
Abstract
Perinatal hypoxic ischemic encephalopathy (HIE) can lead to severe neurodevelopmental outcome and death. Therapeutic hypothermia is neuroprotective for infants with moderate-to-severe HIE. However, therapeutic hypothermia is only offered at high-level regional neonatal intensive care units (NICUs), necessitating the need to transport sick infants to referral centers. The goal of this study was to evaluate whether active cooling on transport is more effective than passive cooling in achieving temperatures in the treatment target range (33°C–34°C) on arrival to the Texas Children's Hospital (TCH) NICU. This was a retrospective quasi-experimental study of 42 infants who were transported to TCH for treatment of perinatal HIE between August 2012 and April 2016. Active cooling using a continuous core temperature servo-controlled cooling device (CritiCool) began in January 2014; before that, passive cooling on transport was used. Passive cooling was initiated by turning off external heating devices. Fourteen infants received active cooling, and 28 were passively cooled. Demographic data, gestational age at birth, birth weight, and Sarnat stage were not different between groups. Although TCH arrival temperatures were not different between the groups (p = 0.841), there was greater variability of temperatures in the passively cooled group (p = 0.001). More actively versus passively cooled patients arrived at the cooling center within the goal temperature range (79% vs. 25%, p = 0.003). After controlling for multiple variables, active cooling was a significant independent predictor for arriving at the cooling center within the goal temperature range. Active cooling during transport of infants with moderate-to-severe HIE was more effective than passive cooling in achieving the target goal temperature range on arrival at the cooling center. If cooling is being considered during transport, we suggest that active servo-controlled therapeutic hypothermia be used.
Introduction
T
Therapeutic hypothermia for the treatment of HIE is usually provided at Level III and IV neonatal intensive care units (NICUs) (American Academy of Pediatrics Committee on Fetus and Newborn, 2012), such as Texas Children's Hospital (TCH). Although providing therapeutic hypothermia is not difficult with the current servo-controlled hypothermia devices (i.e., CoolCap, Blanketrol, and CritiCool), it is the ability to care for and monitor the sickest of newborns with multiorgan failure, provide state-of-the art neuroimaging, and the availability of all pediatric subspecialists, that limits its use to high-level, high-volume NICUs in regional and children's hospitals. Thus, newborns with HIE at hospitals with Level I and II NICUs, where the majority of infants in the United States are born, must be transported to higher level hospitals for therapeutic hypothermia. Since valuable time can be lost during transport, passive cooling initiated at referral hospitals and during transport (although not studied in randomized controlled trials) has become commonplace (Fairchild et al., 2010; Kendall et al., 2010; O'Reilly et al., 2011; Akula et al., 2013). Unfortunately, a substantial number of infants receiving passive cooling are overcooled (Hallberg et al., 2009; Fairchild et al., 2010; Akula et al., 2013; Chaudhary et al., 2013) or not cooled, and less than half arrive at the cooling center within the desired temperature range (O'Reilly et al., 2011; Akula et al., 2013; Chaudhary et al., 2013).
Because passive cooling is often ineffective during transport, and because of the theoretical benefit of beginning therapeutic hypothermia as early as possible, TCH began using active cooling during transport with a servo-controlled hypothermia device in January 2014. Studies have shown increased risk of adverse outcomes with both low and elevated temperatures in infants with HIE (Wyatt et al., 2007; Hallberg et al., 2009; Laptook et al., 2013). Thus, controlling temperature more systematically during transport should be safer and deliver neuroprotection sooner and more effectively (Gulczynska et al., 2015; McNellis et al., 2015). The purpose of this study was to evaluate whether active cooling on transport was more effective than passive cooling in achieving temperatures in the treatment goal range (33°C–34°C) when infants arrived at the TCH NICU.
