
Abstract
The survival rate among patients admitted to hospital after out-of-hospital cardiac arrest (OHCA) was generally poor. And the optimal hospital care for patients after OHCA is not exactly known because multiple organ systems are affected. We implemented comprehensive packages of postcardiac arrest care, including therapeutic hypothermia (TH) to improve outcomes in patients with successfully resuscitated from OHCA. All patients with OHCA from January 2009 to September 2010 (intervention period) were included and compared to controls from January 2006 to December 2007 (control period). An adjusted analysis was performed using multivariate regression to test association of outcomes with the package. During the intervention period, 168 patients were brought to the emergency department, 76 patients regained spontaneous circulation, and 41 patients were eligible for TH. Of these 41 patients, 36 (87.8%) ultimately achieved temperatures of <34°C. During the control period, 149 patients were brought to the emergency department, 57 patients regained spontaneous circulation, and 35 patients were eligible for TH. Of these 35 patients, 4 (11.4%) ultimately achieved temperatures of <34°C. In the adjusted analysis, patients admitted during the intervention period demonstrated improved survival (odds ratio: 2.609, 95% confidence interval: 1.318–5.166) and had favorable neurologic outcomes (odds ratio: 3.568, 95% confidence interval: 1.224–10.399) compared with those admitted during the control period. Comprehensive packages of postcardiac arrest care can be successfully implemented in a tertiary teaching hospital. In addition, implementation of TH was associated with significant improvements in survival and neurologic outcomes after OHCA.
Introduction
Targeted temperature management also known as therapeutic hypothermia (TH), has been proven to improve neurologic outcomes for unconscious survivors of OHCA due to ventricular fibrillation (VF) (Bernard et al., 2002; The Hypothermia after cardiac arrest study group, 2002). The International Liaison Committee on Resuscitation recommends cooling of unconscious patients who present after having been resuscitated from OHCA to 32°C–34°C for 12–24 hours (Neumar et al., 2008). The optimal target temperature, however, is not known (Nielsen et al., 2011). In the 2010 American Heart Association (AHA) guidelines for postcardiac arrest care, the committee gave TH a Class I recommendation for use in out-of-hospital VF cardiac arrest and a Class IIb recommendation for in-hospital cardiac arrest of any initial rhythm or OHCA with an initial rhythm of pulseless electrical activity or asystole (Peberdy et al., 2010).
However, the optimal hospital care for patients after OHCA is not known because multiple organ systems are affected. Previous studies of implementation of comprehensive packages of postcardiac arrest care that included TH and percutaneous coronary intervention (PCI) has been shown to improve survival from cardiac arrest (Oddo et al., 2006; Knafelj et al., 2007; Sunde et al., 2007; Wolfrum et al., 2008; Gaieski et al., 2009). So, a comprehensive, structured, multidisciplinary system of care for the treatment of postcardiac arrest patients was recommended for Class I in the 2010 AHA guideline (Peberdy et al., 2010).However, the impact of postcardiac arrest care, including TH for Koreans is not dictated in any of the articles.
In January 2009, the Seoul St. Mary's Hospital implemented comprehensive packages of postcardiac arrest care that included TH, emergency cardiac catheterization, glucose management, ventilator management, target hemodynamic parameters, seizure control, and neurologic prognostication. This package was accompanied by an organized implementation strategy to address the barriers that had hindered adoption of TH.
We conducted a retrospective study using prospectively collected local TH registry data. The aim of this study was to examine whether comprehensive packages of care after OHCA were successfully implemented and ultimately improved survival to hospital discharge and favorable neurologic outcomes.
Methods
Patients
This retrospective study was conducted at a tertiary care teaching hospital in Seoul, Korea. Seoul St. Mary's Hospital serves a regional population of about 400,000 individuals. Annually, 60–100 patients are brought to our hospital due to OHCA. The study was approved by our institutional review board. All patients with nontraumatic OHCA admitted to Seoul St. Mary's Hospital between January 2006 and December 2007 were included as the control group, and patients admitted between January 2009 and September 2010 were included as the intervention group. Out-of-hospital resuscitation was delivered by paramedics who brought the patient to the emergency department where resuscitation was continued by emergency physicians.
Packages of postcardiac arrest care
The packages of postcardiac arrest care were initiated as soon as possible after arrival to the emergency department.
