
Abstract
Liquid ventilation was initially proposed for lung lavage and respiratory support. More recently, it was also investigated as an experimental strategy for ultrafast cooling or organ preservation during ischemic disorders. The goal of this article is to identify and review the studies that investigated liquid ventilation in the field of resuscitation sciences. An exhaustive analysis of the literature was performed using the Medline database up to 15th September 2015. Articles were selected according to their relevance. All articles focusing on respiratory support were excluded. On the basis of 76 retrieved studies from the Medline database, 29 were included in this review. All studies were experimental reports and most of them investigated the cooling properties of liquid ventilation in animal models of experimental cardiac arrest or coronary artery occlusion in rabbits or pigs. Animal studies demonstrated a wide range of potential applications of total liquid ventilation in resuscitation sciences. This strategy is able to provide ultrafast cooling, independent of the body weight. In animal models of cardiopulmonary resuscitation, it was shown to provide potent benefits widely linked to cooling rapidity.
Introduction
L
Chemically, PFCs are organic compounds in which hydrogen atoms have been substituted by fluorides or other halogen atoms. They have a high density (nearly twice higher than water), very low surface tension (Kaisers et al., 2003), and a great oxygen and carbon dioxide carrying capacity (16 and 3 times more than blood for O2 and CO2, respectively) (Davies, 1999). Due to their very high vapor pressure, PFC is very volatile and can also be easily eliminated by evaporation from the lungs (Jeng et al., 2001). All these properties make them good candidates as a medium for gases' transportation within the lungs through liquid ventilation. They have been mainly studied for the treatment of respiratory dysfunction through two major modalities of total liquid ventilation (TLV) or partial liquid ventilation (PLV).
TLV was the first to be investigated. In this situation, lungs are completely filled with PFC and a tidal volume of liquid is administered at the respiratory frequency (Shaffer et al., 1992; Wolfson et al., 1992; Hirschl et al., 1995). Due to the complete filling of the lungs, this strategy abolishes the liquid–gas interface and subsequently improves the lungs mechanics. TLV has also been shown to increase the mechanical recruitment of collapsed alveoli and the ventilation/perfusion ratio by compressing blood vessels (Davies, 1999). In addition, TLV can mechanically remove debris and secretion from the airways (Galvin et al., 2013) and present surfactant-like (Wolfson and Shaffer, 2005) and anti-inflammatory properties (Zhu et al., 2010).
TLV was initially shown to improve gas exchanges during acute respiratory distress syndrome (ARDS) or acute lung injury (ALI) in animal studies (Fujino et al., 2000; Pakulla et al., 2004; Wolfson et al., 2008). However, the procedure of TLV requires the use of a liquid ventilator able to safely ventilate the lung with PFC. It can indeed lead to dramatic baro-/volutrauma if the pulmonary pressure and volume are not adequately controlled during liquid ventilation.
Accordingly, TLV was not really investigated in clinical trials, except one study with “gravitational” liquid ventilation. In this study, the lungs were alternatively filled and drained by the force of gravity in three preterm babies experiencing dramatic respiratory distress. A transient improvement in lung compliance and oxygenation was observed (Greenspan et al., 1989), but severe barotrauma appeared in one infant and supported the need for a specific liquid ventilator controlling airway pressure and PFC output.
Since such a ventilator was challenging to design, another and apparently simpler modality of liquid ventilation was proposed through PLV, which consists in the conventional gaseous ventilation of PFC-filled lungs. PLV does not require any specific device except the PFC itself. It was widely investigated for the treatment of respiratory distress during pulmonary diseases (ARDS, ALI, surfactant depletion, and so on) with many promising results in laboratory and small clinical trials (Hirschl et al., 2002; Kacmarek et al., 2006). However, a large-scale clinical trial reported a lack of benefit of PLV in adult patients with ARDS. It was even associated with increased risk of adverse events such as hypoxia, bradycardia, and respiratory acidosis (Galvin et al., 2013). These findings reduced interest in the use of PLV in ARDS patients.
