
Abstract
Hypothermia is known to be neuroprotective and is one of the most effective and promising first-line treatments for central nervous system (CNS) trauma. At present, induction of local hypothermia, as opposed to general hypothermia, is more desired because of its ease of application and safety; fewer side effects and an absence of severe complications have been noted. Local hypothermia involves temperature reduction of a small and specific segment of the spinal cord. Our group has previously shown the neuroprotective effect of short-term, acute moderate general hypothermia through improvements in electrophysiological and motor behavioral assessments, as well as histological examination following contusive spinal cord injury (SCI) in rats. We have also shown the benefit of using short-term local hypothermia versus short-term general hypothermia post-acute SCI. The overall neuroprotective benefit of hypothermia can be categorized into three main components: (1) induction modality, general versus local, (2) invasive, semi-invasive or noninvasive, and (3) duration of hypothermia induction. In this study, a series of experiments were designed to investigate the feasibility, long-term safety, as well as eventual complications and side effects of prolonged, semi-invasive, moderate local hypothermia (30°C±0.5°C for 5 and 8 hours) in rats with uninjured spinal cord while maintaining their core temperature at 37°C±0.5°C. The weekly somatosensory evoked potential and motor behavioral (Basso, Beattie and Bresnahan) assessments of rats that underwent 5 and 8 hours of semi-invasive local hypothermia, which revealed no statistically significant changes in electrical conductivity and behavioral outcomes. In addition, 4 weeks after local hypothermia induction, histological examination showed no anatomical damages or morphological changes in their spinal cord structure and parenchyma. We concluded that this method of prolonged local hypothermia is feasible, safe, and has the potential for clinical translation.
Introduction
S
Contusive SCI is characterized by three main phases (Dietrich, 2009, 2011a; Gupta et al., 2010; Kwon et al., 2010). The primary phase includes hematoma formation and development of necrosis at the injury epicenter that occurs within hours of impact. Subsequently, the secondary phase of injury develops within days progressing to months upon onset of injury. It is accompanied by an irregular progression of cavity formation, a delayed degeneration of surrounding neural tissue and thus further destruction of healthy neural pathways and spinal cord parenchyma. These processes augment inflammation, demyelination, apoptosis, and necrosis. Following this, the tertiary phase of injury develops over years. One of the primary focuses in the field of translational SCI research and designing therapeutic strategies is preventing or limiting the secondary phase of injury.
Acute general and local induction of hypothermia as a first line of neuroprotection postcontusive SCI is the focus of research in our laboratory. Acute hypothermia has been investigated in this study and other studies as a neuroprotective treatment with encouraging results for a variety of conditions such as stroke (Piironen Auriat, 2014), cerebral aneurysm (van der Worp et al., 2007; Chang and Marshall, 2012; Lakhan and Pamplona, 2012), traumatic brain injury (TBI) (Marion et al., 1997; Faridar et al., 2011; Lotocki et al., 2011), cardiac arrest (The Hypothermia after Cardiac Arrest Study Group, 2002; Arrich, 2007; Belliard et al., 2007; Bro-Jeppesen et al., 2009; Batista et al., 2010; Beddingfield and Clark, 2012), and ischemia–reperfusion injury (Kawamura et al., 2006). Studies with mild (>33°C) and moderate (<32°C) hypothermia have also shown benefits in the treatment of SCI (Kwon et al., 2008; Dietrich et al., 2009, 2011b).
The true mechanism of the neuroprotective effects of hypothermia is yet to be fully understood. Acute hypothermia treatment applied soon after contusive SCI is hypothesized to reduce (1) metabolism and consumption of oxygen and glucose, (2) the risk of energy failure and cell death, (3) excitotoxic neurotransmitter release, (4) free radical formation, (5) sustained electrical depolarizations, (6) proinflammatory and apoptotic pathways, (7) edema, (8) inflammation, as well as (9) stabilize the blood–brain barrier.