Materials and Methods
Patient population
The Baylor College of Medicine IRB-approved TCH HIE database was queried for newborns with moderate-to-severe HIE, who met institutional criteria for therapeutic hypothermia treatment and were transferred from birth hospitals outside the Texas Medical Center by the TCH Kangaroo Crew Transport Team. TCH is a large referral/birth center with 2500 admissions per year to the NICU; 20–30 infants with moderate-to-severe HIE receive therapeutic hypothermia annually. Untrained referral physicians, in consultation with a TCH neonatologist receiving the transport call, determined eligibility for cooling. When it was decided that cooling criteria were met, passive cooling (turning off external heat sources) was initiated. Institutional criteria (Section of Neonatology Guidelines, 2015–2016) for cooling, modified from the NICHD Neonatal Research Network whole-body hypothermia trial (Shankaran et al., 2005), is as follows: ≥35 weeks' gestation; and biochemical evidence of a hypoxic ischemic event (pH ≤7 or base deficit ≥16 mmol/L on a cord gas or within the first hour of life, or, if no blood gas was available or pH 7.01–7.15, or base deficit 10–15.9 mmol/L, and presence of an acute perinatal event and an Apgar score <5 at 10 minutes of age, or need for resuscitation for ≥10 minutes); and evidence of moderate-to-severe encephalopathy (seizures or abnormalities in 3 of 6 modified Sarnat criteria). All transported infants were included in the study if cooling was initiated within 6 hours of life. Infants with HIE born at our birthing center were not included in the study, as transfer to the NICU for therapeutic hypothermia only takes minutes. The current hypothermia program began in August 2012 and active cooling on transport was initiated in January 2014.
Data collection
Maternal and neonatal demographic and clinical data including maternal age, race, prenatal care, gravidity, mode of delivery, delivery complications, date and time of birth, gestational age at birth, birth weight, gender, size for gestational age, Apgar scores at 1, 5, and 10 minutes, Sarnat stage at initiation of cooling, presence of seizures, days intubated, lowest blood sugar, and discharge disposition (death before hospital discharge) were queried from the HIE database for this quasi-experimental study. Additionally, total transport time, and temperatures (with the corresponding times) at the Transport Team's arrival at the birth centers, when entering the ambulance for return to TCH, during transport (approximately every 15 minutes), and upon admission to the TCH NICU were obtained. Total transport time was calculated as the time from the Transport Team's arrival at the referral hospital to arrival at TCH NICU (Akula et al., 2015).
Infants with HIE are transported from birth hospitals by ground ambulance to TCH using the specialized Kangaroo Crew Transport Team (the Transport Team does not use helicopters). Further, no infants with HIE are transported for cooling via fixed wind aircraft because most referral hospitals are within 90 miles of TCH. The team consists of a pediatric/neonatal critical care nurse, a pediatric/neonatal critical care respiratory therapist, and a Neonatal Nurse Practitioner. Management and stabilization of newborns with HIE by the Kangaroo Crew is under the supervision of the NICU transport physician. Since the current active cooling device does not have a battery, it is not taken into the birth hospital, and stabilized passively cooled infants are first placed on it in the ambulance on the way back to TCH.
For active cooling on transport and at TCH, the CritiCool System and Cure Wrap blanket (Mennen Medical Ltd., Feasterville-Trevose, PA) are used. The CritiCool cooling unit has been used during transport and in NICUs throughout the world for the treatment of moderate-to-severe perinatal HIE (O'Reilly et al., 2011; Weiss et al., 2014; Sharma, 2015). The device is about 35 kg, about 1 m high, has a handle, and easy-lock wheels, and is easily secured in the ambulance. Tap water is placed into the device and circulated via tubing into the Cure Wrap cooling blanket, which wraps around the infant's head and body. The system is set to 33.5°C and is continuously servo-controlled to the patient's rectal temperature. Rectal temperature probes versus esophageal probes are used during transport because they do not require X-ray confirmation of proper placement, which would delay admission to the cooling center. Once in the TCH NICU, the infant is moved to another precooled CritiCool device, and cooling continues for a total of 72 hours. At the end of cooling, active controlled rewarming is achieved automatically (algorithm increases temperature 0.5°C/hour) until the infant becomes normothermic.
