
Abstract
For more than 50 years, hypothermia has been used in aortic surgery as a tool for neuroprotection. Hypothermia has been introduced into thoracoabdominal aortic aneurysm (TAAA) surgery by many cardiovascular centers to protect the body's organs, including the spinal cord. Numerous publications have shown that hypothermia can prevent immediate and delayed motor dysfunction after aortic cross-clamping. Here, we reviewed the historical application of hypothermia in aortic surgery, role of hypothermia in preclinical studies, cellular and molecular mechanisms by which hypothermia confers neuroprotection, and the role of systemic and regional hypothermia in clinical protocols to reduce and/or eliminate the devastating consequences of ischemic spinal cord injury after TAAA repair.
Introduction
There are two main approaches to protecting the spinal cord during TAAA repair surgery. The first involves preservation of regional blood supply and increasing the ischemic tolerance of the spinal cord during aortic cross-clamping. This approach focuses on maximizing effective collateral perfusion by reimplantation of intercostal arteries, left heart bypass grafting, or CSF drainage (Coselli and LeMaire, 1999; Coselli et al., 2002; Griepp and Griepp, 2007). The second approach involves induced hypothermia (systemic and regional) and/or use of neuroprotective agents (Acher et al., 1994; Kouchoukos et al., 1995; Safi et al., 1998).
The induction of systemic hypothermia is a reliable method for conferring neuroprotection and is used by many cardiovascular surgeons. It acts by decreasing oxygen consumption, reducing tissue metabolism, inhibiting the synthesis and release of excitatory neurotransmitters, and eventually restraining the inflammatory response caused by ischemia (Fig. 1) (Busto et al., 1989; Martelli et al., 2002). However, systemic hypothermia also can be associated with adverse events such as impairment of coagulation, increased risk of infection, electrolyte imbalance, cardiac arrhythmia, and pulmonary dysfunction (Rohrer and Natale, 1992; Kurz et al., 1996).
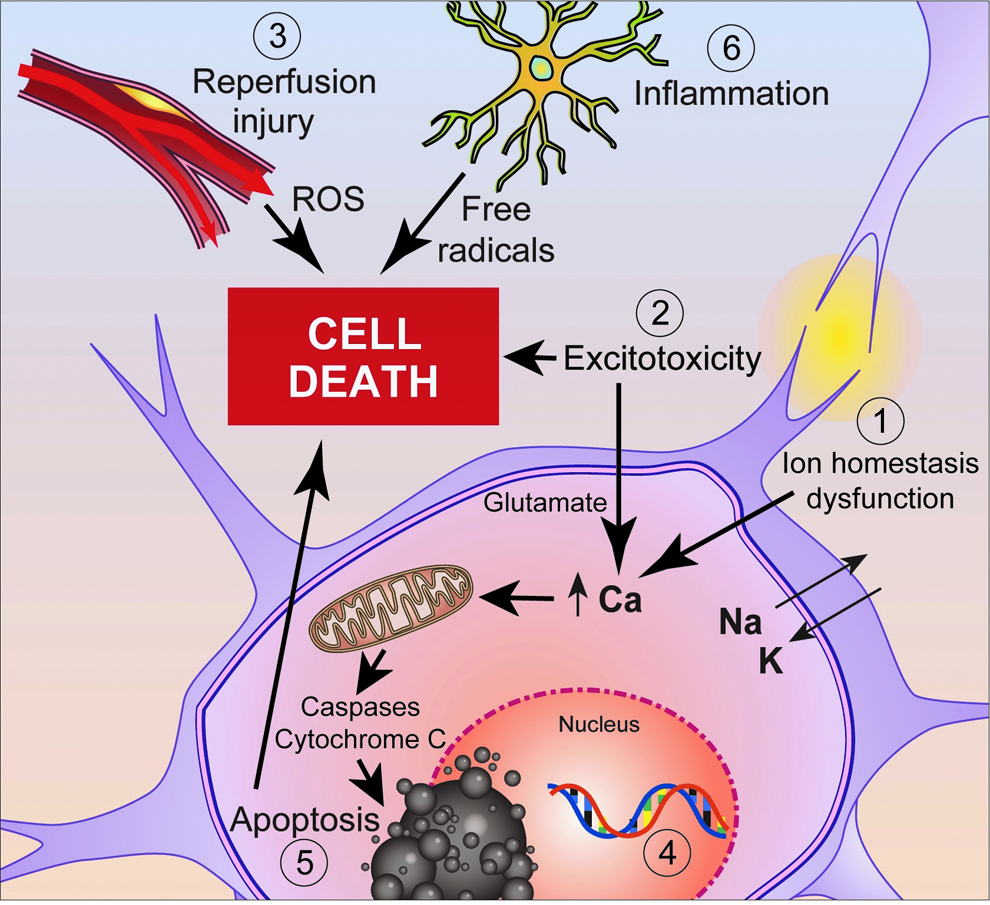
Hypothermia affects several mechanisms of ischemic neuronal injury and repair, including (1) maintenance of cell membrane homeostasis; (2) excitotoxicity; (3) oxidative stress subsequent to reperfusion; (4) increasing expression of neurotrophic genes and genes associated with cell survival (e.g., Bcl-2) while also downregulating proinflammatory and apoptotic genes. (5) Blocking apoptosis by altering cellular levels of p53 and Bcl-2, increase signaling via ERK and Akt and increase secretion of neurotrophins. (6) Attenuating microglial activation and parallel inflammatory cascades.
Conversely, regional hypothermia has fewer side effects, providing neuroprotection without systemic complications (Cambria et al., 1997). It can be applied by infusion of iced saline into the epidural space. However, epidural cooling can cause a sharp increase in CSF pressure, which may attenuate spinal cord perfusion (Meylaerts et al., 2000; Yoshitake et al., 2007). Although systemic or regional hypothermia has some drawbacks, it is still the most frequently used neuroprotective intervention against ischemic spinal cord injury (ISCI) after TAAA surgery.
