
Abstract
In this case report, a 22-year-old male developed severe hypothermia after an accidental overdose of cyclobenzaprine. During transport, the patient developed cardiac arrest. He received active rewarming measures, including pleural lavage, gastric lavage, an intravascular heat exchange catheter, and cardiopulmonary bypass. Intravenous lipid emulsion (ILE) was also administered. A discussion of cyclobenzaprine toxicity, hypothermia, ILE, and accidental hypothermic cardiac arrest follows.
Introduction
A
The BLS crew placed a nasopharyngeal airway and assisted ventilation with supplemental oxygen. Advanced life support (ALS) arrived 5 minutes later and found a blood pressure of 105/88, pulse of 88, respirations of 4, and Glasgow Coma Scale of 3. The patient received 2 mg intranasal naloxone through a mucosal atomization device immediately, while intravenous (IV) access was obtained. After no response, the crew performed endotracheal intubation. Initial end-tidal carbon dioxide capnography was 28 mmHg. Initial rhythm is noted in Figure 1. Under standing orders, ALS gave an additional 1 mg naloxone IV with no response and a 12-lead electrocardiogram (ECG) was obtained (Fig. 2).

Initial rhythm on monitor demonstrating Osborne waves.
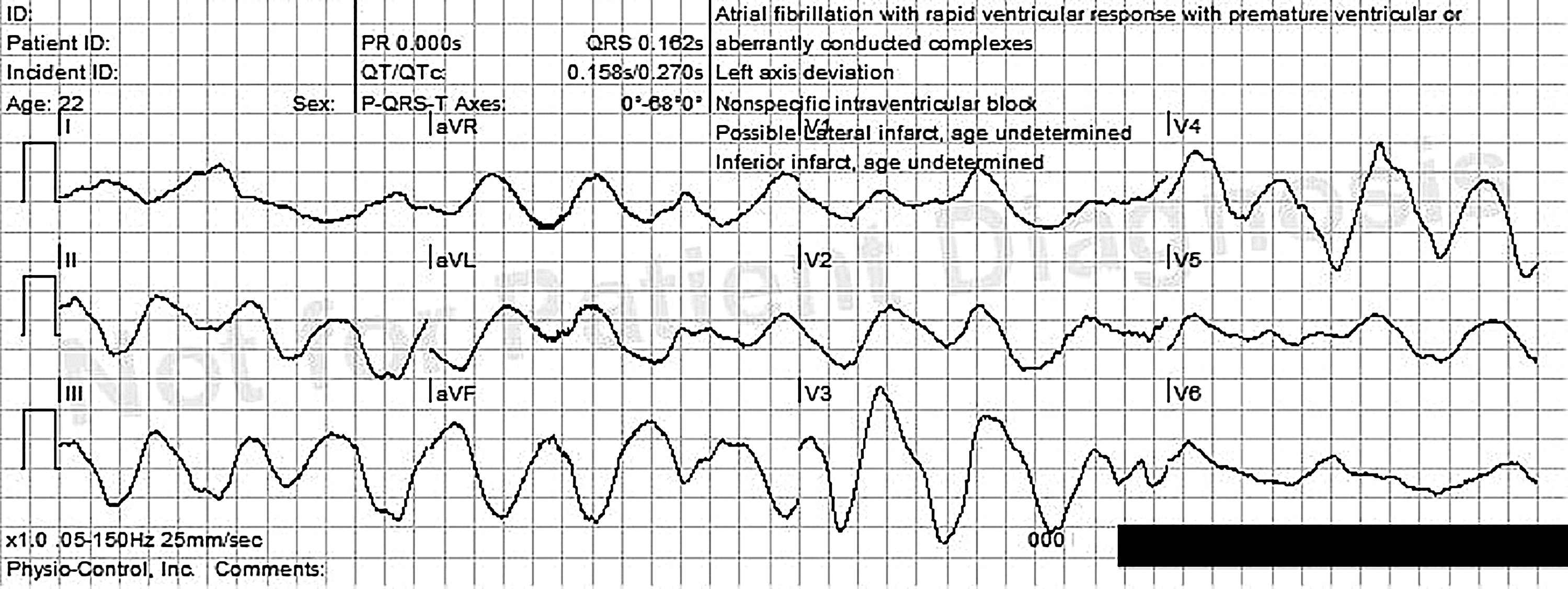
Rhythm following administration of naloxone.
