
Abstract
Large intracerebral hemorrhage (ICH) is associated with poor outcome. In a recent pilot study, therapeutic hypothermia (TH) prevented perihematomal edema growth and led to a high survival rate. Patients of this pilot study were now investigated 12 months after ICH. Twelve patients were treated with mild TH of 35°C for 10 days. All patients survived day 90 after ICH and were investigated with the modified Rankin Scale (mRS) at day 90 and after 12 months. At day 90, only two patients showed a mRS of 3, whereas all other had a mRS of 4 and 5. After 12 months, 2 patients had died, whereas 6 patients (50%) were able to walk without assistance (mRS 3). TH may be a promising treatment option for patients with large ICH, since pilot data indicate a high survival rate and a high chance for an acceptable functional long-term outcome.
Introduction
Methods
As described previously (Kollmar et al., 2010), 12 patients who suffered large supratentorial ICH (58±29 mL) with a median ICH score (1) of 3.5 (range 2–4) were treated with endovascular hypothermia at 35°C for a period of 10 days after the bleeding event. All patients survived day 90 and were assessed by the modified Rankin Scale (mRS) (Kollmar et al., 2010). Patients and relatives were contacted 12 months after ICH and a second follow-up survey for mRS was done via telephone.
Results
At the early time point of 90 days after ICH, functional outcome was not favorable in the majority of survivors treated with hypothermia. Six patients were severely disabled (mRS 4), and four patients were in a vegetative state (mRS 5). Only two out of 12 patients were able to walk without assistance (mRS 3). The survey after 12 months showed improvement of functional status in five patients with now totally six patients (50%) being able to walk without assistance. Two patients (16.7%), initially scored 4 and 5 on the mRS, respectively, had died at that time (Fig. 1).
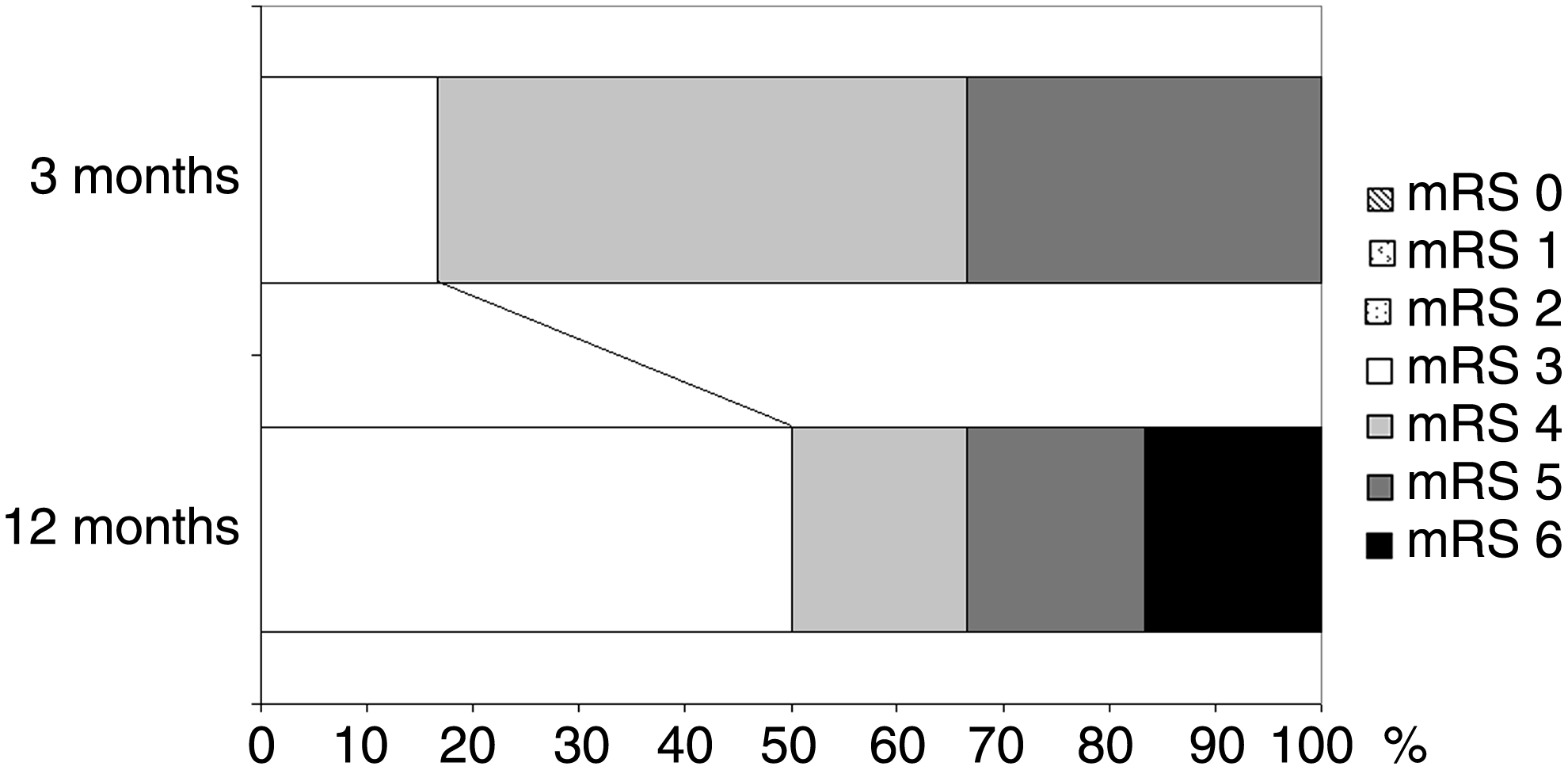
Modified Rankin scale 3 and 12 months after large intracerebral hemorrhage in patients treated with mild hypothermia.
Discussion
Those results are encouraging, because not only short-term (3 months), but also long-term mortality seems to be relatively low in our patients, as compared to available data on ICH (Sacco et al., 2009), despite of the large mean hematoma size in our study. As in large ICH, PHE formation may lead to a considerable additional mass effect, eventually causing herniation (Ropper 1986; Zazulia et al., 1999) hypothermia may have the potential to lower mortality by reducing edema growth.
Another, may be even more important and encouraging finding, is that survival led to functional recovery and regaining of the ability to walk without assistance in a large proportion of our patients (50%) in the long-term follow-up, despite of the relatively high median ICH score value at the time of the bleeding event. In light of the recent debate on hemicraniectomy in malignant middle cerebral artery infarction (Mitchell et al., 2009), the question if lower mortality after large ICH is reached at the cost of survival with a severe deficit also needs to be addressed.
Our preliminary results certainly do not allow any recommendation for the clinical routine, but rather show that this treatment option remains an attractive topic for further clinical research and the effects of hypothermia on mortality and functional outcome in ICH patients need to be investigated in a larger study. Currently, a German-Austrian randomized controlled trial to assess safety, feasibility and efficacy of mild hypothermia after ICH is under way (Kollmar et al., 2011).
Author Disclosure Statement
No competing financial interests exist.