Statistical analysis
Comparison was made between passive and active cooling groups using Fisher's exact test for categorical variables and the Wilcoxon rank-sum test for quantitative variables. Conover's test was used to compare the groups' variability in arrival temperature. The median and interquartile range was used to describe Apgar scores while the mean and standard deviation was used to describe other quantitative variables.
Logistic regression analysis was used to compare the groups' odds of arriving in the target temperature range after adjusting for covariates that were statistically different using bivariate analysis between the groups (Apgar score at 5 minutes and transport time) and for clinically relevant covariates (Sarnat stage, birth weight, and gender). Additionally, logistic regression was used to examine the association of group with arriving in the target temperature range after adjusting for propensity score.
Propensity scores were computed by fitting a logistic regression model with “group” (active vs. passive cooling) as the dependent variable and including all variables exhibiting a significant bivariate association with group as the independent variables. Propensity scores are the estimated probability of being assigned to the active cooling group from this fitted logistic regression model. Then propensity score and group were the independent variables in the subsequent logistic regression model with arriving in the target temperature range as the dependent variable, to investigate the association of active cooling with odds of arriving in the target temperature range after adjusting for group differences (i.e., propensity score). Use of propensity scores reduces bias and facilitates causal inference in nonrandomized studies involving group comparisons (D'Agostino, 1998).
Linear regression was used to investigate differences in the groups' arrival temperature after adjusting for transport time. Additionally, linear regression was used to compare the groups' absolute difference in arrival temperature from the target range of 33°C–34°C after adjusting for propensity score. The absolute difference in arrival temperature from the target range of 33°C–34°C (absolute difference) was computed as follows: (1) if the arrival temperature was 33°C–34°C (inclusive), the absolute difference = 0°C; (2) if the arrival temperature was <33°C, then the absolute difference = 33 minus arrival temperature (°C); and (3) if the arrival temperature >34°C, then the absolute difference = arrival temperature minus 34°C.
SAS version 9.4 (SAS Institute, Inc., Cary, NC) was used for all data analysis. The power analysis indicated that 14 patients in the active cooling group and 28 patients in the passive cooling group provide 80% statistical power to detect, at the 5% significance level, group differences of about 40% in the proportion arriving in the target temperature range.
Results
Maternal and neonatal demographic and cooling data for the 42 patients (28 passively cooled and 14 actively cooled) are included in Table 1. All infants received passive cooling at the birth hospital before the transport team arrived. Generally, infants who received passive cooling on transport were not different than those who received active cooling, with the exception of having lower Apgar score at 5 minutes (p = 0.004) and decreased transport time (p = 0.033). On arrival at the birth hospital, temperatures were not different (34.5°C ± 1.8°C vs. 34.7°C ± 2.2°C, p = 0.841) between passively and actively cooled infants. Mean temperatures on transport were also not different (34.1°C ± 1.7°C vs. 33.4°C ± 0.6°C, p = 0.065) between passively and actively cooled infants. Although arrival temperatures to TCH NICU were not different, passively cooled patients had significantly higher variability in temperature on arrival to the cooling center than actively cooled patients (standard deviation 1.7 vs. 0.6, Conover test Z = −3.3, p = 0.001, Fig. 1).

Temperatures on arrival at the birth hospital, during transport, and arrival at the cooling center in passive versus active cooling patients. Area between horizontal bars is the goal arrival temperature at TCH (33°C–34°C). Hatched bars represent passively cooled infants and open bars represent actively cooled infants. TCH, Texas Children's Hospital.
Mean ± SD with Wilcoxon rank-sum test.
n (%) with Wilcoxon rank-sum test.
n (%) Fisher's exact test.
Median (IQR).
IQR, interquartile range.