Although the patient was found indoors, it was noted during medical control that the bedroom window was open, resulting in a cold environment. Since the crew lacked any means of obtaining a core temperature in the ambulance, avoiding any sudden movement to limit irritating potentially hypothermic myocardium was discussed. Given the sine wave on the ECG, the physician gave orders for 50 mEq of sodium bicarbonate and 1 gm of calcium chloride. Despite the sine wave rhythm, the patient's pulse ranged between 49 and 78 beats per minute, systolic blood pressure ranged from 104 to 129 mmHg, end-tidal capnography was 11 to 28 mmHg, and respiratory effort was weak.
About 15 minutes into transport and just moments before arrival at the hospital, the ambulance ran over a series of pot holes, shaking all items in the patient compartment. After the artifact settled on the cardiac monitor, the patient was noted to be in coarse ventricular fibrillation. The crew started cardiopulmonary resuscitation (CPR) and defibrillated the patient with no change in cardiac rhythm before arriving at the hospital. An IV bolus of 300 mg amiodarone was given, along with 1 mg epinephrine. The patient arrived in the emergency department (ED) in cardiac arrest with ventricular fibrillation on the monitor. Staff continued CPR and advanced cardiovascular life support (ACLS) protocols, with additional defibrillation attempts, epinephrine 1 gm calcium chloride and 50 mEq sodium bicarbonate IV pushes. Rectal temperature (Welch Allyn SureTemp® Plus 692, Skaneateles Falls, NY) was unobtainable, as the temperature was below the lower limit of measurement of 26.7°C (80°F). Additional IV access was obtained and warm fluid boluses of 0.9% sodium chloride were administered. A temperature-sensing Foley revealed a core of 23.3°C (74°F). Efforts were then focused away from ACLS and toward rewarming measures. An orogastric tube was placed and continuous warm fluid gastric lavage was started. Seven minutes after arrival, the patient had a femoral countercurrent heat-exchanging central line placed (ZOLL ICY Model No. IC-3893, Chelmsford, MA) connected to an intravascular temperature management system (ZOLL Thermogard XP® Temperature Management System). After 23 minutes, the patient's temperature had increased to 26.3°C (79.3°F), and the patient remained in cardiac arrest with ventricular fibrillation.
The patient's family arrived 40 minutes into the resuscitation and reported that the patient may have ingested as many as thirty 10 mg cyclobenzaprine tablets. The ED pharmacist at bedside started a 150 mEq sodium bicarbonate in 5% dextrose infusion at 150 mL/h and a 100 mL bolus of intravenous lipid emulsion (ILE) was given. Temperature was unchanged from 26.3°C. At 50 minutes, two right-sided chest thoracostomy tubes were placed, and warm sterile saline lavage was started. Before insertion of the left-sided chest thoracostomy tubes, the cardiothoracic team arrived in the ED. The patient's temperature was 26.9°C (80.4°F), and occasional respiratory efforts and organized QRS complexes were seen. However, the patient remained pulseless. The patient went to the operating room for cardiopulmonary bypass through femoral cutdown access 74 minutes after arrival to the ED.
Discussion
Accidental hypothermia and hypothermic cardiac arrest
Accidental hypothermia has been defined as an involuntary drop in core body temperature below 35°C (95°F) (Silfvast and Pettila, 2003). Primary hypothermia occurs when the heat production mechanism in a healthy individual becomes overwhelmed by environmental conditions. Patients who have illness that blunts their ability to maintain stable body temperature suffer from secondary hypothermia. These patients, in general, succumb to their primary medical condition and not hypothermia (Brown et al., 2012). Our patient presented with primary and secondary hypothermia due to cyclobenzaprine overdose, an agent that may have central and peripheral nervous system antimuscarinic activity, potentially influencing temperature regulation (Cheshire and Fealey, 2008).
Hypothermia is classified as mild (35–32°C, 95–89.6°F), moderate (32–28°C, 89.6–82.4°F), and severe (<28°C, 82.4°F) (Danzl, 2007). As core temperature of a patient drops below 30°C (86°F), the likelihood of cardiovascular collapse increases significantly and is associated with severe morbidity and mortality (Larach, 1995; Brown et al., 2012).