Since that period, new ventilation devices have been developed to overcome the limitations of previous studies (Robert et al., 2006, 2009; Avoine et al., 2011). This has also been proposed for other applications than respiratory distress such as hypothermia induction or lung lavages. In the present review, our goal is to review the state of the art of other promising applications of TLV in the resuscitation field. Several recently published studies support the need of an update of the established findings and future challenges for an ultimate clinical translation of this technique.
Methods
We carefully analyzed all the publications focusing on liquid ventilation in cardiopulmonary resuscitation. Articles were identified by a single reviewer through a systematic search of the Medline and Science direct databases up to 15th September 2015. The search was performed using the following terms: “cardiac arrest”; “ventricular fibrillation”; and “hypothermia,” coupled with the words referring to the intervention (“total liquid ventilation”; “liquid ventilation”; or “perfluorocarbons”), as described in Appendix 1. Articles were read by two reviewers and selected according to their relevance with the subject.
We included investigations in the setting of cardiac arrest, myocardial ischemia, or therapeutic hypothermia with PLV or TLV. Two studies with PFC administration, although intranasal or intrapulmonary administrations were also identified with the previous key words and included in our analysis. All studies focusing on respiratory dysfunction or nonpulmonary administration of PFC were excluded. Included studies were limited to the English language and to original research articles (Fig. 1).
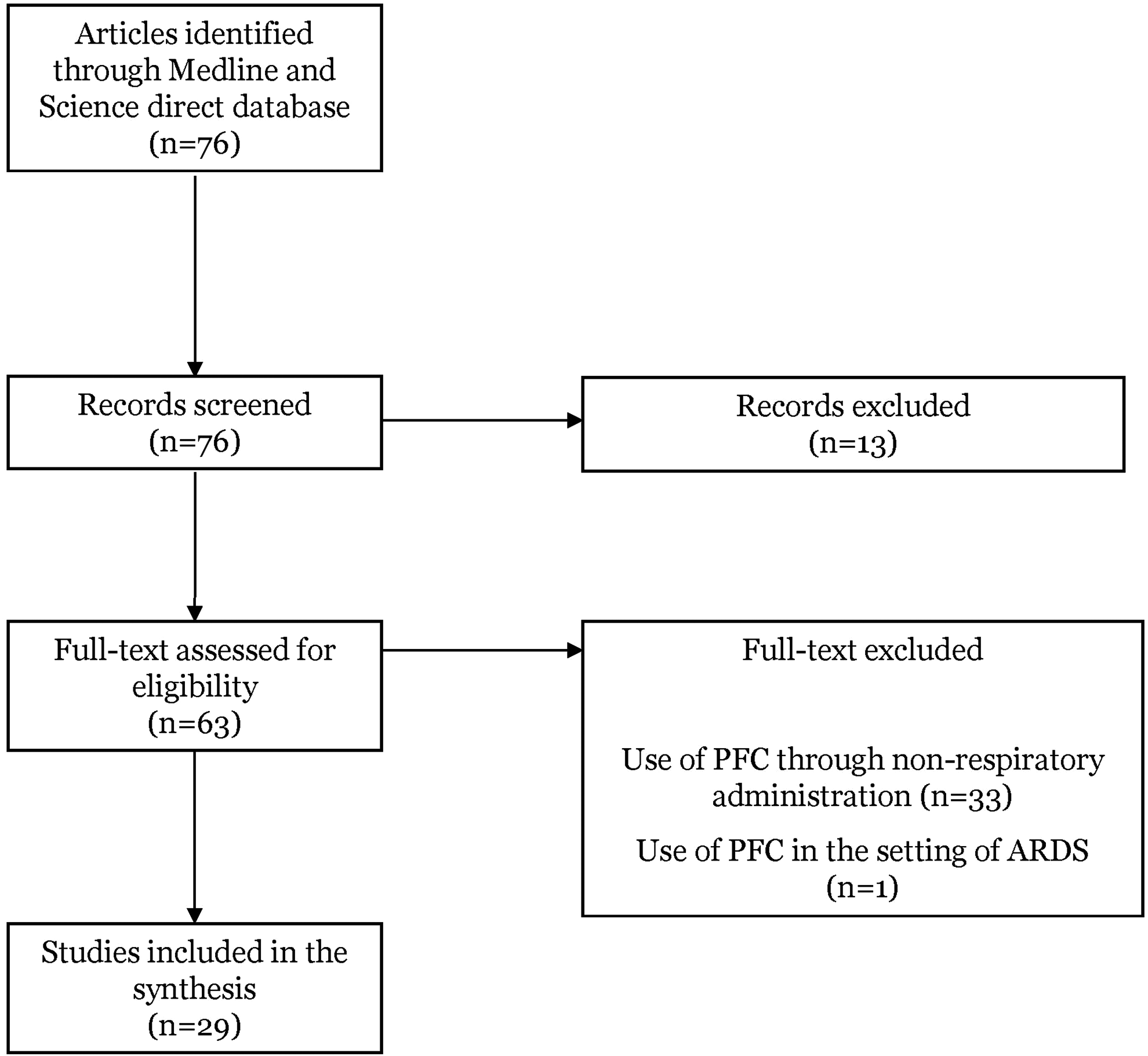
Algorithm of decision process for the selection of articles. ARDS, acute respiratory distress syndrome.
Results