Actively cooled versus passively cooled patients had increased odds of arriving at the cooling center with temperatures in goal range (11/14 [79%] vs. 7/28 [25%]; unadjusted odds ratio 11.0, 95% CI 2.4–51.1, p = 0.002) (Table 2). More infants in the passive group arrived at the cooling center with temperatures below the goal range than actively cooled infants, but the difference was not significant (6/28 [21%] vs. 2/14 [14%], p = 0.670). Moreover, more infants in the passive group arrived at the cooling center with temperatures above the goal temperature range than actively cooled infants (15/28 [54%] vs. 1/14 = [7%], p = 0.006). The proportion of patients below goal, at goal, and above goal arrival temperature was different between the active versus passive cooling groups (p = 0.003). The trajectory of temperatures from birth hospitals to the cooling center is shown for each patient, and by cooling status in Figure 2.
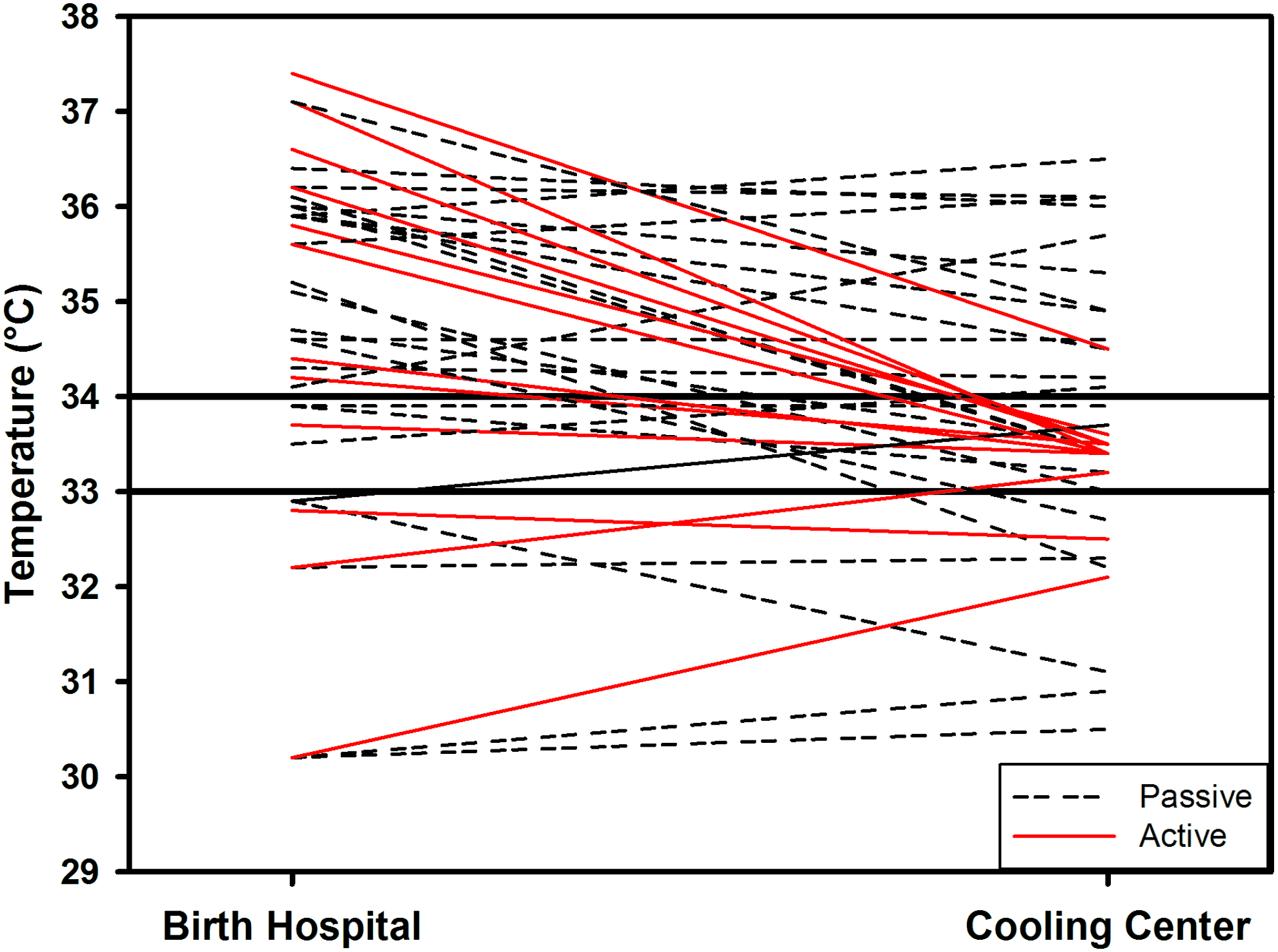
Temperature trajectory from birth hospital to cooling center for individual passive versus active cooling patients. Area between horizontal bars is the goal arrival temperature at TCH (33°C–34°C). Black (dashed) lines represent passively cooled infants and red (solid) lines represent actively cooled infants. Color images available online at www.liebertpub.com/ther
Adjusted for Apgar score at 5 minutes, transport time, Sarnat stage, birth weight, and gender.
After adjusting for Apgar score at 5 minutes, transport time, Sarnat Stage, birth weight, and gender, infants exposed to active cooling had significantly higher odds of arriving in the goal temperature range than passively cooled patients (adjusted odds ratio 22.0, 95% CI 2.0–247.5, p = 0.012) (Table 2). The Hosmer–Lemeshow goodness of fit test did not indicate a significant lack of fit for this logistic regression model (χ2 = 9.0, df = 8, p = 0.341). After adjusting for propensity score, patients exposed to active cooling had significantly higher odds of arriving in the goal temperature range than passively cooled infants (adjusted odds ratio 27.3, 95% CI 2.7–278.9, p = 0.005) (Table 2). The Hosmer–Lemeshow Goodness-of-fit test did not indicate significant lack of model fit (χ2 = 7.4, df = 8, p = 0.491).