In this article, we review the history of induced hypothermia in aortic surgery, mechanism of hypothermia-mediated neuroprotection, experimental animal studies, and clinical reports regarding hypothermia application in TAAA surgery. We conducted a PubMed search using keywords such as hypothermia, therapeutic hypothermia, systemic hypothermia, regional hypothermia, spinal cord ischemia, neuroprotection, TAAA surgery, aortic arch, and endovascular repair. We summarized the gathered information and presented in this article to reflect the current state of induced hypothermia in TAAA repair surgery.
History
Induced hypothermia has been the mainstay of spinal cord protection since the inception of aortic aneurysm surgery. Hypothermia has been shown to protect spinal cord function during periods of aortic occlusion in other experimental studies (Pontius et al., 1954; Owens et al., 1955; Parkins et al., 1955). Thereafter, regional hypothermia was proposed as a technique to prevent ISCI. In the early 1960s, Negrin and Klauber used iced saline perfusion through an epidural catheter to protect motor neurons during thoracic aorta cross-clamping (Negrin and Klauber, 1960). In 1975, Hansebout et al. used regional hypothermia to minimize damage and promote recovery after experimental spinal cord compression injury (Hansebout et al., 1975). In the early 1990s, several publications documented success with regional spinal cord cooling in animal models (Allen et al., 1994; Salzano et al., 1994). In 1993, Tabayashi et al. and Marsala et al. reported that epidural cooling was neuroprotective in a canine model of ISCI (Tabayashi et al., 1993; Marsala et al., 1993). Davison et al. evaluated this technique in a clinical study in 1994 and found that epidural cooling was effective in preventing ISCI in eight patients undergoing thoracic or TAAA repair (Davison et al., 1994). In 1995, Kouchoukos applied hypothermic bypass with circulatory arrest during descending thoracic and TAAA surgery (Kouchoukos et al., 1995).
Deep hypothermia was also used to protect the brain during aortic arch surgery (Griepp et al., 1975). In the 1980s, in addition to using systemic hypothermia, anterograde or retrograde cerebral perfusion was added as a supplement to the hypothermia brain protection strategy (Soma et al., 1982). Over the last 15 years in the clinic, many adjuncts have been introduced into the spinal cord protection protocols during TAAA repair, including CSF drainage, distal aortic perfusion, evaluation of motor-evoked potentials (MEPs) and sensory-evoked potentials (Safi et al., 1996; de Haan et al., 1997; Coselli and LeMaire, 1999; van Dongen et al., 2001; Coselli et al., 2002), sequential clamping, prevention of retrograde bleeding from segmental arteries, cardiovascular stability (Shimizu and Yozu, 2011), and imaging of the spinal cord blood supply (Nijenhuis et al., 2007). Still, systemic and/or regional induced hypothermia remains one of the most effective methods of neuroprotection in most cardiovascular surgery centers.
Mechanisms of Neuroprotection
Hypothermia interrupts several mechanisms of neuronal ischemic injury (Fig. 1), which include, but are not limited to, excitotoxicity, oxidative stress, gene expression, microRNA response, apoptosis, and inflammation.
Effects of hypothermia on metabolism
The relationship between cerebral metabolic rate and temperature was investigated in a number of experimental studies by Michenfelder (Michenfelder and Theye, 1968; Michenfelder and Milde, 1991, 1992). He found that hypothermia could affect the neurological functions through alteration of biochemical reactions in the neurons, in a complex relationship. On the other hand, Rosomoff and Holaday (1954) showed a linear relationship between cerebral oxygen consumption and a decrease in body temperature. Hypothermia slows the cellular metabolic rate by 5%–7% for every 1°C drop in body temperature (Michenfelder and Milde, 1992; Svyatets et al., 2010). It decreases glucose and oxygen consumption after reperfusion and maintains high levels of oxygen in the blood (Erecinska et al., 2003). Although high oxygen levels may pose a risk during reperfusion (Lin et al., 2008), oxygen is needed to maintain oxidative metabolism in neurons. Hypothermia also helps maintain cell membrane biophysics. This is accomplished by (1) minimizing or reducing intracellular Ca++ influx, which in turn limits mitochondrial dysfunction (Eguchi et al., 1997); (2) re-establishing K+ gradients (Sick et al., 1999); and (3) recovering Ca++/calmodulin-dependent protein kinase activity (Hu et al., 1995).
Effects of hypothermia on excitotoxicity
Because the synthesis and uptake of neurotransmitters are temperature-dependent processes, glutamate excitotoxicity could be mitigated by hypothermia (Kataoka and Yanase, 1998). Various animal studies have shown that key processes of excitotoxicity (e.g., accumulation of glutamate or its coagonist glycine) can be interrupted or blocked by hypothermia (Busto et al., 1989; Baker et al., 1991; Rokkas et al., 1995; Globus et al., 1995a; Winfree et al., 1996). On the other hand, Yamamoto et al. (1999) showed, in an experimental study, that neuroprotection effect induced by mild hypothermia cannot be linked to reduction of glutamate release. More research is needed to clarify this controversy.
Effects of hypothermia on oxidative stress
The inflammatory reactions that occur secondary to reperfusion injury are associated with enhanced generation of free radicals, such as reactive oxygen species, which cause DNA damage and induce apoptosis. Globus et al. (1995b) were the first group to show that free radical-induced neuronal injury can be interrupted by hypothermia. In fact, a linear correlation exists between reactive oxygen species production and temperature changes (Novack et al., 1996). Several studies have shown that hypothermia attenuates reactive oxygen species formation and protects cells from oxidative stress (Maier et al., 2002; Horiguchi et al., 2003).
Effects of hypothermia on gene expression
The neuroprotective mechanisms of hypothermia extend to modification of neuronal gene expression. Under hypothermic conditions, beneficial genes (cell survival and trophic genes) are upregulated (Boris-Moller et al., 1998; Vosler et al., 2005; Zhao et al., 2005), while proinflammatory and pro-apoptotic genes are downregulated or repressed (Xu et al., 2002; Van Hemelrijck et al., 2005). Such changes in gene expression could be linked to upregulation of cold shock proteins (Han and Yenari, 2007), or to specific transcription factors that are temperature sensitive (Hicks et al., 2000; Han et al., 2003). Temperature-dependent regulation of gene expression also has been documented in inflammatory cells. Sonna et al. (2006) found that several heat shock proteins (Hsps) were decreased in leukocytes exposed to moderate hypothermia (32°C for 24 hours). This could limit the function and survival of inflammatory cells responding to ischemia/reperfusion injury.