There are two main methods of hypothermia application, general and local. General hypothermia involves temperature reduction of the entire body. It is an easy and, to a limited extent, an effective method of treatment in patients with acute SCI. However, serious complications have been reported with inducing general hypothermia, which makes it less than ideal as a first line of treatment (The Hypothermia after Cardiac Arrest Study Group, 2002; Levi et al., 2010). The major clinical complications include the following: (1) peripheral vasoconstriction, which may cause kidney dysfunction, (2) onset of bradycardia that results in reduced myocardial contractility, cardiac output, blood pressure, and consequently cardiac fibrillation, (3) impaired leukocyte phagocytic function and hence immunosuppression, (4) mild coagulopathy and platelet dysfunction, (5) failure of thermoregulatory defense and shivering, (6) raised blood pH through increased CO2 solubility and decreased pCO2, (7) hyperglycemia through insulin resistance, and (8) hypoglycemia through increased insulin sensitivity during rewarming.
Local hypothermia, that is, temperature reduction of only a short and specific segment of the spinal cord, is currently considered a promising first line of treatment for acute contusive SCI. Local hypothermia could be classified into the following: invasive, semi-invasive, and noninvasive categories (the more invasive the procedure, the less clinically applicable). Invasive methods of inducing hypothermia require major surgical procedures (including laminectomy), which would unlikely be used in a clinical setting, especially for patients with acute SCI. On the other hand, semi-invasive methods involve minor surgical procedures that may be the treatment of choice for SCI patients. Noninvasive methods, which are the most desirable, are easy to execute. However, they present difficulties in localizing and maintaining the desired temperature for the necessary period of time (Yoshitake et al., 2007; Levi et al., 2010; Morizane et al., 2012; Li et al., 2013). In this study, we investigated the feasibility of localizing and maintaining prolonged moderate local hypothermia through a semi-invasive method that could easily be translated to a noninvasive method applicable in clinical settings.
Most studies of SCI therapy are based on general hypothermia. Expectedly, animal models of general hypothermia post-SCI have shown improvements in locomotion, cortical evoked potentials, as well as reduced damage in the spinal cord tissue (Yu et al., 2000; Lo et al., 2009; Maybhate et al., 2012). Furthermore, current methods of local hypothermia used in animal studies are either mostly invasive or efficacious appearing for a short period of time. To date, only a few groups, including ours, have developed a clinically applicable semi-invasive method to effectively induce local hypothermia. However, our study does not follow the general trend because it investigates the beneficial effects of inducing prolonged acute, moderate, and local hypothermia through a semi-invasive method that can be translational.
An editorial note by Prof. Dalton Dietrich on our previous publication (Maybhate et al., 2012) suggested that our results provide evidence that the duration of hypothermia induction postacute SCI could play a major role in contributing to potential long-term benefits (Dietrich, 2009, 2012). We have shown improvements in electrophysiological (somatosensory evoked potentials [SSEPs]) and motor behavior (Basso, Beattie, and Bresnahan [BBB] score) assessments as well as histological examinations after 2 hours of moderate general hypothermia in a contusive rat model of SCI (induced 2 hours postinjury). Interestingly, the electrophysiological improvements (increased amplitude) were sustained for up to 1 month posthypothermia induction. In addition, we described that although this is a temporary improvement, it increases the time-wise window of opportunity for treatment administration targeted at permanent benefits (Maybhate et al., 2012).
In 2014, in another study, our group also demonstrated the benefits of using short-term local hypothermia versus short-term general hypothermia post-SCI. One important observation was that general hypothermia induction reduces the temperature of the entire central nervous system (CNS), including the brain, which is one of the undesired effects of general hypothermia induction. In contrast, local hypothermia induction does not affect the cortex, thus indicating greater benefit, effectiveness, and less complication (Bazley et al., 2014b). As a follow-up to our previous studies, we have extended our studies to investigate the potential risks and benefits of prolonged, local, acute moderate hypothermia induction through a semi-invasive method, in consideration of the translational feasibility of this study design into eventual clinical trials. In this study, we investigated the potential complications and eventual harmful effects after 5 and 8 hours of local hypothermia induction in the thoracic region of the spinal cord. For this purpose, motor behavioral and histological examinations as well as electrophysiological assessments, an objective tool to detect even very minor insults to the CNS, were carried out. The innovative aspect of this research lies in prolonging the duration of local moderate hypothermia induction through a novel semi-invasive method, which can also be considered for clinical application.
