
Abstract
Targeted temperature management (TTM) improves outcome after out-of-hospital cardiac arrest (OHCA). We hypothesized that there may be a significant relationship between the dose of hypothermia, the time to return of spontaneous circulation (ROSC), and survival to discharge. Retrospective pilot investigation on 99 consecutive OHCA patients with initial shockable rhythm, surviving to admission, and undergoing TTM between 2008 and 2011. Dose of hypothermia was defined as the sum of the induction interval (time to target temperature [from ROSC to 33°C]); the controlled hypothermia interval (from reaching 33°C until rewarming); and the rewarming interval (from 33°C to 37°C). Time to ROSC was measured from pulselessness or 911 call time to ROSC. The ratio between the two was termed the hypothermic to ischemic ratio. Purposeful variable selection for logistic regression modeling was used to assess the influence of the hypothermic/ischemic ratio on survival. Odds ratios (OR) were used to examine the effects of predictor variables on survival. Of 99 patients, eight were excluded for deviation from protocol, death during protocol, or missing data. From the univariate models, survivors were more likely to be younger, have a shorter time to ROSC, and have a larger hypothermic/ischemic ratio. Survivors also had a nonsignificant trend toward a longer time to target temperature. In multivariable modeling, the hypothermic/ischemic ratio was the most significant predictor for survival (OR 2.161 [95% confidence interval 1.371, 3.404]). In this pilot study, the hypothermic to ischemic ratio was significantly associated with survival to discharge for patients with an initial shockable rhythm. Further investigation of the relationship between the dose of hypothermia and time to ROSC for postresuscitation TTM is needed.
Introduction
C
Patients who survive out-of-hospital cardiac arrest (OHCA) to hospital admission are at the mercy of a physiologically complex cascade of ischemia–reperfusion injury. However, differences in the historical and clinical facts of each OHCA event place each patient upon a spectrum of clinical presentation from awake and stable to comatose and tenuous. Whereas TTM is advocated as part of the bundle of comprehensive postresuscitation care (Sunde et al., 2007; Gaieski et al., 2009) to blunt the brain injury, most OHCA patients receive, if at all, the same institution-specific protocol for induced hypothermia, regardless of presentation (i.e., time to return of spontaneous circulation (ROSC), initial rhythm, and age). The variability in presentation following OHCA may suggest modifying standardized protocols and tailoring therapy to individual patients to improve outcomes. Time to ROSC is a readily available, although crude, measure of suffered ischemic insult that is typically captured and reported for each patient.
The purpose of this pilot study was to assess the relationships between the dose of hypothermia (i.e., hypothermic treatment time), the duration of ischemia (i.e., time to ROSC), and survival to hospital discharge in patients admitted after OHCA presenting with a shockable rhythm. A longer or shorter dose of hypothermia may be needed for each patient, using time to ROSC as the most readily available measure of ischemic insult.
Materials and Methods
Study population and setting
This pilot study was a single-center, retrospective cohort using data between January 2008 and January 2011. Consecutive, adult, nontraumatic OHCA subjects surviving to hospital admission were considered for inclusion into a comprehensive postresuscitation program at an urban academic, tertiary-care center, regardless of presenting rhythm. This investigation was approved by the Institutional Review Board at Virginia Commonwealth University, including a waiver for informed consent. Patients were accepted in transfer from regional satellite centers and from our own emergency department (ED) if they met the following inclusion criteria: (1) witnessed arrest with ROSC independent of presenting cardiac rhythm, (2) unwitnessed arrest with initial cardiac arrest rhythm of ventricular fibrillation (VF) or pulseless ventricular tachycardia (pVT), (3) age at least 18 years, and (4) remaining comatose (defined as nonpurposeful movements or unresponsive to verbal commands) after ROSC.
Patients were excluded for this investigation if (1) presenting rhythm other than pVT or VF, (2) significant prearrest neurological dysfunction, (3) terminal illness or advanced directives precluding aggressive care, (4) severe hemodynamic instability or shock, despite aggressive resuscitative efforts, and (5) death before completion of therapy. Instability or shock was defined as ongoing hypotension despite adequate fluid resuscitation and two vasopressors. All patients followed a TTM protocol, including intravascular cooling (Alsius Catheter System; ZollMedical Corporation, Chelmsford, MA) and strict hemodynamic monitoring in the Coronary Intensive Care Unit.
