
Abstract
Comatose patients after cardiac arrest should receive active targeted temperature management (TTM), with a goal core temperature of 32–36°C for at least 24 hours. Small variations in brain temperature may confer or mitigate a substantial degree of neuroprotection, which may be lost at temperatures near 37°C. The purpose of this study was to define the relationship between brain and core temperature after cardiac arrest through direct, simultaneous measurement of both. We placed intracranial monitors in a series of consecutive patients hospitalized for cardiac arrest at a single tertiary care facility within 12 hours of return of spontaneous circulation to guide postcardiac arrest care. We compared the absolute difference between brain and core (esophageal or rectal) temperature measurements every hour for the duration of intracranial monitoring and tested for a lag between brain and core temperature using the average square difference method. Overall, 11 patients underwent simultaneous brain and core temperature monitoring for a total of 906 hours of data (Median 95; IQR: 15–118 hours per subject). On average, brain temperature was 0.34C° (95% confidence interval [CI] 0.31–0.37) higher than core temperature. In 7% of observations, brain temperature exceeded the measured core temperature ≥1°C. Brain temperature lagged behind core temperature by 0.45 hours (95% CI = −0.27–1.27 hours). Brain temperature averages 0.34°C higher than core temperature after cardiac arrest, and is more than 1°C higher than core temperature 7% of the time. This phenomenon must be considered when carrying out TTM to a goal core temperature of <36°C.
Introduction
C
Preclinical evidence suggests that reductions of brain temperature by 1°C from 37°C to 36°C may be neuroprotective (Jackson et al., 2015), and that these benefits are not achieved with active normothermia (37°C) (Logue et al., 2007). These data raise concern that the neuroprotective benefits of TTM may be reduced when targeting a core temperature of 36°C, if the unmeasured brain temperature were significantly higher. The purpose of this study, therefore, was to quantify the relationship between brain and core temperature in comatose postcardiac arrest patients through direct, simultaneous measurement of both. We hypothesized that core temperature would substantially underestimate brain temperature across a range of core temperatures. Secondarily, we hypothesized that brain temperature would lag behind core temperature during periods of dynamic temperature change.
Materials and Methods
The University of Pittsburgh Institutional Review Board approved this study. In brief, we identified a series of patients treated after cardiac arrest at a single tertiary care center between 2013 and 2015 who had intracranial monitors placed within 12 hours of ROSC to guide clinical care. We measured baseline severity of postcardiac arrest illness using a previously validated illness severity scale (Coppler et al., 2015). We excluded subjects who had cardiac arrest or had brain monitors placed because of severe trauma or a primary neurological process such as catastrophic cerebrovascular accident. Our neuromonitoring package included placement of a right frontal intracranial access bolt (Licox® IMC Bolt Fitting, Integra LifeSciences; or QFlow 500™ Titanium Bolt, Hemedex, Inc.), through which intracranial pressure, temperature, and tissue oxygen probes were placed in the subcortical white matter. We measure intracranial temperature with either a Licox (Integra LifeSciences) or Raumedic® Neurovent PTO (Raumedic) catheter. Core temperature was measured by either a rectal or esophageal temperature probe. We performed TTM using a CoolGard 3000© endovascular catheter (Alsius Corporation) or Arctic Sun© (Mediance, Bard Medical) surface cooling pads, and targeted a core temperature of 33°C for 24 hours followed by rewarming at 0.25°C/h to a goal of 37°C, which we maintained for at least 5 days after ROSC.
Statistics
We used descriptive statistics to summarize population characteristics, then compared brain and core temperature measurements every hour for the duration of intracranial monitoring within each patient and for the overall population. We tested for a lag between brain and core temperature using the average square difference method. The sum of the squared difference in temperature between each hourly measurement divided by the number of measurements was computed while varying the lag between the two temperature signals between −3 and +3 hours. The minimum of the seven resulting values corresponded to the optimal lag between the two signals for each patient. Computations were programmed in Matlab R2014a (The Mathworks). We calculated the mean lag for the 11 included patients and bootstrapped its 95% confidence interval using the BCa method with 10,000 bootstrap samples in SPSS 23 (IBM).