Therapeutic hypothermia
All unconscious patients who were resuscitated from nontraumatic OHCA and brought to the emergency department were eligible for the TH. Patients were excluded from the TH according to the following criteria: evidence of significant active bleeding, any intracranial hemorrhage, hemodynamic instability unresponsive to volume resuscitation and vasopressor treatment, severe dysrhythmia unresponsive to antiarrhythmic therapy, known terminal illness, poor prearrest neurologic status, and those with a “do not attempt resuscitation” preference. Ultimately, deciding whether a TH was initiated was up to the discretion of the treating physicians.
To induce TH, patients were covered with ice bags over the neck, axillae, torso, and groins. In addition, TH was induced by rapid intravenous infusion of 1–2 L of 4°C saline, evaporative cooling by moist fanning, fully exposing patient, an endovascular cooling device (Thermogard XP® Thermal Management System; Zoll, Sunnyvale, CA) or some combination of these techniques. An arterial line was inserted before TH induction. Patients were given sedation (midazolam), analgesia (fentanyl), and a paralyzing agent (rocuronium). Neuromuscular blockade was discontinued when the goal temperature was reached, but if shivering was not controlled with the sedative and analgesic agents, the continuous infusion of a neuromuscular blocker was restarted. These agents were stopped during rewarming as soon as the central temperature reached 35°C.
The goal was to achieve a temperature of 32°C–34°C as soon as possible and to maintain it for 24 hours. The endovascular cooling device was adjusted manually to keep temperatures close to a goal of 33°C. Rewarming was then started at a rate of 0.25°C/h with absolute avoidance of any active measure, first to a target of 36°C and then ensuring that 37.5°C was not exceeded and using an endovascular cooling device, until 72 hours had elapsed from the return of spontaneous circulation (ROSC).
Emergency cardiac catheterization
Patients with electrocardiographic criteria for ST-segment elevation acute myocardial infarction (i.e., new ST-segment elevation and new or presumably new left bundle branch block) were taken routinely to the cardiac catheterization laboratory for angiography and revascularization if indicated. If there was no evidence of ST-segment elevation but highly suspicious acute myocardial infarction was present, deciding whether emergency cardiac catheterization was initiated was up to the discretion of the treating physicians.
Management of glucose, ventilator, and hemodynamic parameters
All unconscious patients were mechanically ventilated via endotracheal tubes and to maintain arterial blood at SaO2 of 94%–96% and PaCO2 of 35–45 mm Hg. Fluid infusion and the use of vasopressors and inotropes were recommended to achieve a mean arterial pressure of ≥70 mm Hg and a urine output of ≥0.5 mL/(kg·h−1). The use of continuous insulin infusion to achieve glycemic control (≤180 mg/dL) was encouraged.
Seizure control and neurologic prognostication
An electroencephalogram (EEG) for the diagnosis of seizure was performed during TH whenever possible. If there was evidence of electrographic seizure or clinical diagnosis of seizure, then continuous EEG monitoring was conducted and antiepileptic drugs, such as valproic acid, clonazepam, and levetiracetam were started.
Combination methods for postcardiac arrest prognostication were developed using the neurologic exam, median nerve somatosensory evoked potentials, EEGs, and diffusion weighted magnetic resonance imaging.
Data collection and outcome assessment
Data were collected prospectively by recording various factors at resuscitation when advanced cardiovascular life support (ACLS) was performed in the emergency department using a local TH registry data. A retrospective evaluation of the registry, including the EMSs records, the cardiopulmonary resuscitation (CPR) records, the intensive care unit notes, and the neurologic assessment records, were conducted.
The time interval from witnessing (if the event was not witnessed, then the time of calling the EMS was used) to first basic life support attempt represented absolute anoxic time, and the time interval from witnessing (if event was not witnessed, then the time of calling the EMS was used) to the end of ACLS represented the total anoxic time.
The primary outcomes were survival and favorable neurologic outcome at discharge. Neurologic status was assessed using Glasgow-Pittsburgh Cerebral Performance Categories (CPC) and good outcomes were defined as CPC scores of 1 and 2 (Booth et al., 2004). Data were obtained from medical record reviews.