In our experience, ischemia reperfusion injury of spinal cord is associated with a significant increase in the Hsp70 level in the CSF of dogs after aortic cross-clamping (Awad et al., 2008). Whether hypothermia can reduce Hsp70 after spinal cord ischemia has not been tested in ISCI; however, according to data from a recent experiment in a model of cerebral ischemia, hypothermia was able to decrease Hsp70 protein and gene expression (Tirapelli et al., 2010).
Recently, the triangular relationship between microRNA, target gene expression, and hypothermia has been explored in a number of studies (Dresios et al., 2005; Pilotte et al., 2011; Truettner et al., 2011). Dresios et al. (2005) studied the effect of Rbm 3 expression (member of a small, highly conserved family of RNA) on global protein expression by changing the microRNA levels under normal and hypothermic conditions. In addition, Pilotte et al. (2011) found that alteration of microRNA expression by Rbm3 is a temperature-dependent process that can be added to the scope of hypothermia effect on cellular events. Truettner et al. (2011) showed that mild hypothermia (33°C) alters the microRNA response in a rat model of traumatic brain injury. These findings point to other underlying mechanisms of hypothermia-mediated neurprotection though microRNA. This will open a new field of research to further address the possibility of manipulating harmful microRNA expression by induced hypothermia.
Effects of hypothermia on apoptosis
Hypothermia can interrupt the apoptotic pathway, thereby preventing programmed cell death (Inamasu et al., 2000). In a rabbit model of spinal cord ischemia, hypothermia was shown to inhibit nerve cell apoptosis by altering expression of p53 (tumor suppressor protein) and Bcl-2 (apoptosis regulatory protein) (Wang et al., 2005). Hypothermia may also augment cell survival pathways mediated by ERK (extracellular signal regulated kinase) (D'Cruz et al., 2005), Akt (protein kinase B) (Zhao et al., 2005), and upregulation of the anti-apoptotic protein Bcl-2 (Prakasa et al., 2000; Zhang et al., 2001). Hypothermia can also increase expression of trophic factors (Boris-Moller et al., 1998; Schmidt et al., 2004). In experimental models of cardiac arrest, induction of hypothermia was associated with increased secretion of neutrophins, including glial-derived neurotrophic factor and brain-derived neurotrophic factor (Boris-Moller et al., 1998; D'Cruz et al., 2002; Vosler et al., 2005). Hypothermia may also inhibit other aspects of apoptosis, including cytochrome c release (Yenari et al., 2002), Fas (Phanithi et al., 2000), and activation of caspases (e.g., caspases 3 and 8) (Wang et al., 2000; Fukuda et al., 2001).
Effects of hypothermia on inflammation
Several studies have tested the ability of hypothermia to attenuate postischemic inflammation (Aibiki et al., 1999; Kimura et al., 2002; Dietrich et al., 2004). Hypothermia can delay neutrophil influx, suppress activation of microglia, and inhibit release of inflammatory mediators (e.g., cytokines) (Si et al., 1997; Ishikawa et al., 1999; Zheng and Yenari, 2004). In a recent in vitro study, hypothermia was shown to reduce microglial proliferation and downregulate expression of tumor necrosis factor-alpha and monocyte chemotactic protein-1, two proinflammatory mediators. Mild hypothermia was shown to inhibit IκB kinase, an enzyme responsible for phosphorylating IκBα, and an inhibitor of NFκB. Phosphorylated IκBα dissociates from nuclear localization sequences on NFκB, resulting in NFκB-dependent transcription and the onset of inflammatory gene transcription (Han et al., 2003). In addition, degradation of IκBα was reduced and delayed by hypothermia (Diestel et al., 2010).
Conversely, hypothermia can activate microglia, increasing their phagocytic capabilities and their ability to synthesize and release anti-inflammatory cytokines, including interleukin (IL)-1ra and IL-10 (Diestel et al., 2010). Previous studies have shown that IL-10 can protect neurons against glutamate excitotoxicity or ischemic/hypoxic injury (Dietrich et al., 1999; Bachis et al., 2001), and that the neurotoxic effects of IL-1 can be blocked by IL-1ra (Dinarello, 1997). Thus, hypothermia may actively induce neuroprotection via anti-inflammatory mechanisms (Hsieh et al., 2009).
Endothelial cells play a pivotal role in inflammation, acting as gatekeepers for circulating leukocytes. Moreover, maintenance of endothelial cell integrity is critical for minimizing blood–brain barrier injury, hemorrhage, and edema. Hypothermia has cytoprotective effects on endothelial cells. Six hours of mild hypothermia upregulates Bcl-2, a survival protein, and increases IL-6 secretion by endothelial cells (Diestel et al., 2008). Hypothermia also blocks the pro-apoptotic effects of tumor necrosis factor-alpha on human endothelia (Yang et al., 2010).
Induced Hypothermia in Experimental Studies of ISCI
We have recently reviewed the available data on various animal models that have been used for ISCI experimental studies in a book chapter “Animal Models of Spinal Cord Ischemia” (Animal Models in Spinal Cord Repair, edited by Hakan Aldskogius, M.D., Ph.D.). A consistent feature of most models is aortic cross-clamping that simulates the ischemic events that occur during TAAA repair. Different approaches and degrees of hypothermia were applied in some ISCI models to test the feasibility and efficacy of induced hypothermia as a tool of neuroprotection (Table 1).
ACC, aortic cross-clamping; CPB, cardiopulmonary bypass; G, group; iNOS, inducible nitric oxide synthase; SSEPs, somatosensory-evoked potentials;. Temp, temperature; Tarlov scores, scale for assessment of neurological motor function; CSF, cerebrospinal fluid; ISCI, ischemic spinal cord injury.
