
Abstract
Intracerebral hemorrhage (ICH) is often a devastating stroke, and there are no clinically proven neuroprotective treatments. Considerable research points to iron toxicity as a leading contributor to secondary damage after ICH. Iron, released from degraded erythrocytes, catalyzes free radical production, thereby causing cell death in the ensuing days and weeks. Therapeutic hypothermia (TH) is a potential neuroprotective strategy for ICH, but results from animal studies are inconsistent and generally weaker than that found in ischemia models. Thus, we examined whether TH (∼33°C for 24–72 hours) would specifically mitigate iron toxicity, which we modeled by infusing 3.8 μg of FeCl2 in 30 μL of sterile saline into the striatum of rats. Rats were subjected to whole-body cooling beginning 1 hour after FeCl2 infusion. Use of TH reduced (p = 0.025) the small bleed caused by FeCl2 infusion (∼6 μL). However, TH did not lessen FeCl2-induced edema at 24 and 72 hours postinfusion, nor were behavioral impairments (e.g., walking) or brain injury (at 7 and 28 days) attenuated by TH. These results suggest that TH does not directly protect against iron toxicity, which indicates that this is not a means by which TH improves the outlook after ICH.
Introduction
T
Clinical interest for large intracerebral hemorrhage (ICH) is based upon data showing that cooling lessens edema and raised intracranial pressure after ischemic stroke (Yenari and Han, 2012). Furthermore, small clinical studies support the use of TH after ICH (Feng et al., 2002; Staykov et al., 2013; Su et al., 2015), as do animal studies, which find TH to reduce edema (Kawanishi, 2003; Wagner and Zuccarello, 2005; MacLellan et al., 2006b; Fingas et al., 2007; Kawanishi et al., 2008) and intracranial pressure (John and Colbourne, in press) along with other protective effects (MacLellan et al., 2006b; Kawanishi et al., 2008; Sun et al., 2013, 2015). Nonetheless, TH may not effectively target all mechanisms of injury, which probably varies with treatment parameters, models, etc. For instance, some find that TH reduces the harmful effects of thrombin (Kawai et al., 2001), whereas others do not (Wowk et al., 2014).
It is widely accepted that iron toxicity substantially contributes to secondary damage after ICH (Aronowski and Zhao, 2011). Free iron, originating from the breakdown of hemoglobin, catalyzes the production of hydroxyl radicals (oxidative stress). Iron levels increase and remain persistently elevated in the brain after ICH, and this causes oxidative injury (Aronowski and Zhao, 2011). Further evidence from animal studies show that free radical scavengers and iron chelators, such as deferoxamine (Cui et al., 2015), are neuroprotective. Moreover, direct infusion of iron, such as FeCl2, is neurotoxic, thereby adequately modeling iron toxicity following ICH. Notably, FeCl2 infusions cause oxidative stress, edema, and acute and chronic cell death as seen in ICH models (Nakamura et al., 2006; Willmore and Ueda, 2009; Caliaperumal et al., 2012). We hypothesized that cooling would directly attenuate free radical production (through slowing chemical production) while also mitigating downstream effects (e.g., edema) that contribute to injury. Thus, we used a simple model, similar to our recent thrombin study (Wowk et al., 2014), to assess TH against iron (FeCl2)-mediated toxicity. Use of simple models, such as this, is common in stroke research, including for ICH (e.g., balloon inflation model and the infusion of individual blood components), where the goal is to isolate a particular mechanism for study.
Methods
Animals and experimental conditions
All procedures were conducted in accordance with the Canadian Council on Animal Care under the approval of the University of Alberta's Biosciences Animal Care and Use Committee. One hundred fourteen male Sprague Dawley rats (250–350 g, ∼10–11 weeks old) were housed in cages with wood chip bedding in a temperature and humidity controlled room on a 12-hour light cycle. Animals were given ad lib water and food (Rodent Chow, Lab Diet), except during certain testing conditions. Animals were randomized into normothermia (NORMO) or hypothermia (HYPO) groups, and most data were analyzed blinded to group identity. However, blinding was sometimes impossible (e.g., euthanizing rats when they were still cold). Several experiments were done. First, we evaluated whether TH affected bleeding (n = 8/group). Second, we assessed whether TH affected edema at 24 (n = 11/group) and 72 hours postinjury (n = 8/group). Lastly, we determined whether TH impacted tissue loss and behavioral impairments at 7 (n = 14/group, experiment 3) and 28 days postinjury (n = 16/group, experiment 4).
Temperature probe surgery
All rats had a temperature probe (TA10TA-F20 or F40 Transoma Medical) implanted into their peritoneal cavity 4–5 days before FeCl2 infusion. Briefly, rats were anesthetized with isoflurane (4% induction and 1.5–2% maintenance in 60% N2O and balance O2) and a small midline abdominal incision was made for insertion of the sterilized transmitter. The wound was sutured and Marcaine was used as a local anesthetic. Rats were placed in separate cages over receivers (RPC-1; Transoma Medical) for data collection (MacLellan et al., 2006b). Temperature was sampled every 30 seconds through ART 2.3 (Transoma Medical). Probes were calibrated to within 0.2°C accuracy. All rats tolerated this procedure well, and there were no signs of surgical complications.