Results
Overall, 11 patients underwent simultaneous brain and core temperature monitoring for a total of 906 hours (Median 95; IQR: 15–118 hours per subject). The majority of subjects had an asystolic initial rhythm and presented with severe brain injury (Table 1). Esophageal core temperature was monitored in 64% of patients and most subjects (73%) were cooled using an endovascular device. Median time from arrival to placement of intracranial monitoring was 7 hours (IQR: 5.5–8.5 hours).
PEA, pulseless electrical activity; VT/VF, ventricular tachycardia/ventricular fibrillation.
On average, brain temperature exceeded core temperature by 0.34°C (95% confidence interval [CI]: 0.31–0.37
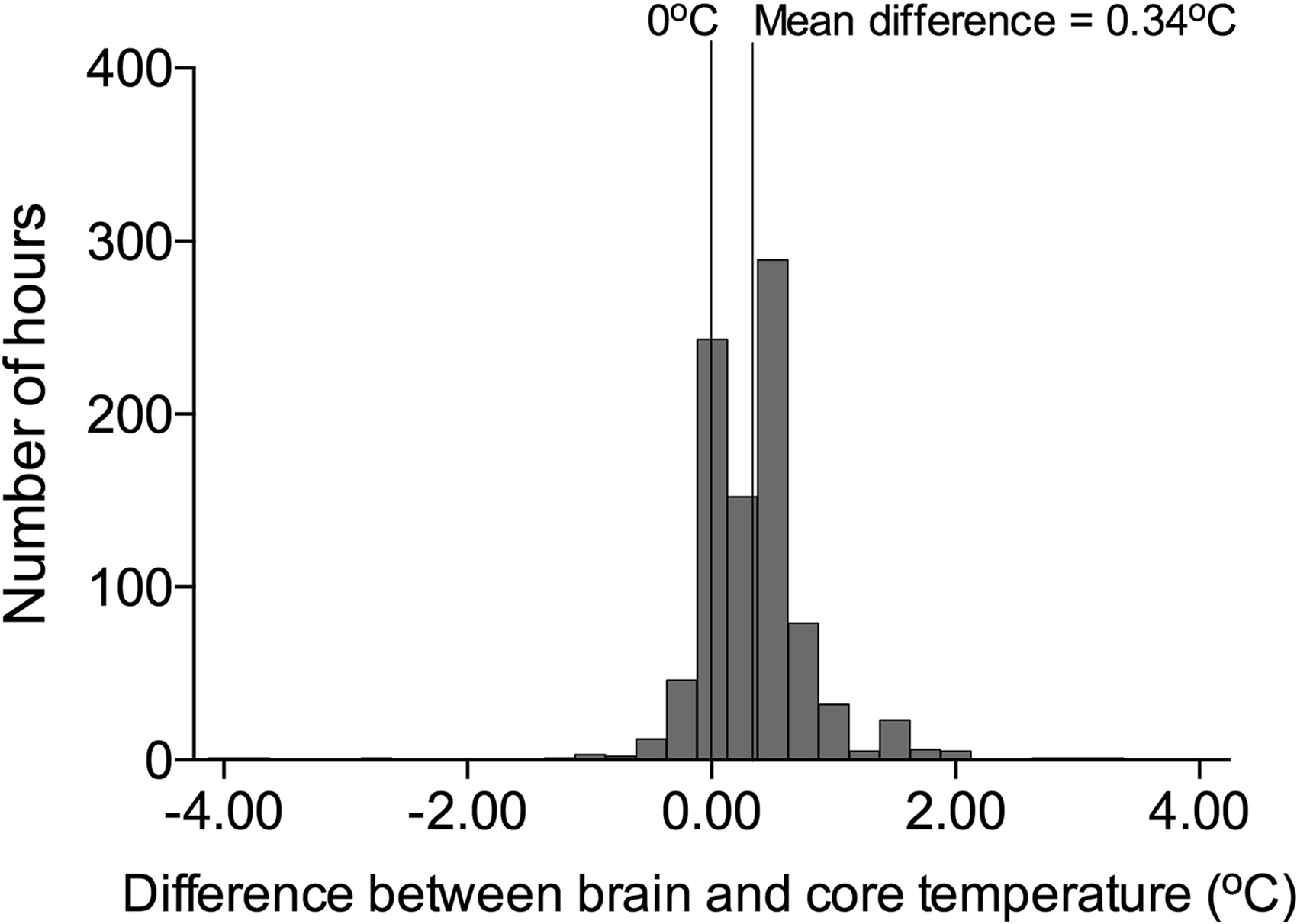
Histogram of total hours of observation and differences between brain and core temperature.