With linear regression, neither type of cooling (p = 0.151) nor transport time (p = 0.119) was significantly associated with arrival temperature. However, using the absolute difference in arrival temperature from the target range of 33°C–34°C (instead of the actual temperature), patients exposed to passive cooling had an absolute difference in arrival temperature 1.0°C greater than patients exposed to active cooling after adjusting for propensity score, and this was significantly different between cooling groups (p = 0.002). This linear regression model explained a significant proportion of the variation in absolute difference in arrival temperature from the target range of 33°C–34°C (R2 = 0.242, p = 0.005).
Discussion
In this study, we observed that active cooling during transport was more effective than passive cooling in achieving the target goal temperature range on arrival at the cooling center in infants with moderate-to-severe HIE. Only one randomized controlled transport trial has been performed comparing usual (passive or ice/gel pack cooling) to servo-regulated device cooling (Akula et al., 2015). They observed, in unadjusted analysis, improved temperature regulation with more infants reaching the target temperature range during transport with a servo-controlled device. In a retrospective study similar to ours, Weiss et al. (2014) reported that 90% of active cooled infants and 50% of passive cooled infants arrived at the cooling center in the goal target temperature range. All transport passive versus active cooling studies, however, did not adjust for transport time, Sarnat stage, or any other perinatal variables. Therefore, to differentiate our study from others, we used multivariable logistic regression and propensity score analysis and found that infants who were actively cooled during transport had much higher odds of arriving at the cooling center in the goal temperature target range. Consistent with the only randomized controlled trial (Akula et al., 2015), we observed that active cooling compared to passive cooling appeared to be safe, resulted in tighter temperature control, and was not associated with increased morbidity or mortality.