Iron infusion surgery
Rats were anesthetized with isoflurane and a midline scalp incision was made. Using a stereotaxic frame, a hole was drilled 0.5 mm anterior and 3.5 mm lateral to Bregma. A Hamilton syringe was lowered 6.5 mm from the skull surface and 3.8 μg of FeCl2 in a 30 μL solution of sterile unbuffered saline was infused over 10 minutes, during which time the body temperature was regulated at normothermia by a heating pad (Nakamura et al., 2006; Caliaperumal et al., 2012). The needle was left in place for an additional 10 minutes to prevent backflow. The scalp was sutured and Marcaine was applied. Rats were then placed in their cage for temperature monitoring.
It should be noted that the insertion of a needle into the brain unavoidably causes a small hemorrhage (a few microliters) and minor brain injury. The slow infusion of 30 μL of saline or acidic saline (to match the FeCl2 infusion), however, appears to be of little additional consequence (Willmore et al., 1980; Caliaperumal et al., 2012). Thus, a FeCl2 infusion causes brain injury and related events almost entirely from iron-mediated oxidative stress.
Temperature monitoring and control
Baseline temperature was recorded on the day before FeCl2 infusion surgery. The NORMO group was only monitored after FeCl2 surgery, whereas HYPO rats also had their temperature regulated by a servo-regulated system consisting of a fan, water mister, and an infrared heat lamp (Colbourne et al., 1996). These devices were situated above the rat's cage, and whole-body hypothermia was precisely maintained in freely moving animals (no anesthesia). The HYPO rats were cooled to ∼33.0°C over 1 hour beginning 1 hour after iron infusion. They were kept at this level until euthanasia at 24 or 72 hours at which time edema was measured (experiments 1 and 2). In experiments 3 and 4, rats were cooled for 72 hours then rewarmed over 6 hours (0.5°C/hour). In our laboratory, such protocols give superior protection in models of global (Colbourne et al., 1999) and focal ischemia (Clark et al., 2008), and they appear to have no lasting behavioral or histological effects in normal animals (Auriat et al., 2012). Although initiating TH an hour after iron infusion may not appear clinically relevant, it should be kept in mind that iron toxicity does not occur immediately after an ICH, and so cooling could easily be applied during much of the acute toxic effects. In addition, FeCl2 infusion causes protracted cell death, edema, and so on, therefore, cooling was applied during this period.
Bleeding
Blood volume was evaluated with a spectrophotometric hemoglobin assay as recently done (John et al., 2015). Rats were anesthetized with isoflurane and decapitated at 48 hours postinjury. Each whole hemisphere was separately homogenized in double distilled water (1:4 weight:volume ratio), left to incubate on ice, and then centrifuged at 15,800 g for 35 minutes. The supernatant was divided into aliquots that were reacted with Drabkin's solution. The absorption values (measured at 540 nm; Model 4001/4; Thermo Fisher Scientific) were compared to a standard curve based on known quantities of blood. This method measured blood present within the vasculature as well as that caused by the experimental procedures (needle insertion and infusion of iron). The contralateral-to-infusion hemisphere contained only blood within the vasculature (i.e., serves as an internal control).
Edema
Rats were anesthetized and decapitated to determine brain water content at 24- or 72-hour survival times. The wet weight of the ipsilateral (IPSI) and contralateral (CONTRA) striatum (from 2 mm anterior to 4 mm posterior to the injection site) and the cerebellum were taken. The brains were then baked for 24 hours at 100°C to determine dry weight. Brain water content was calculated as [(wet weight − dry weight)/wet weight] ×100, with levels >78% indicative of edema.
Behavioral testing
Rats in the last two experiments underwent behavioral assessment before and after surgery. In experiment 3, the corner turn test (CTT), neurological deficit scale (NDS), and the horizontal ladder test were used to evaluate deficits 7 days postinjury. In experiment 4, the horizontal ladder test was used to assess impairments 28 days postinjury, while the Montoya staircase was used on days 24–28. These tests are sensitive to striatal injury (MacLellan et al., 2006a; Caliaperumal et al., 2012).
The CTT consists of two walls (41 cm high by 30.5 cm wide) placed at a 30° angle with a 0.5 cm gap. At baseline, the direction each rat turned coming out of the corner was averaged over 2 days (10 trials/day). Rats with a strong turning bias (<30% in one direction) were excluded from analysis of this test data to avoid floor or ceiling effects that might mask the influence of treatment. The turning preference was determined over 10 trials during the postinsult testing session.
The NDS is a composite of several simple motor tasks (hindlimb retraction, contralateral forelimb flexion, bilateral forepaw grasp, beam walking, and spontaneous circling), each of which range in a score from 0 to 3, except the contralateral forelimb flexion that ranges from 0 to 2. Fourteen is the maximum impairment.