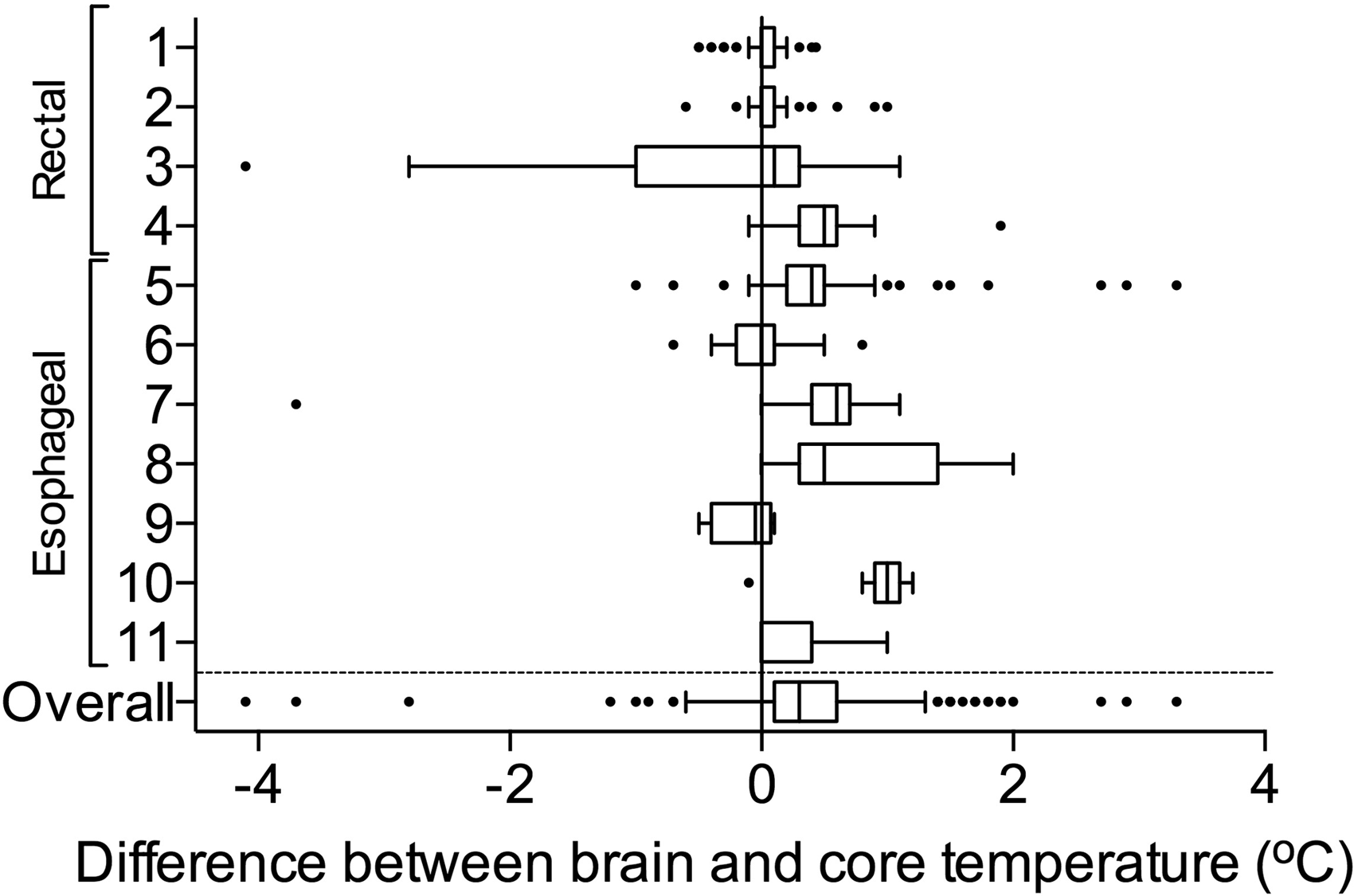
Box and whisker plot of individual patient data and differences between brain and core temperature.