Mild systemic hypothermia
In a study in pigs, Strauch et al. (2004) were able to double the ischemic tolerance of the spinal cord by performing aortic cross-clamping with mild hypothermia (32°C). Neurological functions were intact in animals that underwent aortic cross-clamping for 50 minutes under mild hypothermia, while animals subjected to the same procedure under normothermic conditions developed paraplegia after 30 minutes of aortic cross-clamping. Interestingly, animals that were neurologically intact after 60 minutes of aortic cross-clamping with mild hypothermia did develop delayed onset paraplegia, suggesting that hypothermia slows rather than inhibits mechanisms of tissue injury.
Profound systemic hypothermia
Rokkas et al. (1993) studied the effect of profound hypothermia (15°C) on the neurological outcomes of a primate model of ISCI, in which systemic hypothermia was accomplished through cardiopulmonary bypass (CPB). They found that motor function was preserved in all animals subjected to 60 minutes of experimental ischemia with hypothermia. Animals that were subjected to the same ischemic insult under normothermic (37°C) conditions became paraplegic or paraparetic. Two years later, the same group used profound hypothermia (20°C) in an experimental study of ISCI in pigs to evaluate the effects of hypothermia on changing extracellular levels of excitatory neurotransmitters (Rokkas et al., 1995). Within 60 minutes of ischemia, the concentration of excitatory amino acids was significantly reduced compared to basal (nonischemic) levels in pigs that were hypothermic. In normothermic animals (37°C), excitatory amino acid concentrations remained high in the extracellular space even after reperfusion.
Systemic hypothermia and delayed paralysis
Recently, we developed a mouse model of ISCI in which aortic cross-clamping was performed under conditions of normothermia or systemic hypothermia (33°C). Using this approach, normothermic mice developed immediate paralysis after reperfusion, whereas mice maintained at 33°C during cross-clamping and reperfusion developed paralysis only after a delay of 40–48 hours (Awad et al., 2010). A similar model developed in an independent lab confirmed that aortic cross-clamping performed under normothermia (37.0°C±0.5°C) causes rapid (within 1 hour) hind limb dysfunction (Wang et al., 2010).
In a third model, Kang et al. (2010) studied the effect of hypothermia (34°C) on ischemia-perfusion injury in a mouse model of ISCI. At 24 hours before reperfusion, only mild and transient neurological deficit took place in mice subjected to ischemia under hypothermic conditions. However, at 48 hours, reperfusion delayed onset ISCI developed in half of the mice in the hypothermic group. In addition, they measured markers of systemic inflammation in various organs at 24 and 48 hours of reperfusion. There was no correlation between the neurological deficits and the inflammatory markers in other organs. The authors concluded that the delayed onset ISCI is due to a local event, not as a part of systemic inflammatory response to ischemia.
From these data in preclinical models, we conclude that hypothermia prevents or slows the early phase of ischemic injury through one or more of the mechanisms described above; however, it does not completely prevent delayed neuronal damage. Whether modification of the degree and duration of hypothermia can prevent delayed ischemic injury requires further investigation.
Regional hypothermia
On the topic of regional hypothermia in preclinical studies, Negrin and Klauber applied epidural cooling experimentally for the first time in 1960 to prevent ISCI during aortic cross-clamping (Negrin and Klauber, 1960). Thereafter, regional hypothermia was applied in different experimental studies by perfusion of cold blood or crystalloids into the segmental vessels supplying the spinal cord (Coles et al., 1983; Colon et al., 1987; Allen et al., 1994), or by infusion of iced saline into the subarachnoid (Berguer et al., 1992; Wisselink et al., 1994), or epidural space (Marsala et al., 1993; Tabayashi et al., 1993; Vanicky et al., 1993; Gonzalez-Fajardo et al., 1996). To identify the optimal temperature for spinal cord protection, Martelli et al. (2002) cooled rabbit spinal cords to different degrees via epidural infusion of cold saline. Cooling the spinal cord to 17°C, 24°C or 32°C prevented neurological deficits after 40 minutes of induced ischemia, while infusion of saline at 39°C resulted in paralysis. Histological examination revealed complete necrosis of the anterior horn cells in the spinal cord with epidural cooling at 39°C and incomplete necrosis at 34°C. No histophatologic changes were observed with EC at 17°C and 24°C.
Clearly, additional work is needed in preclinical models to optimize protocols for neuroprotective hypothermia. For example, comparative studies are needed in clinically relevant (large animal) models in order to compare the efficacy of systemic (mild, moderate, and profound) versus regional (infusion of cold blood into vessels supplying spinal cord, or infusion of iced saline into the epidural space or the subarachnoid space) hypothermia with and without mechanical support. In summary, studies of this type should reveal the safest and most efficacious induced hypothermia protocols and should lead to newer institutional strategies to prevent paralysis after TAAA repair surgery.
Induced Hypothermia in TAAA Repair Surgery
The trend of paraplegia incidence after TAAA has significantly declined over the last 25 years, especially after incorporating hypothermic perfusion with CSF drainage along with increasing arterial perfusion and use of neurochemical protection (Shimizu and Yozu, 2011). The observed/expected (O/E) ratios of paraplegia decreased in most clinical reports from ∼1 to 0.25 or less in the last decade (Acher and Wynn, 2010). Over the past 40 years, the Baylor Vascular Center in Houston has reported a progressive decline in the paraplegia rate from 16% (O/E 1.0; ∼1960–1970s) to ∼3.8% (O/E 0.22) (Svensson et al., 1993; de Haan et al., 1997; Coselli et al., 2008). A similar reduction also has been reported in other vascular surgery centers. For example, since the introduction of these strategies in the mid-1980s, the paraplegia rate at University of Wisconsin decreased from 25% (O/E 1.04) to 3.3% (O/E 0.18) (Acher and Wynn, 2010).
Despite these advances, ∼22% of patients undergoing type II repair (type II includes aneurysms involving most of the descending thoracic and most of the abdominal aorta) still become paraplegic (Greenberg et al., 2008). Those patients suffer from severe long-term physical disability and have a shorter lifespan (Svensson et al., 1993). Since 1956 when DeBakey first completed a successful TAAA repair with an aortic homograft, many adjunct therapies have been used to minimize ISCI (Creech et al., 1956). The basic approach to protect the spinal cord has been to facilitate distal aortic perfusion during aortic cross-clamping with a temporary shunt. This passive perfusion approach has since been replaced with active CPB. Other adjuncts include the use of (1) preoperative spinal angiography, (2) reattachment of the intercostal artery, (3) CSF drainage, (4) increasing ischemic tolerance with pharmacological adjuncts (e.g., naloxane, steroids, and barbiturates), (5) monitoring of somatosensory and MEPs, and (6) hypothermia. The remainder of this review will focus on using hypothermia as a critical component of the spinal cord protection protocol. There are two approaches for spinal cord cooling during TAAA surgery, regional and systemic cooling.