Materials and Methods
All procedures were performed in accordance with protocols approved by the Institutional Animal Care and Use Committee of the National University of Singapore. In total, 15 adult female Sprague-Dawley rats (200–220 g; CARE) were used in this study. Rats were housed in individual cages, due to their skull electrode implantation, and were provided with food and water for self-consumption throughout the study period.
Animals were divided into three groups: control (n=5), 5-hour hypothermia (n=5), and 8-hour hypothermia (n=5). All animals were subjected to laminectomy as described below.
Anesthesia
To induce anesthesia for skull electrode implantation, rats were given a mixture of ketamine (75 mg/kg) and xylazine (10 mg/kg) through intraperitoneal injection (0.2 mL/100 g body weight). To induce anesthesia for surgical procedures and prolonged hypothermia, individual rats were held in a transparent chamber containing a mixture of 2% isoflurane gas and room air until the onset of drowsiness. The mouth and nose were then placed within an anesthesia mask (using a rodent size diaphragm that fits well and uses a C-Pram circuit designed to deliver and evacuate the gas through one tube) connected to a mixed flow of 1.5% isoflurane, 80% oxygen, and room air at a flow rate of 1.5 L/min. Ophthalmic ointment was also applied to the eyes following induction of anesthesia to prevent corneal drying.
Transcranial electrode implantation for SSEP recordings
An incision was made in the skin of the head, and the tissue under the skin was removed to clean the cranium bone. Four burr holes were drilled into the cranium near the forelimb and hindlimb somatosensory cortex areas of the right and left hemispheres. A fifth hole was drilled near the lambda for the reference electrode. Transcranial electrodes (E363/20; Plastics One, Inc.) were screwed into the holes such that very light contact was made with the dura mater without compressing the brain tissue. These electrodes were then fixed with dental cement. The head wound was closed and 2% lidocaine gel was applied. This was used for SSEP signal recordings and monitoring.
Laminectomy
Laminectomy is a secure and simple way to expose the spinal cord. It was executed using a Zeiss operating microscope. The laminectomy was performed at thoracic vertebra T8 to expose the dorsal surface of the spinal cord. Extra care was taken to ensure that the dura mater remained intact, which is important in obtaining SSEPs free of noise and artifacts. At the end of the experiment, the paravertebral muscle layers and skin were sutured closed. Rats did not undergo any SCI.
Local hypothermia induction
After induction of general anesthesia, an M-shaped heat exchanger comprising a 10-cm-long, 15-mm-wide, and 2-mm outer-diameter copper tube was inserted in the lower dorsal region of the spinal cord, with the T8 region being in the center. Both ends were connected to a pair of silicon tubes (80 cm long and 2 mm outer-diameter) to form a closed perfusion system. An intrathecal sensor was used to measure the temperature of the spinal cord locally, which was maintained at 30°C±0.5°C. A 2-cm transverse incision at the sacral area was made to open the skin. We made a long tunnel in the subcutaneous tissue from L1 to T4. The M-shaped copper tube was placed over the region of interest (T6 to T10), after which the skin was sutured firmly. An ice water bath reduced the temperature of water to ∼14°C. Cold water was circulated through the tubing at a rate of 120 mL/min using a peristaltic pump (Manostat; model Vera). We used the same circulation system through the M-shaped copper tube for gradual rewarming of the animal's spinal cord. This method allowed for a gradual, constant, uniform, and manageable local hypothermia of rat spinal cords. The experimental setup is shown in Figure 1. We induced selective local hypothermia by reducing the intraparenchymal temperature by ∼1°C every 2 minutes, starting from a normal temperature of ∼37°C to a desired temperature of 30°C. It took 15 minutes to reach the target of 30°C. Thereafter, we maintained local hypothermia for either 5 or 8 hours. Rewarming to 37°C was gradual and ∼1°C every 5 minutes for 30 minutes. A 5-cm rectal probe was used to monitor the core temperature, and rats were placed on a heating pad to maintain their body temperatures at 37°C±0.5°C throughout the experiments (Agrawal et al., 2009, 2010a, 2010b; Bazley et al., 2011; Bazley et al., 2012, 2013, 2014a; Yenari and Hans, 2012) (Fig. 1). The spinal cord temperature profile of rats during 5- and 8-hour hypothermia experiments is shown in Figure 2.
