
Abstract
A number of observational studies have evaluated the association between arterial oxygen tensions and outcome after cardiac arrest with variable results. The objective of this study is to determine the association between arterial oxygen tension and neurological outcome after cardiac arrest. A retrospective cohort analysis was performed using the Penn Alliance for Therapeutic Hypothermia registry. Adult patients who experienced return of spontaneous circulation after in-hospital or out-of-hospital cardiac arrest (OHCA) and had a partial pressure of arterial oxygen (PaO2) recorded within 48 hours were included. Our primary exposure of interest was PaO2. Hyperoxemia was defined as PaO2 > 300 mmHg, hypoxemia as PaO2 < 60 mmHg, and optimal oxygenation as PaO2 60–300 mmHg. The primary outcome was neurological function at hospital discharge among survivors, as described by the cerebral performance category (CPC) score, dichotomized into “favorable” (CPCs 1–2) and “unfavorable” (CPCs 3–5). Secondary outcomes included in-hospital mortality. A total of 544 patients from 13 institutions were included. Average age was 61 years, 56% were male, and 51% were white. A total of 64% experienced OHCA, 81% of arrests were witnessed, and pulseless electrical activity was the most common initial rhythm (40%). More than 72% of the patients had cardiac etiology for their arrests, and 55% underwent targeted temperature management. A total of 38% of patients survived to hospital discharge. There was no significant association between PaO2 at any time interval and neurological outcome at hospital discharge. Hyperoxemia at 12 hours after cardiac arrest was associated with decreased odds of survival (OR 0.17 [0.03–0.89], p = 0.032). There was no significant association between arterial oxygen tension measured within the first 48 hours after cardiac arrest and neurological outcome.
Introduction
N
The relationship between arterial oxygen tension and outcome after cardiac arrest is complex. Cardiac arrest itself is an oxygen supply-dependent state, where the core tenet of cardiopulmonary resuscitation is to maximize oxygen delivery to ischemic tissues (Rosendorff, 2006; Henlin et al., 2014). Return of spontaneous circulation results in markedly increased pulmonary blood flow, rapid reoxygenation of ischemic tissue, and a burst in production of reactive oxygen species. This is the so-called oxygen paradox associated with ischemia and reperfusion.
A number of preclinical studies have demonstrated that reduction in the fraction of inspired oxygen (FiO2) after cardiac arrest decreased neuronal injury and oxidative stress (Liu et al., 1998; Balan et al., 2006; Vereczki et al., 2006; Brücken et al., 2010; Angelos et al., 2011). Clinical studies, however, have demonstrated mixed results. In a retrospective analysis of a large critical care database, Kilgannon et al. (2010) found that arterial hyperoxemia (defined as partial pressure of arterial oxygen [PaO2] ≥300 mmHg) was associated with increased in-hospital mortality and poor functional status. A subsequent analysis by the same group demonstrated that this effect was dose dependent, that is, PaO2 was linearly associated with in-hospital mortality (Kilgannon et al., 2011). Subsequent observational studies have yielded conflicting results: some have demonstrated an association between arterial oxygen tension and mortality after cardiac arrest, whereas other studies have found no relation (Bellomo et al., 2011; Ferguson et al., 2012; Bennett et al., 2013; Janz et al., 2013; Vaahersalo et al., 2014). Few other human studies have examined the relationship between postarrest arterial oxygen tension and neurological outcome (Janz et al., 2013; Vaahersalo et al., 2014).
Many experts have advocated for PCAS “bundles” to optimize outcomes, which include therapies such as targeted temperature management (TTM), early percutaneous coronary interventions, hemodynamic optimization, neurological monitoring and seizure control, low tidal volume ventilation, and meticulous management of electrolytes including glucose and potassium (Neumar et al., 2008; D. Gaieski et al., 2009; D. F. Gaieski et al., 2009; Donnino et al., 2011). Whether stringent control of arterial oxygen tension should be included in postarrest bundles is less clear, although international guidelines recommend targeting an oxygen saturation of ≥94% based on the best available evidence (Peberdy et al., 2010).