Among the 63 reviewed articles, 29 studies were included in the analysis (Fig. 1). They were all experimental reports. Ten articles were properly describing induction of hypothermia (Shaffer et al., 1984; Forman et al., 1986; Harris et al., 2001; Hong et al., 2002; Wolfson et al., 2008; Castren et al., 2010; Nadeau et al., 2013, 2014; Kumar et al., 2014; Hutin et al., 2015), and two articles the induction of core rewarming through PFC-associated methods (Dickson et al., 2001; Tobias et al., 2001). Other articles focused on the use of liquid ventilation after cardiac arrest (n = 8), (Yoshida et al., 2005; Staffey et al., 2008; Riter et al., 2009; Albaghdadi et al., 2011; Chenoune et al., 2011; Darbera et al., 2013; Tissier et al., 2014; Kohlhauer et al., 2015) during coronary artery occlusion (CAO, n = 5) (Tissier et al., 2007, 2009, 2013; Chenoune et al., 2010; Darbera et al., 2012) or for lung preservation (n = 2) (Yang et al., 2005; Jiang et al., 2006). Two additional articles evaluated the hemodynamic tolerance of TLV (Wolfson et al., 1992; Jiang et al., 2011).
Cooling properties of TLV
The cooling properties of TLV were well demonstrated in all experimental reports, regardless of animal species (Table 1) (Shaffer et al., 1984; Forman et al., 1986; Chenoune et al., 2011; Nadeau et al., 2013).
PFC, perfluorocarbons; TLV, total liquid ventilation; PLV, partial liquid ventilation.
In 1984, cooling was first described as a possible adverse effect of TLV due to the high thermal conductivity of the PFC (Shaffer et al., 1984). In this study, anesthetized cats underwent TLV with PFC at 10, 20, and 30°C. With these different temperatures, the authors described a cooling rate of 9.0, 7.8, and 3.6°C per hour for rectal temperature. Forman et al. (1986) confirmed these results in newborn lambs at a comparable cooling rate with PFC at 20°C (8.4°C/h) and 30°C (4.8°C/h). More recently, it was also confirmed in rabbits that the left atrial temperature could reach 32°C in <5 minutes during TLV with PFC at room temperature (Tissier et al., 2007). Such a very rapid decrease is due to the close proximity between the heart and PFC-filled lungs. In all animal models, TLV is therefore cooling the chest first, then the brain, and finally the abdomen (Staffey et al., 2008; Riter et al., 2009; Tissier et al., 2009, 2010, 2013; Chenoune et al., 2010, 2011; Darbera et al., 2012, 2013; Nadeau et al., 2013).
