
Abstract
Therapeutic hypothermia is used in select patients after out-of-hospital cardiac arrest (OHCA) to improve neurologic outcome. Rebound hyperthermia (RH) is commonly observed post-treatment. Previous studies analyzing the association of RH with clinical outcome have reported conflicting results. The purpose of this study is to examine the impact of RH after completion of therapeutic hypothermia in patients postcardiac arrest. We analyzed a retrospective cohort from our institution. All adults who underwent therapeutic hypothermia post-OHCA were divided into two cohorts depending on the presence/absence of fever (T > 38°C) within 24 hours of completing hypothermia protocol. Clinical outcomes were analyzed at hospital discharge or death. Among 306 patients admitted with OHCA, 117 underwent hypothermia, 97 survived 24 hours postrewarming. Twenty-seven patients (50%) with RH died compared with 20 (47%) without RH (OR, 1.15; 95% CI, 0.52–2.57). Twenty-six patients (67%) with RH had a poor neurologic outcome compared with 27 (63%) without RH (OR 1.19, 95% CI, 0.51–2.74). RH is common after completion of therapeutic hypothermia in comatose patients due to cardiac arrest and is associated with poor neurologic outcomes. We found no significant clinical impact of rebound hypothermia on neurologic outcome or mortality, but our study was underpowered to reveal such impact if it exists.
Introduction
C
Rebound hyperthermia (RH; T > 38°C), commonly observed in patients after completing therapeutic hypothermia, has been described in 41–64% of patients (Bro-Jeppesen et al., 2013; Gebhardt et al., 2013; Leary et al., 2013; Winters et al., 2013; Cocchi et al., 2014). Although fever immediately after ROSC is known to be associated with worse neurologic outcome, the clinical significance of fever after therapeutic hypothermia is not well established (Frangogiannis et al., 2002). Studies examining RH have reported conflicting results regarding its clinical impact. We postulated that fever within the first 24 hours of rewarming would correlate with worse neurologic outcome. We conducted a retrospective cohort study of postcardiac arrest patients to evaluate the prognostic implication of RH.
Methods
This study has been approved by the local Institutional Review Board. IRB Approval Number: 152–12.
A retrospective review of 306 patients admitted to our hospital after an OHCA from August 2005 until July 2013 was performed. Inclusion criteria were adults (age ≥18) who presented after cardiac arrest, received resuscitation in the field or the emergency room, and completed therapeutic hypothermia protocol after admission to the intensive care unit. Patients with cardiac arrests on the inpatient service and those who died within 24 hours after reaching target rewarming temperature were excluded.
The institutional therapeutic hypothermia protocol includes using cooling blankets to achieve a target temperature of 32°C–34°C (monitored rectally) within 3–6 hours of resuscitation. Target temperature is maintained for 24 hours and then the patient is rewarmed passively at a rate of 0.25°C per hour until they are euthermic. Temperature is measured every hour upon admission to the intensive care unit. Patients underwent an urgent coronary angiogram at the discretion of the treating physician.
The end points for the retrospective study were in-hospital mortality and neurologic outcome. Neurologic outcome was assessed using cerebral performance category (CPC) scale. Good neurologic recovery was defined as CPC 1 and 2. RH was defined as a temperature greater than 38°C within 24 hours after achieving target rewarming temperature of 37°C. The primary end points were compared between the cohorts with and without RH. Categorical variables were expressed as percentage, and the outcome was compared using Chi-square test. p < 0.05 was defined as statistically different.
Results
Among 306 patients who presented with OHCA and were admitted to our intensive care unit, 117 patients underwent therapeutic hypothermia. Of those, 97 patients survived longer than 24 hours after rewarming and were included in our final analysis (Fig. 1). RH (T ≥ 38.0°C) was observed in 54 (56%) patients within 24 hours of rewarming. Twenty-eight of these patients had a severe RH as defined by T > 38.5°C.
