
Abstract
Adult patients frequently suffer from serious respiratory complications during therapeutic hypothermia. During therapeutic hypothermia, respiratory gases are humidified close to saturated vapor at 37°C (44 mg/L) despite that saturated vapor reduces considerably depending on temperature reduction. Condensation may cause serious adverse events, such as bronchial edema, mucosal dysfunction, and ventilator-associated pneumonia during cooling. To determine clinical variables associated with inadequate humidification of respiratory gases during cooling, humidity of inspiratory gases was measured in 42 cumulative newborn infants who underwent therapeutic hypothermia. Three humidifier settings of 37-default (chamber outlet, 37°C; distal circuit, 40°C), 33.5-theoretical (chamber outlet, 33.5°C; distal circuit, 36.5°C), and 33.5-adjusted (optimized setting to achieve 36.6 mg/L using feedback from a hygrometer) were tested to identify independent variables of excessively high humidity >40.7 mg/L and low humidity <32.9 mg/L. The mean (SD) humidity at the Y-piece was 39.2 (5.2), 33.3 (4.1), and 36.7 (1.2) mg/L for 37-default, 33.5-theoretical, and 33.5-adjusted, respectively. The incidence of excessive high humidity was 10.3% (37-default, 31.0%; 33.5-theoretical, 0.0%; 33.5-adjusted, 0.0%), which was positively associated with the use of a counter-flow humidifier (p < 0.001), 37-default (compared with 33.5-theoretical and 33.5-adjusted, both p < 0.001) and higher fraction of inspired oxygen (p = 0.003). The incidence of excessively low humidity was 17.5% (37-default, 7.1%; 33.5-theoretical, 45.2%; 33.5-adjusted, 0.0%), which was positively associated with the use of a pass-over humidifier and 33.5-theoretical (both p < 0.001). All patients who used a counter-flow humidifier achieved the target gas humidity at the Y-piece (36.6 ± 0.5 mg/L) required for 33.5-adjusted with 33.5-theoretical. During cooling, 37-default is associated with excessively high humidity, whereas 33.5-theoretical leads to excessively low humidity. Future studies are needed to assess whether a new regimen with optimized Y-piece temperature and humidity control reduces serious respiratory adverse events during cooling.
Introduction
F
Recently, therapeutic hypothermia to 32–34°C has been increasingly applied to patients with a range of cerebral injuries (Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest 2002; Todd et al., 2005; Hutchison et al., 2008; Clifton et al., 2011; Jacobs et al., 2013). These patients are generally under unstable cardiopulmonary conditions, most of whom require mechanical ventilation. Because saturated vapor is temperature dependent, it reduces under hypothermic conditions (e.g., to 36.6 mg/L at 33.5°C) (Sottiaux, 2006). However, currently, a humidifier setting for normothermic conditions is recommended, even during therapeutic hypothermia (Lellouche et al., 2006). Gas humidity of this level may be excessive for cooled patients, potentially causing significant water condensation and subsequent adverse events. Indeed, serious infectious complications, such as ventilator-associated pneumonia (VAP) are common during therapeutic hypothermia in children and adults (Todd et al., 2005; Hutchison et al., 2008; Clifton et al., 2011). Prevention of excessive humidification may improve the safety of cooling by reducing the incidence of VAP and other serious respiratory complications, and may increase the range of patients who have the benefit of cooling.
The aim of this study was to elucidate the incidence and independent variables of inappropriate Y-piece gas temperature and humidity in newborn infants, who are undergoing therapeutic hypothermia.
Methods
Methods are provided in detail in the Supplementary Data (Supplementary Data are available online at www.liebertpub.com/ther).
This study was conducted under the approval of the Ethics Committee of Kurume University School of Medicine (08069) with informed consent from substitute decision makers of the patients.
