
Abstract
The aim of this study was to determine the effect of induced mild hypothermia (34°C) on acid-base balance in septic rats. Twenty-eight male Sprague-Dawley rats median weight 306 g, range 251–333 g were used. After anesthesia and when the target temperature was reached (normothermia: 38°C or induced mild hypothermia: 34°C), sepsis was induced by cecal ligation and perforation. Measurements of cardiopulmonary parameters and blood samples were performed at T0h (occurring immediately after chirurgical procedures), T2h, T4h (at each temperature), and T6h (at 34°C only). Blood oxygen saturation, heart and respiratory rates, arterial blood pH, carbon dioxide partial pressure, sodium, potassium, chloride and calcium concentrations, hematocrit, blood lactate, tumor necrosis factor-α and interleukin-6 concentrations were measured on anesthetized rats. Other parameters such as bicarbonate concentration, hemoglobin concentration, base excess, and anion gap were estimated from measured parameters. Main results showed that an increase in both cytokines concentrations was observed in septic rats compared with sham rats. This increase was less marked at 34°C compared with 38°C. Moreover, sepsis induction led to a marked metabolic acidosis and hypothermia delayed this acidosis. Induced mild hypothermia delays the evolution of cytokines and metabolic acidosis during experimental sepsis.
Introduction
S
Among potential approaches, hypothermia could be an interesting one. Indeed, in previous studies on a septic animal model (L'Her et al., 2006; Léon et al., 2012, 2015), beneficial effects of induced mild hypothermia have been reported: the survival duration of septic rats was increased significantly when they were maintained at 34°C (induced mild hypothermia) throughout the experiment compared with those maintained at 38°C (normothermia). Mean survival durations were 7 hrs 22 mins±0 hrs 12 mins and 5 hrs 11 mins±0 hrs 36 mins at 34°C and 38°C, respectively (Léon et al., 2012). Moreover, the impact of induced mild hypothermia after sepsis is established is the same (Léon et al., 2015). Induced mild hypothermia could have this protective effect by decreasing metabolic rate, inflammatory response, and/or ROS production for example (Saito et al., 2003; Scumpia et al., 2004; Polderman, 2009; Aslami et al., 2010; Léon et al., 2013; Hakim et al., 2014; Karnatovskaia et al., 2014). Animal literature shows also a consistent protective effect of hypothermia, for example, on circulatory and pulmonary dysfunction during experimental endotoxemia (Schwarzl et al., 2013), on toxin-induced lung injury (Lim et al., 2003; Chin et al., 2007; Jo et al., 2011) and pneumonia (Beurskens et al., 2012). In that context, it could also be hypothesized that hypothermia exerts its positive effect on survival duration through an alteration of sepsis-associated deleterious metabolic acidosis. However, to our knowledge, no study has been conducted to address this major point.
Thus, the aim of this experimental study was to examine the effect of induced mild hypothermia on acid base equilibrium in septic rats. For this, pH, CO2 partial pressure (PCO2), bicarbonate concentration, and major plasmatic ions concentrations were measured in the arterial blood. To complete the analysis, base excess, anion gap, and hematocrit were determined on whole blood. Moreover, measurements of heart and respiratory rates, blood O2 saturation, arterial O2 partial pressure (PO2) and plasma concentrations of interleukin-6 (IL-6), tumor necrosis factor-α (TNF-α), and lactate were performed. All parameters were measured at two temperatures: normothermia (38°C) or induced mild hypothermia (34°C) in sham and septic rats, at times 0 hours (T0h), 2 hours (T2h), 4 hours (T4h), and 6 hours (T6h, only at 34°C).
Materials and Methods
Animals
This study was performed in accordance with the European Council revised guidelines on animal care for experimental and other scientific purposes (EU Directive 2010/63/EU). The protocol was approved by the local ethic committee in animal experiments (Authorization number: R-2011-KL-01). All efforts were made to minimize the number of animals used and their suffering.
Experiments were performed on 28 male Sprague-Dawley rats (median weight 306 g; range 251–333 g) obtained from Janvier SAS (Le Genest St Isle). Before the experiment, the rats were kept in an animal house under a 12-hours light-dark-cycle at 21°C and were given ad libitum access to food and water. They were randomly assigned to four experimental groups: two groups were maintained at 38°C (normothermia) and two others at 34°C (induced mild hypothermia) throughout the experiment. For each temperature, sham rats and septic rats were performed depending on surgical procedure.
