
Abstract
Targeted temperature management (TTM) may improve respiratory mechanics and lung inflammation in acute respiratory distress syndrome (ARDS) based on animal and limited human studies. We aimed to assess the pulmonary effects of TTM in patients with respiratory failure following cardiac arrest. Retrospective review of consecutive cardiac arrest cases occurring out of hospital or within 24 hours of hospital admission (2002–2012). Those receiving TTM (n=44) were compared with those who did not (n=42), but required mechanical ventilation (MV) for at least 4 days following the arrest. There were no between-group differences in age, gender, body mass index, APACHE II, or fluid balance during the study period. The TTM group had lower ejection fraction, Glasgow Coma Score, and more frequent use of paralytics. Matched data analyses (change at day 4 compared with baseline of the individual subject) showed favorable, but not statistically significant trends in respiratory mechanics endpoints (airway pressure, compliance, tidal volume, and PaO2/FiO2) in the TTM group. The PaCO2 decreased significantly more in the TTM group, as compared with controls (−12 vs. −5 mmHg, p=0.02). For clinical outcomes, the TTM group consistently, although not significantly, did better in survival (59% vs. 43%) and hospital length of stay (12 vs. 15 days). The MV duration and Cerebral Performance Category score on discharge were significantly lower in the TTM group (7.3 vs. 10.7 days, p=0.04 and 3.2 vs. 4, p=0.01). This small retrospective cohort suggests that the effect of TTM ranges from equivalent to favorable, compared with controls, for the specific respiratory and clinical outcomes in patients with respiratory failure following cardiac arrest.
Introduction
I
Animal studies demonstrate an overall favorable effect of TTM on lung function. Hypothermia has been shown to attenuate ischemia–reperfusion lung injury (Shoji et al., 2005; Zhang et al., 2006; Chang et al., 2008) and ventilator-induced lung injury (Lim, 2003a; Suzuki et al., 2004; Morita et al., 2009; Cruces et al., 2011; Aslami et al., 2012). Moreover, animal literature shows a consistent protective effect of hypothermia on toxin-induced lung injury (Lim, 2003b; Scumpia et al., 2004; Chin et al., 2007; Jo et al., 2011) and pneumonia (Beurskens et al., 2012).
Of the limited human data available, the impact of TTM on lung function also appears favorable. Physiologically, implementation of hypothermia results in a decrease in whole body oxygen extraction without affecting oxygen delivery (Bacher et al., 1997). Others documented a reduction in O2 consumption, CO2 production, and calculated energy expenditure in patients who were cooled from a febrile state to normothermia (Manthous et al., 1995). Ensuing reduction in the metabolic rate allowed successful ventilation with a very low tidal volume in a patient with refractory acute respiratory distress syndrome (ARDS), without a substantial increase in PaCO2 and acidosis (Duan et al., 2011). Recently, Aslami et al. (2010) compared respiratory parameters in cardiac arrest patients during hypothermia and after rewarming, and demonstrated a reduction in PaCO2 that was still present following rewarming, as well as an increase in the PaO2/FiO2 ratio upon completion of hypothermia. However, this study lacked a control group, and no comparison data were collected before hypothermia induction. Finally, in a small pilot study of 19 patients with refractory ARDS, a mortality benefit was suggested when hypothermia was implemented as a salvage therapy (Villar and Slutsky, 1993).
In the definitive trials demonstrating the clear neurologic benefit following cardiac arrest (Bernard et al., 2002; HACA, 2002), the effect of TTM on respiratory mechanics was unfortunately not formally assessed. The largest trial to date examining TTM of 33°C versus 36°C on neurologic outcomes of cardiac arrest survivors has not yet reported data on lung function (Nielsen et al., 2013). To further clarify the effects of TTM on pulmonary mechanics, we studied a cohort of patients who suffered a cardiac arrest and compared respiratory parameters in those who were treated with hypothermia versus in those who were not. We hypothesized that TTM in current clinical practice will show improved respiratory mechanics and gas exchange, and provide additional support for the need to investigate TTM as another potential therapy for patients with ARDS.