Statistical analysis
The distributions of baseline characteristics are provided as percentages and mean±standard deviation. For patient characteristics and comparisons between the control period and the intervention period, we used a t-test for continuous variables and a Fisher's exact test and the chi-square test for categorical variables. To determine independent predictors of survival and favorable neurologic outcomes, odds ratios and the 95% confidence intervals were calculated using a logistic regression model. The calculated odds ratios were adjusted for variables associated with outcome (age <65 years, witnessed cardiac arrest, and the presence of a shockable rhythm). CPR performed by bystanders had a positive but nonsignificant effect on patient outcomes, perhaps due to the low rate of CPR received by the general public. Therefore, bystander CPR was not included in the final regression model. After all variables were entered into the model, the intervention period variable was forced in the model to determine its association with outcome. All statistical analyses were performed using SPSS version 16.0 (SPSS, Chicago, IL), and p-values ≤0.05 were considered significant.
Results
Baseline age, gender, past history, cause of arrest, witnessed arrest, and CPR performed by bystanders were similar among the patients from the two periods (Table 1). In regard to the presenting rhythm, both VF and pulseless electrical activity were more common during the intervention period than the control period. During the intervention period, 168 patients were brought to the emergency department, 76 patients regained spontaneous circulation and 41 patients were eligible for TH. Of these 41 patients, 36 (87.8%) ultimately achieved temperatures of <34°C. Of the 35 patients who were not eligible for TH, 1 patient regained consciousness, 8 patients had intracranial hemorrhage, 5 patients were hemodynamically unstable unresponsive to fluids and vasopressors, 11 patients had a poor prearrest neurologic status, 7 patients had a known terminal illness, 1 patient had gastrointestinal bleeding, 1 patient had severe dysrhythmia, and 1 patient had a congenital bleeding disorder. During the control period, only 4 patients received TH.
HTN, hypertension; DM, diabetes mellitus; VF, ventricular fibrillation; VT, ventricular tachycardia; PEA, pulseless electrical activity; CPR, cardiopulmonary resuscitation; APACHE, acute physiology and chronic health evaluation; ROSC, return of spontaneous circulation.
Cardiac catheterization was more likely to be used in patients during the intervention period (p=0.005). Patients with electrocardiographic criteria for an acute ST-elevation myocardial infarction were taken for emergency angiography and revascularization. However, these patients comprised a very small percentage of this study. For patients without ST elevation myocardial infarction, after considering the patient's cardiac enzyme status, echocardiographic findings, and clinical situation, delayed angiography was performed and for most patients it tended to be during the intervention period.
Effect of comprehensive packages of postcardiac arrest care
In June 2008, the local committee of postcardiac arrest care was formed with local champions as central figures. Because all OHCA patients went through the emergency room, the initial barrier-specific intervention was designed for emergency physicians, emergency nurses, paramedics, and others, but gradually, it was applied to other department professors (e.g., cardiologists, intensivists, neurologists, and anesthesiologists). As a result, the use of TH increased during the study; compared with the control period, the use of TH during the intervention period increased eightfold. Insulin infusions also increased about eightfold during the intervention period compared to the control period (Table 2). The adverse events were not statistically different between two time periods (Table 4).
TH, therapeutic hypothermia; PCI, percutaneous coronary intervention; RRT, renal replacement therapy; ICD, implantable cardioverter-defibrillator; EEG, electroencephalogram; SSEP, somatosensory evoked potential; DW-MRI, diffusion-weighted magnetic resonance imaging.
Pulse rate <50/min was defined as bradycardia.
Seizure was defined clinically (i.e., convulsive movements of head, extremities, or trunk) and electrographically.
Bleeding requiring transfusion was defined as bleeding.
Survival and neurologic outcomes
The overall rate of survival to discharge was greater during the intervention period: control period=11.4% versus intervention period=23.8%; p=0.004. In addition, favorable neurologic outcomes were greater during the intervention period than during the control period: control period=4.0% versus intervention period=11.9%; p=0.011 (Fig. 1, Table 1).