Three actively cooled infants arrived at TCH outside of the goal temperature range. One infant was placed on the Criticool device with an initial temperature of 29.0°C; during the 37 minute transport, the infant warmed to 32.1°C. The second infant's lowest temperature was recorded as 30.3°C; during the transport, because of a malfunctioning ambulance, the infant had to be moved to another ambulance. The duration of the transfer to the second ambulance was not documented, therefore it is unclear how long this infant was without active temperature management, and arrived at TCH with a temperature of 32.5°C. The last out of range infant, arrived at TCH above the goal temperature range. During a short transport (37 minutes), the temperature decreased from 37.5°C to 34.4°C. There appeared to be no adverse effects in these three infants.
The major strength of our study is that we used multivariable logistic regression to adjust for other covariates that may impact temperature regulation. Moreover, we also used propensity score analysis and found similar increased adjusted odds ratios to the multivariable logistic analysis. On the other hand, there were some limitations to our study. We used retrospective data from a relatively small sample size from a single center. However, most head-to-head passive versus active cooling studies come from single centers with similar sample sizes. We also used a cooling device that was bulky, heavy when filled with water, and most importantly, could not be easily used in the birth hospital by the transport team during stabilization of sick infants due to its reliance on a power source. However, none of the current FDA-approved devices have a battery, and therefore transported infants are usually cooled after stabilization and when placed in the transport vehicle. Currently, we do not use helicopter or fixed wing transport for infants with HIE who require cooling, therefore our results may not be generalizable to other centers that go longer distances via air transport. We are, however, considering beginning air transport for infants with HIE. Mounts and brackets are available from Mennen Medical, Ltd and a few sites have obtained Federal Aviation Administration approval for use during air transport.
It is also important to acknowledge that one of the major limitations of transport cooling programs, in general, and transport cooling studies, including our own, in particular, is the reliance on untrained physicians from birth hospitals to accurately determine whether infants meet criteria for therapeutic hypothermia despite rarely encountering this condition. Thus, some infants with mild HIE and neonatal encephalopathy due to other causes may receive therapeutic hypothermia when it may not be warranted. This was recently observed in a study comparing active cooling begun at birth hospitals versus active cooling begun by a newborn emergency transport service. They found that 18% of infants who had cooling begun at the birth hospital did not have moderate-to-severe HIE compared to only 2% of those started by the transport team. Importantly, therapeutic hypothermia for those with mild HIE has not been proven to be efficacious. However, therapeutic hypothermia was able to be begun about 2 hours sooner and target temperature was achieved about 1 hour sooner in the group that began cooling at the birth hospital (Roberts et al., 2016). Although therapeutic hypothermia is relatively safe when provided in high-level centers (Edwards et al., 2010; Simbruner et al., 2010; Azzopardi et al., 2014), treating infants who may not need it unnecessarily delays maternal-infant bonding and may increase difficulty with breastfeeding. Although reduced time to cooling has not been shown to improve outcomes in hypothermia randomized controlled trials (Shankaran et al., 2005; Azzopardi et al., 2008), we speculate that the potential benefits for infants with moderate-to-severe HIE likely outweigh the potential risks in those with mild disease who receive therapeutic hypothermia.
In conclusion, active cooling increases the odds of arriving at the referral center in the target temperature range, even after controlling for a number of variables that may affect the speed of temperature decrease. We suggest that referral centers who care for infants with moderate-to-severe HIE develop comprehensive guidelines for cooling on transport and use active cooling with a servo-controlled hypothermia device when available. We expect that servo-controlled devices with batteries designed specifically for transport will be available soon so that the definitive therapy can be begun earlier.
Footnotes
Acknowledgments
The authors are grateful to the Kangaroo Crew and the Neonatal Nurse Practitioners who accompany our patients during transport as well as the cooling nurses at the bedside led by Allison L. Walton, BSN-RNC. Thanks to The Evangelina “Evie” Whitlock Fellowship Award in Neonatology for supporting this research. The work was performed at the Texas Children's Hospital with the approval of the Baylor College of Medicine Institutional Review Board, Protocol H-36500.
Author Disclosure Statement
No competing financial interests exist.