Overall, the entire body can be cooled to 33°C in few minutes, independent of the species or body weight, (Shaffer et al., 1984; Forman et al., 1986; Chenoune et al., 2011; Nadeau et al., 2013) as similar cooling rates have been described in rabbits (Tissier et al., 2007; Darbera et al., 2013; Kohlhauer et al., 2015), lambs (Nadeau et al., 2013, 2014), cats (Shaffer et al., 1984), and pigs (Hutin et al., 2015). This could be expected, as the fractal organization of tracheobronchial tree can allow comparable exchange independent of the size of the animal. One might speculate that a similar cooling rate could be expected in humans.
Other cooling approaches using PFC
Beyond TLV, other experimental methods have been proposed to cool the body with PFC such as lung lavage or repeated PFC exchanges during PLV (Table 1) (Harris et al., 2001; Tobias et al., 2001; Hong et al., 2002; Wolfson et al., 2008; Kumar et al., 2014). However, the cooling rate was much lower than that previously observed with TLV (Harris et al., 2001) and typically lower than that observed with conventional external cooling (Hong et al., 2002; Yang et al., 2005). For example, pulmonary arterial temperature achieved 35°C after only 38 ± 4 minutes with 10–12 repeated pulmonary instillation of perfluorodecalin at 0°C in rabbits.
In comparison, surface cooling was more efficient and allowed to achieve hypothermia after 23 ± 3 minutes in the same study (Hong et al., 2002). Cooling rate was highly dependent on the frequency of lavage. For example, one cycle every 10 minutes with 4°C PFC took 148.4 ± 24.5 minutes to achieve 30°C in juvenile rabbits (Yang et al., 2005). To increase the cooling rate, it was necessary to increase the frequency of PFC renewal within the lungs. To achieve this goal, Harris et al. (2001) used fast lung lavage (every 20 seconds) to reach the temperature of 32°C within about 18 minutes in dogs. However, such a high frequency of lung lavages implies to use appropriate devices able to cyclically deliver PFC and this method was also associated with impaired gas exchanges.
Importantly, another strategy has been proposed to cool the body with PFC through evaporation of a mixture of PFC and oxygen within the nasal passages (RhinoChill® device). This allows rapid and harmless cooling of the brain (inferior frontal lobe, third ventricle, and superficial parietal lobe) by about 3°C within 10 minutes (Wolfson et al., 2008). This method is remarkably easy to use and could even be implemented in the prehospital setting (Abou-Chebl et al., 2011; Poli et al., 2013; Lyon et al., 2014). However, a disadvantage of transnasal evaporative cooling is a relatively selective cooling of the brain with slower changes in rectal or aortic temperatures (Wolfson et al., 2008). A temperature gradient of about 4°C between the brain and aorta is classically obtained in pigs after 60 minutes of cooling (Boller et al., 2010).
Several feasibility studies were conducted in patients after traumatic brain injury, (Abou-Chebl et al., 2011), stroke (Poli et al., 2013), and cardiac arrest (Lyon et al., 2014). Cooling rate was lower than previously observed in laboratory animal studies with, for example, a mean cooling rate of about −1.5°C/h in stroke patients (Poli et al., 2013). More than 100 minutes were also necessary to reach 34°C in cardiac arrest patients (Castren et al., 2010). This led to an overall lack of benefit compared to conventional cooling, except in subgroups of patients with a cardiopulmonary resuscitation time of <10 minutes (Castren et al., 2010). A large clinical trial is currently ongoing in this particular population (Nordberg et al., 2013).
In a recent study, Kumar et al. (2014) also investigated the role of helium–oxygen mixture with PFC mist as a medium of transpulmonary heat extraction. The authors reported that the brain could reach a target temperature of 32°C in about 60 minutes in 50 kg pigs. This study also reported that the cooling efficiency depends on the amount of PFC within the lungs, as well as the number of recruited pulmonary alveoli and cardiac output (Kumar et al., 2014). This is also consistent with experimental data showing that TLV represents one of the most efficient strategies to cool down the body through highest amount of cold PFC and maximization of the ventilation/perfusion ratio (Davies et al., 1999). TLV even provided a relatively high cooling rate in heart-arrested pigs (Hutin et al., 2015). This suggests potential applications in patients presenting impaired cardiac output.