TTM protocol
For patients presenting directly to the ED, prehospital providers began induced hypothermia with up to two liters cold (4°C) saline during resuscitation, as part of their protocols. Not all prehospital agencies provided this therapy or had time to administer therapy during short transport times, however, and in these cases, cold saline was administered in the ED. Temperature was measured initially by the bladder or rectum until an endovascular cooling catheter was placed in the femoral vein soon after ED arrival. Patient temperature was maintained at 33°C for a total of 24 hours followed by controlled rewarming over 16 hours. Normothermia was maintained thereafter. Metabolic, ventilation, and hemodynamic parameters were managed according to goal directed targets for the first 72 hours in consultation with the on-call resuscitation attending.
Bolus paralytics or continuous drips were dosed for patients to control shivering. The core temperature was monitored by a temperature-sensing Foley catheter and maintained in a closed-loop fashion by the cooling system. The intravascular system has an inherent measurement error of 0.3°C. All patients had the catheter removed by 96 hours after insertion.
Data collection and outcomes
Performance improvement data were collected from the hospital and Emergency Medical Service (EMS) records, including baseline demographic characteristics, EMS provision of prehospital cooling, and all relevant time intervals from time of arrest or 911 call to hospital discharge or death, according to the Utstein recommendations (Cummins et al., 1991). Two independent observers reviewed the records for data extraction and discrepancies were resolved by consensus. The best Pittsburgh cerebral performance category (CPC) scores were recorded at hospital discharge as a secondary outcome measure. All patients were included in an intention to treat analysis. The primary outcome was survival to hospital discharge (or survival status, yes/no).
The time to ROSC was defined as the time from witnessed arrest or 911 call receipt to ROSC (sustained for >20 minutes). The dose of hypothermia was defined as the sum of the induction interval (time to target temperature from ROSC to 33°C); the controlled hypothermia interval (from target temperature until initiation of rewarming); and the rewarming interval (from 33°C to 37°C). The target temperature was achieved when 33° was reached and maintained. Figure 1 outlines the time intervals used for analysis. The hypothermic dose divided by the time to ROSC made up the hypothermic/ischemic ratio, calculated for each patient and used in multivariable modeling.
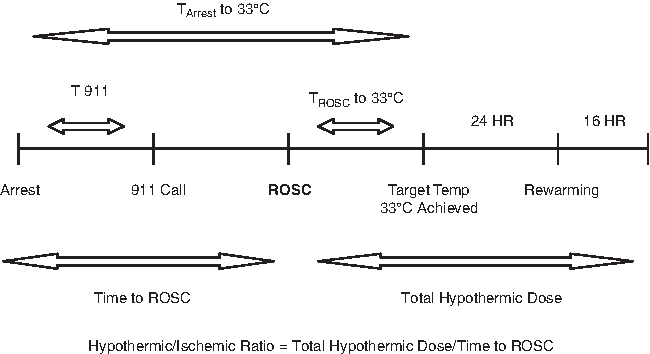
Time interval data. T, time; ROSC, return of spontaneous circulation; HR, hour.
Statistical analysis
Continuous variables, including age (years), initial temperature (degrees Celsius), and all time intervals (minutes or hours) are reported as means and standard deviations (SDs); categorical variables are reported as counts and percentages.
An initially purposeful variable selection was used to model the relationship of the hypothermic/ischemic ratio to survival. Further univariate logistic regression was used to assess each Utstein predictor variable for potential inclusion in the multivariable logistic model. Model assumptions, including linearity in the logit, were assessed. Odds ratios (OR) were used to examine the effects of the predictor variables on survival. Data were analyzed using JMP v.9.0.2 (SAS Institute, Inc., Cary, NC) and SAS v.9.2 (SAS Institute, Inc.) software, with a significance level of alpha=0.05.
Results
A total of 169 patients were considered for this study, of which 99 presented with a shockable rhythm. Eight patients were excluded according to criteria or for missing relevant data. Figure 2 demonstrates the contribution of each patient to our analysis, and Table 1 summarizes the baseline characteristics for the study cohort.