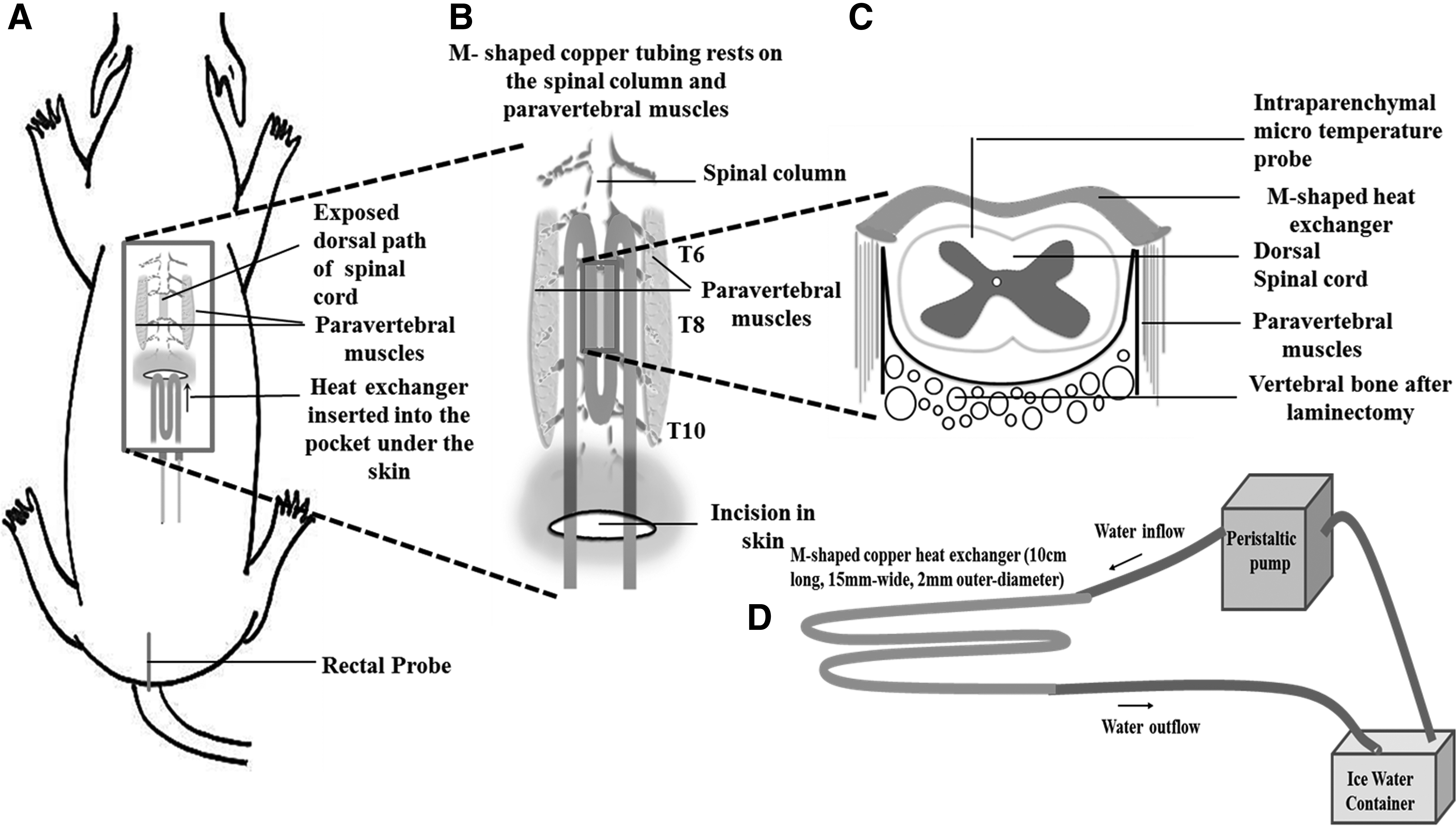
Experimental setup for inducing semi-invasive local hypothermia using the copper heat exchanger.