Rewarming using PFCs
PLV was not only proposed for cooling but also for rewarming with warm PFC (Dickson et al., 2001; Tobias et al., 2001). An original study was performed in miniswine submitted to profound hypothermia (25.9 ± 1.3°C) (Tobias et al., 2001) and eliciting rewarming time of 1.98 ± 0.50 hours to reach normothermia (Tobias et al., 2001). In another study, aortic and pulmonary artery temperatures also increased by 6.6 ± 0.6°C within 30 minutes in pigs submitted to lung lavage with warm PFC after ventricular fibrillation (Dickson et al., 2001). In these two studies, rewarming was, however, slower than that previously observed with cooling, which can be easily explained by the limitation of the maximal temperature of the instilled PFC within the lungs.
Applications in resuscitation
Beyond the direct demonstration of its cooling capacity, several studies further tested the benefit afforded by TLV in animal models of cardiac arrest (Table 2) or focal ischemia (Table 3). The rational relates to the well demonstrated relationship between the benefit provided by hypothermia and its precocity of institution in animal models (Carroll and Beek, 1992; Kuboyama et al., 1993; Colbourne and Corbett, 1995; Takata et al., 2005; Chenoune et al., 2011; Tissier et al., 2013).
CAO, coronary artery occlusion; VF, ventricular fibrillation.
Facilitation of resumption of spontaneous circulation
The first studies with TLV during cardiac arrest were done to test its effect on cardiopulmonary efficacy and resumption of spontaneous circulation (ROSC) facilitation (Menegazzi et al., 2009; Riter et al., 2009; Albaghdadi et al., 2011). Staffey et al. (2008) demonstrated that TLV was able to improve the ROSC occurrence after ventricular fibrillation in swine. Interestingly, this benefit was independent of the temperature of PFC. In addtion, Riter et al. (2009) showed that hypothermic TLV was able to improve ROSC compared to normothermia or cooling through cold saline infusion. This was supposed to be related to the decrease of the right atrial pressure and subsequent improvement of the coronary perfusion pressure.
Independently, it has also been shown that hypothermia, conventionally induced, could improve defibrillation success probability (Menegazzi et al., 2009). Accordingly, the benefit afforded by hypothermic TLV was only observed after ventricular fibrillation, but was not associated with ROSC facilitation in a model of asphyxial cardiac arrest (Albaghdadi et al., 2011). Regarding these conclusions, it seems that the benefit afforded by TLV on ROSC could be related to the procedure by itself rather than hypothermia per se (Staffey et al., 2008). We can assume that the benefit might be exerted through an improvement of both electric shock conduction and cardiac massage efficiency during cardiopulmonary resuscitation (CPR). Interestingly, hypothermia induced by cold saline infusion did not exert any hemodynamic benefit during cardiac massage in a rabbit model of cardiac arrest (Kohlhauer et al., 2014).
Importantly, these studies also showed that it was possible to cool the chest by TLV in arrested-heart animals (Menegazzi et al., 2009; Riter et al., 2009; Albaghdadi et al., 2011). The cooling rate can be further improved in such conditions if a cardiac massage is instituted to resume blood circulation and to improve thermal exchanges in the entire body (Hutin et al., 2015). As an example, abdominal temperature reached 34°C within about 30 minutes in pigs experiencing ventricular fibrillation and cardiac massage (Hutin et al., 2015). The cooling rate remained lower than that previously observed in heart beating pigs (Staffey et al., 2008; Hutin et al., 2015), suggesting that TLV mostly cools through blood circulation from the lungs more than passive convection from the chest. Overall, these studies showed that TLV can be safely instituted during cardiac arrest and chest compression to increase the chance of ROSC and/or preserve the organs during the low-flow period.