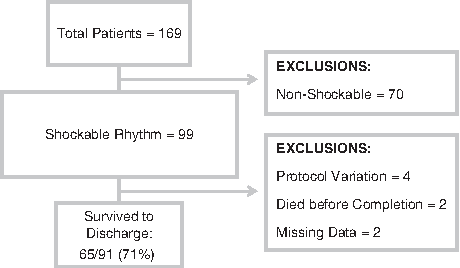
Patient cohort summary. Shockable rhythm, ventricular fibrillation/pulseless ventricular tachycardia; nonshockable, all other rhythms.
Significantly different (p<0.05) for survivors versus nonsurvivors.
Categorical variables: reported as n, (%).
Continuous variables: time intervals (minutes), SD.
CPR, cardiopulmonary resuscitation; EMS, Emergency Medical Service; ROSC, return of spontaneous circulation; SD, standard deviation; STEMI, ST-elevation myocardial infarction; °C, degrees Celsius.
Overall, 65/91 (71%) survived to hospital discharge. CPC scores at discharge are presented in Table 2. The average age was 58.1 (SD 12.55) years, average time to ROSC 26.4 (SD 19.32) minutes, average time to target temperature 5.5 (SD 2.99) hours, and average total hypothermic dose 45.5 (SD 2.99) hours. The hypothermic/ischemic ratio was log transformed for non-normality (Fig. 3). From the univariate models, those patients who survived were significantly younger (mean difference 5.5 years [standard error (SE) 2.63, 95% confidence interval (CI) 0.28, 10.80] p-value 0.0395), had a significantly shorter time to ROSC (mean difference 14.8 minutes [SE 4.37, 95% CI 5.95, 23.59] p-value 0.0016), and a larger hypothermic/ischemic ratio (difference −0.7 [SE 0.12, 95% CI −0.92, −0.44] p-value <0.0001). Survivors also had a trend toward a significantly longer time to target temperature (mean difference 62.0 minutes [SE 38.00, 95% CI −138.12, 14.12], p-value 0.1084). No other available Utstein variables were significantly related to survival. Unadjusted (univariate) OR are presented in Table 3.
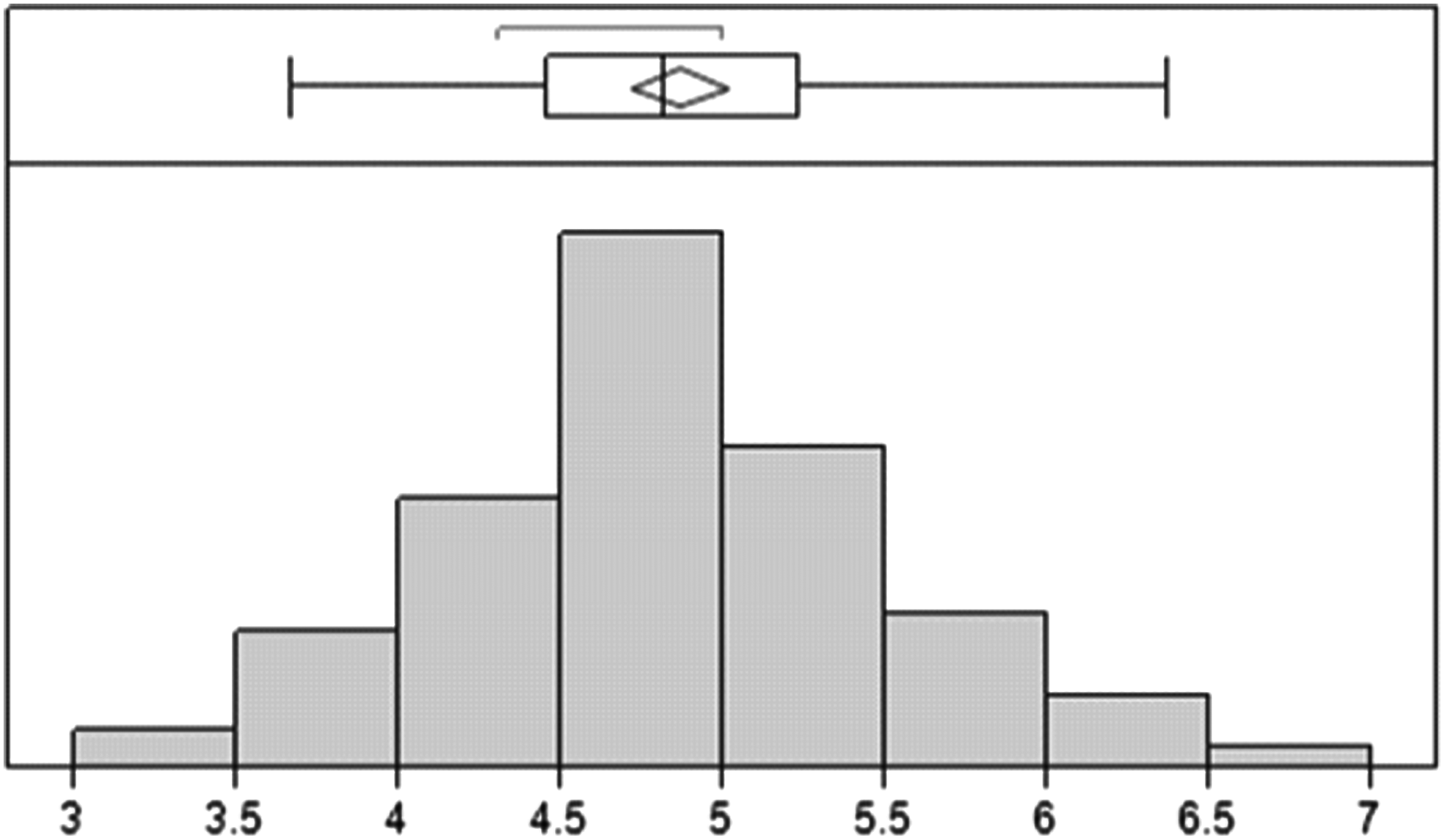
Distribution of hypothermic/ischemic ratio after log transformation.
CPC, cerebral performance category at discharge from the hospital.
Statistically significant.
OR, odds ratio; LL, lower limit of 95% confidence interval; UL, upper limit of 95% confidence interval; M, male; C, Caucasion; Y, yes; °C, degrees Celsius.