Study population
Between July 2011 and November 2014, 42 cumulative newborn infants (i.e., 24 patients were studied 42 times over different days) who were cooled to 33–34°C at two tertiary neonatal intensive care units in Kurume, Fukuoka, Japan, were studied (Table 1). Data collection from the same patient was repeated only after major changes in ventilator settings, such as changes in mean airway pressure >5 cmH2O and changes in ventilation modes, with an interval of at least 24 hours.
Values are shown as number (acumulative) or median (range) unless otherwise specified.
HFOV, high-frequency oscillatory ventilation; PTV, patient-triggered ventilation; SD, standard deviation; VAP, ventilator-associated pneumonia.
Ventilators, circuits, and humidifiers
Five ventilators were used according to the availability and the patient's condition. We used ventilator-fixed humidifiers of either a pass-over humidifier (MR 730; Fisher and Paykel, Auckland, New Zealand) or a counter-flow humidifier (Schumann et al., 2007) (Humicare 200; Gründler Medical, Freudenstadt, Germany) (Fig. 1 and Supplementary Table S1). Ventilator circuits were configured based on the manufacturer's recommendation, which were classified into those with short (≤10 cm) or long (>10 cm) nonheated extension tubes before the Y-piece (Fig. 1).
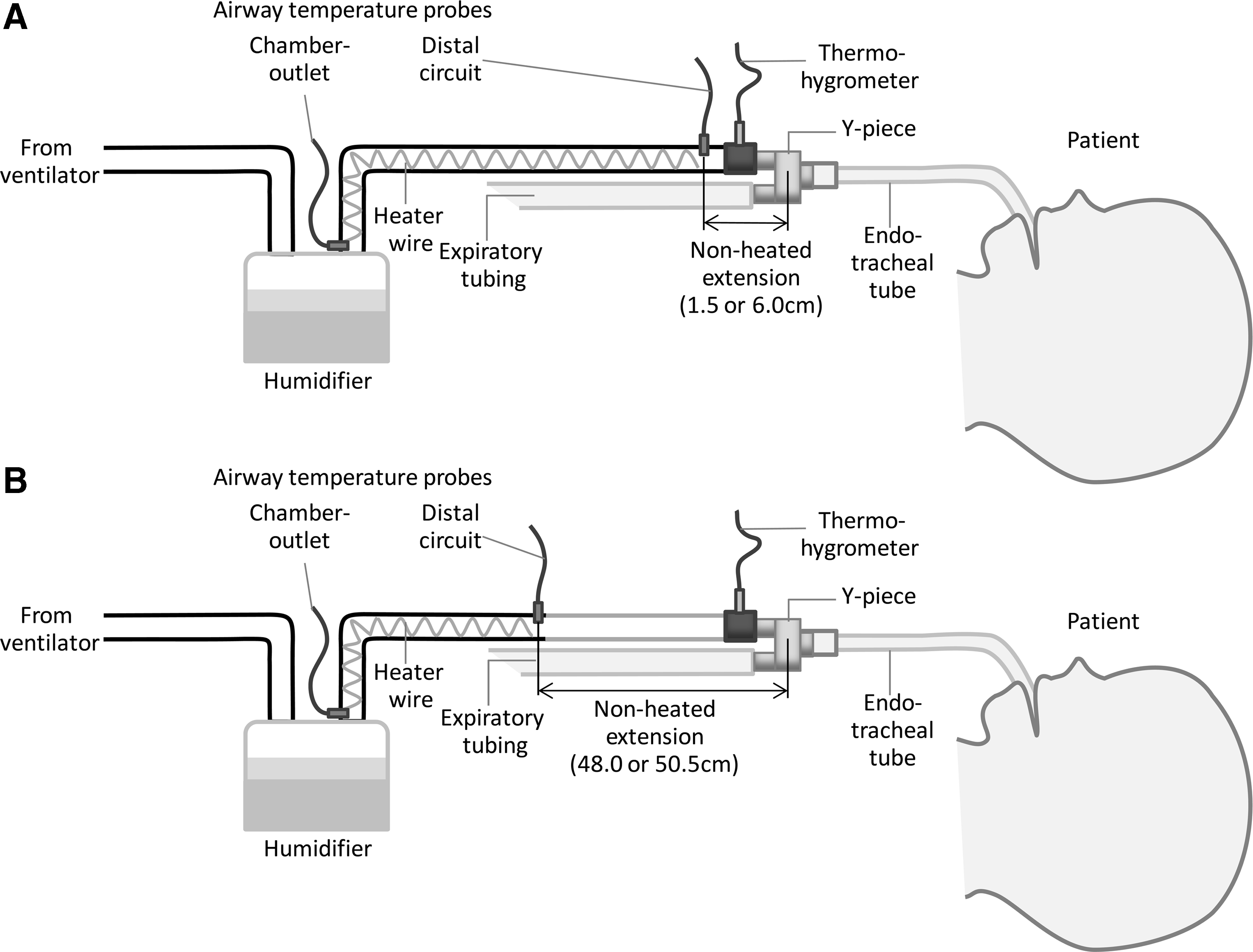
Configurations of humidifying systems and ventilator circuits. Humidifying system and ventilator circuit with short
Data collection
Gases were assessed using a main-stream thermohygrometer (Moiscope, Skynet, Tokyo, Japan) that was placed between the extension tube and the Y-piece (Fig. 1). Temperature values at the humidifying chamber outlet (“chamber outlet” temperature) and the distal end of the heated inspiratory circuit (“circuit” temperature) were provided by humidifying systems. The ambient and esophageal temperatures were also recorded simultaneously. Data were collected for three humidifier settings as follows: (1) 37-default (default setting under normothermia; chamber outlet, 37°C; circuit, 