
Abstract
Background:
The use of therapeutic hypothermia (TH) is a burgeoning treatment modality for post-cardiac arrest patients.
Objectives:
We performed a retrospective chart review of patients who underwent post-cardiac arrest TH at eight different institutions across the United States. Our objectives were to assess how TH is currently being implemented in emergency departments and to examine the feasibility of conducting TH research using multi-institution prospective data.
Methods:
A total of 94 cases were identified in a 3-year period and submitted for review by participating institutions of the Peri-Resuscitation Consortium. Of those, seven charts were excluded for missing data. Two independent reviewers performed the data abstraction. Results were subsequently compared, and discrepancies were resolved by a third reviewer. We assessed patient demographics, initial presenting rhythm, time until TH initiation, duration of TH, cooling methods and temperature reached, survival to hospital discharge, and neurological status on discharged.
Results:
The majority of cases had initial cardiac rhythms of asystole or pulseless electrical activity (55.2%), followed by ventricular tachycardia or fibrillation (34.5%). The inciting cardiac rhythm was unknown in 10.3% of cases. Time to initiation of TH ranged from 0 to 783 minutes with a mean time of 99 minutes (SD=132). Length of TH ranged from 25 to 2,171 minutes with a mean time of 1,191 minutes (SD=536). The average minimum temperature achieved was 32.5°C, with a range from 27.6°C to 36.7°C (SD=1.5°C). Of the 87 charts reviewed, 29 (33.3%) of the patients survived to hospital discharge.
Conclusion:
The implementation of TH across the country is extremely varied with no universally accepted treatment. While our study is limited by sample size, it illustrates some compelling trends. A large, prospective, multicenter trial or registry is necessary to elucidate further the optimal parameters for TH and its benefit in various population subsets.
Introduction
Over the past decade, the use of therapeutic hypothermia (TH) has gained prominence as an intervention that could potentially improve patient outcomes. Two major trials introduced the concept of TH in the management of cardiac arrest. Bernard et al. found a significant neuroprotective effect from TH, with an odds ratio for favorable outcome of 5.25, while the Hypothermia After Cardiac Arrest study group reported an odds ratio of 1.5.4,5 A subsequent meta-analysis found similar results with an odds ratio of 1.68 (95% CI: 1.29–2.07). 6 While the precise mechanism of action of TH remains unclear, it is postulated that the act of cooling a patient after cardiac arrest may reduce tissue oxygen demand and diminish the production of inflammatory cytokines and stress, thereby preserving neurological and cardiac function.4,5,7–17
Since these original publications, the implementation of and research on TH has grown tremendously. In 2005, the American Heart Association published their Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care, advocating that unconscious adult patients with ROSC after out-of-hospital cardiac arrest should be cooled to 32–34°C for 12–24 hours. 18 In 2008, an ILCOR consensus statement from the International Liaison Committee on Resuscitation also recommended that patients with ROSC after out-of-hospital ventricular fibrillation (VF) arrest should be cooled to 32–34°C for at least 12–24 hours, and that induced TH may also benefit patients with out-of-hospital arrest secondary to other rhythms. 14 Since that time, several studies have documented successful implementation of TH with a morbidity and mortality benefit.19–21
While there have been several documented successes with TH, the precise clinical implications of the treatment remain unclear. There is no universal protocol for TH implementation and methods vary widely with regard to means of cooling and duration, drugs used for shivering and sedation, and goal temperature to be achieved. 22 The aim of our study was to characterize the current methods of TH used in various institutions across the United States.
Methods
Both in-hospital and out-of-hospital cardiac arrest patients with ROSC were included in this study. Institutional Review Board approval was obtained and all charts were de-identified by the home institution prior to submission for review.
The chart review and data abstraction were performed by two independent reviewers. Any discrepancy was resolved by a third independent reviewer. Paramedic run sheets, emergency department (ED) charts, and data from the intensive care unit stay were included in the analysis. Charts were assessed for patient demographics, initial presenting rhythm, time until TH initiation, duration of TH, cooling methods used, and minimum temperature reached. We opted to use time from ED arrival to initiation of TH as our metric of comparison because many of the EMS run sheets reported unknown time of arrest, and 25 of the arrests were unwitnessed with unknown downtime.
The primary outcome was survival to hospital discharge. Given the limitations of our data set and the variable reporting of neurological function in the charts, we were not able to identify a uniform method to assess neurological outcome.