Anesthesia/Analgesia and temperature control
Rats were initially anesthetized by the intraperitoneal (i.p.) injection of ketamine (10 mg/100 g body mass) and xylazine (1 mg/100g body mass) mixture. One hour later, a half dose of the mixture was injected (i.p.) to maintain a deep level of anesthesia. In addition, an intraperitoneal catheter connected to a perfusion system was inserted to allow continuous saline, anesthetic, and analgesic infusion (0.4 mg xylazine and 12 mg ketamine in 1 mL saline solution) until the end of the experiment. The saline perfusion was started 1 hour after the half dose of anesthetic, at a rate of 0.5 mL/h per 100 g body mass. Experiments were made with animals' breathing room air.
The procedure used to maintain core temperature was previously described in Léon et al. (2012). In summary, during the entire experiment, the animals were placed on a thermoregulated mattress (Huber Polystat CC1, Peter Huber Kältemaschinenbau GmbH, Germany) and core temperature was continuously monitored using a telethermometer, connected to a rectal probe (YSI telethermometer, Yellow Spring Instruments). The core temperature was maintained constant at 38°C or 34°C (±0.5°C) and if slightest variations (due to sepsis and/or anesthesia) were observed, they were immediately counteracted by the temperature modification of the thermoregulated mattress.
Surgical procedures
Surgical procedures were performed after the animals were deeply anesthetized and had reached the temperature goal. First, a heparinized (83 U/mL) catheter was inserted into the right femoral artery of rats and clamped until blood samplings. Second, sepsis induction was performed using the cecal ligation and puncture model (Léon et al., 2012). In sum, a 2-cm midline incision was made in the abdominal wall (laparotomy). The cecum was carefully extruded and ligated on the middle to avoid bowel obstruction. Afterward, the cecum was punctured once from side to side using a pulmonary trocar (8 Gauge) and replaced in the abdominal cavity. For sham rats, only a laparotomy was realized.
Analytical procedures
For each rat, the experimental procedure consisted in (1) measurements of cardiopulmonary parameters (2) blood samples to allow measurements of following described parameters. Measurements were taken at regular time intervals: at T0h (occurring immediately after chirurgical procedures), T2h, T4h (at each temperature), and T6h (at 34°C only) depending on survival duration of rat.
Cardiopulmonary parameters, that is, blood oxygen saturation, heart rate, and respiratory rate, were measured using a noninvasive infrared sensor (Mouse Ox, Bioseb) set up at the throat of each anesthetized rat. Oxygen saturation, heart rate, and respiratory rate were expressed in percent (%), in beats per minute (bpm) and breaths per minute (bpm) respectively.
Arterial blood sample (300 μL) was collected (indwelling catheter) and 70 μL were immediately analyzed using a blood gas analyzer (ABL 77, Radiometer). Several parameters were measured: arterial blood pH, carbon dioxide partial pressure (PCO2), hematocrit, sodium, potassium, chloride and calcium concentrations. Other parameters such as bicarbonate concentration, hemoglobin concentration, base excess, and anion gap were estimated from previous measured parameters. All below analyzed values are values corrected in function of the rats temperatures. The remaining 230 μL of blood sample were centrifuged at 1600 g during 10 minutes at 4°C. The obtained supernatant was frozen at −80°C until assays of plasma cytokines and lactates. Blood TNF-α and IL-6 concentrations were measured by microElisa method using rat immunoassay kits (RTA00 and R6000B R&D Systems). Cytokines were expressed as pg/mL of plasma. The amount of lactates was determined by an enzymatic method using the L-lactic acid kit (N°022 BIOSENTEC) according to the manufacturer's instructions. Lactate concentrations were expressed in g/L of plasma.
Statistical analysis
Results were expressed as median±interquartile range. Differences in median values between groups were assessed using Wilcoxon rank sum tests. Differences where p-value <0.05 were considered significant.
Results
IL-6 and TNF-α plasma concentrations
Changes in IL-6 and TNF-α plasma concentrations in each experimental condition are depicted in Figure 1A and B, respectively.