The ladder test measured the walking ability across a horizontal ladder (1 m) with metal rings (3 mm diameter) randomly spaced 1–4 cm apart. Rats were trained to make four traverses while they were video recorded for later determination of the number of successful steps and errors. Rats were excluded if they did not cross at least twice, and this was to ensure we had a sufficient sample to accurately estimate their performance.
The staircase test measures skilled reaching. Rats were placed in a plexiglass box (length: 30 cm; width: 6.8 cm; height: 12 cm) and trained to reach for sugar pellets (45 mg; Bio-Serv) from a bilaterally placed staircase. The number of pellets consumed with each forelimb was recorded (maximum 21 pellets/side/trial) during training (two 15-min trials/day, 5 days/week, 4 weeks) and testing (24–28 days post-FeCl2). The last week of training served as a baseline measurement (stable performance), and any rat that failed to reach at least eight pellets with a paw was excluded from this test. This was done to avoid floor effects (i.e., exclude poor performers). During training and testing in the staircase test, the rats were food deprived to ∼90% of their free-feeding body weight accounting for natural growth over time. Body weight was repeatedly measured during this period and found to be similar between groups. In this study, food deprivation ended several days before surgery to allow rats time to regain lost weight. In addition, these rats were not food deprived again until ∼3 weeks after FeCl2 surgery.
Histology
After behavioral assessment at 7 or 28 days, the rats were anesthetized with pentobarbital (100 mg/kg, i.p.) and perfused through the heart with 0.9% saline followed by 10% formalin. The brains were removed and later cryosectioned for assessment of lesion volume. For this, a 40-μm thick section was taken every 200 μm starting anterior to the lesion and ending posterior to injury. Sections were stained with Cresyl Violet and 1 in every 10 sections was analyzed using ImageJ software (Scion Corporation). The following formulas were used to determine tissue loss (MacLellan et al., 2006a; Caliaperumal et al., 2012):
Hemisphere volume = average (area of the complete coronal section of the hemisphere − area of ventricle − area of damage) × interval between sections × number of sections.
Lesion volume = remaining volume of normal hemisphere − remaining volume of injured hemisphere.
Statistical analyses
Descriptive statistics are given as mean ± standard deviation (SD) or medians. Data were analyzed using analysis of variance (SPSS v.21; SPSS, Inc.), except the NDS scores, which were analyzed with Mann–Whitney U and Wilcoxon tests.
Results
Experiment 1