We used one-sample t-tests to evaluate our data. Data analysis was performed using SPSS Statistics software. Institutions contributing charts included the University of Southern California, Advocate Christ Medical Center, Cook County Hospital, University of California at Davis, Highland General Hospital, Shands Jacksonville Medical Center, York Hospital, and the University of Nevada at Las Vegas. Information regarding these institutions can be found in Table 1 above.
Results
Participating institutions from the Peri-Resuscitation Consortium contributed a total of 94 charts from between 2008 and 2011 for this review. Of the charts reviewed, seven were excluded for missing data, leaving a total of 87 charts in the final analysis. Patient demographics are detailed in Table 2. Most significantly, the majority of patients (55.2%) presented with an initial rhythm of asystole or pulseless electrical activity (PEA). In 34.5% of patients, the presenting rhythm was ventricular fibrillation (VF) or ventricular tachycardia (VT), and the final 10.3% had an unknown initial rhythm (Table 3). Time from ED arrival until TH initiation varied widely, with a range of 0–783 minutes and a mean of 99 minutes (SD=132 minutes). Similarly, length of time of TH was non-uniform, with an average cooling time of 1,191 minutes (19 hours 51 minutes) and a range of 25–2,171 minutes (SD=536 minutes). The majority of patients (54%) were cooled for between 1,201 and 1,800 minutes. The mean nadir temperature reached was 32.5°C (SD=1.48°C). Cooling measures included ice packs, cooling blankets, catheter-based cooling systems, and cold saline. One third of the patients (33.3%) survived to hospital discharge (Table 3).
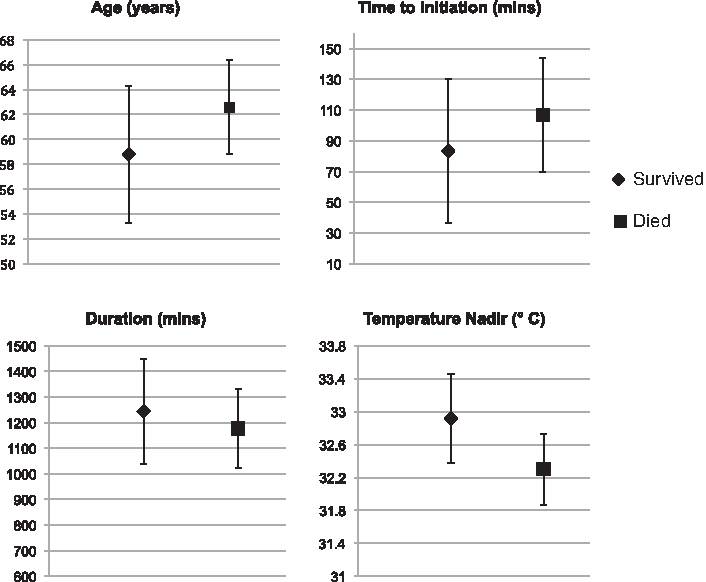
Of those patients who survived, the mean age was 58.8 (95% CI: 53.3–64.4) compared to a mean age of 62.6 (95% CI: 58.8–66.4) in those who died. The mean time to initiation of TH was 83.3 minutes (95% CI: 36.4–130.2) for those who survived and 106.9 minutes (95% CI: 69.8–144.0) for those who died. In those who survived to hospital discharge, mean duration of TH was 1244 minutes (95% CI: 1,038.5–1,449.4) and was 1,176.8 minutes (95% CI: 1,023.8–1,329.9) in those who died. The nadir temperature reached was 32.9°C (95% CI: 32.4–33.5) in survivors and 32.3°C (95% CI: 31.9–32.7) in those who died (Table 4, Fig. 1). Further details on survival by demographic can be seen in Table 5.
Survival.