IL-6 plasma concentrations
In sham rats at 38°C and 34°C compared to T0h, IL-6 plasma concentration increased slightly but significantly (p<0.05), whereas no change in TNF-α plasma concentration was observed throughout the experiment.
In septic rats at 38° and 34°C a significant increase both in IL-6 and TNF-α plasma concentrations was observed compared to T0h (p<0.05). Induced mild hypothermia had no effect on TNF-α increase compared to normothermia. However, compared to T0h, significant IL-6 increase was observed latter when septic rats were at 34°C (T4h) compared to those at 38°C (T2h). Moreover, in septic rats, for the same sample time, IL-6 concentration was significantly lower (p<0.05) at 34°C (T2h: 465±141 pg/mL and T4h: 659±336 pg/mL respectively) compared with results obtained at 38°C (T2h: 584±233 pg/mL and T4h: 2430±1716 pg/mL).
Lactate plasma concentration
Lactate plasma concentration depending on the tested condition is depicted in Figure 2. In sham rats at 38°C and 34°C, despite a transient increase, lactate plasma concentration was similar to the one measured at T0h and at the end of the experiment. In septic rats at 38°C, a significant increase in lactate plasma concentration occurred at T2h and T4h compared to T0h (p<0.05). At 34°C, in septic rats, an increase in lactate concentration was observed from T2h compared to T0h but measured values were similar to those observed in sham rats for the same temperature.

Lactate plasma concentrations (mM) in normothermia (38°C) and hypothermia (34°C) in sham and septic rats at T0h, T2h, T4h, and T6h (34°C). For each sampling time, n=6 for sham and n=8 for septic. Data are expressed as medians±IQR. * indicates a significant difference between T0h and other times in the same condition (p<0.05). ▪ indicates a significant difference between sham and septic rats at each time at a given temperature (p<0.05). ∧ indicates a significant difference between sham rats at 38°C and sham rats at 34°C or between septic rats at 38°C and septic rats at 34°C at each time (p<0.05).
pH, PCO2, and bicarbonate concentration
Changes in pH, PCO2, and bicarbonate concentration depending on the tested condition are shown in 38°C and 34°C Davenport diagrams (Fig. 3A, B respectively; values corrected).

Davenport Diagrams showing pH, PCO2, and bicarbonate (HCO3−) concentrations (values corrected) of sham rats (C) and septic rats (S) in normothermia
Whatever the tested temperature was, no significant change in pH was shown over time in sham rats. At the opposite, a significant decrease in pH was observed throughout the experiment in septic rats both at 38°C and 34°C (Fig. 3A, B respectively, p<0.05). This acidosis occurred earlier in septic rat in normothermia (T2h) compared to those in hypothermia (T4h). The decrease in pH observed in septic rats was associated with a decrease in blood bicarbonate concentration without change in PCO2 values.
Arterial O2 saturation, heart rate, respiratory rate, and hematological parameters
Arterial O2 saturation, heart and respiratory rates were measured in the different experimental groups (Fig. 4A–C respectively). Whatever the tested condition, no marked variation of the three parameters was observed over time. Moreover, no difference was measured between sham and septic rats at a given temperature. Both in sham and septic rats, arterial O2 saturation tented to be higher at 34°C compared to 38°C. At the opposite, heart and respiratory rates tended to be lower when rats (sham and septic) were exposed to hypothermia compared with those in normothermia.

Arterial O2 saturation
Hematological parameters are presented within Table 1. Whatever the experimental condition, no significant change in hematocrit and hemoglobin concentration occurred.
Data are expressed as medians±IQR (n=6 for sham rats and n=8 for septic rats).
Whole blood Na+, K+, Ca2+, and Cl− concentrations
Whole blood Na+, K+, Ca2+, and Cl− concentrations were determined in each tested condition (Table 2).
Data are expressed as medians±IQR. For each sampling time, n=6 for sham rats and n=8 for septic rats.
Indicates a significant difference between T0h and other times in the same condition (p<0.05).
Indicates a significant difference between sham and septic rats for each time and temperature (p<0.05).
At a given temperature and a given sample time, no difference in Na+ concentration was highlighted between sham and septic rats. An increase in blood Na+ concentration was observed compared to T0h throughout the experiment in both groups of rats. This increase occurred later at 34°C compared to 38°C.