Scatter plot of temperature during the five phases (Observation, Cooling, Hypothermia, Rewarming, and Stabilization) 5 hours
Electrophysiological monitoring
SSEPs are widely used to study the functional integrity of ascending dorsal sensory pathways. In current clinical practice, SSEPs are used for several diagnostic purposes such as intraoperative monitoring during high-risk surgeries and in patients with neurological deficits for the purpose of monitoring conductance and integrity of neuropathways. To monitor SSEPs, four pairs of stainless-steel stimulating needle electrodes (Safelead F-E3-48; Grass Technologies) were placed in proximity to the tibial nerves in the right and left hindlimbs and to the median nerves in the right and left forelimbs. A reference needle electrode was placed subdermally at the neck. The needle electrodes were connected to a stimulus generator (Digitimer Ltd.). OpenEx software was used to control the stimulator. The cranium screw electrodes were connected to an amplifier for the recording of SSEP signals. The stimulus generators generated stimulating pulses of 3.5 mA intensity and with a pulse width of 200 microseconds at a rate of 1 Hz, sequentially stimulating each of the four limbs (right forelimb→left forelimb→left hindlimb→right hindlimb→right forelimb and so on). In total, ∼150 sweeps were recorded per limb per electrode. The neuroelectrophysiology monitoring setup (Tucker-Davis Technology) was used for multilimb acquisition of SSEPs as previously described (Agrawal et al., 2010b; Bazley et al., 2011; Maybhate et al., 2012). Upon each stimulation, SSEP signals were recorded simultaneously from all four cortical screw electrodes using the amplifier and data acquisition setup. A baseline recording was taken for each animal before hypothermia induction and weekly thereafter for 4 weeks.
Histological examination
After 28 days, spinal cords were harvested from the control and hypothermia-treated rats. The animals were deeply anesthetized and perfused with freshly prepared 4% paraformaldehyde. The spinal cord column was gently removed, fixed in paraformaldehyde for 4 hours, and subsequently in 15% sucrose overnight at 4
Postoperative care, pain management, and euthanasia
Rats generally regained consciousness 30 minutes after the experiments. For hydration, the rats received subcutaneous injections of isotonic saline (20 mL/kg) administered daily for 5 days. The care and treatment of rats were in strict accordance with the guidelines set by the Responsible Care and Use of Laboratory Animals and the guidelines for the Use of Animals in Neuroscience Research and National University of Singapore IACUC. Topical analgesic (lidocaine 2% gel) was applied to the sites of incision. Buprenorphine (0.05 mg/kg; 0.2 mL/100 g body weight) was given postoperatively twice a day for 5 days to relieve pain from the paravertebral muscle. The gentamicin (8 mg/kg; 0.2 mL/100 g body weight) antibiotic was given postsurgery for 5 days. Rats were never allowed to regain consciousness throughout the experimental procedures. Rats were deeply anesthetized and then euthanized through transcardial perfusion with formaldehyde. The rats' spinal cords were harvested for histological studies.
Results
Analysis of electrophysiological assessment
The SSEP signals within a window between 0 and 40 milliseconds after the stimulation were extracted. The average SSEP was derived by calculating the mean of ∼150 single sweeps. From the average SSEP waveform, two parameters were defined: amplitude representing the total peak-to-peak value of the signal within 5–40 milliseconds after the stimulation and N1 latency representing the time from the stimulation to the first negative peak in the SSEP. The derivation of the average SSEP waveform as well as signal parameters is illustrated in Figure 3.

Determination of the average somatosensory evoked potential (SSEP) waveform as well as the amplitude and N1 latency signal parameters. The average SSEP waveform is calculated by averaging the 150 single sweeps. The signals represent the recordings of one rat during left hindlimb stimulation. The stimulation happens at time 0.
In the baseline recordings of the 15 rats, the SSEP amplitude and N1 latency values (mean±SD) were 164.9±58.0 μV and 20.3±2.6 milliseconds on the left hindlimb and 142.7±48.3 μV and 18.9±2.3 milliseconds on the right hindlimb, respectively. Figure 4 shows how the parameter values changed on different recording days in the three study groups; control, 5 hours, and 8 hours hypothermia. There were no changes in amplitude and N1 latency after 5 and 8 hours of local hypothermia induction. The difference in the parameter values among rats in the control (n=5), 5-hour hypothermia (n=5), and 8-hour hypothermia (n=5) groups was statistically nonsignificant throughout the 4 weeks.