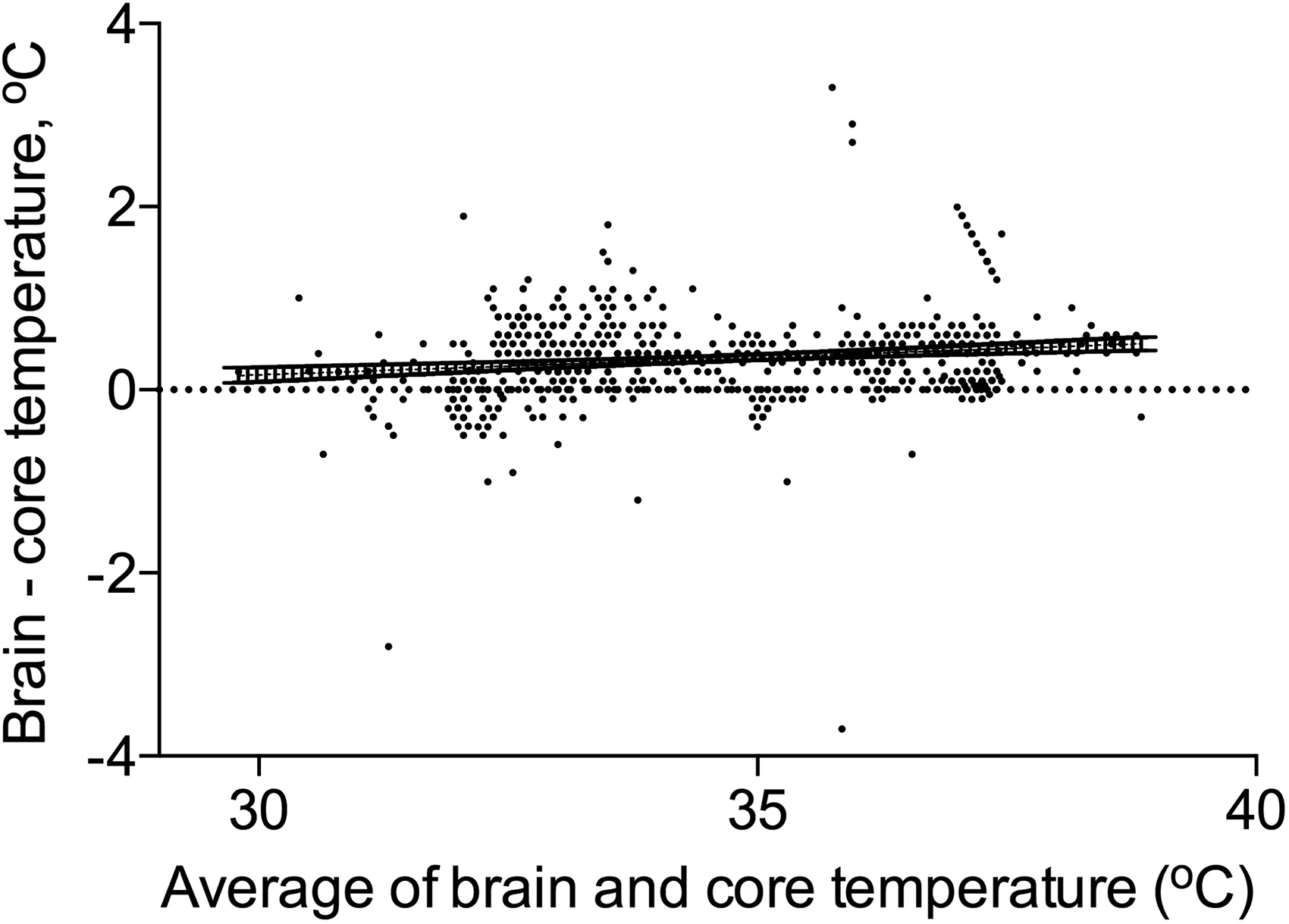
Bland–Altman plot of absolute difference in core and brain temperature and relative core temperature.