No change in K+ concentration was observed over time in sham rats at both temperatures. In septic rats, an increase in K+ concentration was demonstrated at T4h at 38°C and from T2h at 34°C compared to T0h.
In sham rats, at 38°C but not at 34°C, a transient increase in Ca2+ concentration occurred. In septic rats, whatever the tested temperature, no significant change in Ca2+ concentration was observed.
At a given temperature and a given sample time, no difference in Cl− concentration was noted between sham and septic rats. A significant increase in Cl− concentration was observed compared to T0h throughout the experiment for the three other groups (p<0.05), except for septic rats at 34°C.
Anion gap
Anion gap in whole blood was also measured in each tested condition (Fig. 5). Compared with T0h, a significant increase in anion gap occurred in all experimental groups (p<0.05). At 38°C, no difference was observed between sham and septic rats. At the opposite, at 34°C, the increase was significantly higher in septic rats compared with sham rats from T2h.
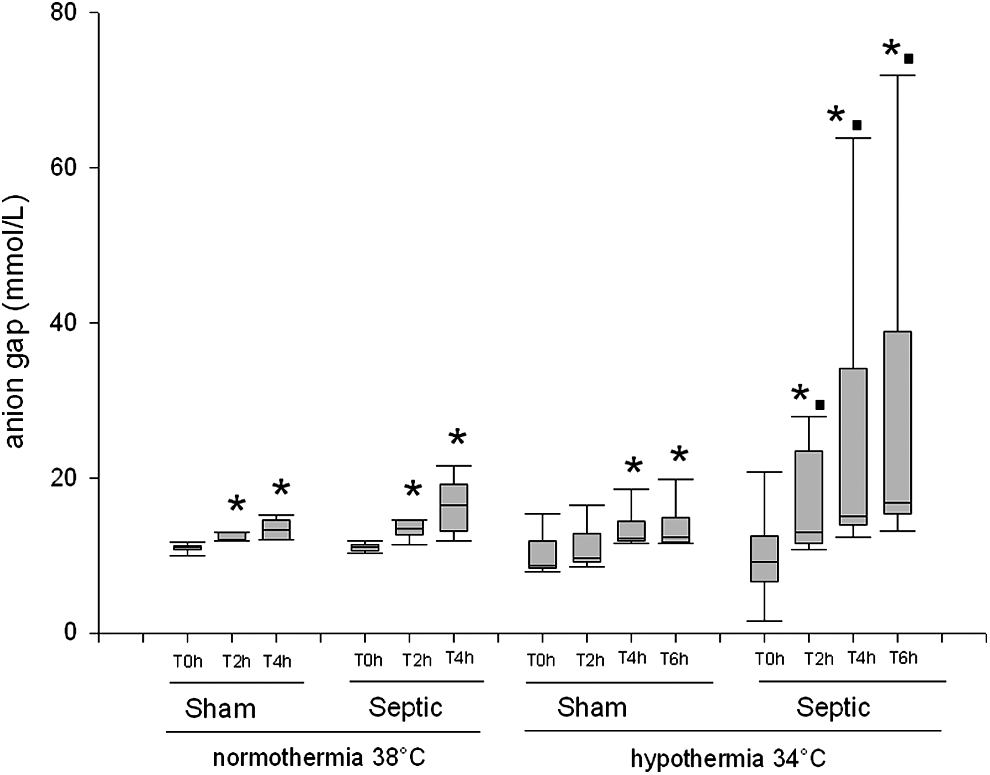
Anion gap (mM) in normothermia (38°C) and hypothermia (34°C) in sham and septic rats at T0h, T2h, T4h, and T6h (34°C). For each sampling time, n=6 for sham and n=8 for septic. Data are expressed as medians±IQR. * indicates a significant difference between T0h and other times in the same condition (p<0.05). ▪ indicates a significant difference between sham and septic rats at each time and temperature (p<0.05).
Base excess
Changes in base excess in whole blood were measured in each experimental condition and presented in Figure 6. In all experimental conditions, a significant decrease in base excess was observed throughout the experiment compared with T0h (p<0.05). The decrease in base excess was more pronounced in septic rats compared with sham rats, especially at 34°C.