Postcardiac arrest syndrome
In addition to its benefit for intra-arrest hypothermia, the effect of hypothermic TLV has also been tested for brain and heart protection after cardiac arrest. Chenoune et al. (2011) investigated the benefit of hypothermic TLV immediately after ROSC in rabbits submitted to 10 minutes of ventricular fibrillation. They reported dramatic benefits with TLV regarding the neurologic status after 7 days of follow-up compared to Control animals and conventional cooling. This neuroprotection was associated with a dramatic improvement in the survival rate (70% vs. 30% and 0% in the groups treated by hypothermic TLV, conventional cooling or normothermic resuscitation, respectively) (Chenoune et al., 2011). The benefit of TLV was only related to the cooling properties as normothermic TLV was not protective in this study.
In another study, Darbera et al. (2013) investigated the benefit afforded by hypothermic TLV in rabbits experiencing 8 minutes of ventricular fibrillation during CAO. This model was characterized by intense cardiac dysfunction due to ischemic myocardial lesions in addition to neurological deficit. TLV was able to cool down the tympanic and esophageal temperature to 32°C within 5–10 minutes, while conventional cooling took about 30–45 minutes. Such ultrafast cooling was associated with similar neurological benefit than that observed with the previous study (Darbera et al., 2013).
In addition, TLV restored the cardiac function and dramatically decreased myocardial infarct size (12% vs. 42% and 55% of risk zone in the groups treated by hypothermic TLV, conventional cooling or normothermic resuscitation, respectively) (Darbera et al., 2013). The survival rate was further increased in the TLV group through significant reductions in both neurological and cardiovascular mortality (80% vs. 30 and 0% in the groups treated by hypothermic TLV, conventional cooling or normothermic resuscitation, respectively).
In a recent study, hypothermic TLV was also able to improve survival by neurological dysfunction limitation after the nonshockable cardiac arrest induced by asphyxia in rabbits. In this model, the neurological benefit provided by TLV was highly related to oxidative stress, blood–brain barrier preservation, and improvement of cerebral hemodynamic. Interestingly, hypothermic TLV was associated with mitigation of the “sepsis-like syndrome,” (Kohlhauer et al., 2015) supporting the importance of systemic cooling and whole body cooling by TLV.
Again, all the protective effects of hypothermia were dramatically increased by TLV in this situation, in comparison to conventional cooling by cutaneous ice packs and cold saline infusion. The potent benefits of TLV were therefore actually related to the rapidity of cooling as conventional cooling did not provide a clear benefit. The latter study also opens promising perspectives regarding the application of hypothermic TLV in the pediatric setting, for example, for pediatric cardiac arrest or neonatal hypoxic encephalopathy.
Cardioprotection
Several studies also investigated the effect of TLV as a protective strategy to limit ischemic myocardial lesions after experimental CAO (Tissier et al., 2007, 2009, 2013; Chenoune et al., 2010; Darbera et al., 2012). As an example, hypothermic TLV was potently able to reduce infarct size when induced during a 30-minute CAO in rabbits (Tissier et al., 2007). Such reduction was observed with intraischemic TLV, but not when hypothermic TLV was initiated at the onset of reperfusion (Tissier et al., 2007).
A further study demonstrated that the benefit afforded by TLV persisted in more severe conditions with 60 minutes of CAO (Chenoune et al., 2010). The cardioprotection was closely related to the delay of induction during ischemia, (Chenoune et al., 2010) with a maximal benefit when TLV was instituted at the onset of CAO compared to 20 minutes later (infarct size: 45 ± 18% and 58 ± 5% of the area at risk, respectively, compared to 82 ± 7% in Control conditions) (Chenoune et al., 2010). In this study, the authors also demonstrated that an external cooling method was insufficient to provide any limitation of infarct size in this model, even when started at the onset of ischemia. All these findings evidenced that the rapidity of cooling is critical for the cardioprotective effect of hypothermia. In this setting, hypothermia is indeed known to target the myocardial ischemic phase, but not the reperfusion injury (Tissier et al., 2010).