In multivariable modeling, a larger hypothermic/ischemic ratio was significantly related to favorable survival. Controlling for all Utstein variables available for this study, as well as age, initial temperature, and time to target temperature, the most significant predictor was the hypothermic/ischemic ratio (OR 2.161 for a unit change of 0.1 [95% CI 1.371, 3.404]). Adjusted (multivariable) OR are presented in Table 4.
Degrees of Freedom for each variable=1.
Statistically significant.
Discussion
Our pilot investigation identified that the hypothermic/ischemic ratio may be significantly related to survival from OHCA. Our findings are consistent with other current initiatives to identify a more potent treatment goal than core body temperature, and as such, our preliminary results suggest that the relationship between the total hypothermic dose and the ischemic insult, that is, time to ROSC, needs further study.
The possibility for a customized approach to postresuscitation care would be a profound shift in the current postarrest treatment paradigm. No large, human clinical cardiac arrest studies have directly examined the relationship between the duration of ischemia and duration of hypothermia. Most animal model research has focused on varying the timing, induction rate, or depth of hypothermia, with all other variables remaining fixed (Abella et al., 2004; Boddicker et al., 2005; Tsai et al., 2008; Weihs et al., 2010). Coimbra and Wieloch (1994) observed that while 3.5 hours of hypothermia allowed some neuroprotection, 5 hours of hypothermia allowed marked protection after 10 minutes of ischemia. Whereas their conclusion centered on the timing of moderate hypothermia, they concluded that the short “duration of the hypothermic episode” was the reason for lack of neuroprotection in earlier studies. They recognized that the duration of hypothermia was an important factor for a favorable outcome and that there may be a dose–response relationship between the total hypothermic dose and ischemic time.