The amplitude and N1 latency values of SSEPs in the control (n=5), 5-hour hypothermia (n=5), and 8-hour hypothermia (n=5) groups on different recording days. The values for the postoperative days 7, 14, 21, and 28 (D7–D28) are given as a percentage compared to the baseline (BL) recording and represent group means and standard deviations. The difference between the values of the control and 5-hour hypothermia groups as well as the control and 8-hour hypothermia groups was not statistically significant (p>0.05) at any of the postoperative recordings.
The SSEP amplitude and latency values were statistically compared between the control group and the 5-hour hypothermia group as well as the control group and the 8-hour hypothermia group over a 4-week observation period. The comparison was carried out using the two-sample t-test where p-values<0.05 were considered to be statistically significant. We detected no statistically significant changes among the groups.
We detected no statistically significant changes among the groups (Table 1). The statistical test was designed to have a power of 0.90 to show a 50% drop in the amplitude (mean=100, SD=25) and a 10% increase in the N1 latency (mean=100, SD=5) with a significance level of 0.05.
The results show that no statistically significant changes were observed among the groups.
Histological examination and results
Representative images of the proximal (T6), epicenter (T8), and distal (T10) regions of the stained spinal cord are shown in Figure 5 (Fig. 5A: 5-hour hypothermia, Fig. 5B: 8-hour hypothermia, Fig. 5C: control). Observation of the spinal cord parenchyma shows that there was no discernible damage or hemorrhage. This indicates that the process of laminectomy and semi-invasive prolonged local hypothermia induction did not cause any injury at the region of interest in the spinal cord. This is also consistent with SSEP results.
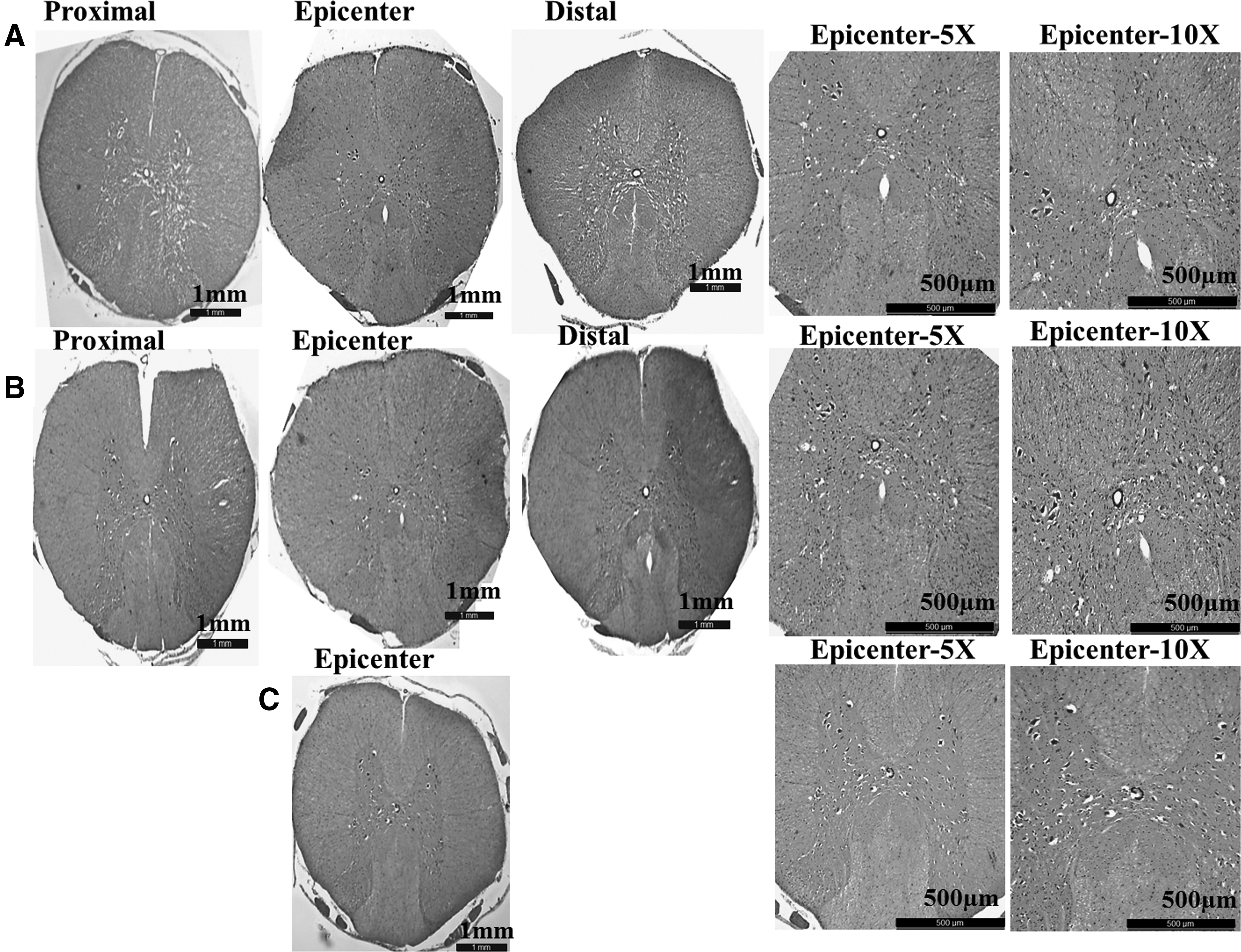
Hematoxylin and eosin staining of the spinal cord tissue at day 28 after
Motor behavior evaluation
The BBB score from 0 to 21 was used to assess joint movement, hindlimb movements, stepping, limbs coordination, trunk position, paw placement, and tail position (Basso et al., 1995, 1996). The BBB scoring of 15 rats in control, 5-, and 8-hour hypothermia groups revealed no deficits in motor behavior. The analysis of the motor behavior scores also showed no statistically significant changes (Fig. 6).