Due to the lack of large databases of such patients, treatments are varied and based on individual practitioner experience or guidelines, which have limited supporting data (van der Ploeg et al., 2010).
EMS personnel can use clinical signs and the Swiss staging system to describe hypothermic patients (Durrer et al., 2003). Rescue collapse is the term for cardiac arrest that occurs during extrication or transport of a hypothermic patient, possibly due to myocardial irritability (Brown et al., 2012; Schober et al., 2014). Similar to our patient, a retrospective cohort analysis of 18 accidental hypothermic cardiac arrest patients showed that 67% were a result of rescue collapse (Schober et al., 2014). Intoxication and the initial presence of Osborne waves are each significantly associated with improved rates of survival with the odds ratios of 28 and 16, respectively; 50% of the cohort survived to hospital discharge and all had good neurological outcomes. EMS providers may minimize movements of the profoundly hypothermic patient to avoid rescue collapse, but transport to the hospital is necessary.
Accurate core temperature measurement is a challenge. Core temperature sensing devices with low-range accuracy are rarely available in the prehospital setting. Oral and axillary temperatures are generally unreliable, and rectal temperatures may fail to accurately reflect core temperature and may have a significant lag (Corneli, 2012). Tympanic temperature is an option and was initially used in the 2002 therapeutic hypothermia trials, but only until pulmonary artery catheter (PAC) or bladder sources were available (Hypothermia after Cardiac Arrest Study 2002) (Bernard et al., 2002). Their utility in the very low range is unclear. Esophageal and urinary catheter probes are preferred, but can give false readings when warm gastric or bladder lavage is used for rewarming. In one study, investigators observed that bladder temperature correlated with brain temperature better than rectal and PAC temperature measurements in neurosurgical patients undergoing cardiopulmonary bypass and deep hypothermia with mean temperatures of 21.3°C (70.3°F) (Camboni et al., 2008). Furthermore, an irritable myocardium may be a concern with PAC placement during profound hypothermia. In this case, a bladder catheter was used to monitor rewarming efforts in the absence of warm bladder lavage. It was directly linked to the Thermogard XP Temperature Management System (can also use esophageal catheter or PAC probes) to provide an auto feedback loop temperature regulation.
In the prehospital setting, the goal is to prevent further heat loss. Removal of wet or cold clothing and institution of passive warming techniques like blankets and heating packs should be initiated, but should not impede life-saving treatment. Basic and advanced life support (BLS) should be provided to the patient with active and passive rewarming measures instituted as soon as possible. CPR should be initiated after an extended pulse check of no <60 seconds due to the slowing of cardiac output during prolonged severe hypothermia (Soar et al., 2010). If possible, warmed IV fluids can be administered. If the patient exhibits signs of cardiac instability, core temperatures <28°C, or cardiac arrest, transport to a facility with cardiopulmonary bypass or extracorporeal membrane oxygenation capabilities may be considered (Brown et al., 2012).
In-hospital rewarming treatments include the abovementioned minimally invasive techniques. Forced-air heating blankets can be used as long as their utilization does not impede access to the patient during resuscitation. Invasive rewarming methods should be considered when the patient is in extremis or when the core body temperature is unimproved despite active external rewarming. Warm humidified air at temperatures up to 40°C can be delivered by the ventilator. The heat provided does not contribute greatly to the overall rewarming due to poor lung heat exchange, but it can minimize heat and humidity lost by respiration. Heated irrigation techniques include gastric, bladder, peritoneal, and thoracic lavage, which have varied rewarming rates directly correlated with the surface area exposed to the warm solution. Extracorporeal blood rewarming may be considered in cardiac arrest with caution toward rapid rewarming complications such as hemolysis, pulmonary edema, and acute tubular necrosis (Lasater, 2008).