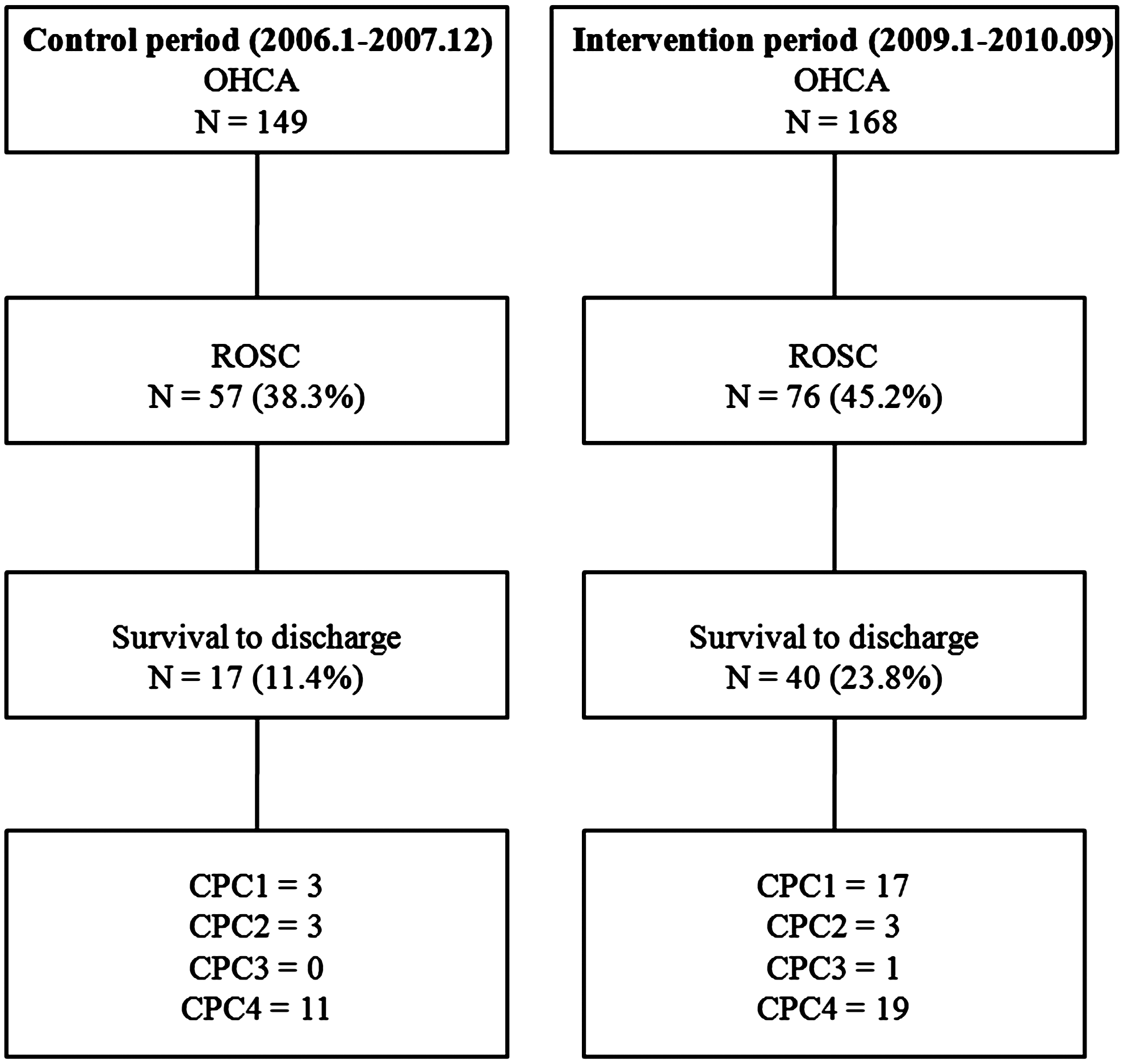
Flowchart for patients with out-of-hospital cardiac arrest in the control and intervention periods.
The univariate and multivariate predictors of survival for discharge and favorable neurologic outcomes are shown in Table 3. The odds ratios of survival to discharge and a favorable neurologic outcome during the intervention period were 2.609 (95% CI: 1.318–5.166) and 3.568 (95% CI: 1.224–10.399), respectively (Table 3).
OR, odds ratio; CI, confidence interval.
Discussion
The primary aim of this study was to assess whether a comprehensive package of care after OHCA could successfully be implemented and ultimately improved survival to discharge and favorable neurologic outcomes. In our experience, the package can be successfully implemented and implementation of the package improved survival and neurological outcomes in the patients with OHCA regardless of initial rhythm. When trying to improve the quality of care of postcardiac arrest patients, a package of care, including TH and emergency angiography/PCI seems to be of importance.
In Korea, the overall survival rate and favorable neurologic outcome were very poor compared with other countries (Nichol et al., 2008; Iwami et al., 2009; Ahn et al., 2010). Low rates of a public access defibrillator, low rates of bystander CPR, and low rates of checkup of prehospital ECG and defibrillation would impact the low rate of survival (Ahn et al., 2010). So, there were no patients with ROSC before arriving to our hospital. Our data support that comprehensive packages of postcardiac arrest care are effective even if the quality of prehospital care may be low.