Graph plot shows the motor behavior scores of 5 hours
The analysis of the motor behavior scores also showed no statistically significant changes. The average BBB scores for 5- and 8-hour hypothermia groups at day 28 were 20.8 (p=1.00) and 21.0 (p=1.00), respectively. The scores were statistically compared with the control group using the Mann–Whitney U test suitable for data not following a normal distribution. p-values<0.05 were considered statistically significant.
Discussion
Many studies of SCI involving both contusion and compression injury also observe improved outcome and reduced damage in spinal cord tissue posthypothermia therapy (Martinez-Arizala and Green, 1992; Yu et al., 2000; Dietrich, 2009; Dietrich et al., 2009; Batchelor et al., 2010). General hypothermia has shown promise in studies of TBI, cardiac arrest, as well as SCI (Dietrich et al., 2011a). Although the mechanism is not known yet, it appears that hypothermia may improve the functional outcome in the CNS (Lotocki et al., 2011). Lotocki et al. (2011) showed that 4 hours of general or local hypothermia improves functional outcome in rats with TBI by reducing oligodendrocyte cell death. Other studies of TBI have also shown positive results of hypothermia therapy (Faridar et al., 2011). General hypothermia therapy has also been shown to reliably improve the survival rate in patients postcardiac arrest (Belliard et al., 2007; Bro-Jeppesen et al., 2009; Batista et al., 2010). Others as well as our research has shown that although general hypothermia could be considered an effective acute therapeutic strategy in patients with trauma to the CNS, it is known to be associated with severe complications (The Hypothermia after Cardiac Arrest Study Group, 2002; Melhuish, 2009; Polderman and Herold, 2009; Lenhardt, 2010; Levi et al., 2010). Hence, local hypothermia offers a promising alternative to general hypothermia. Because hypothermia is localized, most of the adverse effects of general hypothermia could be avoided while still attaining the benefits of hypothermia induction as a treatment for traumatic CNS injuries (Zhang et al., 2007; Batista et al., 2010; Levi et al., 2010).