We used intravascular targeted temperature management systems (IVTTMs) to augment rewarming as a bridge to cardiopulmonary bypass. The heat exchange catheter ZOLL ICY (Model number IC-3893, three heat exchange balloons, three infusion ports) provided immediate central venous access. IVTTMs are approved by the Food and Drug Administration for control of fever in neurocritically ill patients requiring central access and temperature regulation in cardiac and neurosurgery patients since even moderate hypothermia is associated with coagulopathy and impaired wound healing (Al-Senani et al., 2004; Diringer, 2004; Broessner et al., 2009; Davis et al., 2013). When used in patients with subarachnoid hemorrhage and traumatic brain injury, these systems were found to be more precise than external cooling and antipyretics for fever prevention, although the impact of the increased precision is unknown (Diringer, 2004; Hinz et al., 2007). They have also been used for the maintenance of normothermia in burn, organ donation, and other patient populations (Broessner et al., 2009; Davis et al., 2013).
The use of the IVTTMs in the induction and maintenance of therapeutic hypothermia after cardiac arrest is common but off-label. In this application, they were found to cool faster and with less overshoot than external methods such as external gel-coated, water-circulating, and air-circulating cooling devices, although the clinical importance was unclear (Al-Senani et al., 2004; Hoedemaekers et al., 2007).
In our patient, the targeted temperature management system was inserted at a femoral site when the patient's core temperature was 23.3°C (74°F). Fifty minutes later, the patient's core temperature was 26.9°C (80.4°F) just before the operating room transfer. The countercurrent heat exchange catheter requires some degree of circulation, in this case provided by CPR, to warm blood as it flows past the catheter. While the IVTTMs may appear to have less warming than cooling power since the selectable target temperature ranges from 31°C to 38°C, the initial temperature differential in our severely hypothermic patient was a substantial 15°C (38–23°C) (Laniewicz et al., 2008; Lasater, 2008; Taylor et al., 2008).
In the setting of other interventions, our rewarming rate of 3.5°C in 50 minutes is faster than the 1.5°C/h cooling rate noted by Hoedmakers; thus, IVTTMs do not appear to have less warming than cooling ability (Hoedemaekers et al., 2007). Laniewicz reported intravascular IVTTM in a 68-year-old not in arrest with a temperature of 22.7°C (72.9°F), but with some respiratory effort and an organized rhythm. Cardiopulmonary bypass was avoided with a warming rate of 3°C/h (Laniewicz et al., 2008). Taylor et al. (2008) found a mean rewarming rate of 1.5°C±1°C/h in a series of critically ill trauma surgery patients. In addition, IVTTM was used in an 89-year-old with hypotension, bradycardia, and a temperature of 28.8°C (83.8°F) with rewarming of about 1°C/h (Chua and Lundbye, 2012). The physical limitations of surface warming techniques in patients who are operating room bound are noted, as well as theoretical concerns for metabolic derangements and volume redistribution with utilization of previously constricted peripheral vascular beds due to surface warming.
If return of spontaneous circulation (ROSC) is achieved, which did not occur in our patient, the goal of rewarming may shift to a more traditional 33°C. Camp-Rogers report a patient with profound accidental hypothermia and cardiac arrest who had IVTTM inserted after ROSC with a controlled rewarming bridge (1°C/h) to more traditional therapeutic hypothermia (Camp-Rogers et al., 2012). Friberg and Rundgren (2009) similarly report on the use of IVTTM after ROSC in a patient with drowning-related accidental hypothermia who was warmed 1°C/h up to 33°C where he was maintained for 24 hours.
The decision to end resuscitative efforts of severely hypothermic patients has not been studied in detail. The mantra that a patient “is not dead until they are warm and dead” has been universal in teachings without comprehensive data examining resuscitation endpoints. Many sources advocate to warming to 30–32°C (86–89.6°F) before cessation of resuscitation because temperature-mediated electrophysiological derangement is less likely to be the sole source of cardiac dysfunction. One author recommends that due to the elevated levels of potassium in cell death and hypoxia, a potassium level >12 mM is an indication to terminate CPR (Brown et al., 2012).
Management of cyclobenzaprine toxicity
In addition to CPR and aggressive rewarming, we attempted to treat the cyclobenzaprine overdose. We utilized traditionally described treatments for cyclobenzaprine overdose, similar to tricyclic antidepressant overdose, focusing on sodium bicarbonate and ILE.