Methods
Study population
We retrospectively reviewed consecutive cases of cardiac arrest admitted to a single tertiary care academic center in a 10-year period (2002–2012). Inclusion criteria aimed to identify those patients who had return of spontaneous circulation following a cardiac arrest that occurred either out of hospital or within 24 hours of admission, resulting in intubation and MV for at least 3 days. Patients who had an arrest later in a hospital stay were excluded to minimize the effect of iatrogenic factors. Additionally, patients without serial arterial blood gas or ventilator data, those who received limited care (e.g., palliative care or withdrawal of life support), or did not achieve sustained hypothermia (32–34°C) were also excluded. The study protocol was approved by the local Institutional Review Board.
Intervention
TTM patients received sedation, analgesia, shiver control, and paralysis as per a predefined institutional protocol. As per this clinical protocol, patients had serial or continuous measurements of electrocardiography, blood gas, renal function, coagulation profile, complete blood counts, surveillance cultures, and vital signs. Arterial blood gas measurements were analyzed uncorrected for body temperature (alpha-stat). Induction of hypothermia was typically achieved by rapid infusions of cold saline and further controlled by an external cooling device using two water-circulating blankets (Arctic Sun, Bard Medical, Medivance, Inc., Louisville, CO). The target core temperature of 32–34°C was maintained for 12 or 24 hours (at the discretion of the clinician) before the controlled rewarming (typically 0.5°C per hour).
Data collection
All data were collected from clinical records. Demographic and clinical information and the Acute Physiology and Chronic Health Evaluation (APACHE) II score were obtained from admission data. Respiratory data included blood gases, corresponding ventilator settings, and airway pressures. For patients who received TTM following cardiac arrest, these respiratory parameters were gathered at baseline (i.e., postintubation, prehypothermia), at peak hypothermia (i.e., data at target temperature before rewarming), posthypothermia at Day 4 (i.e., after complete rewarming), and subsequently, throughout their hospital course for up to 7 days. Since the non-TTM group of patients (control) did not have hypothermia induced, peak hypothermia data in the TTM group were compared with Day 2 data in the non-TTM group. A few patients (n=7) in the TTM group did not have Day 4 values because they were rewarmed and extubated earlier, and three of the non-TTM group patients were also extubated by Day 3. For these patients, Day 3 data were carried over for comparison purposes at the posthypothermia/Day 4 time point. The Sequential Organ Assessment (SOFA) Score was calculated daily. Additional data on parameters that could influence lung function, such as the cumulative fluid status, amount of transfused blood products, need for vasopressor drugs, and mean blood pressures at times of blood gas collection, were collected daily for up to 7 days. We have also documented whether patients received medications that might affect their risk for developing lung injury by either being a risk factor such as amiodarone (Dhokarh et al., 2012) or providing a potentially protective effect such as aspirin (Kor et al., 2012), statin (O'Neal et al., 2011), intravenous heparin (Gedik et al., 2012), and angiotensin-converting enzyme inhibitor/angiotensin receptor blocker (Wösten-van Asperen et al., 2008).
Outcome variables
Respiratory outcomes included indices of oxygenation and ventilation compared at the time of intubation (prehypothermia) to Day 4 (posthypothermia, after complete rewarming): PaO2/FiO2, positive end-expiratory pressure (PEEP), pH, PaCO2, peak inspiratory pressure, tidal volume, and dynamic compliance (calculated as tidal volume/[peak inspiratory pressure–PEEP]). Subsequently, we explored clinical outcomes of survival, duration of MV, ventilator-free days, hospital and intensive care unit (ICU) length of stay (LOS), and cerebral performance category (CPC) on discharge.
Statistical analyses
Groups were comprised on the basis of whether patients received TTM following cardiac arrest or not (control). Reported descriptive variables include medians with their interquartile ranges or means with their standard deviations (±SD), where appropriate. Univariate analyses were performed to compare demographics, comorbidities, and in-hospital medications between the groups. The chi-square test and the t-test were used to evaluate for group differences in nominal and continuous variables, respectively. If parametric assumptions could not be met, the Fisher's Exact and Mann–Whitney tests were used. For matched or paired data (e.g., change in a parameter at day 4 compared with baseline of the individual subject), the change or differences are expressed as their mean with their 95% confidence intervals (95% CI).