In addition to its infarct size reducing properties, hypothermic TLV is also able to improve postischemic cardiac function in rabbits. An initial cooling during the ischemic phase was indeed associated with an ultimate improvement of the regional cardiac contractile function over the three days after reperfusion in rabbits (Tissier et al., 2009). Such improvement was also associated with an improved mitochondrial function regarding transition permeability pore opening and mitochondrial oxygen consumption (Tissier et al., 2009, 2013).
Kidney preservation
Beyond its neuro- and cardioprotective effects, ultrafast cooling with TLV has also been tested for kidney preservation (Table 2). Rabbits undergoing 15 minutes of ventricular fibrillation were submitted to ultrafast cooling through TLV after ROSC. The authors demonstrated that this strategy was able to induce potent organ preservation and limitation of inflammatory kidney markers. This was evidenced by not only morphological markers (electronic microscopy and histology) but also improvement in renal functional parameters (urine production, blood clearance of creatinine, and markers of tubular damage, including N-acetyl-β-(
Lung preservation
Liquid ventilation has also been tested for lung preservation in models of lung ischemic injury (cardiac arrest or cardiopulmonary bypass) (Tables 2 and 3). For example, Yoshida et al. (2005) reported that partial liquid ventilation was able to protect the lung injury after hypotension and cardiac arrest in rabbits. The authors demonstrated that PLV was able to limit significantly the lung endothelial swelling, exudation of neutrophils, and alveolar atelectasis. This was also associated with decreased interleukin-8 levels in the lungs after cardiac arrest. Interestingly, this study demonstrated similar benefit provided by normothermic or hypothermic PLV, suggesting an intrinsic beneficial effect of PFC associated with liquid ventilation rather than a benefit through ultrafast hypothermia.
A study also investigated the cardiovascular tolerance of hypothermic TLV in a piglet model of cardiopulmonary bypass (Jiang et al., 2011). The authors demonstrated that mean pulmonary arterial pressure was not altered by TLV compared to Control conditions. This confirmed that TLV could be very well tolerated regarding the cardiopulmonary function, even in animals with impaired cardiac function during hypothermia induction.
Conclusion and Future Directions
Liquid ventilation has been widely studied during the last decades for respiratory applications. More recently, it has also been investigated at the bench side for induction of therapeutic hypothermia during ischemic disorders. The cooling efficiency of PFC-induced hypothermia is closely related to the amount of PFC within the lung and the rate of liquid exchanges. Among the different PFC-based cooling approaches, TLV therefore presents the highest cooling efficiency compared to other lung instillation methods (lung lavage, partial liquid ventilation, and so on).
Experimentally, it has been shown that such ultrafast cooling is able to maximize the neuro- and cardioprotective effects of therapeutic hypothermia after cardiac arrest and/or myocardial infarction. For several years, TLV was put aside due to technical challenges regarding the control of airways dynamics and barotrauma issues. We are now requiring original liquid ventilators providing secured liquid ventilation. Some prototypes are developed to date and might be tested in patients in the near future (Nadeau et al., 2013, 2014; Hutin et al., 2015; Kohlhauer et al., 2015).
Footnotes
Acknowledgments
This study was supported by “Region Ile-de France” (CORDDIM) and by “Fondation pour la Recherche Médicale” (Grant DBS20140930781).
Author Disclosure Statement
R.T. and A.B. are named as inventors on a patent application on cooling with liquid ventilation (US 13/039415). P.M. is named as an inventor on two patents related to the liquid ventilator (US 7726311; WO 2014205548).
| Search term | Number of results | |
|---|---|---|
| Condition | #1 “cardiac arrest” | 25,532 |
| #2 “ventricular fibrillation” | 22,826 | |
| #3 “hypothermia” | 39,032 | |
| Intervention | #4 “total liquid ventilation” | 69 |
| #5 “liquid ventilation” | 682 | |
| #6 “perfluorocarbons” | 487 |
Search strategy for MEDLINE: last performed on 15/09/2015.
#7 (#1 OR #2 OR #3) (Results: 78,502).
#8 (#4 OR #5) (Results: 9064).
#9 (#7 AND #8) (Results: 76).
#10 (limit #9 to English langage, result: 71).