No exclusions or mortality occurred in experiment 1. Infusion of FeCl2 caused a small ∼6 μL increase in blood volume in NORMO rats at 48 hours (p < 0.0011 vs. contralateral hemisphere), which TH attenuated (Fig. 1, p = 0.025). The contralateral hemispheres were similar between groups (p = 0.659). Temperature was controlled as desired, and discussed below for Experiment 4 (representative data).
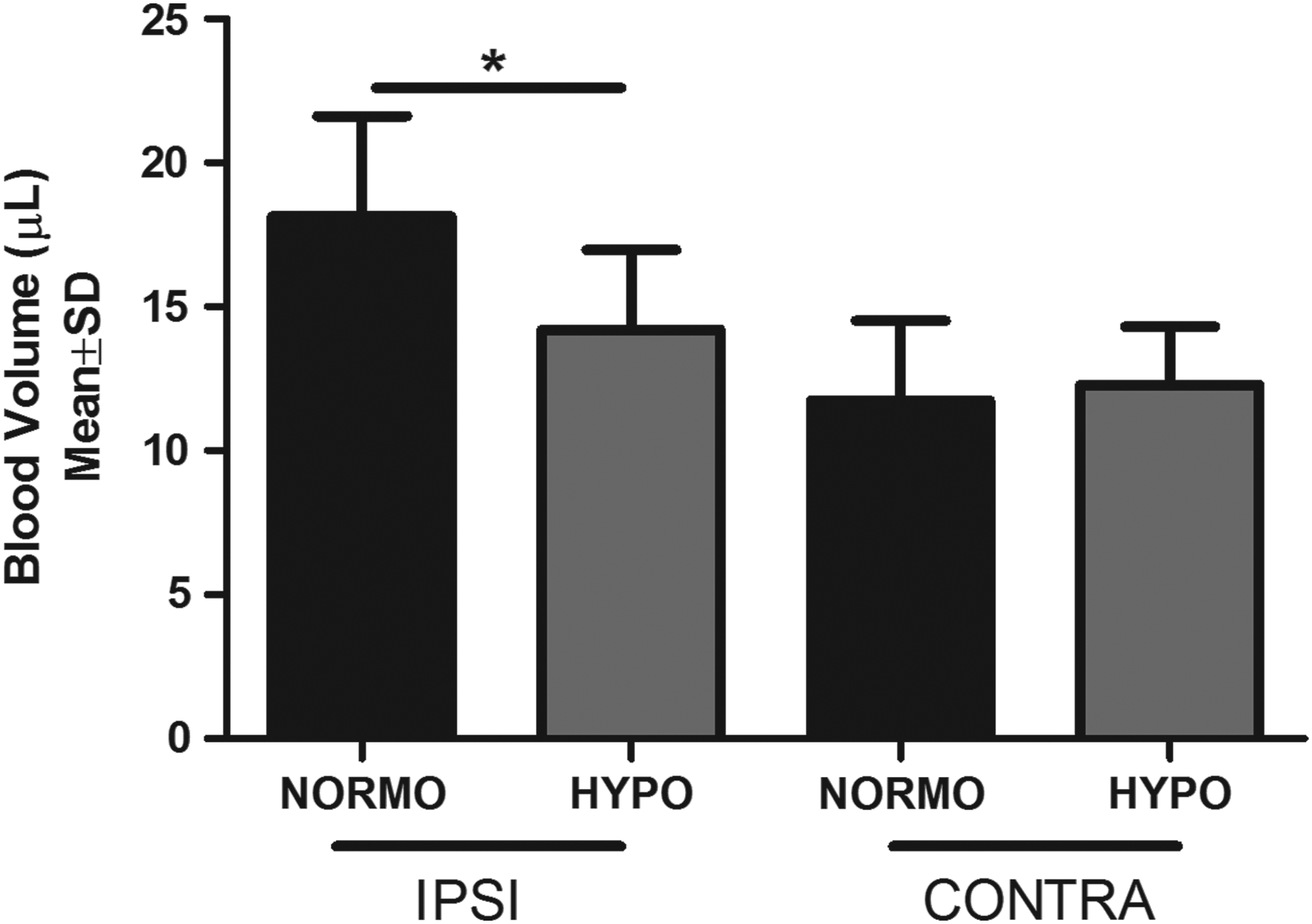
The effect of therapeutic hypothermia (TH) on trauma (needle insertion) and iron-induced bleeding is shown. There was a small bleed in the NORMO group's ipsilateral (to infusion, IPSI) hemisphere. The total volume of blood in this hemisphere was attenuated by TH (*p < 0.025). The contralateral (CONTRA) hemisphere data show the normal amount of blood found within the cerebral vasculature (i.e., it is a control sample), which was not affected by cooling (of the IPSI hemisphere). HYPO, hypothermia; IPSI, ipsilateral; NORMO, normothermia; SD, standard deviation.
Experiment 2
One NORMO and one HYPO rat died during surgery of unknown cause. Infusion of FeCl2 caused striatal edema at 24 (Fig. 2A) and 72 hours (Fig. 2B). Cooling had no effect (p ≥ 0.139). Cerebellum control samples were normal (p ≥ 0.650).

Infusing FeCl2 caused significant edema (i.e., above normal brain water content) at 24
Experiment 3
Two HYPO-assigned rats died from surgical errors (before HYPO treatment) and one was euthanized early because its temperature did not remain normothermic after rewarming. For the CTT, one animal was excluded from each group due to baseline turning bias. At 7 days postinjury, no behavioral deficits were detected with the CTT (Fig. 3A) because there was no Time (p = 0.214), Group (p = 0.247), or interaction (p = 0.548) effects. For the NDS, there was a significant postinfusion impairment (Fig. 3B, p = 0.001), but no treatment effect on day 7 (p = 0.120). For the forelimb success rate on the ladder test (Fig. 3C), there were significant Time (p < 0.001) and Group effects (p = 0.047), but no interaction (p = 0.978). As baseline forelimb scores differed (p = 0.047), we analyzed the day 7 data as a percent of baseline, which were not different between groups (p = 0.787). Thus, cooling had no impact on forelimb walking errors. The success rate for the hind limb was significantly different over time (Fig. 3D, p < 0.001), and there were significant Group (p = 0.010) and interaction effects (p = 0.008). While there was no difference in baseline scores (p = 0.963), there was a significant difference at day 7 (p = 0.004) when HYPO rats had greater walking impairment. Finally, FeCl2 caused substantial striatal damage by 7 days (Fig. 4A, B), which TH did not significantly mitigate (p = 0.110, Fig. 4C).