Because existing data on this topic are mixed and few studies have assessed neurological impairment as an outcome, we aimed to test the hypothesis that both supranormal and low arterial oxygen tensions are associated with poor neurological outcome and increased mortality after cardiac arrest.
Materials and Methods
Study design and setting
A retrospective cohort analysis was performed using data from the Penn Alliance for Therapeutic Hypothermia (PATH) registry, a web-based, multicenter database of IHCA and OHCA hosted by the University of Pennsylvania. The PATH database includes cardiac arrest data of patients from the prehospital, emergency department, and in-hospital settings, with a focus on postarrest care (Leary et al., 2013). This study was approved with waiver of informed consent by the Institutional Review Board of the University of Pennsylvania.
Patient selection
Adults enrolled in the PATH registry who were successfully resuscitated after cardiac arrest and had PaO2 values recorded were included. Patients who did not survive initial resuscitation were excluded.
Data abstraction
The following demographic and cardiac arrest characteristics were abstracted from PATH: gender, race, age, location of arrest event, whether the arrest event was witnessed, bystander CPR, initial pulseless cardiac rhythm, etiology of arrest, and use of TTM. PaO2 values at 1, 6, 12, 24, and 48 hours were also abstracted, as well as neurological status (as measured by a CPC score) and survival at hospital discharge.
Definitions and outcomes
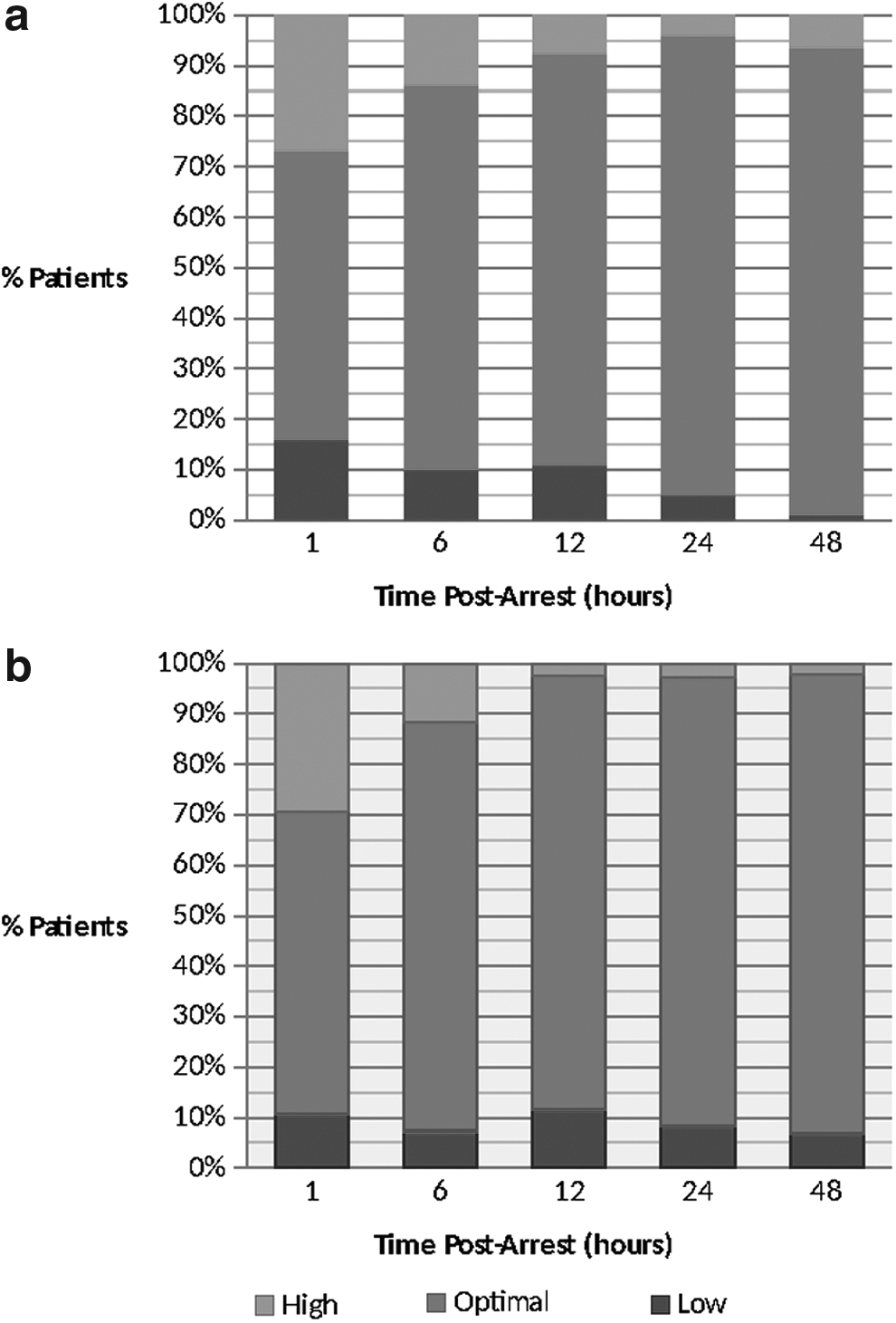
Our primary exposure of interest was arterial oxygen tension at each of the following time intervals after cardiac arrest: 1, 6, 12, 24, and 48 hours. Based on prior studies, high PaO2 (hyperoxemia) was defined as PaO2 > 300 mmHg, low PaO2 (hypoxemia) was defined as PaO2 < 60 mmHg, and optimal PaO2 (normoxia) was defined as PaO2 between 60 and 300 mmHg (Kilgannon et al., 2010, 2011). The threshold for inclusion of a PaO2 value was ±2 hours. The primary outcome was neurological function at hospital discharge among survivors, as described by the cerebral performance category (CPC) score. Neurological outcome was dichotomized into “favorable” (CPCs 1–2) and “unfavorable” (CPCs 3–5). The secondary outcome was survival to hospital discharge.