Discussion
To our knowledge, this is the first report to compare brain and core temperature in human cardiac arrest patients. We found that during active temperature management, core temperature consistently underestimated brain temperature, often by a substantial degree. This phenomenon has also been observed after brain trauma and stroke (Karaszewski et al., 2009; Childs and Lunn, 2013). Since the landmark TTM trial showing equivalent effects of treatment at 33°C versus 36°C on patient outcomes (Nielsen et al., 2013), clinical practice has shifted toward targeting 36°C in comatose survivors of cardiac arrest (Callaway et al., 2015; Leary et al., 2015; Deye et al., 2016). The TTM trial demonstrated equivalent patient outcomes at a population level, yet even within the context of this trial the 95% error bars in the 36°C cohort crossed 37°C (Nielsen et al., 2013). Clinical practice outside of the context of a robust trial may be less precise, and patients treated with a target core temperature of 36°C are at greater risk of exceeding 37°C than patients treated with a lower target core temperature (Rittenberger et al., 2015). Given the discrepancy we demonstrate between brain and core temperature, our results highlight the importance of vigilant prevention of even small rises in core temperature above 36°C to prevent unintended cerebral normothermia or fever during TTM.
Our work has several limitations. We present single center observational data including some of the most severe brain-injured cardiac arrest patients. The generalizability of our findings to less severe brain-injured postcardiac arrest patients is unknown. It may be that in a more mildly injured cohort, brain metabolism is less severely impaired and there is actually more cerebral thermogenesis, or that homeostasis is better preserved and there is less of a difference. In addition, the site of core temperature measurement and the device used for TTM were not consistent across patients. This variety likely reflects current clinical practice among cardiac arrest centers (Coppler et al. unpublished data 2016). Finally, with regard to detection of a lag between brain and core temperature, hourly measurements may be too infrequent and relatively insensitive to identify a lag that may exist on the order of minutes. However, we feel that such a brief lag, if it exists, is unlikely to be clinically relevant.
Conclusion
Brain temperature exceeds core temperature in comatose patients after cardiac arrest, sometimes by more than 1°C. Small elevations in core temperature above 36°C may risk brain normothermia and reduce the neuroprotective effect of TTM.
Footnotes
Acknowledgments
The Pittsburgh Post-Cardiac Arrest Service researchers are Jon C. Rittenberger, MD, MS; Clifton W. Callaway, MD, PhD; Francis X. Guyette, MD, MPH; Ankur A. Doshi, MD; Cameron Dezfulian, MD; Jonathan Elmer, MD, MS; Bradley J. Molyneaux, MD, PhD; and Lillian Emlet, MD, MS. Source of funding: Dr. Elmer's research time is supported by the NHLBI 5K12HL109068; Dr. Dezfulian's research time is supported by the NINDS KO8NS069817; and Dr. Elmer's research time is supported by the NHLBI 5K12HL109068.
Author Disclosure Statement
No competing financial interests exist.