40°C), (2) 33.5-theoretical (theoretically adjusted setting for moderate hypothermia; chamber outlet, 33.5°C; circuit, 36.5°C), and (3) 33.5-adjusted (settings were adjusted to achieve a temperature of 36.5 ± 0.5°C and humidity of 36.6 ± 0.5 mg/L or the closest values at the Y-piece). Each variable was recorded three times approximately every 3 minutes after chamber outlet and circuit temperatures became stable. Patients’ characteristics, treatments, and adverse events were observed from the clinical records.
Statistical analysis
Values are mean (SD) unless otherwise stated. Data were first compared between groups defined by the ventilation mode, ventilator circuit, and humidifier, using the Student's t-test (significance assumed for p < 0.006 correcting for eight comparisons). Associations between the ambient temperature, esophageal temperature, and Y-piece gas humidity/temperature were assessed using the linear regression analysis. Inappropriate Y-piece temperature/humidity was defined as follows: high temperature >38.5°C (i.e., 36.5 plus 2.0°C), low temperature <34.5°C (i.e., 36.5 minus 2.0°C), high humidity >40.7 mg/L (saturated vapor at 35.5°C [i.e., 33.5 plus 2.0°C]), and low humidity <32.9 mg/L (saturated vapor at 31.5°C [i.e., 33.5 minus 2.0°C]). These thresholds were defined based on clinical recommendations that Y-piece temperature should be controlled to ±2°C from the target level (ISO, 2007). Independent variables of inappropriate Y-piece temperature/humidity were then assessed. Instead of repeating regression analyses over 12 combinations of data sets derived from four dependent variables and three humidifier settings, generalized estimating equations were used to evaluate the impact of each independent variable with adjustment for three humidifier settings (SPSS-21; IBM, New York, NY). Statistical significance for univariate analysis was assumed for p < 0.006 correcting for eight comparisons. Independent variables for multivariate analysis were assigned by findings from univariate analysis and clinical relevance of the model.