Statistical analysis
Continuous data are presented as means with standard deviations or as medians with interquartile ranges (IQR). Categorical data were reported as proportions with 95% confidence intervals. Data elements were compared using two-tailed chi-squared tests and Fisher's exact test for categorical variables, and t-tests for continuous variables. Identified potential confounders and effect modifiers were analyzed in a multivariate model. The demographic risk factors and pre-existing conditions were considered in multivariate logistic regressions. Analysis was conducted using STATA 12.0 (College Station, TX).
Results
Patient and cardiac arrest characteristics
A total of 544 adult patients from 13 institutions were included (Table 1). Average age was 61 ± 17 years, 56% were male, and 51% of patients were white. A total of 64% of patients experienced OHCA, and 81% were witnessed. The most common initial cardiac rhythm was pulseless electrical activity at 40%. More than 72% of the patients had cardiac etiology for their arrests, and 55% underwent TTM. A total of 38% of patients survived to hospital discharge; 87% of survivors had a CPC of 1 or 2. Patients who had a favorable neurological outcome were more likely to be male, have a witnessed cardiac arrest, have their initial cardiac rhythm be ventricular tachycardia or fibrillation, and have a cardiac etiology of the arrest.
CAD, coronary artery disease; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; CPC, cerebral performance category; IQR, interquartile range; PEA, pulseless electrical activity; SD, standard deviation; TTM, targeted temperature management; VT/VF, ventricular tachycardia/ventricular fibrillation.
Oxygenation data
Median PaO2 values at 1, 6, 12, 24, and 48 hours were 89 (IQR: 80, 313), 133 (IQR: 87, 211), 121 (IQR: 79, 177), 108 (IQR: 81, 155), and 102 (IQR: 81, 137) mmHg, respectively. Approximately 60% of patients had a PaO2 in the normal range (between 60 and 300 mmHg) within 1 hour after cardiac arrest, and more than 80% had a PaO2 in the normal range by 12 hours after arrest. This was not statistically different between patients with favorable or unfavorable neurological outcome (Fig. 1a, b).