The objective of our study was to evaluate the safety of prolonged moderate local hypothermia through a semi-invasive method in the spinal cord and the rest of the CNS. We also investigated whether a long duration of hypothermia at 30°C caused any side effects in rodents' biological systems. To attain this, in addition to traditional motor behavior scoring and histological examination, we implemented an objective method (SSEP) to assess the integrity of the entire CNS.
The aim of this study was to prove the concept and pave the way for designing a translational experimental procedure, in which local hypothermia can be applied in a noninvasive manner as a first line of treatment in patients with acute SCI. While existing literature has described the safety and neuroprotective effects of hypothermia induction, there are currently no studies reporting the effect of prolonged 5 and 8 hours of local hypothermia on the spinal cord. For instance, in a previous study carried out by Auriat et al., 2012, the authors investigated the effects of 3-day systemic hypothermia (32°C) in rats. In addition, they cooled the right hemisphere of rats for either 3 or 21 days to assess the impact of longer durations of focal cooling on the brain and observed no detrimental damage, indicating that prolonged hypothermia does not cause harm to the healthy brain (Auriat et al., 2012). In our experiments, the motor behavior and electrophysiological recordings were performed weekly for 28 days. The histological examination of spinal cords was carried out at the end of 4 weeks of observation. Statistical analyses of BBB and SSEP in rats that underwent semi-invasive 5 and 8 hours of local hypothermia showed no significant changes in comparison to the control group. Although laminectomy was performed in our experimental procedure, to measure temperature changes in the spinal cord, it is feasible to mimic the same measurement even without any invasive surgical procedure in patients using sophisticated instruments available today.
We have previously shown the benefit of 2 hours of general hypothermia in a contusive model of SCI (Maybhate et al., 2012). While extending the duration of hypothermia treatment might potentially improve its therapeutic effect, the possible harmful effects of such treatment on the CNS need to be studied. In this respect, we have shown that prolonging local hypothermia is safe and could be translational in clinical settings.
Compared to previous studies, the present study has important novelties. First, while most studies have used target hypothermia temperatures of 32°C–33°C–34°C (Khan et al., 2007; Kang et al., 2010; Grulova et al., 2013; Saito et al., 2013), a lower target temperature of 30°C was used in our experiment. This temperature was considered close to that of therapeutic general hypothermia (32°C) induced 2 hours after contusive SCI (Maybhate et al., 2012). Second, local hypothermia was prolonged to meet the needs of clinical application to desired durations of 5 and 8 hours (Lotocki et al., 2011; Grulova et al., 2013; Saito et al., 2013).
In this study, we reported the local hypothermia treatment to have no long-term or permanent adverse effects on SSEPs, motor behavior, and anatomical structure. However, in the first week after hypothermia induction, the SSEP amplitudes varied quite strongly in the group of animals that underwent 8 hours of local hypothermia. This variation in amplitudes was mainly related to anomalous recordings in a few subjects in which the amplitude paradoxically increased, following local hypothermia induction. One explanation for this could be the increased isoflurane tolerance of these subjects. Anesthetics have been shown to affect both electroencephalography and SSEP measures (Kortelainen et al., 2008, 2014). In the 8-hour hypothermia group, the rats were exposed to the anesthetic for a longer period of time due to the experimental requirements. The possible increased drug tolerance could have resulted in lighter anesthesia during the subsequent recordings that were temporally close to the treatment leading to the increase of SSEP amplitudes.
Future studies will establish the efficacy and safety of local hypothermia as a therapeutic strategy in the hostile environment of a contused spinal cord. Efficacy will be assessed using objective electrophysiological assessments as well as motor behavior examinations. Cell apoptosis, demyelination, and axonal injury assays will determine the safety of semi-invasive, local moderate hypothermia treatment.
Footnotes
Acknowledgments
This research was supported by the National University of Singapore (NUS) grant: R-175-000-122-112 (Tier 1, PI: A. All) and R-175-000-121-133 and R-175-000-121-733 (Start-Up, PI: A. All), and the Singapore Institute for Neurotechnology (SINAPSE, PI: A. All) Institute Seed Fund. It was also supported by the Maryland Stem Cell Research Fund grant proposal (2013-MSCRFII-0109-00, PI: A. All) and the National Institutes of Health under grant 5R01HL071568 (PI: N. Thakor).
Author Disclosure Statement
No competing financial interests exist.