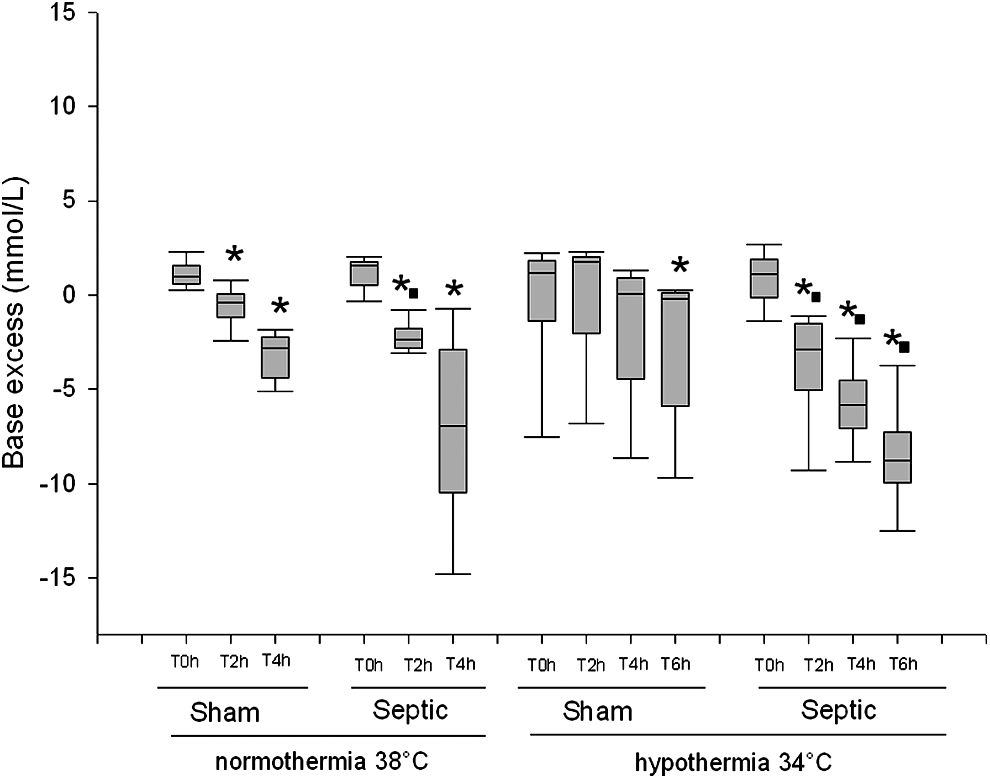
Base Excess (mM) in normothermia (38°C) and hypothermia (34°C) in sham and septic rats at T0h, T2h, T4h, and T6h (34°C). For each sampling time, n=6 for sham and n=8 for septic. Data are expressed as medians±IQR. * indicates a significant difference between T0h and other times in the same condition (p<0.05). ▪ indicates a significant difference between sham and septic rats at each time and temperature (p<0.05).
Discussion
This study questioned about the effect of induced mild hypothermia on acid-base balance in septic rats. To ensure that sepsis was really induced in our experimental conditions and that the inflammatory process took place, two circulating mediators of inflammation the cytokines TNF-α and IL-6 were measured.
Indeed, TNF-α is one of the coordinators of the inflammatory response observed during sepsis (Blackwell and Christman, 1996), whereas IL-6 participates to its activation (Damas et al., 1997; Leon et al., 1998; Riedemann et al., 2003). In this study, a significant increase in IL-6 and TNF-α plasma concentration was observed in septic rats at 38°C from 2 hours of induction. Measured values were in agreement with those found in the literature (Gogos et al., 2000; Demirbilek et al., 2004) and proved the establishment of sepsis in our model. When mild hypothermia was applied, a decrease in IL-6 plasma concentrations was observed in septic rats. These results tended to show that induced mild hypothermia could delay the inflammatory process observed in case of sepsis and could thus have an anti-inflammatory effect.
In this experiment changes in acid-base equilibrium were observed. In sham rats, a compensated alkalosis that allows maintaining the extracellular pH was observed at both temperature (38°C and 34°C).
At the opposite, in septic rats at 38°C and 34°C, the extracellular pH decreased and was not regulated over time. In our study, the induction of sepsis led to a marked acidosis. This acidosis evolution observed in septic rats appeared temperature dependent: indeed, decrease temperature from 38°C to 34°C appeared to delay the extracellular pH decrease. Thus, by slowing down the evolution of acidosis, hypothermia may help to protect the body from its harmful effects.