A p-value of less than 0.05 was considered statistically significant. All analyses were performed using the JMP Pro 10.0.2 statistical software (SAS Institute, Inc., Cary, NC).
Results
Patient selection
One hundred individuals underwent TTM following cardiac arrest, starting November 2006 through August 2012. Of the 56 excluded patients, 17 did not have serial arterial blood gas data, 23 had an arrest later in the hospital stay, 9 received palliative care or died before completion of TTM, 5 did not achieve target temperatures, one had only 5 hours of hypothermia, and one patient was excluded due to the mechanism of cardiac arrest (suicide attempt by hanging). The remaining 44 patients of this TTM group with cardiac arrest either out of hospital or within 24 hours of admission had blood gas and corresponding ventilator setting recorded prehypothermia, during hypothermia, and following rewarming.
A total of 42 cases were identified in the comparison cohort of cardiac arrest survivors who received 3 or more days of MV and had the required data, but did not undergo hypothermia. A majority of these subjects (28) were admitted before 2006, reflecting changing clinical practice. Some of the documented reasons for not receiving TTM in the remaining patients included the lack of comatose state (n=5), bleeding diathesis (n=4), and limitation on escalation of care (n=1).
Group characteristics
There were no baseline between-group differences in age, gender, ethnicity, body mass index, or APACHE II scores (Table 1). The TTM group had more patients with out-of-hospital arrest of a shockable rhythm (VF or nonperfusing ventricular tachycardia), lower ejection fraction, and a lower Glasgow Coma Score postevent. There were no between-group differences for documented history of atrial fibrillation, congestive heart failure, gastroesophageal reflux disease, hypertension, lung disease, or sleep apnea. The control (i.e., non-TTM) group had a higher documented incidence of diabetes and chronic kidney disease. With regard to medications that could affect lung function, there were no between-group differences for in-hospital administration of amiodarone, aspirin, intravenous heparin, angiotensin-converting enzyme inhibitors/angiotensin receptor blockers, and statins over the first 7 days of hospital stay. As expected, administration of paralytics was significantly higher in the TTM group (91% vs. 17%, Table 1).
±Standard deviation.
APACHE, acute physiology and chronic health evaluation; BMI, body mass index; GCS, Glasgow Coma Score; GERD, gastroesophageal reflux disease; ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; TH, therapeutic hypothermia.
The mean duration of hypothermia, including the cooling and rewarming phases, was 30 hours (SD 8). Patients in the TTM group underwent frequent blood, urine, and sputum sampling as per protocol and had significantly higher documented rates of positive sputum or urine, although not blood cultures. There were no significant group differences in SOFA scores, mean blood pressures at times of blood gas collection, cumulative fluid balance, or amount of transfused units of red blood cells or other blood products for any of the 7 study days. More patients in the TTM group required vasopressors on day 3 of hospital stay (p=0.03); otherwise, there were no significant differences between the groups in the number of patients on vasopressor support for any of the remaining days.
Respiratory outcomes
The tidal volumes (VTs) at admission for patients receiving TTM were significantly less than those of controls (503 mL±67 vs. 562 mL±108, p=0.001). During hypothermia (Day 2) and postrewarming (Day 4), the VTs were also maintained lower in the TTM group as compared with the control group (Table 2), however, no significant change in the VT occurred from baseline to Day 4 in either the TTM group (−13.3, 95% CI −44 to 18) or the controls (−4, 95% CI −36 to 28).
p-value reported for difference between values.
TTM, targeted temperature management; PEEP, positive end expiratory pressure; VT, tidal volume; PIP, peak inspiratory pressure; Cdyn, dynamic compliance.
Similarly, the peak inspiratory pressures were consistently lower in the TTM group at baseline/prehypothermia (26 cmH20±7 vs. 30 cmH20±9, p=0.016), during hypothermia compared with Day 2 of controls (24 cmH20±6 vs. 28 cmH20±7, p=0.01), and following rewarming on Day 4 (22 cmH20±6 vs. 25 cmH20±7, p=0.009). When comparing baseline to day 4, the peak inspiratory pressure decreased in both the TTM (−4.2 cmH20, 95% CI −6.6 to −1.8) and the non-TTM group (−5.5 cmH20, 95% CI −3.0 to −8.0), but not significantly between groups.