The effects of TH on iron-induced behavioral deficits 7 days postinjury on the CTT
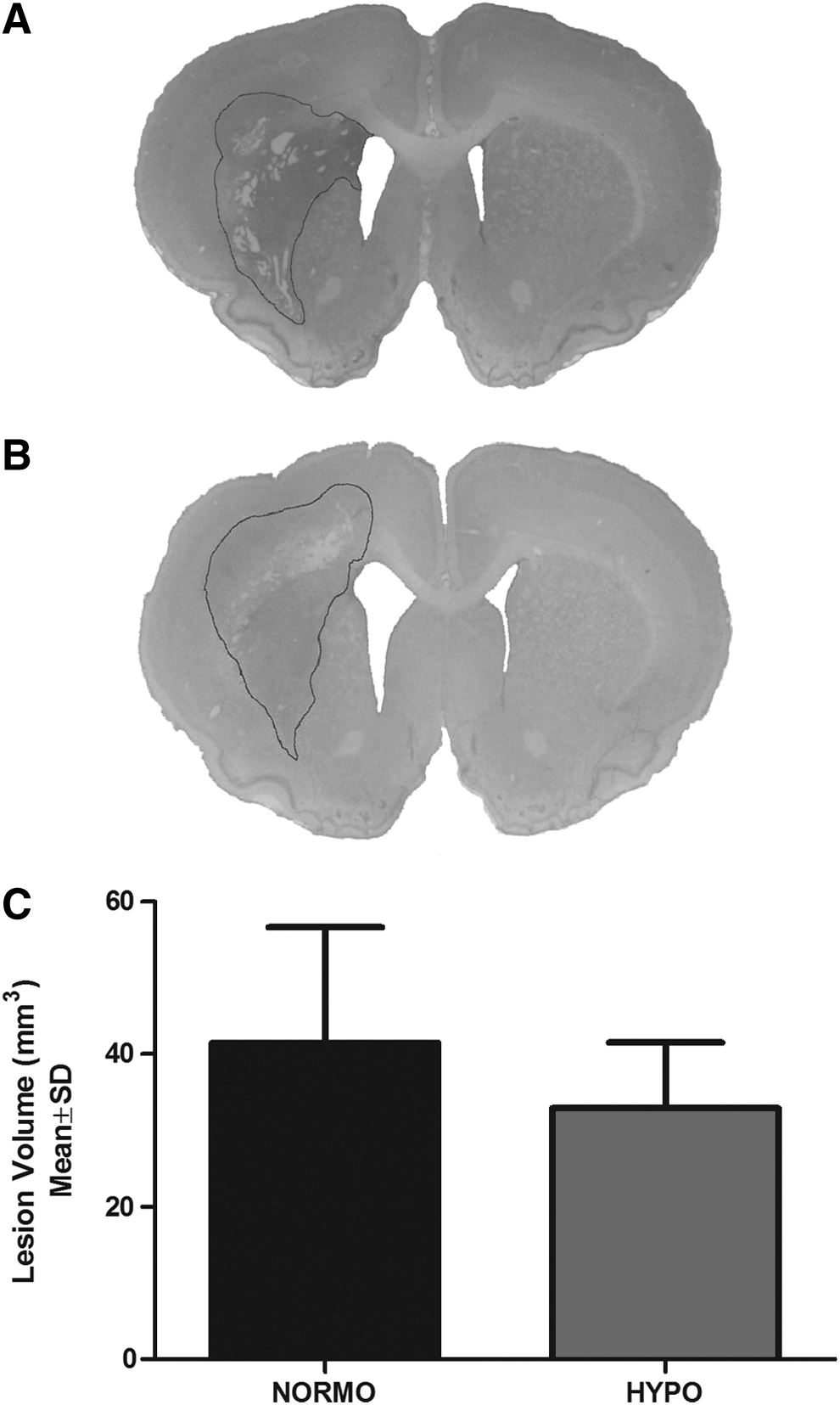
Infusion of FeCl2 caused significant tissue loss largely within the striatum of both NORMO
Experiment 4
No mortality occurred in this experiment. Figure 5 contains the postinfusion temperature data that are also representative of the other experiments, but note that HYPO rats were euthanized before rewarming in experiments 1 and 2. Baseline temperature data were normal in all cases (not shown).
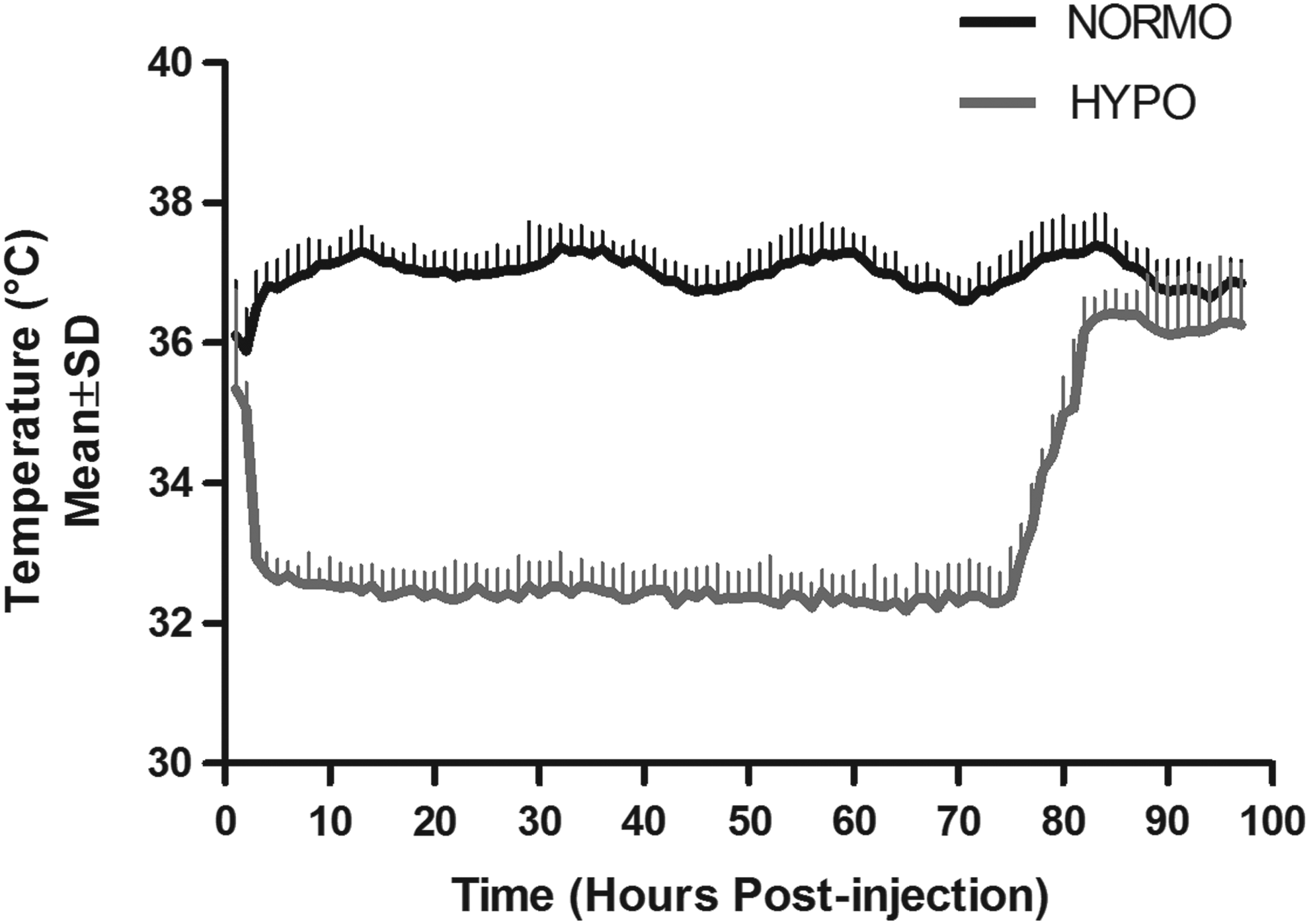
Core temperature (°C) was measured through implanted telemetry probes (two samples per minute with data averaged every hour). Whole-body hypothermia was initiated at 1 hour after FeCl2 infusion and typically kept to within 0.5°C of the target temperature. These data from experiment 4 are representative of all experiments. Baseline temperature data (not shown) were normal in all cases.
