
Abstract
The safety, feasibility, and hemodynamic effects of mild hypothermia (MH) induced by transnasal cooling were studied in transcatheter aortic valve replacement (TAVR). MH is a common therapy following cardiac arrest and seems to have favorable effects in myocardial infarction and on hemodynamic stability. In TAVR, hemodynamic instability is common during rapid pacing. Twenty subjects undergoing TAVR were randomized 1:1 to hypothermia or normothermia. Hemodynamic endpoints were mean arterial blood pressure and required dosage of vasoactive and inotropic drugs. Patients were followed up at 6 months. All patients in the MH group (n=10) reached the target temperature of 34°C before first rapid pacing. Tympanic and urinary bladder temperature remained significantly lower in the MH group during the procedure. No adverse effects of cooling were observed. Mean arterial pressure was higher in the MH group (90±20 mm Hg) than in the control group (71±13 mm Hg) at the start of the procedure, at first rapid pacing (94±19 vs. 80±16 mm Hg), and at balloon aortic valvuloplasty (90±17 vs. 73±14 mm Hg). Less norepinephrine was administered to the hypothermia group. Transnasal cooling during TAVR was safe and well tolerated. We observed a more stable hemodynamic profile in the MH group, indicated by higher blood pressure and lower levels of vasoactive drugs required. A larger study of patients with severe ventricular dysfunction is required to more comprehensively investigate the hemodynamic effects of transnasal cooling in TAVR.
Introduction
M
A hydrocarbon-based liquid coolant mixture is sprayed into the nasal cavity along with oxygen administration, which evaporates the mixture within the nasal cavities causing rapid cooling that, in turn, cools the brain (Busch et al., 2010). Transnasal evaporative cooling has demonstrated safety, feasibility, and a significant reduction in time from induction of hypothermia to target temperature compared to other noninvasive methods (Castren et al., 2010). This cooling method also allows for maintenance of hypothermia after the target temperature is reached.
Transcatheter aortic valve replacement (TAVR) is a catheter-based therapy for treatment of severe aortic stenosis that has shown significant reduction in mortality compared to drug therapy and produces results comparable to surgical aortic valve replacement (SAVR) (Leon et al., 2010; Smith et al., 2011). TAVR is associated with a significantly higher survival rate compared to SAVR in a select high-risk population (Adams et al., 2014). Patients currently selected for TAVR are primarily elderly with extensive comorbidities. During TAVR, hemodynamic instability is common after rapid ventricular pacing (RVP), balloon aortic valvuloplasty (BAV), or following valve implantation (Guinot et al., 2010; Ruggeri et al., 2012). MH may be beneficial in TAVR to increase hemodynamic stability, but has not been evaluated.
The primary aim of the present study was to determine the safety and feasibility of transnasal evaporative cooling during TAVR and to investigate the hemodynamic response in TAVR-patients during MH.
The secondary aim was to investigate neurological effects of transnasal-induced hypothermia during TAVR, as indicated by neurological biomarkers.
Materials and Methods
Design
The TAVR-CHILL was a prospective randomized open-label trial with a descriptive hypothesis-generating design. The study was conducted as a single-center trial at Skane University Hospital, Lund, Sweden, from January 2013 to January 2014. Patients scheduled for TAVR were admitted 1 day before the procedure and considered eligible for inclusion if the following criteria were fulfilled: age ≥18 years, severe aortic stenosis (indications for TAVR according to multidisciplinary conference), life expectancy >1 year, and signed informed consent before randomization. Key exclusion criteria were previous cerebral vascular insult, malignant hyperthermia, previous surgery in the epipharynx area, and confusion and/or inability to comprehend the study information. Twenty-two patients scheduled for TAVR were included. A patient who received standard aortic valve replacement with open-heart surgery and one suffering a femoral artery complication at initiation of TAVR did not undergo cooling and were excluded from the analysis (Fig. 1). The remaining 20 patients were randomized 1:1 between the hypothermia (n=10) and control (n=10). All patients were followed up for a 6-month period.

Patient flowchart.
Ethical considerations
The Ethics Review Board of Lund University, Sweden, formally approved the study (Dnr 2012/630). Oral and written informed consent was obtained from all subjects before enrollment and randomization.