Systemic Hypothermia
Technique and approach
Systemic hypothermia can be induced through CPB and temperature can be mild (32°C–35°C), moderate (28°C–32°C), deep (20°C–28°C), or profound (15°C–20°C). With regard to organ protection during aortic surgery, two methods are commonly used: hypothermic circulatory arrest and left heart bypass. For hypothermic circulatory arrest, after induction of anesthesia, femoral vessels are exposed and systemic heparinization is achieved. A long catheter is introduced through the femoral vein and advanced to settle in the right atrium for venous blood drainage under transesophageal echocardiography guidance. The femoral or external iliac artery is the route for the arterial inflow cannula. Other sites for arterial cannulation can be used, such as aortic arch or subclavian artery, in case of extensive atherosclerosis of the femoral or iliac arteries. Once femoral vessels are cannulated and connected to the CPB machine, cooling of the blood starts by indirect contact with cold water (Safi et al., 1998; Kouchoukos et al., 2001). Once the target temperature is reached, the CPB is suspended and the aortic replacement will be done in a bloodless field.
To avoid the systemic drawbacks of deep hypothermia, the surgeon can use the left heart bypass technique. This technique includes using a centrifugal pump to circulate the blood in a closed circuit without using an oxygenator or a warming device. A cannula is introduced into the left atrium via inferior pulmonary vein for draining the blood, and blood is then returned to the distal thoracic aorta or the femoral artery through another cannula (Coselli et al., 1996; Coselli et al., 2004). Using the left heart bypass technique, patient core temperatures fluctuate between 32°C to 34°C (Wong et al., 2011). This approach does not require full heparinization, which avoids the synergism between hypothermia and anticoagulation.
Complications and limitations of systemic hypothermia
Despite the protective effects of systemic hypothermia, the procedure has side effects, including pulmonary dysfunction, generalized edema, and cardiac arrhythmia (Schubert, 1995; Ogino, 2010). Hypothermia causes coagulopathy through reversible platelet dysfunction, enhanced fibrinolytic activity, and slow enzymatic activity required for clotting (Rohrer and Natale, 1992). Moreover, using CPB for induced hypothermia requires full heparinization, which increases the risk of bleeding along with the coagulopathy caused by hypothermia (Okita, 2011). In addition, an increase in the incidence of infection at wound sites has been reported with systemic hypothermia application (Beltramini et al., 2011). This likelihood of infection can be attributed to impaired leucocytes migration, phagocytosis, and bactericidal oxidative burst activity (van Oss et al., 1980; Wenisch et al., 1996).
Regional Cooling
Technique and approach
Regional cooling was introduced as a way to avoid the complications associated with systemic cooling. The day before the surgery, an epidural catheter is inserted at the level of T11–T12 and advanced cranially under radiological guidance. Therefore, regional cooling of the spinal cord is usually accomplished via infusion of iced saline (4°C) into the epidural space through the catheter connected to a transfusion pump. Infusion is started 30 minutes before cross-clamping at a rate of 3–5 mL/min. This interval is important to reach the target temperature of CSF (25°C–28°C). Initial increase of CSF pressure occurs with starting the epidural infusion. Thereby, a gradient of (≈40 mmHg) is kept between the mean arterial pressure and the CSF pressure to maintain the cord blood perfusion. During the cross-clamp procedure, iced saline infusion rate is maintained at 0–7 mL/min then is discontinued at the end of the procedure. During cooling, CSF temperatures range from 25°C to 28°C with no significant change in body temperature and infusion of mean volume 489 mL (range 80–1700 mL) of iced saline solution. Another catheter is introduced into the subarachnoid space for CSF drainage and pressure measurement (checked every 5 minutes by a medical engineer). Epidural cooling is discontinued after re-anastomosis of critical arterial supply to the cord is achieved (Davison et al., 1994; Motoyoshi et al., 2004).
Complications and limitations of regional cooling
Although effective, regional cooling can increase CSF pressure, which can impair spinal cord perfusion (Meylaerts et al., 2000; Yoshitake et al., 2007). In a large cohort of patients (n=102) undergoing TAAA repair surgery, Tabayashi et al. (2010) reported that high CSF pressure during EC epidural cooling was associated with proximal center cord syndrome in two out of four patients who developed ISCI. However, the authors were not able to determine a mechanism of increased CSF pressure in these four patients whether it was due to a mechanical issue related to the catheter insertion, rate of infusion or anatomical variations within the epidural space among these four patients.
This potential drawback of regional cooling can be controlled by CSF drainage or epidural fluid drainage (Cambria et al., 1997, 2000). However, insertion of a second epidural catheter for drainage might be difficult with the high flow rate of saline infusion that is required to reach the targeted spinal cord temperature. In such clinical situations, the mean spinal cord perfusion (mean arterial pressure−mean CSF pressure) can be improved by manipulating the cold saline infusion rate or increasing the systemic pressure (Black et al., 2003). Figure 2 shows techniques of the epidural cooling system used by Massachusetts General Hospital.