There were no significant group differences in the calculated dynamic compliance at baseline between the TTM and control groups (29.5 mL/cmH20±12.3 vs. 26.7 mL/cmH20±13.5, p=0.08) or during hypothermia/Day 2 (29 mL/cmH20±9.4 vs. 28.4 mL/cmH20±11.3, p=0.4). However, the TTM group had a significantly better compliance following rewarming on Day 4 (39.7 mL/cmH20±23.3 vs. 34.7 mL/cmH20±27.2, p=0.045). From baseline to Day 4, the compliance improved in both the TTM (11.0 mL/cmH20, 95% CI 2.5 to 19.5) and the non-TTM group (9.3 mL/cmH20, 95% CI 0.6 to 17.9), although not significantly between groups.
There were no significant differences in the initial PaO2/FiO2 between TTM and control groups (248±135 vs. 224±138, p=0.39). During hypothermia, the PaO2/FiO2 increased in the TTM group, but did not differ significantly from Day 2 values for the control group (292±106 vs. 274±153, p=0.15). Following rewarming, the PaO2/FiO2 remained consistently higher in the TTM group (303±122 vs. 254±89, p=0.03). When comparing the change in the PaO2/FiO2 from baseline to Day 4, despite the TTM group demonstrating a greater increase in the PaO2/FiO2 (54, 95% CI 4 to 104) compared with the non-TTM group (35, 95% CI −15 to 84), the difference between those changes was not statistically significant.
For the PaCO2, there were no significant initial differences between TTM and control groups (47 mmHg±13 vs. 43 mmHg±11, p=0.11). During hypothermia, PaCO2 values in the TTM group paralleled Day 2 values for the controls (34 mmHg±8 vs. 34 mmHg±7, p=0.47). Following rewarming, there was a trend for lower PaCO2 in the TTM group (35 mmHg±9 vs. 38 mmHg±8, p=0.054). When changes in PaCO2 for each group were compared from baseline to day 4, there was a greater decrease for the TTM group (−12, 95% CI −16.4 to −7.8) as compared with the controls (−5.4, 95% CI −9.8 to −1.0, p=0.02).
There were no significant differences between or within the TTM and control groups for pH and PEEP during the comparison periods (Table 2). Figures 1 and 2 depict changes in PaO2/FiO2 and PaCO2 for the groups throughout the 7-day study period.

PaO2/FiO2 for the two groups.
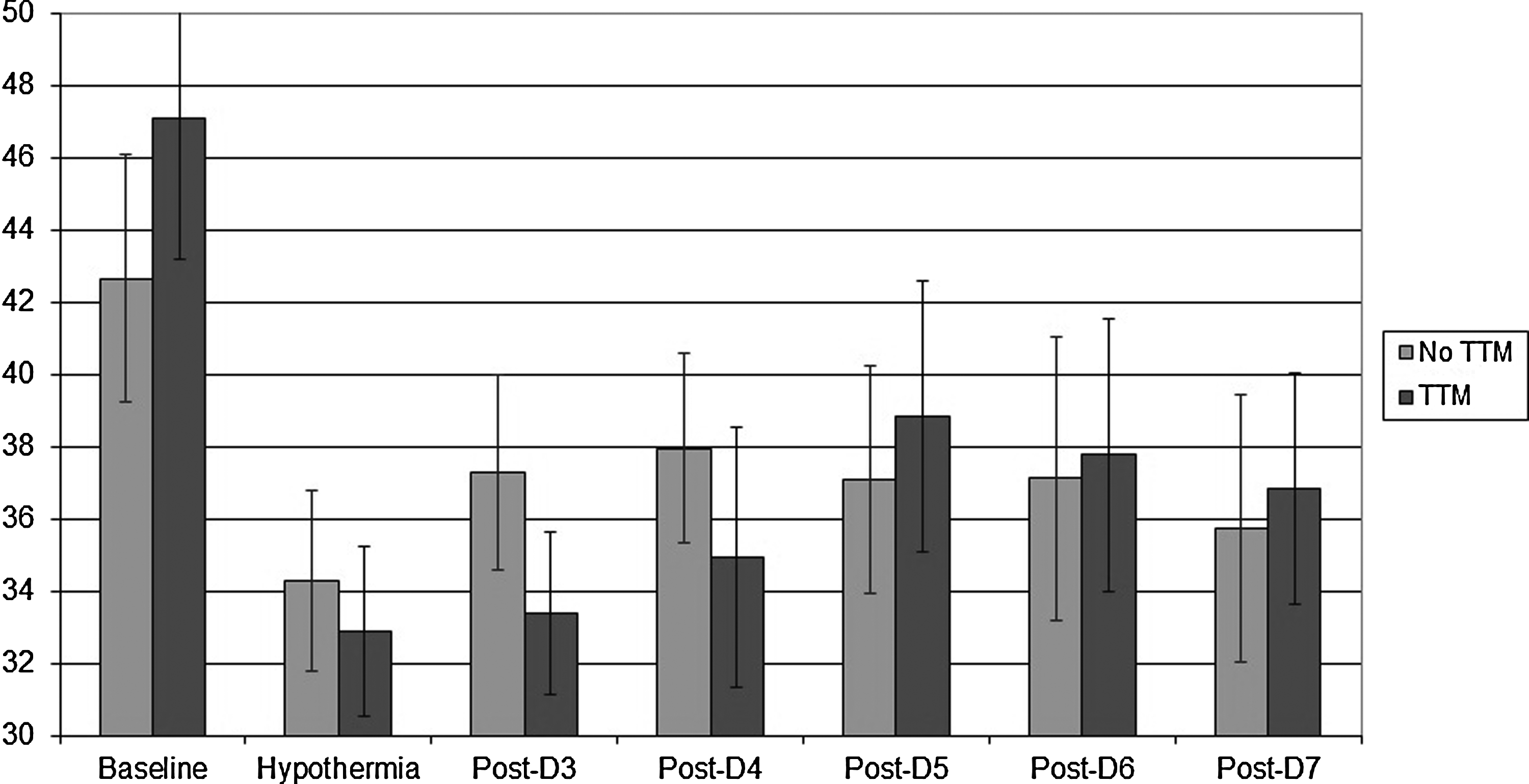
PaCO2 values for the two groups.
Clinical outcomes
TTM group received fewer days of MV (7.3±7.7 vs. 10.7±10.9, p=0.04), although this did not affect the duration of ICU or hospital LOS, ventilator-free days, or survival (Table 3). The TTM group had a significantly better CPC on discharge (3.2±1.7 vs. 4±1.3, p=0.01).