Results
Clinical characteristics of patients
Data were successfully obtained from all 42 neonates, who were 38.3 (2.0) weeks gestation at birth and 1.2 (1.0) days old at the time of study. High-frequency oscillatory ventilation (HFOV), counter-flow humidifiers, and long extension tubes were used in 8, 8, and 25 patients, respectively. The mean airway pressure and the fraction of inspired oxygen were 8.3 (3.6) cmH2O and 0.238 (0.059), respectively. The esophageal temperature at the commencement of the study was 33.4 (0.3)°C, which remained at similar levels throughout the data collection. No relationship was observed between the ambient temperature, esophageal temperature, and Y-piece gas humidity/temperature.
Y-piece temperature and humidity for each humidifier setting
Setting of 37-default
Y-piece temperature and humidity were 37.1 (2.4)°C and 39.2 (5.2) mg/L, respectively (Fig. 2). The Y-piece gas condition was similar between patient-triggered ventilation (PTV) and HFOV. Y-piece temperature and humidity were higher when counter-flow humidifiers (vs. pass-over humidifiers) and short extension tubes (vs. long extension tubes) were used (both p < 0.001).
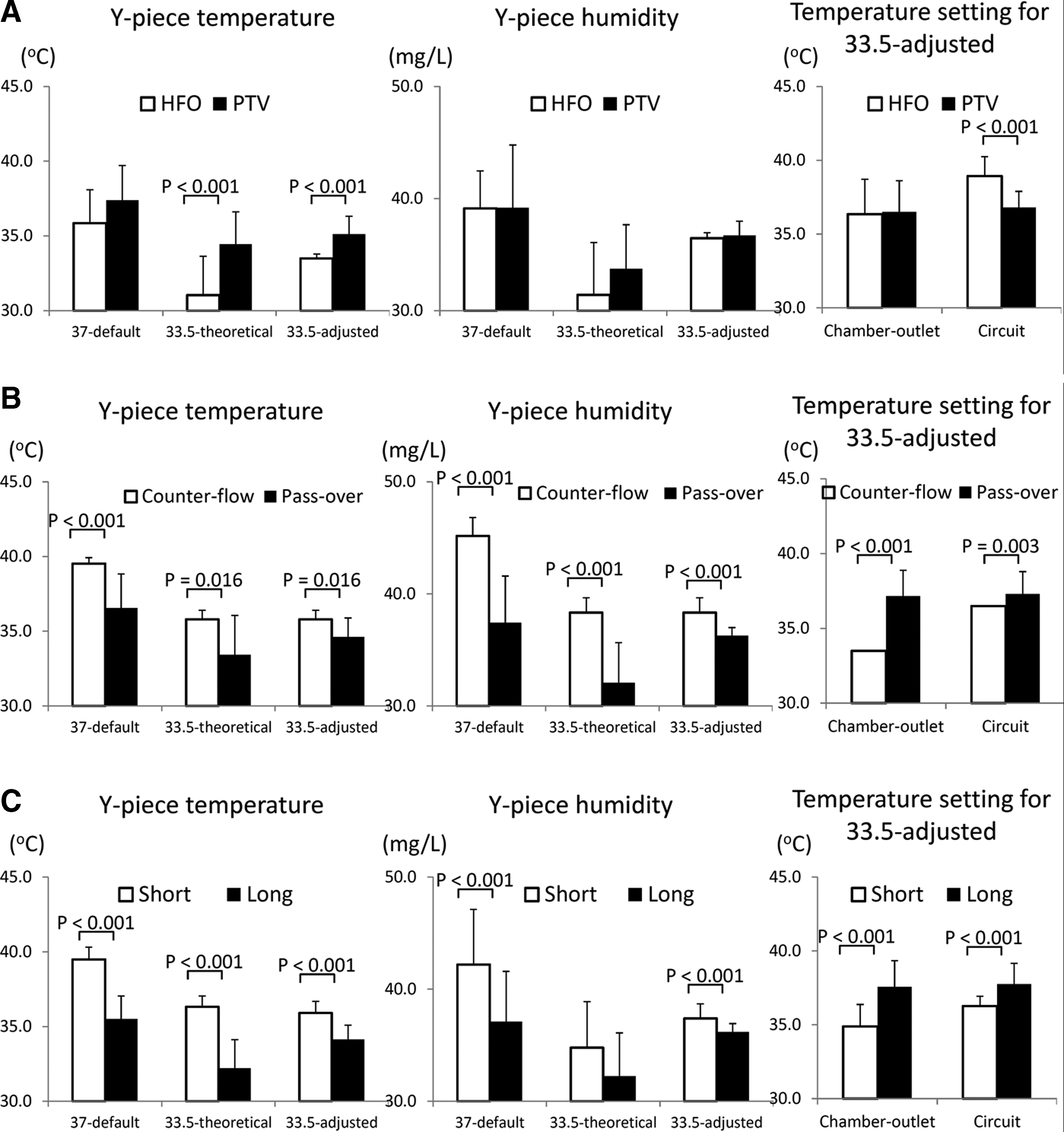
Effect of ventilation modes and humidifying systems on Y-piece gas conditions.