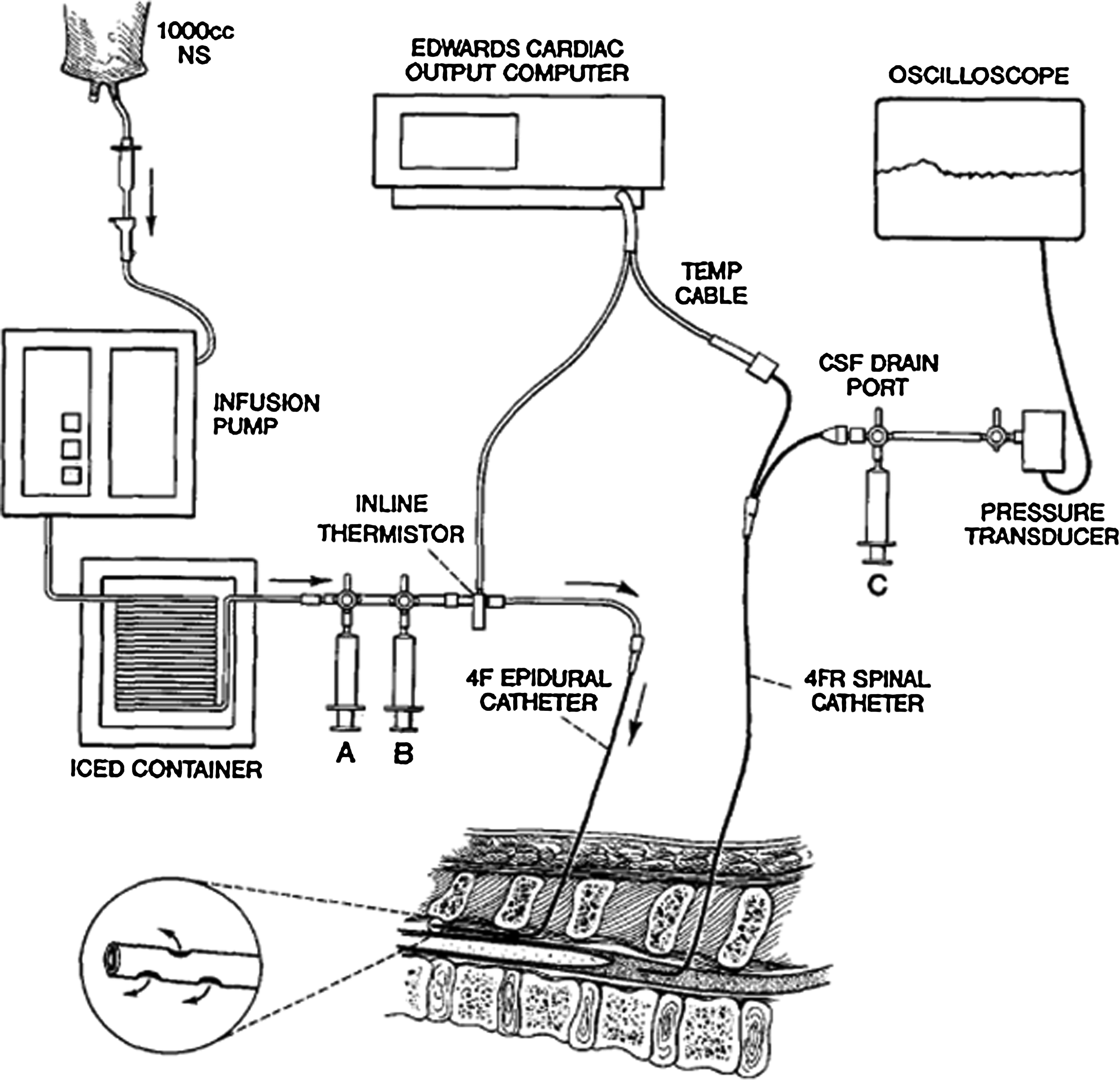
Equipment setup for epidural cold infusion and measurement of CSF temperature and pressure. Syringe A: local anesthesia; syringe B: blousing and removing infusate; and syringe C: CSF drainage. CSF, cerebrospinal fluid. Reprinted from Dennison et al. (1994), with permission from Elsevier.
CSF temperature is measured during epidural cooling as an indicator of temperature within the spinal cord parenchyma. This makes it difficult to take an accurate measurement of spinal cord temperature (Ogino, 2010). This makes homogeneous cooling uncertain and could affect the clinical outcome.
The Effects of Induced Hypothermia on Electrophysiological Monitoring
Induced hypothermia affects the reliability of evoked potentials monitoring in detecting ISCI during aortic cross-clamping. MEPs and somatosensory evoked potentials (SSEPs) are used in some aortic surgery centers for monitoring spinal cord function during TAAA repair surgery (Shine et al., 2008; Keyhani et al., 2009). MEPs are recorded from limb muscles after trans-cranial electrical stimulation of the motor cortex with electrodes placed on the scalp. SSEPs are recorded from the scalp after stimulating the peripheral nerves. The function of spinal cord anterior columns can be assessed with MEPs while SSEPs can be used to evaluate posterior column function.
Recently, the reliability of neurophysiologic monitoring during TAAA surgery was debated (Coselli and Tsai, 2010; Koeppel et al., 2010). Because hypothermia can decrease nerve conduction velocity that will slow transmission of nerve impulses across synapses, an increase in the latency of cortical-evoked potentials is expected (Katz and Miledi, 1965; Benita and Conde, 1972; Ludin and Beyeler, 1977; van Rheineck et al., 1986). In addition, decreasing spinal cord temperature could diminish signal amplitude, which would require an increase in the stimulation threshold. Collectively, the adverse effects of hypothermia on these physiological variables could conceivably make MEPs/SSEPs monitoring difficult if not unreliable (Seyal and Mull, 2002; Wang et al., 2009; Coselli and Tsai, 2010).
However, the monitoring of MEPs was shown to be useful for alerting the surgical team about impending spinal cord damage. Using MEPs along with other adjunct therapies (e.g., CSF drainage and bypass grafting), one group was able to reduce the risk of paralysis after TAAA surgery to <3% (Jacobs et al., 2002). This same group also found no adverse affect of moderate hypothermia (28°C) on monitoring MEPs in a pig model of ISCI (Jacobs et al., 2002). However, profound cooling (14°C) markedly reduced the amplitude of MEPs and increased the latency. From these data, it was concluded that MEP monitoring becomes unreliable when CSF temperatures are below 25°C (Meylaerts et al., 1999).
In a preclinical cat model of ISCI, Browning et al. (1992) also noted an effect of temperature on evoked potentials. Specifically, the amplitude of MEPs increased at 28°C, while a significant increase in SSEP amplitude occurred at 34°C. The latency of both evoked potentials increased at 28°C. This group also recommends that, in addition to temperature, anesthetics and arterial CO2 partial pressure should be considered when monitoring-evoked potentials. The need for expert individuals to monitor each of these physiological variables, in addition to monitoring and interpreting evoked potentials, likely explains why monitoring of evoked potentials is not a common practice in all aortic surgery centers.