ICU, intensive care unit; LOS, length of stay; MV, mechanical ventilation; CPC, cerebral performance category.
Discussion
In this retrospective observational study of patients who suffered a cardiac arrest, individuals who received TTM demonstrated a greater decrease in PaCO2 compared with those who did not despite having consistently lower tidal volumes. Additionally, the TTM group had a favorable increase in PaO2/FiO2 by day 4 despite similar PEEP. TTM patients had better dynamic compliance following rewarming; however, variations within each group were similar.
Our observation of decreased PaCO2 in the TTM group following rewarming is consistent with results reported by Aslami et al. (2010) in postcardiac arrest patients undergoing hypothermia. The authors hypothesized that hypothermia could decrease CO2 production based on their measurement of concomitantly decreased exhaled CO2 values. Indeed, hypothermia is known to lower the metabolic rate by about 8% per degree C drop in core temperature and to also reduce oxygen consumption (Polderman and Herold, 2009). Clinically, this suggests that hypothermia may facilitate the use of lung protective ventilation. Also, similar to their findings (Aslami et al., 2010), the PaO2/FiO2 increased following hypothermia and was more greatly improved in the TTM patients than controls. Lowering of body temperature is known to result in increased stability of the oxyhemoglobin dissociation complex from the leftward shift in the oxyhemoglobin dissociation curve. However, even though less oxygen is available at the tissue level, a seeming reduction in oxygen delivery might be offset by a concomitant increase in the solubility of oxygen at decreased temperatures (Pilkington et al., 1996). Conversely, in rats with induced sepsis, a decrease in the oxygen–hemoglobin affinity was noted at 38°C, but no significant change in the blood oxygen transport capacity was observed at 34°C, yet cooled rats survived longer; the authors concluded that hypothermia might increase the survival duration by slowing down sepsis evolution (Léon et al., 2012). Clinically, hypothermia then may hasten the weaning of FiO2 to nontoxic levels in addition to potentially playing a role in those patients with refractory hypoxemia. Also, confirming the results reported by Aslami et al. (2010), TTM had no significant effect on respiratory compliance as similar changes occurred in both groups. In summary, our findings support that TTM is at least not harmful and may favorably improve parameters of both ventilation and oxygenation.