Setting of 33.5-theoretical
Y-piece temperature and humidity were 33.9 (2.5)°C and 33.3 (4.1) mg/L, respectively. Use of HFOV resulted in lower Y-piece temperature than PTV, whereas humidity was higher when counter-flow humidifiers were used (vs. pass-over humidifiers) (both p < 0.001). Gas temperature was lower when long extension tubes were used than when short extension tubes were used (p < 0.001).
Setting of 33.5-adjusted
Humidifier settings for the chamber outlet and the circuit temperature were 36.5 (2.1)°C and 37.2 (1.4)°C, respectively, leading to Y-piece temperature and humidity of 34.9 (1.2)°C and 36.7 (1.2) mg/L, respectively. The humidifier setting at the circuit probe was lower when ventilated with PTV than with HFOV; however, Y-piece temperature was higher with PTV than with HFOV (both p < 0.001). When counter-flow humidifiers were used, the 33.5-theoretical setting provided sufficient temperature and humidity required for the 33.5-adjusted setting without adjustment. Although humidifier settings were lower at the chamber outlet and circuit probes when counter-flow humidifiers were used than with pass-over humidifiers (p < 0.001 and p = 0.003, respectively), Y-piece humidity was higher with counter-flow humidifiers than with pass-over humidifiers (p < 0.001). Humidifier settings were higher with long extension tubes than with short extension tubes for the chamber outlet and circuit probes (both p < 0.001). However, subsequent Y-piece temperature and humidity were lower with long extension tubes than with short extension tubes (both p < 0.001).
Independent variables of inappropriate Y-piece temperature and humidity
High temperature >38.5°C
Univariate analysis showed that the incidence of excessively high temperature was greater with the use of counter-flow humidifiers (p = 0.004), short-extension tubes (p < 0.001), and the 37-default setting (vs. 33.5-theoretical and 33.5-adjusted, both p < 0.001) (Supplementary Table S2A). Multivariate analysis suggested that excessively high Y-piece gas temperature was associated with the use of short extension tubes and the 37-default setting (vs. 33.5-theoretical and 33.5-adjusted) (all p < 0.001).
Low temperature <34.5°C
Univariate analysis showed that the incidence of excessively low temperature was greater with the use of HFOV, pass-over humidifiers, long extension tubes, the 33.5-theoretical and 33.5-adjusted settings (vs. 37-default), and a higher mean airway pressure (all p < 0.001) (Supplementary Table S2B). Multivariate analysis showed that excessively low temperature was positively associated with the use of HFOV (p = 0.038), long extension tubes (p < 0.001), and the 33.5-theoretical and 33.5-adjusted settings (vs. 37-default, both p < 0.001).
High humidity >40.7 mg/L
Univariate analysis showed that observation of excessively high humidity was greater with the use of counter-flow humidifiers (p = 0.001) and the 37-default setting (vs. 33.5-theoretical and 33.5-adjusted, both p < 0.001) (Table 2A). Multivariate analysis showed that short extension tubes (p = 0.003), the 37-default setting (vs. 33.5-theoretical and 33.5-adjusted, both p < 0.001), and a higher constant flow (p < 0.001) were associated with a greater risk of excessively high humidity.