Arterial oxygen tension and neurological outcome
With regard to the primary outcome, there was no significant association between PaO2 at any time interval and neurological outcome at hospital discharge (Table 2). Using a multivariate model that included age, gender, witnessed arrest, and initial pulseless rhythm, no association between PaO2 and neurological outcome was found at any time interval (Table 3). In addition, no association between PaO2 and neurological outcome was found when patients were stratified according to whether they received TTM (Table 4).
CPC, cerebral performance category, IQR, interquartile range; mmHg, millimeters of mercury; PaO2, partial pressure of arterial oxygen.
The multivariate model included the following: age, gender, witnessed arrest, and initial pulseless rhythm.
CI, confidence intervals; CPC, cerebral performance category; OR, odds ratio; ROSC, return of spontaneous circulation.
The multivariate model included the following: age, gender, witnessed arrest, and initial pulseless rhythm.
CPC, cerebral performance category.
Arterial oxygen tension and survival
In a multivariate model that included gender, age, witnessed arrest, and initial pulseless rhythm, no association between PaO2 and survival was found at any time interval except for 12 hours after arrest. Hyperoxemia at 12 hours after cardiac arrest was associated with decreased odds of survival (OR 0.17 [0.03–0.89], p = 0.032; Table 3).
Discussion
We found no significant association between arterial oxygen tension within 48 hours after cardiac arrest and neurological outcome at hospital discharge among survivors with, in general, PaO2 values in the normal range. We did find an association between hyperoxemia at 12 hours and lower odds of survival to hospital discharge, although the impact of a single recorded episode of hyperoxemia is unclear. This is one of the largest studies to have examined the association between arterial oxygen tension and neurological outcome in a population of patients who suffered either OHCA or IHCA and received TTM. Several previous studies have shown no relationship between PaO2 and outcome, whereas others have demonstrated poor outcome associated with both low and supranormal arterial oxygen tensions (Kilgannon et al., 2010, 2011; Bellomo et al., 2011; Bennett et al., 2013; Janz et al., 2013; Vaahersalo et al., 2014).
An observational study by Kilgannon et al. (2010) of 6326 critically ill patients found that arterial hyperoxemia (defined as PaO2 ≥ 300 mmHg) was associated with an 18% absolute increase in hospital mortality when compared with patients who were maintained within the normal range (PaO2 60–300 mmHg). There was also a 9% decrease in the proportion of patients achieving functional independence in the hyperoxemia group when compared with those whose PaO2 remained in the normal range. Their study differs from ours in a number of ways. First, Kilgannon et al.'s study used a large, multi-institutional critical care database, which included postarrest patients, but was not exclusively designed for this population. The authors did not assess which proportion of patients, if any, received TTM. Second, the authors only examined arterial oxygen tensions for the first 24 hours after cardiac arrest, and the time from arrest to measurement of the PaO2 was not collected. Third, the median postarrest PaO2 was substantially higher in this study (231 mmHg) than our data (89–133 mmHg at various time intervals). Data for the study by Kilgannon et al. were collected from 2001 to 2005, before the American Heart Association and other organizations incorporated reduction of postarrest FiO2 into their guidelines. This significant baseline difference in median PaO2 between this study and ours might have contributed to the disparate findings reported.
The same group subsequently demonstrated that the relationship between PaO2 and both in-hospital mortality and functional independence was linear, implying dose dependence (Kilgannon et al., 2011). More specifically, they found that each 100 mmHg increase in PaO2 was associated with a 24% increase in risk of death. A key limitation of this study is that the authors define their exposure based on the highest measured PaO2 value within the first 24 hours after arrest. The true “dose” would be more accurately expressed as a time-dependent variable, or, as in this study, by looking at multiple measurements over many hours. It is difficult to know whether a single, markedly elevated PaO2 actually represents a high cumulative exposure to supranormal oxygen tensions. However, in our study, hyperoxemia was associated with decreased survival at a single time point, suggesting that isolated or brief episodes of hyperoxemia may be clinically important during times of cellular recovery.