Procedures
All procedures were carried out under general anesthesia, including endotracheal intubation, according to standard procedures. TAVR was performed with the Edwards SAPIEN XT™ valve prosthesis (Edwards Lifesciences Corp., Irvine, CA) Vasoactive and inotropic drugs (norepinephrine and dobutamine) were used to maintain hemodynamic stability, a target MAP of >80 mm Hg. MH was initiated following endotracheal intubation, defined as the baseline point in the protocol. Oxygen flow to the evaporative cooling device (RhinoChill™; BeneChill, Inc., San Diego, CA) was initiated at medium setting for 1 minute and, if no hemodynamic event occurred, increased to a high flow. This was maintained until the target temperature was reached and then turned off. Target tympanic temperature was 34°C. Tympanic and urinary bladder temperatures were measured simultaneously throughout the procedure (Thermoscan 4000 Pro™; Braun, Kronberg, Germany). Room temperature was controlled at 20°C. At completion of the procedure, defined as puncture site closure, the rewarming process was initiated at a maximum rate of 0.5°C/h by external heating (3M Bair Hugger™; Arizant, Inc., Eden Prairie, MN). During rewarming, general anesthesia was continued with a propofol and remifentanil infusion until a bladder temperature of 36°C was reached. The patient was subsequently extubated in the intensive care unit (Fig. 2).

Hypothermia was induced by a transnasal evaporative cooling device straight following endotracheal intubation, defined as baseline in the protocol. Target tympanic temperature was 34°C and hypothermia was maintained throughout the procedure until valve implantation was performed. The dotted line indicates target temperature. Mean time from induction of hypothermia to target temperature was 27±9 minutes. BAV, balloon aortic valvuloplasty.
Data collection
Central venous, systolic, diastolic, and MAP were measured at 5-minute intervals from baseline to the conclusion of the procedure and were recorded at baseline, procedure initiation (defined as transfemoral or transapical puncture), first initiation of RVP, BAV, valve implantation, and at puncture site closure. In addition, HR and end-tidal carbon dioxide (etCO2) were monitored (Philips Intellivue® Cardiac System, version M8010A; Royal Philips Electronics, Amsterdam, Netherlands). Cerebral oxygen saturation (SctO2) (INVOS™5100C; Covidien, Dublin, Ireland) and the dosage of vasoactive and inotropic drugs were recorded. Measures of venous oxygen saturation (ScvO2), pH, pCO2, pO2, hemoglobin, bicarbonate (HCO3−), and lactate were conducted at baseline, during hypothermia, and 24 hours postprocedure. The N-terminal pro-brain natriuretic peptide (NT-proBNP), estimated glomerular filtration rate measured by cystatin-C, and C-reactive protein (CRP) were assessed at baseline and 72 hours postprocedure. The neurological biomarkers, neuron-specific enolase (NSE) and S-100B, were analyzed at baseline and 24 hours postprocedure. All laboratory analyses were collected from arterial and central venous lines.
Sample size and statistical analysis
The sample size was estimated based on previous experience of explorative studies of hypothermia at the Skane University Hospital, Sweden. The a priori number of subjects intended to be included in the trial was 10 patients treated in each group. Statistical analysis was performed using the IBM® SPSS® Statistics software version 22 (IBM Corp., Armonk, NY).
Continuous variables were monitored and reported as mean±standard deviation or as median (interquartile range) if asymmetrically distributed. For the hemodynamic variables and the biochemical marker ScvO2, an area under curve (AUC) analysis was performed. The significance of between-group differences was assessed by the Mann–Whitney U-test (Wilcoxon rank-sum test). A p-value of<0.05 was considered significant.
Results
Patient characteristics, procedural data, and efficacy
There were no significant differences in baseline characteristics or in procedure duration (81±20 vs. 79±12 minutes, p=0.90), radiation dose (117.3±48.8 vs. 114.3±42.2 Gy×cm2, p=0.91), or amount of contrast media used (86±27 vs. 90±27 mL, p=0.64). In one control patient, the valve was incorrectly implanted and another was inserted. Overall, success of the procedure was similar in groups (Table 1).
There were no significant differences between the groups. Values are presented as number (n) and mean±SD.
See Dewey et al. (2008).
BAV, balloon aortic valvuloplasty; COPD, chronic obstructive pulmonary disease; MI, myocardial infarction; PCI, percutaneous coronary intervention.