HFOV, high-frequency oscillatory ventilation; PTV, patient-triggered ventilation.
Low humidity <32.9 mg/L
Univariate analysis showed that the risk of excessively low humidity was greater with the use of pass-over humidifiers and the 33.5-theoretical setting (vs. 37-default) (both p < 0.001) (Table 2B). Multivariate analysis revealed that the risk of excessively low humidity was associated with the use of pass-over humidifiers and the 33.5-theoretical setting (vs. 37-default) (both p < 0.001).
Clinical adverse events
All of the patients survived to discharge. Two newborn infants developed septicemia during cooling, whose blood cultures at admission (i.e., before cooling) were positive (Table 1). A newborn infant experienced endotracheal tube obstruction, in whom extremely low humidity was confirmed with the 37-default and 33.5-theoretical settings when studied after reintubation.
Discussion
In our study, during therapeutic hypothermia, the use of a default humidifier setting for normothermia increased the risks for excessively high Y-piece gas temperature and humidity. The humidifier setting that was theoretically adjusted for body temperature was associated with an increased incidence of excessively low Y-piece gas temperature and humidity. In addition to humidifier settings, types of humidifying systems and inspiratory circuits and the constant flow of the ventilator were identified as important independent variables of inappropriate gas humidification. To deliver appropriately humidified gases to hypothermic patients, humidifier settings need to be adjusted with the feedback from Y-piece hygrometer readings, or, alternatively, a counter-flow humidifier can be used with a theoretically body-temperature-adjusted setting.
Problems of the default humidifier setting for normothermia during cooling
International guidelines of resuscitation currently recommend cooling severely asphyxiated newborn infants and adult patients after cardiac arrest (Peberdy et al., 2010; Perlman et al., 2010). This has resulted in an increasing number of patients undergoing therapeutic hypothermia (Azzopardi et al., 2012; Nelson et al., 2012; Dankiewicz et al., 2014; Iwata et al., 2014). Although the safety and efficacy of whole-body cooling to 33.5°C for 72 hours have been established in newborn infants (Jacobs et al., 2013), therapeutic hypothermia only has a narrow margin of benefit in child and adult patients due, in part, to high mortality associated with serious systemic and respiratory complications (Hypothermia After Cardiac Arrest Study Group, 2002; Todd et al., 2005; Hutchison et al., 2008; Clifton et al., 2011). In our study, we showed that the currently recommended humidifier setting led to a considerable incidence of excessive heating (35.7%) and humidification (31.0%). Current humidifying systems generally provide only modest humidity as opposed to the ideal level (Pelosi et al., 2007; Al Ashry and Modrykamien, 2014). Therefore, we rarely encounter excessive humidity during ventilation. However, saturated vapor differs by 7.3 mg/L between 33.5°C and 37.0°C. When a hypothermic patient of 3.5 kg is ventilated using the 37-default setting, 14.7 mL of water is delivered to the airway per day, assuming that the tidal volume is 8 mL/kg and the respiratory rate is 50 breaths/min. Unlike isotonic fluids, distilled water of this volume may cause airway edema, bronchial spasms, and mucosal dysfunction (Williams et al., 1996; Williams, 1998; Sottiaux, 2006; Pillow et al., 2009). Improved humidification of respiratory gases may significantly ameliorate respiratory complications of patients who undergo therapeutic hypothermia.