These findings add to a growing body of literature on the effect of therapeutic hypothermia on PaCO2 reduction and improved oxygenation. Historically, the first report of its implementation for the purpose of improving gas exchange dates back to 1977 where Flachs et al. (1977) noted an improvement in the PaO2 in a patient on extracorporeal membrane oxygenation (ECMO) when the temperature accidentally dropped to 34°C. Since this original human study, multiple reports and series documented the potential therapeutic or protective role of hypothermia in hypoxemic (+/− hypercapneic) respiratory failure (Hurst et al., 1985; Wetterberg and Steen, 1992; Villar and Slutsky, 1993; Moonka and Gentilello, 1996; Pilkington et al., 1996; Matsuno et al., 1997; Eriksson and Steen, 1998; Compagnoni et al., 2008; Duan et al., 2011; Varon et al., 2012). Unfortunately, many of these studies predate the definition of ARDS, as well as the advantages of modern ventilators, intensive care units and, most importantly, the use of lung protective ventilation. Despite this, implementation of hypothermia in these series has shown consistently protective effects in situations where therapeutic options are still very limited, without a signal for harm, even with prolonged application for over 48 hours (Hurst et al., 1985; Wetterberg and Steen, 1992; Villar and Slutsky, 1993; Moonka and Gentilello, 1996; Eriksson and Steen, 1998; Compagnoni et al., 2008; Duan et al., 2011). With regard to whether arterial blood gas measurements need to be corrected for body temperature (pH-stat) or not (alpha-stat), there appears to be some practice variation. A recent review of acid-base measurements in patients undergoing circulatory arrest during cardiac surgery reported better correlation with outcomes using pH-stat in pediatric patients, but alpha-stat in adults (Abdul Aziz and Meduoye, 2010).
At present, few options for management of refractory hypoxemia exist, and ECMO is not available in most centers. However, even in those patients with ARDS who do survive and leave the hospital, the hypoxemia they endured may continue to exert lasting consequences. A recent study examining risk factors for long-term cognitive impairment in ARDS survivors identified only conservative fluid strategy and hypoxemia as risk factors for long-term neuropsychological impairment (Mikkelsen et al., 2009). Given the well-established neuroprotective effect of therapeutic hypothermia (Delhaye et al., 2012), its application might prove to be beneficial even beyond the improvement in gas exchange, should it be offered to those who remain difficult to oxygenate with the use of conventional methods.
As far as potential adverse effects, the TTM group did have a significantly higher number of patients with positive urine and sputum cultures. This appears to reflect the institutional hypothermia protocol in place that schedules surveillance cultures due to the inability of the patient to mount a fever during induced hypothermia. Notably, there was no higher incidence of bacteremia. The existing literature does not support urinary tract infections as a concern in patients who receive TTM (Mongardon et al., 2011), but there may be an increased incidence of pneumonia with consequent increased duration of MV and ICU LOS, although not mortality or CPC (Kamps et al., 2011; Mongardon et al., 2011; Nielsen et al., 2011). Given that the patients in these studies have suffered a cardiac arrest, it could be difficult to separate aspiration from cardiogenic pulmonary edema from pneumonia that specifically resulted from TTM. Trials examining the outcomes of cardiac arrest survivors report pneumonia as being the most frequent infectious complication both before the era of TTM (Rello et al., 1995; Gajic et al., 2004; Tsai et al., 2005) and after (Mongardon et al., 2011; Nielsen et al., 2011; Perbet et al., 2011). A review of studies published after the implementation of TTM in cardiac arrest revealed the same incidence of pneumonia (47%) in patients who received therapeutic hypothermia compared with historical controls (Sagalyn et al., 2009). Most recent meta-analysis of 63 trials demonstrated a trend toward a higher rate of pneumonia in hypothermia compared with the normothermia group (Xiao et al., 2013). In concord with published data, despite a higher rate of positive sputum cultures in our TTM group, those patients overall had shorter ventilator days and similar ICU LOS. Other clinical variables or respiratory parameters showed no signal for harm or were favorable toward TTM.