There were significant walking impairments on the ladder test, but no effect of TH. This was evident by the significant Time effects (p < 0.001) with the nonsignificant Group (p ≥ 0.688) and interaction effects (p ≥ 0.193) for the affected forelimb (Fig. 6A) and hind limb (Fig. 6B). In total, six animals were excluded on the staircase test for failing to meet baseline criteria—2 NORMO and 4 HYPO rats. There was a significant Time effect (Fig. 6C, p < 0.001), but no Group (p = 0.444) or interaction effect (p = 0.873). Thus, rats had reaching impairments after FeCl2 infusion, but there was no effect of TH. Significant tissue loss was observed at 28 days (Fig. 7A, B) and there was no effect of TH (Fig. 7C, p = 0.132).
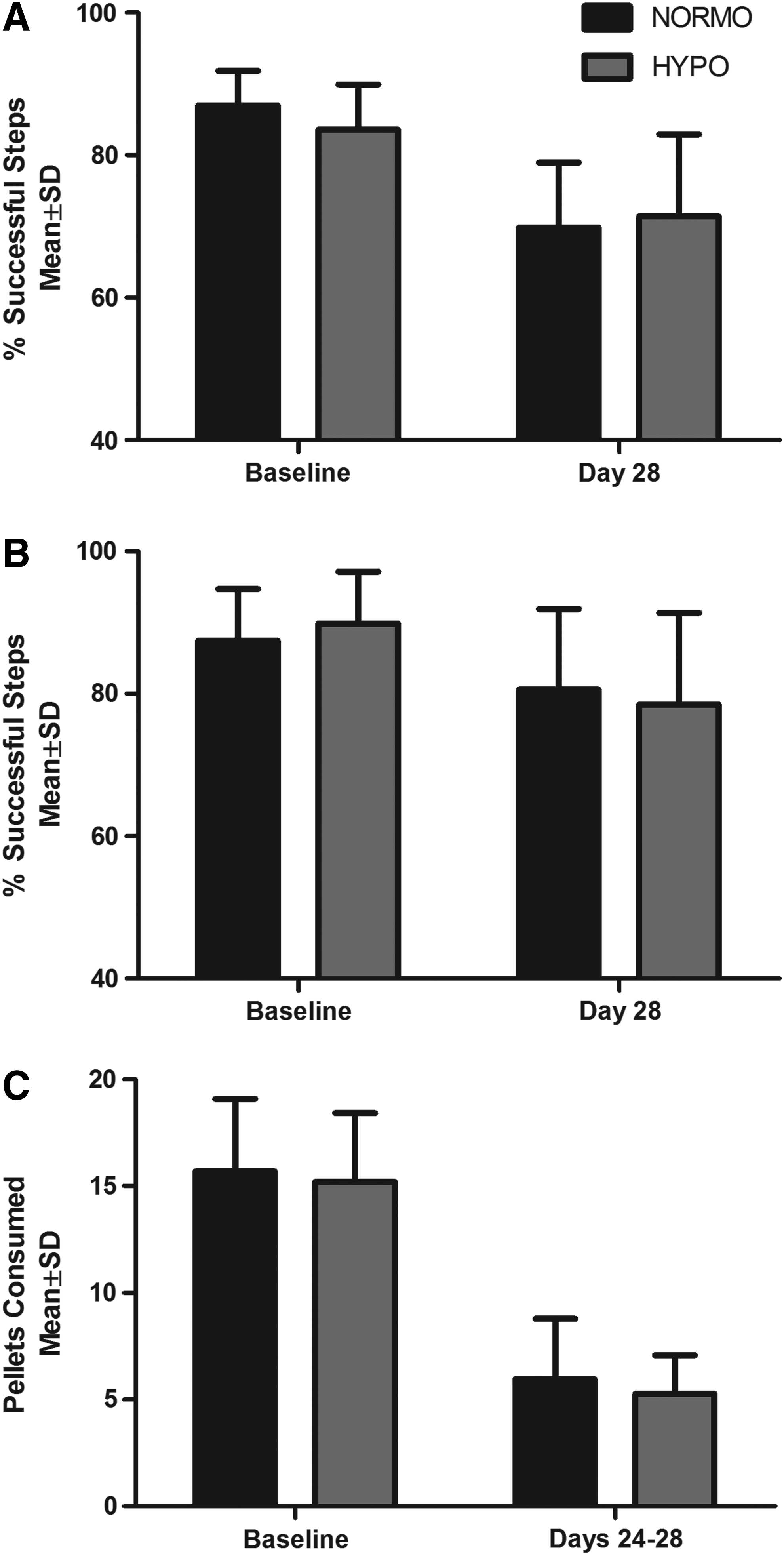