Discussion
Our study highlights the current variability in the implementation of TH protocols across the country. Although the benefits of TH are generally accepted, the parameters and methods of cooling remain undecided. 23 Our data also shows some compelling trends that should be elucidated further in a larger prospective study. As might be expected, our data suggest that younger age and initial rhythm of VF or VT may confer a survival benefit, while older age, initial rhythm of asystole, and lower temperature nadir may be associated with a worsened outcome. The benefit seen in VF is likely secondary to the ability to defibrillate patients with relative success.24,25 The trend seen of lower nadir temperature and worsened outcome may be secondary to the side effects seen with excessive cooling, such as impaired coagulation, impaired immune response, cardiac arrhythmia, hyperglycemia, and other electrolyte disorders. 26 Alternatively, cooling may have been less aggressively pursued or less tightly monitored in those patients who seemed to be recovering neurologically after TH onset. Finally, average duration of cooling was also longer in survivors versus non-survivors. This could be due to a survival benefit of TH of longer duration, or due to confounders such as sicker patients not surviving the full 24 hours. While all these findings hint at possible approaches to standardized implementation of TH, our study is limited by our small sample size and is thus underpowered to make statistically significant conclusions.
We specifically identified several aspects of TH implementation that seemed to vary significantly by institution. Most surprisingly, the length of hypothermia seemed to vary widely among and within institutions, often falling outside of the 12–24 hours recommended by national guidelines. The two seminal studies on TH utilized cooling time targets of 12 and 24 hours respectively, with improvements in neurological outcome and mortality, and as a result the AHA guidelines that followed these studies recommend a target TH length of 12–24 hours.4,5,18 As mentioned above, we observed cooling times ranging from 25 minutes to slightly over 36 hours. In most instances where cooling was halted before 24 hours, the cause was an unstable patient or a family opting to withdraw care. However, we also noted instances where there the cessation of cooling seemed to result from a lack of inter-physician communication or from complications initiating the protocol. We noted several cases where a patient was started on TH in the ED. However, once the patient arrived in the ICU, cooling was halted without explanation.
In addition to duration of hypothermia, we also noted significant variation in time to initiation of TH. Mean time from ED arrival to initiation was 99 minutes. However, the standard deviation was 132 minutes. A portion of this variability can be explained by prolonged resuscitation, charting limitations, and so on. However, in several instances, TH was not initiated until several hours after hospital arrival. This further reiterates the need for clear protocols. No specific parameters exist for time to target temperature, but most protocols in the United States seem to specify initiation within 1 hour of ROSC.18,27 While several studies have shown no relationship between onset of TH and survival, two animal studies have shown that intra-arrest initiation of hypothermia may improve cardiac function and overall survival, and the induction of TH by paramedics is in the early stages of study and practice.28–31 Further, a multicenter, randomized control trial of EMS-initiated TH is currently underway. 30
In our data set, we also noted significant variation in methods used to induce cooling. We felt that this was less significant, as there are a multitude of options available for cooling and none have yet been shown to be superior, each having unique advantages and disadvantages.32–34 For instance, Tomte et al. compared intravascular and surface cooling devices in 167 patients and found no differences in mortality or neurological outcome. 33 With so many options and limited data thus far, institutions are choosing cooling devices that fit within their individual cost, staffing, and monitoring situations. A comparison of several common cooling systems is shown in Table 6.
Limitations
Our study is limited by sample size and retrospective study design. Further, because the chart review was retrospective, many of the charts did not clearly identify the parameters we hoped to measure. For instance, given the limitations of prehospital data, we were unable to document time from cardiac arrest until ROSC reliably. Further, as discussed above, we were unable to document neurologic outcome reliably.
Conclusion
Cardiac arrest continues to be a significant public health concern, and TH is currently the only modality that has been shown to improve neurologic outcome in survivors of cardiac arrest. Despite national guidelines, multiple barriers exist in the uniform implementation of TH. Specifically, the implementation parameters of TH are varied across the United States. This may be a result of limited data in the literature and a lack of consensus about the selection of patients and application of therapy. The optimal cooling techniques for induction, maintenance, and reversal of TH have yet to be described and validated. Although advances in technology and availability of new products have made the process of inducing and maintaining TH easier to achieve, there are limited data comparing the use of specific products.
Additionally, post-cardiac arrest care is multidisciplinary and requires the cooperation of multiple departments and healthcare providers. Our findings emphasize the need for clear, well-established hospital-wide protocols to address interprofessional barriers.
Further research is necessary to determine the optimal parameters for TH. As our sample size was too small to make specific parameter recommendations beyond those already published, a large, prospective, multicenter, randomized clinical trial or registry is warranted to study the effect of TH on patient-oriented outcomes.
Footnotes
Disclosure Statement
Dr. Kulstad's spouse is equity holder in a medical device start-up for patient temperature management.