According to our results and confirmed by the literature (Mecher et al., 1991; Hart et al., 2003; O'Dell et al., 2007; Noritomi et al., 2009; Mallat et al., 2012), the origin of the observed acidosis stems from a metabolic deregulation without respiratory compensation. Several results obtained in this study tend to confirm this hypothesis.
First, a significant decrease in base excess, synonymous of metabolic acidosis, was observed in septic rats. This decrease in base excess was significantly higher in rats at 34°C compared with those maintained at 38°C.
Second, the absence of significant changes in blood PCO2 and respiratory rate in septic rats compared to sham rats whatever the temperature tested confirmed the lack of respiratory compensation at the two temperatures tested.
Third, the decrease in extracellular pH in septic rats was associated with a significant increase in anion gap. According to the theory of Stewart, this anion gap corresponds to the lactate, the weak acids (plasma proteins) and the unmeasured anions whose origin remains to be determined. In normothermia septic rats, an important and significant increase in lactate plasma concentration was observed. This result could be linked to the use of anaerobic metabolism indicating the existence of hypoperfusion and tissue hypoxia (Kaplan and Frangos, 2005). This increase in blood lactate concentration was less marked in rats maintained at 34°C compared to those maintained at 38°C. By lowering the O2 tissue consumption and decreasing the hypoperfusion effects induced by sepsis, hypothermia could reduce the use of anaerobic metabolism. It is important to point out that a large individual variation in blood lactate was measured in normothermic septic rats. The same result is frequently reported in septic patients (Mallat et al., 2012). The increase in anion gap could also be linked to an increase in production of weak acids or unmeasured anions by peripheral tissues (Kaplan et al., 2004). This increase in anion gap was higher in septic rats maintained at 34°C than those maintained at 38°C, whereas lactatemia was lower. This increase could be the result of a hepatic (Kellum et al., 1995) or renal dysfunction (Moviat et al., 2003). Further investigations are necessary to test this hypothesis.
In this experiment, a hyperchloremia was also observed in septic rats. This increase in plasma chloride concentration could not be linked to the observed metabolic acidosis in septic rats. Indeed, this increase was also observed in sham rats without significant changes in acid-base balance compared to septic rats. This hyperchloremia was probably linked to our experimental protocol and due to the perfusion with saline throughout the experiment.
It was also important to note that, in case of sepsis, acidosis evolution is indicative of a poor prognosis (Smith et al., 2001; Park et al., 2006). A severe acidosis is well recognized to suppress myocardial contractility, predispose to cardiac arrhythmias, and decrease vascular resistance and blood pressure, and therefore contribute to increase in morbidity and mortality. Therefore, as induced mild hypothermia appeared to delay metabolic acidosis, these adverse effects could be reduced.
Our study presents several limitations that should be discussed. First, anesthetic agents used may contribute to biochemical changes (anti-inflammatory effect for example). However, sham group were performed at each temperature. This allows us to discriminate the effect of hypothermia on sepsis evolution independent of the experimental procedure. Second, our experimental animal model could be considered not clinically relevant. Indeed, it is a severe-acute sepsis model and survival duration was less than 24 hours. But, it allows us to better understand the major mechanisms induced by sepsis. Moreover, hypothermia was induced before sepsis and our animals were not under respiratory assistance. However, this experimental model allowed us to test the effect of hypothermia on physiological functions such as acid-base equilibrium and could bring a better understanding of mechanism induced by sepsis. Moreover, in a previous study (Léon et al., 2015), we have shown that whatever was the induction time of hypothermia a decrease in body temperature was beneficial in terms of survival. Moreover, clinical study tend to show that the control of body temperature improve survival in case of sepsis (Schortgen et al., 2012).
Conclusion
In this study, induced mild hypothermia appeared to delay the evolution of metabolic acidosis during sepsis may be by reducing the overall sepsis severity. These results suggest that induced mild hypothermia could be an appropriate therapeutic option for some septic patients. It does not prevent death but the control of body temperature, by providing the time needed to administer the proper treatment, could be decisive for a favorable prognosis for septic patients.
Footnotes
Acknowledgment
This research was supported by a grant from the Brittany Regional Council.
Author Disclosure Statement
No competing financial interests exist.