Temperature management
The baseline tympanic and urinary bladder temperature did not differ between groups. All patients in the hypothermia group (n=10) reached target tympanic temperature (34°C) before the first RVP event (Fig. 2). Mean time from initiation of MH to target temperature was 27±9 minutes. Target tympanic and urinary bladder temperature was reached at valve implantation and was significantly lower in the MH group throughout the procedure (Fig. 2). Total time of anesthesia, defined as time from intubation to extubation, was 412±113 minutes in the hypothermia group and 166±162 minutes in the control group (p=0.014).
In-hospital complications
There were no serious complications related to the transnasal evaporative cooling. One case of postoperative epistaxis was reported. No discoloration of or sensitivity reactions in the epipharynx area were observed. Subcutaneous emphysema occurred in one patient, considered by an independent adjudicator to be related to the transapical procedure. One patient received a permanent pacemaker postoperatively (hypothermia group) and one vascular complication requiring additional surgery occurred (control group).
Major adverse cardiac and cerebral events during 6-month follow-up
No deaths occurred during the 6-month follow-up period. One transitory ischemic attack and one hemorrhagic stroke were reported in the MH group, and one thromboembolic stroke occurred in the control group. All cerebral events occurred more than 4 months after TAVR. No myocardial infarction, device failure, or major bleeding was reported (Table 2).
There were no significant differences between the groups. Values are presented as numbers (n) of total.
MACCE, major adverse cardiac and cerebral events.
Hemodynamic data
Baseline hemodynamic measurements were similar in both groups. Systolic blood pressure was higher in the MH group compared to the normothermia group at the start of the procedure (137±32 vs. 106±12 mm Hg). MAP was also higher at this time point (89±20 vs. 71±13 mm Hg). At the first initiation of RVP, there was no difference between groups in any hemodynamic parameter (Fig. 3a).
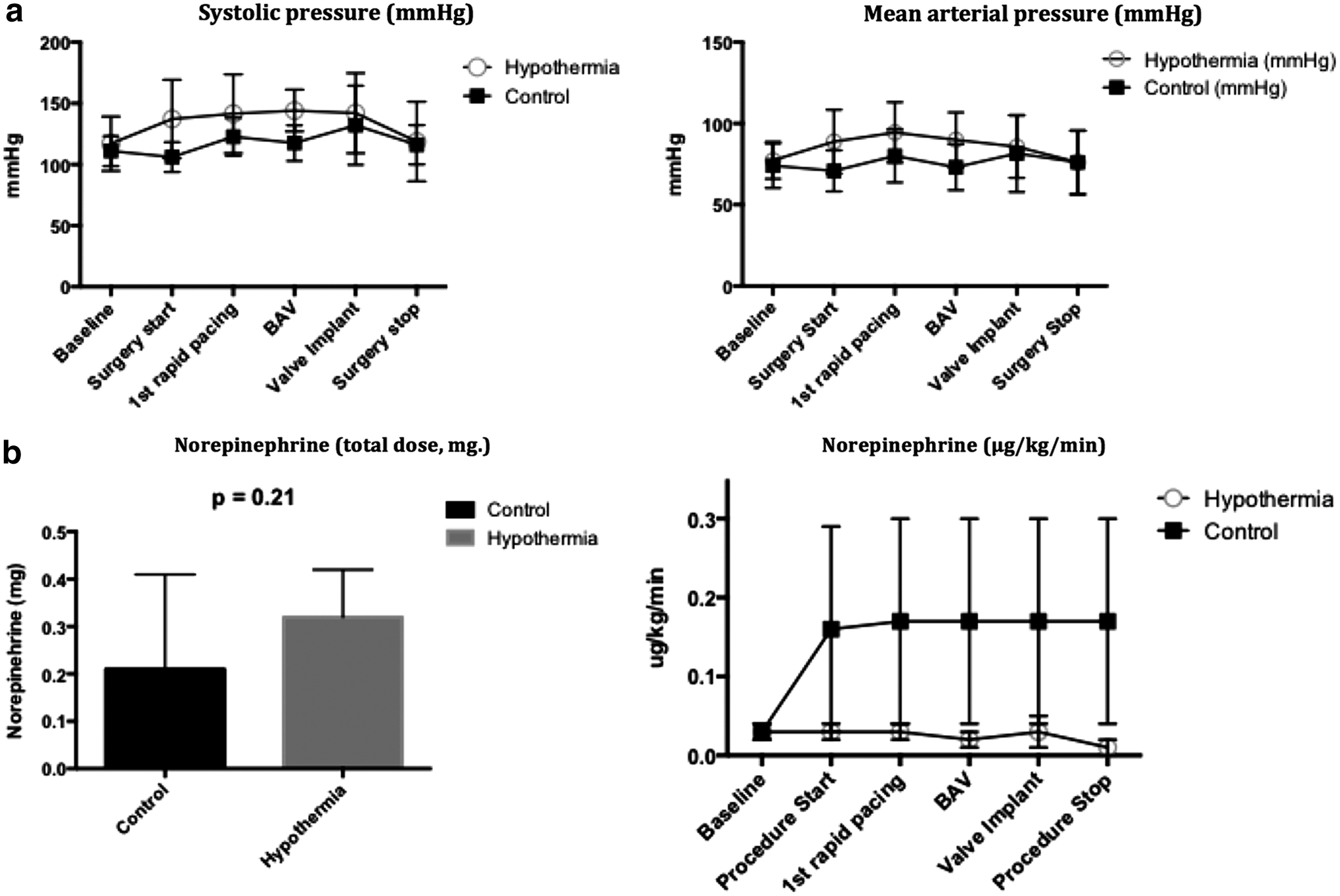