In a clinical series reported from Mayo Clinic, Shine et al. (2008) evaluated the sensitivity and specificity of evoked potential monitoring in predicting the neurological outcomes of 58 patients who underwent TAAA repair surgery. Epidural cooling was applied to reach CSF temperature 26°C–28°C. Ten patients developed paraplegia after surgery. By conducting comparative analysis of the 10 paraplegic patients' data and the remaining data from the 48 patients without paraplegia, the investigators found that the sensitivity of MEPs monitoring in predicting ISCI was 88%, while the specificity was 65%. The negative predictive value of MEPS at 20 minutes after aortic cross-clamping was 96%. Also, they reported that during aortic cross-clamping, the signal was lost after 10 minutes in patients with paraplegia and 31 minutes in patients without paraplegia. They concluded that the chances of developing paraplegia are low when an MEP signal is present and that loss of an MEP shortly after aortic cross-clamping is a sign of impending paraplegia (Shine et al., 2008).
MEP monitoring may also be useful for revealing the hemodynamic significance of collateral blood supply to the spinal cord. Takahashi et al. showed that segmental cold blood infusion, which accelerates a decline in MEPs, is useful for determining when specific arteries need to be reconstructed (e.g., artery of Adamkiewicz). This technique was found to minimize reconstruction time and limit spinal cord damage (Takahashi et al., 2011).
Neurological Outcomes of TAAA Surgery with Hypothermia Application
Systemic hypothermia
Several clinical studies have reported the effectiveness of hypothermia in decreasing the risk of spinal cord injury during TAAA repair over the last 20 years (Table 2). A linear correlation seems to exist between temperature reduction and ischemic tolerance of the spinal cord (Hollier, 1987). Von Segesser et al. (2001) studied the direct impact of systemic hypothermia on the clinical outcomes in 100 patients undergoing TAAA repair surgery. Partial CPB with normothermic perfusion (36°C) was applied in 52 patients, and hypothermic perfusion (28°C) was applied in 48 patients. Application of hypothermia allowed more cross-clamping time, which enabled the surgical team to perform more complex repairs. Mortality, paraplegia, and surgical revision were all significantly reduced in the hypothermic group.
EC, epidural cooling; HA, hypothermic arrest; MAP, mean arterial pressure; O/E, observed/expected; SFD, spinal fluid drainage; TAA, thoracic aortic aneurysm; TAAA, thoracoabdominal aortic aneurysm.
Carrel et al. (2000) compared the effects of deep hypothermia (18°C) with a period of circulatory arrest and moderate hypothermia (33°C) with left heart bypass during TAAA repair. Paraplegia incidence was 8.8% in the moderate hypothermia group, while it was 2.6% in those individuals provided with deep hypothermia. With deep hypothermic circulatory arrest, it was also easier to identify the dissection tear site in the proximal aorta with a bloodless field and without an aortic clamp. They attributed the differences in the outcomes to the easier surgical access to all segments of the aorta, the biochemical effect of deep hypothermia on the extracellular excitatory amino acids release, and reduction of CSF lactate production.
These two studies examined the effect of normothermia versus hypothermia and which degree of hypothermia has a better outcome with regard to ISCI and paralysis. However, the optimal temperature management strategy is not clearly defined, and there is no agreement among different surgical teams about the ideal range of induced hypothermia to balance the risk–benefit ratio. Clinical trials should be directed to further investigate the optimum temperature management.
Regional cooling
Epidural cooling was introduced for the first time in TAAA repair surgery by Davison et al. (1994) at Massachusetts General Hospital in Boston. They successfully applied epidural cooling in eight patients undergoing TAAA repair with no incidence of postoperative neurological dysfunction. Since then, this same group reviewed the clinical outcomes of 445 cases of TAAA repair between 1998 and 2007 with epidural cooling applied in 240 TAAA surgeries for spinal cord protection. The overall incidence of ISCI was 13.2%, with 9.5% patients developing major paraplegia. They reported that when epidural cooling was applied during TAAA repair, the risk of ISCI was significantly reduced compared to cases without epidural cooling (13.2% with epidural cooling vs. 29% without epidural cooling; p=0.01) (Conrad et al., 2007).
The epidural cooling technique was also used at the Mayo Clinic in a consecutive series of 58 patients who underwent TAAA repair surgery between 1998 and 2000 (Shine et al., 2008). MEPs and SSEPs also were used to monitor spinal cord function during aortic cross-clamping. The ISCI incidence after surgery was 17.2% in this clinical series.
In Japan, a leading surgical team compared the ISCI incidence in 38 patients who had TAAA repair with mild hypothermia alone (33°C) and 78 patients with mild systemic hypothermia, epidural cooling, and CSF drainage. The incidence of ISCI was 16.2% in patients receiving only mild hypothermia; however, it was reduced to 3.8% in those receiving mild hypothermia with epidural cooling and CSF drainage (Tabayashi et al., 2008).
In 2008, the epidural cooling technique was applied for the first time in Germany in a small group of patients (Tschop et al., 2008). They reported no paraplegia in all seven patients after TAAA repair surgery; however, three patients died from other comorbidities.
Clinical considerations (systemic vs. regional cooling)
The application of induced hypothermia for spinal cord protection in TAAA repair varies between major aortic surgery centers. Some surgeons recommended profound hypothermia with circulatory arrest, while others prefer moderate hypothermia with left heart bypass (Borst et al., 1994; Okita et al., 1997; Carrel et al., 2000; Kouchoukos et al., 2001). The choice of approach and technique is based mainly on the preference and experience of the operating team as well as the extent of the aneurysm. Although deep hypothermic circulatory arrest is used in many aortic surgery centers (Grabenwöger et al., 1994; Kouchoukos and Rokkas, 1999; Carrel et al., 2000; Fehrenbacher et al., 2007), some surgeons recommend using this technique only in the following situations: aneurismal involvement of the aortic arch, extensive atherosclerosis of the aorta which makes aortic cross-clamping hazardous, and catastrophic bleeding intraoperatively due to the side effects of deep hypothermic circulatory arrest on the whole body (Coselli et al., 1996; Safi et al., 1998; Wong et al., 2011).
