed the 6-month group to be significantly stiffer than the 3-month group (Fig. 6). The terminal posterior capsular stiffness achieved in this study in comparison to historical studies is recorded in Table 3.

Terminal passive extension angles (PEAs) and capsular stiffness.

Terminal passive extension angles
Present Study Compared to Previously Published Capsular Stiffness Measurements
Discussion
Joint contractures are a problematic pathology that develops secondary to a traumatic joint insult, arthrotomy, periarticular fracture reduction and fixation, total joint arthroplasty, arthroscopy, or neuromuscular disease.27–32 They decrease the native range of motion of a joint and hinder the normal function of a joint, with significant negative ramifications on patient quality of life due to the ensuing negative sequelae, such as difficulties with activities of daily living and gait.5,6 Unfortunately, nonoperative treatment regimens require extensive bracing/casting and physical therapy that are difficult to adhere to and time-consuming, which often necessitates surgical intervention.33,34 Surgical interventions not only expose patients to the inherent risks of surgery, but the range of motion attained is often difficult to preserve, and recurrence of contracture is common. 35 Pharmacologic therapies have the potential to limit the pathophysiologic fibrotic cascade responsible for the development and recurrence of joint contractures following joint insults. To pursue studies of chemotherapeutics that limit the causative fibrosis of pathological joint contracture, a robust animal model is required.
Although multiple animal models have been described for the study of joint contractures, the rabbit is the most commonly used due to its size and analogous anatomy to the human knee joint.11–17,19–21 The first described rabbit models of joint contracture induced knee joint contracture via immobilization alone.36,37 Unfortunately, it was demonstrated that contractures induced via immobilization were rapidly reversible upon remobilization.36,37 Finsterbush and Friedman 36 demonstrated that all animals immobilized for 2 weeks regained full range of motion, and nine of 14 rabbits immobilized for 6 weeks regained knee function. Histological analysis demonstrated normal joint tissues after remobilization. Similarly, Akeson et al. 37 illustrated that rabbits immobilized for 9 weeks regained range of motion within 3 to 6 weeks after remobilization, with normal histological analysis of periarticular tissues.
To overcome the limitations of a rapid return to a natural physiological state following immobilization, Hildebrand et al. 15 built upon previous rabbit knee joint contracture models by combining arthrotomy, femoral condyle cortical bone removal, and immobilization for 8 weeks using Kirschner wire fixation at 150°. While Hildebrand et al. 15 produced a model with a sustained joint contracture, the differences between the 8- and 24-week remobilization arms of the experiment were not significantly different from unoperated contralateral limbs with an average flexion contracture of 8°. With an average contracture difference of less than 10°, the model was unable to meaningfully compare the efficacies of chemotherapeutics with potentially subtle differences.
Nesterenko et al. 16 further improved the established model of rabbit knee joint contracture. They created defects in the femoral condyles, transected the cruciate ligaments, hyperextended the knee joint to −45° to injure the posterior capsule, and immobilized the knee joint using Kirschner wires for 8 weeks as previously described. In Nesterenko et al.’s study, 16 a control group without posterior capsule disruption was created. At remobilization, animals with a posterior capsule disruption had an average larger flexion contracture that was sustained through 16 weeks following remobilization. The sustained large knee joint contracture subsequently enabled the study of numerous pharmacotherapies for the treatment of joint contractures.23,25,26,38–41
While effective for the evaluation of pharmacotherapies for the treatment of joint contractures, the gold-standard rabbit model of knee joint contracture as defined by Nesterenko et al. 16 is time-intensive and costly. The protocol requires an 8-week immobilization period followed by 16 weeks of remobilization for a total experimental time of 6 months. An abbreviated model would be more cost- and time-effective, allowing more accessibility of this model. Hazlewood et al. 42 created a shorter model based on Nesterenko’s 16 finding that disruption of the posterior capsular induced most of the contracted phenotype. 16 They directly visualized and disrupted rabbit posterior capsules and immobilized each limb with absorbable sutures, with the aim of avoiding a secondary surgery for remobilization. While they were able to create stable, irreversible contractures, the average magnitude of flexion contracture of approximately 20° was significantly smaller than that achieved by Nesterenko et al., 16 with the subsequent inherent issue of Hildebrand et al.’s model. 15
In the present study, we aimed to establish an abbreviated model of rabbit knee joint contracture by disrupting the posterior capsule as described by Nesterenko et al. 16 with Kirschner wire immobilization as previously established. However, we used an immobilization period of 4 weeks and a remobilization period of 8 weeks for a 3-month total model protocol. In a direct comparison at 8 weeks, the 3-month and 6-month models diverged, with 6-month rabbits having significantly stiffer limbs at that experimental timepoint. Both models remained stiffer than their contralaterals at the end of their timelines. Thus, the 3-month model flexion contractures remain large enough for assessment of gross therapeutic alterations on flexion contractures and do not suffer from the same issue as that of Hildenbrand’s and Hazlewood’s studies.15,42
On analysis of posterior capsular stiffness following terminal passive extensive angle assessment and sacrifice, we demonstrate that the 6-month model posterior capsule was significantly stiffer in comparison to the 3-month model, with posterior capsular stiffnesses of 4.7 and 2.4 Ncm/°, respectively. The 3-month model was significantly stiffer in comparison to unoperated control limbs that had an average posterior capsular stiffness of 0.05 Ncm/°. Given this finding, we do not anticipate that the 3-month model would be useful in studies that report posterior capsular stiffness as a terminal data point. Moreover, this suggests that this abbreviated model may not be sensitive enough to study histological, architectural, or mechanistic changes to the synovial capsule associated with joint contractures.
In summary, we established a 3-month model of rabbit knee joint contracture with average passive extension and complementary flexion contracture angles that were overall similar to the standard 6-month model. However, the posterior capsular stiffness was significantly lower in our 3-month model. We propose that this abbreviated model of rabbit knee joint contracture may be useful in studies reporting gross outcomes reliant on reporting differences in flexion contractures but not studies reporting posterior capsular stiffness.
Footnotes
Acknowledgment
The authors would also like to acknowledge the Andrew A. and Mary S. Sugg Professorship in Orthopedic Surgery for its philanthropic support that made such research possible (to M.P.A.).
Authors’ Contributions
K.D.A., M.F.C., and M.P.A.: Conceptualization; K.D.A., M.F.C., C.E.B., O.B.D., A.N.P., and R.T.: Data collection and curation; K.D.A., M.F.C., M.E.M., J.S.S., D.J.B., A.D., and M.P.A.: Data analysis and interpretation; K.D.A. and M.F.C.: Writing of original article; K.D.A., M.F.C., C.E.B., O.B.D., A.N.P., R.T., M.E.M., J.S.S., D.J.B., A.D., and M.P.A.: Article review and editing; M.P.A.: Funding acquisition.
Disclosure Statement
K.D.A. (N), M.F.C. (N), C.E.B. (N), O.B.D. (N), A.N.P. (N), R.T. (N), M.E.M. (Bonebridge, Elsevier), J.S.S. (Acumed LLC, Elsevier, Exactech Inc, JSES, Oxford University Press, Precision OS, PSI, Stryker), D.J.B. (Bodycad, DePuy, Elsevier, Wolters Kluwer), A.D. (N), M.P.A. (OsteoRemedies, Springer, Stryker).
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Funding Information
This study was funded by the National Institute of Arthritis and Musculoskeletal Disease and Skins Disease of the National Institutes of Health (MPA, R01AR072597) and the Anna-Maria and Stephen Kellen Foundation (MPA).