At BAV, systolic pressure was higher in the MH group (144±17 vs. 118±15 mm Hg), as was MAP (90±17 vs. 73±14 mm Hg). There were no differences in the assessed hemodynamic parameters at valve implantation or at the end of the procedure (Fig. 3). The AUC for systolic blood pressure and MAP did not differ significantly (MH 12,355±188.1 vs. control 11,689±286.6 [arbitrary units], p=0.09), and (MH 7962±155.9 vs. control 7631±387.5 [arbitrary units], p=0.31). Central venous pressure, HR, and etCO2 variables did not show differences at any point. Levels of SctO2 did not differ significantly between the groups.
Vasoactive and inotropic drugs
Norepinephrine was used in 19 of 20 patients and dobutamine in 11 of 20 patients (4/10 in MH and 7/10 in control). At the start of the procedure, the dose of norepinephrine was lower in the hypothermia group (0.03±0.01 μg/kg/min [0.01–0.04] vs. 0.16±0.30 μg/kg/min [0.01–0.05]). Lower norepinephrine usage during hypothermia was also recorded at first rapid pacing (0.03±0.02 μg/kg/min [0.01–0.04] vs. 0.17±0.40 μg/kg/min [0.03–0.06]), at BAV (0.02±0.02 μg/kg/min [0.02–0.04] vs. 0.17±0.40 μg/kg/min [0.02–0.05]), and at valve implantation (0.03±0.05 μg/kg/min [0.02–0.04] vs. 0.17±0.40 μg/kg/min [0.02–0.06]) (interquartile range 25–75%) (Fig. 3b). The AUC for the norepinephrine dose was significantly lower in the hypothermia group (0.06±0.05 vs. 0.8±1.8 arbitrary units, p=0.008). Lower doses of dobutamine were also used in the MH group, with an AUC of 3.2±4.9 versus 10.7±14.9, p=0.25. The total amount of norepinephrine used was 0.32±0.1 mg in the MH group versus 0.21±0.20 mg in the control, p=0.21.
The amount of dobutamine used was 6.1±14.3 mg in the MH group versus 12.3±14.9 mg in the control, p=0.17 (Fig. 3b).
Biochemical markers
No between-group differences were found, although a significant increase of CRP from baseline was seen at 72 hours in the entire patient cohort (3.8 [1.4–10.9] vs. 62.5 [34.8–97], p=<0.001). There was a significant increase of NSE in the study population at 24 hours compared to baseline (16.0 [15.0–23.3] vs. 20.0 [19.8–28.5], p=0.02) (Fig. 4), but no significant between-group differences were found. There was no significant change in S-100B in the study population during the procedure or difference between groups (0.06 [0.05–0.06] vs. 0.07 [0.04–0.10], p=0.33).