Whereas not statistically significant in this cohort, we found that a longer time to target the temperature interval tended to be related to a favorable survival, which is consistent with the findings of others (Vanston et al., 2010; Haugk et al., 2011). A popular explanation for this seemingly paradoxical relationship is that patients with more severe ischemic injury, and thereby anoxic brain injury, have impaired thermoregulation and are not only colder on presentation but are also easier to cool (Sessler, 2009). However, it may be that patients with a longer time to target temperature are effectively treated for a longer total time than those who achieved goal temperature quickly and thus have a longer hypothermic treatment dose. This observation, however, also requires further investigation.
The significance of prehospital cooling with 4°C intravenous saline as a categorical variable is noteworthy in our study, but difficult to interpret. Previous investigations of prehospital cooling demonstrated mixed results (Bernard et al., 2010; Skulec, 2010) and practice recommendations remain controversial (Castren et al., 2010; Garrett et al., 2010; Scolletta et al., 2012). In our study, conducted contemporaneously with the recent Kim et al. trial showing potential harm with this technique (Kim et al., 2014), ∼50% of our patients received some amount of intravenous cold saline in the prehospital setting; however, little data regarding its administration (timing, volume, etc.) are available for our cohort. In accounting for this lack of data, we considered the initial ED temperature as a surrogate for influence of EMS cooling on time to target temperature, but normal physiologic responses to postcardiac arrest syndrome, as well as other patient and situational variables, complicate this assumption. Ultimately, the study design chosen limits the ability of this investigation to evaluate prehospital cold saline therapy for its impact on survival. The aggressive practice to initiate hypothermia as early as possible was the protocol for the patients included in this study and the investigators supported this recommendation during the study period.
External validation and prospective studies considering the predictive ability of the hypothermic/ischemic ratio are needed as nearly all of the variability in this study was due to the time to target temperature and time to ROSC. The controlled hypothermic interval (24 hours) and rewarming interval (16 hours) are typically fixed in our protocol. Whereas we could have conveniently constructed the hypothermic/ischemic ratio as the ratio between time to target temperature and time to ROSC alone, this construct would have limited the external generalizability of our findings to those institutions that do not fix all intervals in the ratio. Anticipating further evaluation of the hypothermic/ischemic ratio in these populations, as well as in patients presenting with nonshockable rhythms (Lundbye et al., 2012), the authors constructed the ratio as presented.
Limitations
Inherent to all retrospective studies, this study was limited by the quality of medical records and the inability to control for all measured and unmeasured confounders. The comprehensive prehospital provider Utstein characteristics are not reported, since several different agencies transported patients to our hospital. Patients were ultimately included or excluded from this study after survival to hospital admission, not in the field. In an attempt to mitigate these problems, the data collection was meticulous and rigorously internally validated as part of a quality improvement review. Two independent reviewers abstracted key data elements and discussed each discrepant element for consensus.
The sample size was a limiting factor in this pilot investigation for meaningful subanalysis, and our results should be considered as hypothesis generating rather than advocating for a specific clinical practice. Similarly, given that our study cohort was treated with a comprehensive postresuscitation program, our results may not be completely generalizable to other centers and patients. However, in spite of these shortcomings, our study uncovered several interesting questions for further study, including whether the hypothermic/ischemic ratio could be important for tailoring temperature management at the individual patient level.
Conclusions
In conclusion, our pilot study has investigated the relationship between the dose of hypothermia and time to ROSC and found it to be significantly related to survival to discharge in patients undergoing TTM after cardiac arrest with a shockable rhythm. The optimal total hypothermic treatment time after OHCA may be related to each individual's duration of time to ROSC and should be further investigated.
Footnotes
Acknowledgments
The authors acknowledge Dr. Roy Sabo, PhD, for his review of their statistical analyses. They also acknowledge Dr. Kyle Gunnerson, MD, for his review of the article.
Author Contributions
K.N.S. and M.C.K. conceived the study and designed the methods. M.C.K. made significant contributions to the ideas presented and the writing of the article. R.K.E. provided statistical expertise and review. M.G. and C.R. participated significantly with data collection and patient care. The remaining authors made significant contributions to the article and its revisions. K.N.S. takes responsibility for the article as a whole and is unaware of any copyright constraints.
Disclosure Statement
No competing financial interests exist for any author.