Pitfalls of the theoretical body temperature-adjusted humidifier setting
In our study, use of the 33.5-theoretical setting resulted in a considerable incidence of excessively low temperature (54.8%) and humidity (45.2%). This finding might be explained by the previously mentioned trend of currently available humidifying systems, which are generally under powered (Pelosi et al., 2007; Al Ashry and Modrykamien, 2014). The use of long extension tubes may further reduce Y-piece temperature and humidity (Todd et al., 2001). Long extension tubes are used to minimize the effect of a relatively high ambient temperature within closed incubators. However, because even newborn infants are usually cooled in an open incubator (Gluckman et al., 2005; Azzopardi et al., 2009; Iwata et al., 2012), long extension tubes might merely be harmful. In addition, significant changes in the performance of pass-over humidifiers have been reported when the temperature difference of gases between the inlet and outlet of the humidifying chamber becomes small (Carter et al., 2002; Lellouche et al., 2004). When the chamber inlet temperature is already close to the target level (e.g., 37°C), the humidifier turns off its heater, where only the target temperature, but not the target humidity, is achieved at the chamber outlet. Such a phenomenon may also be yielded by a lowered target gas temperature at the chamber outlet, as with the 33.5-theoretical setting.
Current solutions to optimize humidity of respiratory gases under hypothermia
Our data suggested that the counter-flow humidifier is likely to provide perfect temperature/humidity control during cooling. However, considering the relatively more expensive price of counter-flow humidifiers, alternative solutions are necessary. In this study, when the humidifier setting was adjusted by obtaining feedback from Y-piece gas monitoring, excessively high and low humidification were totally eliminated. Consistent to previous findings in normothermic patients (Pelosi et al., 2007; Chikata et al., 2009), Y-piece temperature/humidity is dependent on ventilation mode and constant flow of the ventilator even in cooled patients. Further studies are required to specify independent variables of inappropriate humidification.
Limitations
Our study population is too small to determine all of the problems and their solutions. The pass-over humidifier that was used in our study (MR 730) has since been replaced by a new fully automated model (MR 850), which does not allow manual adjustment of the chamber outlet and circuit temperatures, leading to difficulty in avoiding excessively high humidity in hypothermic patients. We assumed a temperature reduction of respiratory gasses within the endotracheal tube as ∼3°C regardless of the target Y-piece temperature, which might be different under cooling. We defined an “inappropriate Y-piece temperature/humidity” based on the statement by the International Organization for Standardization (ISO, 2007), which might be different from the actual threshold humidity levels associated with clinical adverse events.
Conclusions
Neither the default setting for normothermia nor the theoretically adjusted setting for hypothermia provides optimal Y-piece temperature and humidity during therapeutic hypothermia. To prevent inappropriate humidification, temperature and humidity of respiratory gases need to be monitored and adjusted. Alternatively, a counter-flow humidifier might be used with a theoretically adjusted setting. Independent variables that are associated with inappropriate Y-piece temperature and humidity, such as the use of long-extension tubes and relatively high constant flow of ventilators, should be avoided. Future studies need to assess whether a new regimen with optimal Y-piece temperature and humidity control reduces serious respiratory complications associated with therapeutic hypothermia in a wide age range of patients. Finally, an additional mode for hypothermic patients needs to be urgently developed for fully automated humidifiers.
Footnotes
Acknowledgments
The authors thank Profs. Toyojiro Matsuishi and Masanori Tamura for their useful advice and Drs. Hiroki Saitsu, Mitsuaki Unno, and Akiko Hirose, and Mr. Ryouji Kijima, Mr. Osamu Yamaga, and Mr. Shintaro Tomonaga, and Ms. Chiho Yoshii for their assistance in data collection. This work was supported by the Japanese Ministry of Health, Labour, and Welfare (H27-001, special research in perinatal medicine). Dr. O. Iwata is also funded by the Japan Science and Technology Agency and the Ministry of Education, Culture, Sports, Science, and Technology (Grant-in-Aid for Scientific Research B01-24119004, Constructive Developmental Science, Innovative Areas). Dr. S. Iwata is funded by the Japan Science and Technology Agency and the Ministry of Education, Culture, Sports, Science, and Technology (Grant-in-Aid for Scientific Research C24591533).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.