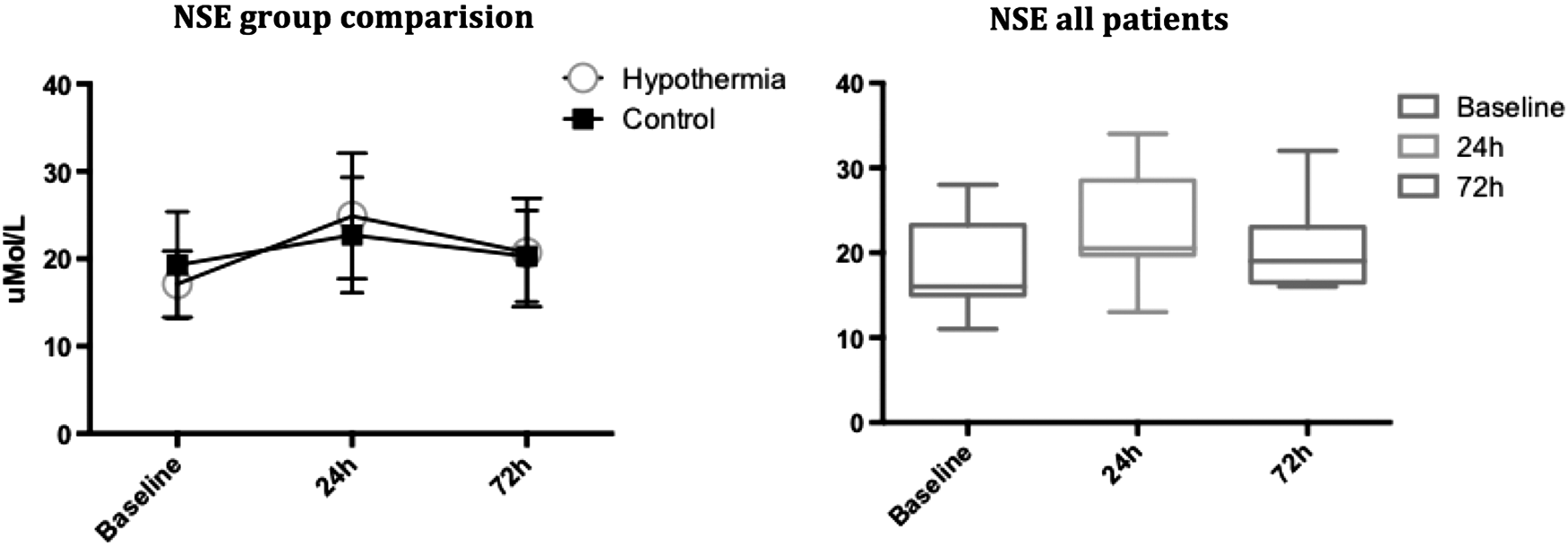
There were no differences between the groups, but there was a significant increase of neuron-specific enolase (NSE) for the entire study population from baseline to the 24-hour analysis (n=20), p=0.03.
Discussion
In this small clinical trial, we evaluated whether transnasal evaporative cooling during TAVR would be safe and feasible and associated with a more stable hemodynamic profile compared to standard TAVR. No adverse effects of transnasal cooling were observed and some possibly favorable hemodynamic effects were noted. Target temperature was achieved in all patients within 27±9 minutes.
Safety
TAVR is most often performed on patients drawn from an elderly population with considerable comorbidities (Leon et al., 2010), and a major concern is that MH might be associated with adverse side effects. Infusion of cold saline is also a noninvasive cooling method (Kim et al., 2007; Erlinge et al., 2014), but in the TAVR population, impaired left ventricular ejection fraction (LVEF) and pulmonary hypertension (PAH) are common (Kamperidis et al., 2014), and rapid infusion of 1000–2000 mL cold saline could lead to increased risk of pulmonary edema and acute heart failure. Although no major adverse side effects were observed, a case of minor epistaxis occurred. Epistaxis was also reported at an incidence of 1.5% in the PRINCE trial investigating transnasal hypothermia (Castren et al., 2010). No cases of discoloration or sensitivity reactions of the epipharynx were reported. Our trial population was carefully selected and treated in a controlled environment, unlike circumstances encountered in an out-of-hospital cardiac arrest, which might explain the low complication rate. One patient suffered a left-sided pneumothorax and subcutaneous emphysema in the neck and epipharyngeal area 1-day postprocedure. This event was independently deemed to be associated with the transapical approach of the procedure. In the PRINCE trial, a case of periorbital emphysema was reported.
Three cases of neurological events were reported during the 6-month follow-up. All appeared more than 4 months after the procedure and were most likely unrelated to MH or the TAVR procedure. The total anesthesia time was significantly prolonged in the hypothermia group. Potential adverse side effects can result from delayed extubation compared to immediate extubation following valve implant and the use of conscious sedation during TAVR (Petronio et al., 2015). If positive effects of hypothermia in TAVR were to be confirmed in a larger trial, the duration of anesthesia would be an important factor to consider when defining a potential target group for the treatment.