Epidural cooling is a newer and more complex approach requiring insertion of an epidural cooling catheter, constant monitoring of CSF pressure and maintenance of a gradient between the nasopharyngeal temperature and the CSF temperature. Accordingly, it is not as widely used as systemic hypothermia for multiple reasons. It is technically demanding, requiring additional skilled personnel and the rate of paralysis is not lowered compared to centers using systemic hypothermia. The incidence of ISCI is high in centers that are attempting to adopt this technique (Shine et al., 2008; Tschop et al., 2008). On the other hand, in centers that routinely use epidural cooling, it has been shown to effectively reduce ISCI incidence with fewer complications associated with systemic hypothermia (Conrad et al., 2007; Tabayashi et al., 2008; Tabayashi et al., 2010).
In general, induced hypothermia, systemic or regional, plays a beneficial role in protecting the spinal cord during ischemic injury. However, clinical application of either systemic or regional hypothermia was not successful in eliminating the ischemic injury.
Induced Hypothermia in Aortic Arch Surgery
There is an ongoing debate about whether deep hypothermia or moderate hypothermia with selective antegrade cerebral perfusion should be used for brain and spinal cord protection during aortic arch surgery. A recent editorial argues that prolonged selective antegrade cerebral perfusion with moderate hypothermia might not be enough to protect the spinal cord during aortic arch repair surgery (Ranasinghe and Bonser, 2009). The authors suggest performing a multi-center study with appropriate stratification for aortic pathology and extent of repair instead of relying on retrospective reports with missing data, era effects, learning curves or animal studies (Ranasinghe and Bonser, 2009). We agree with this position of the editorial.
Endovascular Repair
Recent advances in endovascular repair are being applied to the treatment of aortic aneurysm diseases. Initially, endovascular repair was limited to infra-renal or descending thoracic aortic aneurysm (TAA) patients, that is, those patients at high risk for open surgery (Greenberg and Lytle, 2008). However, the development of fenestrated and branched aortic endografts has allowed endovascular therapies to be used in more extensive TAAA surgeries. Still, even with this less invasive approach, spinal cord injury remains a risk. The incidence of spinal cord injury after endovascular repair of TAA is 2%–10% (Dake et al., 1998; Greenberg et al., 2005; Makaroun et al., 2005; Eagleton and Greenberg, 2010). In a clinical report from the Cleveland Clinic, the incidence of ISCI was found to decrease after endovascular repair by ∼3% compared to open surgical repair (4.3% endovascular repair vs. 7.5% surgical repair, p=0.08) (Eagleton and Greenberg, 2010).
The ISCI during endovascular repair could be attributed to several factors, such as immediate ischemic injury from occlusion of critical intercostal arteries, episodes of hypotension, or loss of collaterals needed for maintaining spinal cord perfusion. Coverage of critical intercostal arteries by the stent does not result in immediate occlusion because these arteries can maintain blood flow through collaterals, which is sometimes evident as an endoleak. Delayed thrombosis of these intercostal arteries due to low blood flow with resolution of the endoleak could be another mechanism of delayed ischemic injury. Visceral ischemia also can develop during endoaortic abdominal repair and could increase the release of inflammatory mediators with subsequent secondary spinal cord ischemia (Carroccio et al., 2003).
Endovascular techniques seem to be a promising alternative for the conventional open TAAA repair; however, the prospect of causing spinal cord injury is still of great concern. Identification of critical intercostal vessels, maintenance of interoperative arterial blood pressure, CSF drainage, and neuroprotective drugs have been incorporated as protective measures to minimize ISCI during endovascular repair (Greenberg and Lytle, 2008; Eagleton and Greenberg, 2010). To date, regional hypothermia has not been tested before as an adjunct to endovascular therapy in a systematic way.
As we have described above, several reports have used induced hypothermia to prevent spinal cord dysfunction in animal models and/or in patients undergoing open surgery repair. Application of systemic or regional hypothermia in endovascular repair should be evaluated in further experimental and clinical studies so that ISCI incidence will be markedly reduced in this minimally invasive technique.
In a recent study, the performance of the prosthetic grafts used in endovascular repair was tested under hypothermic conditions (in vitro) (Robich et al., 2012). These grafts showed significant reduction in the radial expansion and deployed diameter at or below 30°C. Failure of full expansion of the endografts may lead to serious complications such as migration or endoleak. Special attention should be given to cases undergoing endovascular repair of TAA or TAAA by using these prosthetic grafts under hypothermic conditions.
Conclusions and Future Directions
Despite marked advances in the surgical treatment of TAAA and a general decline in rates of paraplegia across most vascular surgery centers (Acher and Wynn, 2010), paraplegia and paraparesis remain devastating postsurgical complications. Hypothermia is an effective neuroprotective therapy capable of limiting histological and neurological deficits caused by ISCI in diverse experimental models and clinical settings. Hypothermia not only reduces the metabolism and energy requirements of neurons, it also interrupts the ischemic injury cascade at the cellular and molecular levels through alteration of gene expression and protein synthesis in neurons, glia and inflammatory leukocytes. Still, more research is needed to fully understand the cellular and molecular mechanisms of neuroprotection afforded by hypothermia. This increased knowledge will help researchers and clinicians to develop more effective interventions against ISCI.
Regarding the area of endovascular repair, there are no randomized controlled clinical trials that targeted the temperature management for spinal cord protection. Furthermore, the relationship between temperature management, synthetic grafts durability, and endoleak needs further research.
Recently, drug therapeutics such as cannabinoids were shown to induce hypothermia and have organ protection effects which could synergize with or potentially replace systemic and regional hypothermia (Tisherman, 2010). Looking to the future, it might be feasible to simulate the effects of hypothermia using pharmacological agents that induce a poikilothermic state in the nervous tissue and avoid the side effects of physical hypothermia.
Footnotes
Disclosure Statement
All authors declared that no competing financial interests exist.