Significant and lasting behavioral deficits (p < 0.001) occurred weeks after FeCl2 infusion for the ladder (
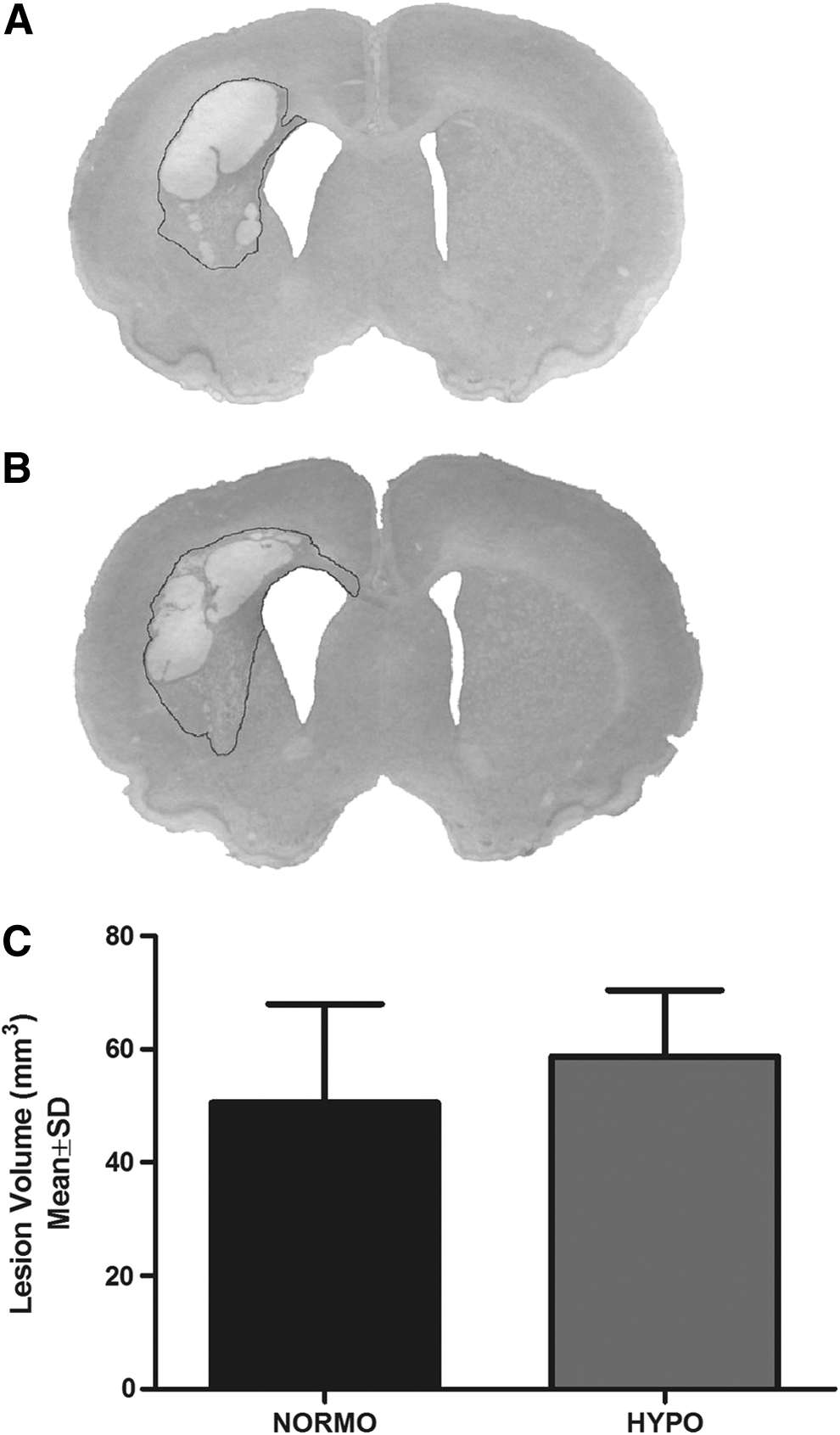
Infusion of FeCl2 caused damage largely to the striatum of NORMO
Discussion
We used the simple FeCl2 model as a way to estimate the specific therapeutic effects of TH against iron-mediated secondary damage after ICH. While iron infusions caused cell death, edema, and behavioral deficits, the use of TH was ineffective. Accordingly, it follows that the beneficial effects of using TH after ICH, such as reducing edema and raised intracranial pressure, are likely not mediated through attenuating iron toxicity. This therapeutic weakness against a key mechanism of secondary degeneration might explain hypothermia's modest efficacy against ICH. As such, it may be possible to augment the benefits of TH by adding a drug that targets iron toxicity (Goossens and Hachimi-Idrissi, 2014).