One potential important confounder that cannot be addressed in this observational study is the effect of paralytics. The Task Force of the American College of Critical Care Medicine issued a Grade C recommendation for the use of neuromuscular blocking agents to manage ventilation and decrease oxygen consumption, but only when other means have been tried without success (Murray et al., 2002). Since then, administration of neuromuscular blockers has been shown to improve outcomes in patients with early severe ARDS in two randomized controlled trials (Papazian et al., 2010; Needham and Brindley, 2012). However, paralytics might not be beneficial for those not in ARDS: in ventilated animals with mild lung injury, spontaneous breathing actually improved oxygenation and lung recruitment; addition of paralytics was beneficial only to those with severe lung injury, where spontaneous breathing resulted in increased atelectasis (Yoshida et al., 2013). In a recent study evaluating the effect of neuromuscular blockade on outcomes of cardiac arrest patients undergoing TTM, there was no difference in the PaO2/FiO2 between the groups who did and did not receive paralytics either during hypothermia or following rewarming (Salciccioli et al., 2013). It is therefore quite plausible that the use of neuromuscular blockade has not significantly affected our findings.
There are several other important limitations to this study. This is a retrospective chart review. However, given that TTM is currently the standard of care for comatose cardiac arrest survivors, a prospective trial involving a control group without temperature management would not be ethical. Moreover, our control group consisted of mostly historic patients who appeared to have had different ventilator settings overall as evidenced by consistently higher tidal volumes. Thus, differences between groups may reflect changes in practice over the decade, in which this cohort was identified rather than an effect of TTM. We were surprised at the overall low adherence to the low-tidal-volume strategy as well, and it may mitigate the effect observed between those who received TTM and those who did not. Additionally, controls were selected on the basis of receiving a minimum of 3 days of MV following arrest, introducing a selection bias on respiratory outcomes; however, no other way of identifying a comparable group with complete variables was feasible. Reassuring, however, is that most of the patient characteristics, which could influence measured respiratory outcomes, particularly the severity of illness scores, cumulative daily fluid balance, the amount of transfused blood products, blood pressure, and medications that may affect lung injury, were well balanced between the two groups. Comparing outcomes and these modifying factors to a control group of patients, who did not receive TTM, is the strength of our study as it helps to confirm whether the potential benefits in respiratory mechanics observed in the prior single arm observational study of patients with TTM (Aslami et al., 2010) are sustained posthypothermia and hold true when compared with a reasonable control group. Despite the lack of perfect controls, short of a randomized controlled study, we feel this observational study provides additional insight and evidence for the potential benefits of TTM on respiratory mechanics.
The clinical implication of our findings could be a consideration for systematic study of TTM as a potential therapy for patients with severe hypoxemia. Ours and other studies support that specific clinical benefits may be derived through improvements in both ventilation and oxygenation, although theoretical benefits at the inflammatory level also exist, as well as potential long-term neurocognitive effects. At what severity of hypoxemia and to what extent TTM should be implemented is unclear, but given the potential benefits in oxygenation and ventilation, it might first be considered in those patients with severe ARDS or PaO2/FiO2<100 despite PEEP or where lung protective ventilation is difficult to achieve (plateau pressure >30 or VT>6 mL/kg). The widespread use in clinical practice cannot be advocated as of yet.
Conclusions
The use of TTM in cardiac arrest survivors suggests favorable and nonharmful gas exchange and respiratory mechanics effects. Based on this and prior studies, we feel that systematic studies on the role of TTM in patients, with severe hypoxemia or ARDS, as a potential rescue therapy may be justified.
Footnotes
Disclosure Statement
No competing financial interests exist.