A smaller study examined the relationship between arterial hyperoxemia and outcome in 170 patients who were treated with TTM after cardiac arrest (Janz et al., 2013). They found that survivors had a significantly lower maximum PaO2 than nonsurvivors (198 mmHg vs. 254 mmHg). In a multivariate analysis, hyperoxemia, which was defined as the highest measured PaO2 within the first 24 hours, was associated with increased in-hospital mortality and unfavorable neurological outcome. In contrast, Vaahersalo et al. (2014) found no association between hyperoxemia and long-term (12 months) neurological outcome after cardiac arrest in 409 patients. The mean PaO2 of 113 mmHg in this study was comparable with PaO2 values in our study. It is possible that patients in our study, as well those in the study by Vaahersalo et al., did not have sufficient exposure to hyperoxia to affect neurological outcome.
It is also possible that TTM modifies the effect of hyperoxemia on neurological outcome. In the study by Vaahersalo et al., the majority of patients with favorable outcome (87%) received TTM. Similarly, in our study, the majority of patients (55%) received TTM. The effect of TTM on neurological outcome after cardiac arrest has been well documented, but its exact mechanisms are unknown (Bernard et al., 2002; Hypothermia after Cardiac Arrest Investigators, 2002; Nielsen et al., 2013). One feature of the PCAS is widespread circulation of reactive oxygen species, leading to tissue injury and inflammation, which is thought to be exacerbated by supraphysiological arterial oxygen tensions (Sakoh and Gjedde, 2003; Stub et al., 2011). Two studies using animal models for cardiac arrest demonstrated that a delivery of an FiO2 of 21% compared with 100% after arrest resulted in less oxidative stress and more favorable neurological outcome (Liu et al., 1998; Vereczki et al., 2006). In swine, it was demonstrated that titrating oxygen to a saturation of 94–96% resulted in improved neurological deficit scores and fewer injured neurons in the CA-1 hippocampal region when compared with receipt of 100% oxygen (Balan et al., 2006). It has been demonstrated that induced hypothermia decreases the quantity of reactive oxygen species in several models of neurological injury (Globus, Alonso, et al. 1995; Globus, Busto, et al. 1995; Weng and Sun, 2012). It remains to be proven whether TTM attenuates oxidative stress and related neurological injury after cardiac arrest, or whether exposure to hyperoxia modifies this interaction.
Limitations
The PATH database is robust and contains a geographically and clinically diverse population of more than 500 patients at 13 institutions. Limited data were available, however, about baseline patient comorbidities and long-term outcomes. Because ABGs were collected at the discretion of the treating clinicians, there may have been episodes of hyperoxemia or hypoxemia that were not captured. As mentioned, a significant number of missing PaO2 values existed, especially for later time points. We suspect that many of these missing values resulted from either changes in aggressiveness of treatment, withdrawal of life-sustaining treatment, or clinical improvement, but missingness certainly may have impacted our results. In addition, this study was retrospective in nature, so no causal inferences can be made; the retrospective nature makes it possible that time points were not entered accurately. We did not account for repeated measures, which could affect the interpretation of our results. Furthermore, it is possible that our study was not powered to detect a difference in neurological outcome that might be clinically important or detectable in a larger sample. Finally, one of the strengths of this study is also a potential weakness: the majority of patients had normal oxygen tensions at all time points. This may have affected the likelihood of finding an association between hyperoxemia and neurological outcomes because of the paucity of hyperoxemic values.
Conclusion
There was no significant association between arterial oxygen tension and neurological outcome within the first 48 hours after cardiac arrest among survivors receiving, in general, normoxemia. These data, taken with other observational studies, provide an impetus for future prospective trials to address the relationship between oxygenation goals, neurological outcomes, and mortality in this unique population.
Footnotes
Author Disclosure Statement
No competing financial interests exist.