Hemodynamic characteristics
This was a small exploratory trial and not powered to detect minor differences in hemodynamic variables. However, despite the relatively small sample size, we did find hemodynamic consistencies. Although not significant, the hypothermia group exhibited higher systolic blood pressure, MAP, and ScvO2. In addition, the dosage of norepinephrine required to maintain an MAP >80 mm Hg was lower with hypothermia, implying greater hemodynamic stability. Positive hemodynamic effects of MH have been reported in previous research (Moriyama et al., 1996; Dumas et al., 2011). We did not find major differences in these factors, possibly due to the low frequency of severe LVEF impairment or PAH in our cohort. Positive effects of MH during hemodynamic instability may be more pronounced in a patient population with greater impairment of ventricular function. We found increased cerebral oxygenation (SctO2) in the MH group, implying improved cerebral circulation. This was not statistically significant, but the finding was consistent throughout the procedure. The difference could be attributed to improved cardiac function as well as being an effect of hemodynamics in general. It is possible that improved cerebral circulation during TAVR will reduce long-term adverse neurological effects.
Biochemical markers
The analysis of arterial blood gas, hemoglobin, HCO3, lactate, NT-proBNP, and CRP did not reveal remarkable findings. At 72 hours postprocedure, CRP was significantly elevated from baseline, in accordance with previous reports that TAVR as well as SAVR can evoke a postprocedure inflammatory response (Sinning et al., 2012; Stahli et al., 2012). An association between TAVR and increased levels of the neurological biomarker NSE has been shown in previous publications (Ghanem et al., 2010, 2013). NSE is a widely used biomarker of cerebral ischemia, but MH is reported to alter the correlation of NSE levels with neurological outcomes (Storm et al., 2013). The observed levels of NSE were low compared to those reported in patients resuscitated following cardiac arrest; however, we found a significant rise in NSE from baseline at 24 hours for the entire patient cohort, most likely associated with RVP.
The consequence of RVP is impaired microvascular tissue perfusion, and following RVP, compensatory mechanisms mediate a reperfusion phenomenon (Selle et al., 2014). Based on out-of-hospital cardiac arrest trials, reperfusion is considered a secondary insult and could be one of the most important complications managed by MH and TTM.
Limitations of the study
The present study has a number of limitations. Due to the nature of the safety and feasibility trial, the number of subjects was low. The effects of MH are closely correlated with core temperature, which we did not measure in this trial. Tympanic temperature, in combination with urinary bladder temperature, is considered reliable, but some deviation from true core value is probable. Several publications have demonstrated tympanic measurements to be sufficient (Joost and Guldager, 2003; Nielsen et al., 2014). In this trial, all subjects reached the target temperature of 34°C for both tympanic and urinary bladder before valve implantation, and thus, the cooling procedure was effective.
We did not measure cardiac output, cardiac index, or pulmonary artery pressure. The absolute values and variations in arterial pressure, ScvO2, and SctO2 were taken into consideration when evaluating the hemodynamic state. These measurements do not replace extended invasive analysis, but are validated methods of estimating oxygen consumption and, by extension, hemodynamic stability (Yahagi et al., 1998).
Finally, this was a small trial and some beneficial or detrimental effects of the hypothermia treatment may have been missed due to the type II error. We found consistencies in the hemodynamic response to hypothermia that need to be confirmed in larger trials.
Conclusions
Transnasal evaporative cooling during TAVR was found to be feasible and well tolerated without adverse side effects. The RhinoChill device demonstrated efficacy in cooling the subjects as well as in maintaining MH throughout the procedure. We observed signs of a more stable hemodynamic profile in the hypothermia cohort as well as lower oxygen consumption and use of lower doses of norepinephrine. A significant increase of NSE, implying an impact on cerebral circulation, was reported for the total study population, with no difference between the groups. Transnasal evaporative cooling provided a noninvasive method of inducing and maintaining MH in TAVR, which could be associated with more favorable hemodynamics.
Footnotes
Acknowledgments
The authors would like to acknowledge David Erlinge, MD, PhD, Professor of Cardiology and Head of the Department of Cardiology, Lund University, for his invaluable support and scientific counseling. The study was supported by BeneChill, Inc. (San Diego, CA), in providing the cooling device and education of the staff. No funding or grants were provided.
Author Disclosure Statement
No competing financial interests exist.