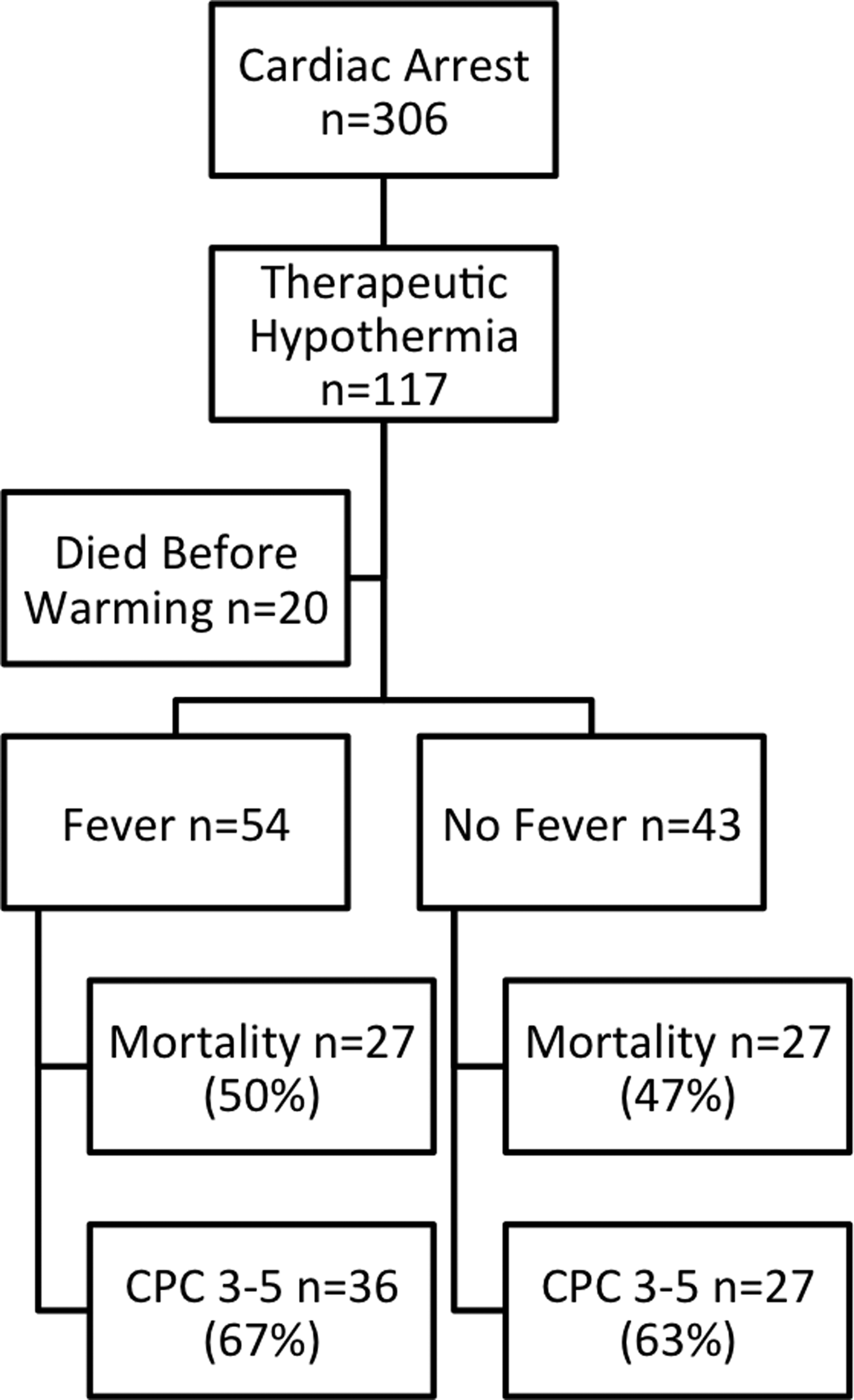
Patient selection. CPC, cerebral performance category.
Clinical characteristics were similar in patients with and without RH except for increased white blood cell counts in the RH group (p = 0.05) (Table 1). The incidence of pneumonia was similar in the two groups, but broad spectrum antibiotics were given more often in the RH group than in the non-RH group (87% vs. 73%, Fig. 2). Twenty-two percent of patients in the RH group had a positive blood culture. Blood cultures from the non-RH group were not routinely obtained. Thirty-three percent of patients in the RH group had an acute coronary lesion compared with 19% in the non-RH group.
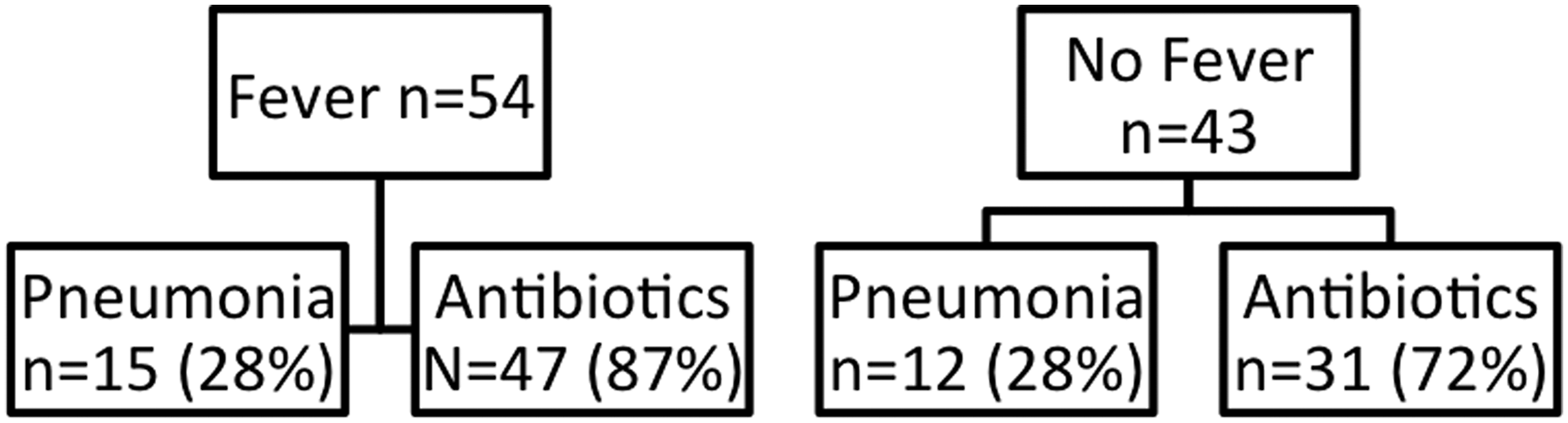
Incidence of pneumonia and utilization of broad spectrum antibiotics.