In 2008, we conducted an Internet-based survey of physician members who have actively participated in the Korean Society of Critical Care Medicine (Kim et al., 2009). According to the survey results, only 37% of physicians implemented TH. This result is similar to survey reports for critical care and intensive care unit (ICU) physicians in other countries (Abella et al., 2005; Laver et al., 2006; Merchant et al., 2006; Wolfrum et al., 2007). In our survey, the most common reason for nonuse was a lack of agreement (i.e., had not considered this treatment option). Although our hospital has used TH in comatose survivors after cardiac arrest since 2002, implementation was difficult and underused.
The previous literature regarding implementation strategies has noted that barriers may be related to changing clinician knowledge, attitudes, and behaviors (Cabana et al., 1999; Brooks and Morrison, 2008); thus, we planned a stepwise and multifaceted approach to overcome specific barriers and to ultimately implementation of comprehensive packages of postcardiac arrest care. The first step was to update our postcardiac arrest care protocols and create a standard order set in the electronic medical record system. The contents of our protocol were as follows: indications and contraindication for TH, cooling technique (induction, maintenance, rewarming), emergency cardiac catheterization, glucose management, ventilator management, target hemodynamic parameters, seizure control, and dosages of some medications. The second step was holding an education session for emergency physicians and emergency nurses. They were trained to freely handle the endovascular cooling machine during a simulation workshop and tailored education sessions to understand our postcardiac arrest protocol. Because postcardiac arrest patients demonstrated various clinical outcomes and not all of them could be recorded in the postcardiac arrest protocol, we conducted evidence-based topic review whenever possible and followed the local champion's opinion when evidence was insufficient. The third step was to change attitudes. Rounds were held with members familiar with the postcardiac arrest procedure for neurologically intact survivors and generated feedback for the postcardiac arrest procedure. Finally, interprofessional education for CPR and TH was held by local champions.
Unlike a conventional study conducted in a controlled ICU setting (Oddo et al., 2006; Sunde et al., 2007; Werling et al., 2007), our research is a study of implementation in the emergency department. According to a telephone survey conducted in the United Kingdom, only 35% of respondents are willing to initiate cooling in an emergency department (Galloway and Sherren, 2010). However, the emergency department's decision not to start cooling could have an impact on a patient's prognosis. There is commonly a delay in getting patients to the ICU from the emergency department in tertiary, teaching hospitals, especially in South Korea. Thus, initiating cooling in the emergency department is critical to reduce delays in therapy.
The feasibility and efficacy of primary PCI in patients who survive cardiac arrest with ST elevation myocardial infarction (STEMI) have been well established and the combination of mild TH with primary PCI is also feasible (Hovdenes et al., 2007; Knafelj et al., 2007). Patients with STEMI should undergo immediate angiography and revascularization if indicated. Implantable cardioverter defibrillators decrease mortality compared with antiarrhythmic therapy in secondary prevention of OHCA (Connolly et al., 2000; Kuck et al., 2000). So, it should be considered in patients with neurologically intact survivors from cardiac arrest. Optimal glucose control after cardiac arrest is not well proven. However, elevated serum glucose was associated with poor outcome after cardiac arrest (Mullner et al., 1997). Moreover, TH may increase blood glucose level due to increased insulin resistance. So, insulin treatment should be considered as part of packages of postcardiac arrest care.
Our study has several limitations. First, this study is an experience from a single tertiary teaching hospital, limiting the generalizability of these results. Second, the retrospective nature of the study leaves it open to several biases. Third, there was a relatively small sample size in our study. It has been suggested that there was no impact on survival or neurologic outcomes when the initial rhythm was not VF when implementing a postcardiac arrest protocol (Don et al., 2009). However, due to the smaller sample size, our study could not determine whether the shockable or nonshockable initial rhythm has an impact.
Conclusions
Comprehensive packages of postcardiac arrest care can be successfully implemented in a tertiary teaching hospital. In addition, implementation of the package was associated with significant improvement in survival and neurologic outcomes in patients with an OHCA.
Footnotes
Acknowledgments
The authors thank Eun Mi Ko for data collection and management. We also appreciate Clifton W. Callaway, MD, in the Department of Emergency Medicine, University of Pittsburgh, who kindly provided the critical review of the article.
The authors report this study did not receive any outside funding or support.
Author Disclosure Statement
There are no financial or other relations that might pose a conflict of interests.