Cyclobenzaprine is structurally similar to the tricyclic antidepressant amitriptyline, except for the presence of a double bond in the central ring of cyclobenzaprine (Fig. 3). It has been used clinically for nearly half of a century for its skeletal muscle relaxant properties. Cyclobenzaprine also possesses anticholinergic properties and has antihistamine and sedative effects. It is a weak reuptake inhibitor of both norepinephrine and serotonin (Hurlbut, 2004).

Chemical structure of amitriptyline
Although the toxic dose of cyclobenzaprine is not known, patients with acute ingestions ranging from 260 to 900 mg have survived (Spiller et al., 1995). Clinical manifestations following an acute toxic ingestion may be consistent with anticholinergic toxicity (Bebarta et al., 2011). While it has been suggested that QRS complex widening, ventricular dysrhythmias, and seizures may occur due to its structural similarity to tricyclic antidepressants, several previous studies have demonstrated that the actual incidence of these events in the setting of cyclobenzaprine toxicity is relatively rare (Spiller et al., 1995; Bebarta et al., 2011).
Previous case reports have documented the use of sodium bicarbonate therapy in cyclobenzaprine toxicity (Bebarta et al., 2011). This may theoretically benefit patients, especially those with widened QRS complexes due to structural similarity to tricyclic antidepressants.
In addition, the ED pharmacist suggested addition of ILE. Few prospective studies have been performed on the efficacy of ILE; its usage is based largely on theory and anecdotal evidence. ILE has demonstrated its benefits in patients with life-threatening toxicities secondary to ingestion of lipophilic substances, although most data are in animal studies (Cave et al., 2013). Its proposed mechanisms include sequestration of the lipophilic agent from the system and capturing it in the extended lipid compartment created by the presence of ILE (known as the lipid sink theory), and supplementation as a cardiac myocyte energy source to overcome depleted adenosine triphosphate and calcium, which may improve cardiac contractility (French et al., 2011; Weinberg, 2012). Cyclobenzaprine is relatively lipophilic with a partition constant (log p) value of 4.9 (Dorwald, 2012). The toxic effects of lipophilic agents can be reversed with the use of ILE if the partition coefficient of the ingested agent is >2 (Bern et al., 2011; French et al., 2011).
A prospective study demonstrated a significant shortening of recovery time after isoflurane anesthesia with ILE infusions given at the end of surgery (Li et al., 2014). However, in a study of healthy volunteers who were subjected to receive lidocaine injections, followed by either ILE or placebo, there was no difference in symptoms or electroencephalographic waves; nonetheless, a slight decrease in free lidocaine in the blood was noted in the ILE group (Heinonen et al., 2014). A review of several case studies of ILE therapy for toxicological cardiovascular collapse demonstrated no changes in mean arterial pressure with administration of ILE, and several complications, including digit amputation, lung injury, and deep venous thrombosis, were designated as possible or probable complications of the therapy. At this point, it was recommended that ILE be reserved only for cases of drug-induced cardiotoxicity with consequent cardiac arrest or refractory shock (Geib et al., 2012). It is impossible to determine the clinical effects of ILE in this patient, as multiple treatment efforts were occurring simultaneously during resuscitation.
Case Resolution
The patient received ∼90 minutes of cardiopulmonary bypass, and pulses returned ∼30 minutes into rewarming on bypass. The patient remained intubated and was taken to the cardiothoracic surgical intensive care unit. He was following commands at that time, but remained intubated due to marked pulmonary edema. On hospital day 3, the patient was extubated, awake, eating, and conversing with family. The event was determined to be accidental in nature and he was cleared by psychiatry. The patient fully recovered back to baseline mental status and his Cerebral Performance Category score was 1. Upon discharge, due to some residual weakness in his legs, he required physical therapy and a walker.
Conclusion
Our case demonstrates the successful use of an IVTTM as an adjunct to other therapy and bridge to cardiopulmonary bypass in the setting of profound hypothermia and intractable ventricular fibrillation cardiac arrest. Its use did not impede other aggressive resuscitative efforts. Given its ease of use and rewarming rate, particularly in patients who already require central access but may not be in extremis, one may consider limiting other invasive aggressive treatments such as pleural and/or peritoneal lavage.
Footnotes
Author Disclosure Statement
No competing financial interests exist.