CABG, coronary artery bypass graft; PCI, percutaneous coronary intervention; V.Fib, ventricular fibrillation; V.Tach, ventricular tachycardia; PEA, pulseless electrical activity; ROSC, return of spontaneous circulation.
Twenty-seven of 54 patients (50%) with RH died during the hospital stay, whereas 20 of 43 (47%) died in the non-RH group (p = 0.84). Eighteen of 54 (33%) of those with RH had a favorable neurologic outcome compared with 16 of 43 (37%) in the non-RH group (p = 0.85) (Table 2). Among patients with severe RH (T ≥ 38.5°C), 18 of 28 (64%) died during the hospital stay, whereas only 29 of 69 (42%) without severe RH died before hospital discharge (p = 0.078). Eight of 28 (29%) patients in the latter cohort had a favorable neurologic outcome compared with 26 of 69 (38%) who had it in the group without severe RH (p = 0.48) (Table 3).
IABP, intraaortic balloon pump; CPC, cerebral performance category.
Discussion
Although RH postcardiac arrest is a relatively common phenomenon, its significance has not been fully investigated. Fifty-six percent of the patients in our cohort with OHCAs who underwent hypothermia protocol developed fever within 24 hours of initiation of rewarming, which is consistent with previous studies. This retrospective analysis did not show statistically significant difference in mortality or neurologic outcome between the patients with and without RH, although it showed a strong tendency of higher mortality if we apply stricter definition of hyperthermia.
There are several possible causes for fever in the postcardiac arrest period. In our retrospective cohort, acute lesions on coronary angiography were seen in 33% of patients with RH and in 19% of patients without RH (p = 0.16). Acute myocardial infarction can cause systemic inflammatory response syndrome (SIRS). SIRS was shown to be prevalent in 25% of ST-elevation myocardial infarction patients on presentation in one series and it may be a major cause of RH in subjects with cardiac arrest secondary to an acute myocardial infarction (van Diepen et al., 2013). Infection is an important cause of fever. In our cohort, 23% of those with fever had a positive blood culture. Another postulated mechanism for fever in a patient with SIRS is impaired perfusion of the intestinal tract, which enables transmigration of bacteria across the mucosal lining. In the SHOCK trial, 18% of patients with an acute coronary occlusion were found to meet SIRS criteria and 74% of those patients had a positive blood culture (Kohsaka et al., 2005). A meta-analysis suggests an association between therapeutic hypothermia and sepsis (Geurts et al., 2014). Since fever is masked by therapeutic hypothermia, careful attention is necessary for signs of infection.
Another possible etiology for RH is neurogenic fever from profound cerebral ischemia, a phenomenon known to portend a poor prognosis in acute stroke (Azzimondi et al., 2005). Furthermore, fever may exacerbate neurologic injury and is known to be detrimental in the immediate postcardiac arrest period (Zeiner et al., 2001).
Previous studies have varied their temperature cutoff of rebound hypothermia, ranging from 38.0°C to 38.5°C (Bro-Jeppesen et al., 2013; Gebhardt et al., 2013; Leary et al., 2013; Winters et al., 2013; Cocchi et al., 2014). In our cohort, using the stricter 38.5°C cutoff for RH, we found mortality increased from 50% to 64% in the RH group and it decreased from 47% to 42% in the group without RH. The incidence of RH dropped from 56% to 29% using the new cutoff temperature. Although the difference was not statistically significant, there was a strong trend in increased mortality by applying strict criteria. The clinical impact of RH may be proportional to the magnitude of the RH. A larger study may be able to show the difference.
Conclusions
RH is common after completion of therapeutic hypothermia in comatose patients due to cardiac arrest. We found no significant clinical impact of rebound hypothermia on neurologic outcome or mortality, but our study was underpowered to reveal such impact if it exists.
Footnotes
Author Disclosure Statement
No competing financial interests exist.