Although this simplified model of iron-induced injury has been repeatedly used in ICH research (Nakamura et al., 2006; Caliaperumal et al., 2012), it certainly has limitations, as do all such models (e.g., balloon inflation). First, these models exclude many interacting effects with other mechanisms of damage, some of which are likely sensitive to TH. Furthermore, extrapolating from the FeCl2 model to ICH is complicated by the fact that we do not yet fully know the real impact of iron toxicity after ICH. This means, for example, that the lack of benefit against iron toxicity may not mean that much in those ICHs where iron toxicity is minimal. Second, there are specific concerns with the bolus infusion of FeCl2, such as the fact that iron release from hemoglobin occurs much more slowly. Nonetheless, the FeCl2 model does induce several mediators of injury that are shared with ICH, such as oxidative injury, edema, and seizures (Nakamura et al., 2006), and the acute and chronic tissue loss seems similar (Caliaperumal et al., 2012). Third, we timed TH to overlap with much of the injury caused by FeCl2 and the time course over which drugs have been found effective, including chelators such as deferoxamine (Cui et al., 2015). As well, our TH protocol roughly matches effective doses used for ischemia (Colbourne et al., 1999; Clark et al., 2008) and ICH (MacLellan et al., 2004; Kawanishi et al., 2008), including in some clinical studies (Staykov et al., 2013). Nonetheless, other TH regimens or methods may have provided more benefit or they may have worked against milder or more severe FeCl2 insults. Such general possibilities exist with any negative study, and by the same logic, these concerns hold for follow-up studies to an initially positive finding.
The effectiveness of TH varies considerably among ICH studies owing to numerous study differences (e.g., models and protocols). Regardless, even in the best of cases, it seems that TH is considerably less effective than against ischemia. Perhaps this is because TH cannot directly impact primary (mechanical) damage and it apparently fails to mitigate several mechanisms of secondary damage, including iron (present data) and thrombin toxicity (Wowk et al., 2014). Additionally, TH may cause several side effects that limit efficacy, including aggravating bleeding (MacLellan et al., 2004; John et al., 2015). While we excluded that possibility here (bleeding was slightly less), it is conceivable that TH blunts the upregulation of endogenous protective mechanisms that counter iron toxicity, such as ferritin expression (Aronowski and Zhao, 2011). Likewise, the anti-inflammatory effects of TH after an ICH (MacLellan et al., 2006b; Kawanishi et al., 2008) might not be helpful against iron toxicity, where such cells play an essential role (e.g., hematoma clearance after ICH). Such counterproductive effects may certainly occur in these models, which we are currently evaluating in ICH (e.g., whether TH affects iron release and distribution).
Although TH appears to treat high levels of edema and intracranial pressure after ICH (Feng et al., 2002; Staykov et al., 2013; John and Colbourne, in press), there are significant limitations. The current findings illustrate one of these, which is the lack of benefit against iron toxicity—a potentially key contributor to secondary damage after ICH (Aronowski and Zhao, 2011). These findings shed light on the inconsistent and limited protective properties of TH in the setting of ICH. Furthermore, they suggest a way forward, which is the combination of rationally selected treatments with TH (Goossens and Hachimi-Idrissi, 2014) along with the careful control of physiological complications.
Footnotes
Acknowledgments
Research support provided by the Canadian Institutes of Health Research by a grant to F. Colbourne who is supported by a “Canada Research Chair in Intracerebral Hemorrhage” salary award. The authors thank Michael Williamson and Colby Nadeau for helpful comments on the article.
Author Disclosure Statement
No competing financial interests exist.