
Abstract
Targeted temperature management (TTM) improves survival and neurological outcome after nontraumatic cardiac arrest. However, TTM is not used widely after traumatic cardiac arrest because of concerns that it might exacerbate bleeding. We report the use of postarrest TTM after repair of blunt myocardial rupture. A 48-year-old man was admitted after being rescued from a major traffic accident by the local emergency service. Focused sonography showed pericardial fluid without cardiac tamponade. Computed tomography showed a large hematoma in the anterior mediastinum associated with hemopericardium. The patient developed cardiac arrest during the operative preparations. Repeat bedside sonography revealed a large pericardial effusion and signs of cardiac tamponade. Spontaneous circulation was restored after ultrasound-guided pericardiocentesis. His Glasgow Coma Scale score was 3. The patient was transported promptly to the operating room and underwent median sternotomy without cardiopulmonary bypass. A rupture of the junction of the superior vena cava/right atrium and left atrial appendage was detected and was closed by direct suturing. Immediately after return to the intensive care unit, we performed TTM (target body temperature 34.5°C) using a surface-cooling device at 4 hours postarrest. TTM was maintained for 24 hours and controlled gradual rewarming was then initiated. He regained consciousness 36 hours postrewarming with limited speech ability. The patient recovered with no further cardiac events and was discharged 3 weeks after admission, with no other serious complications. The patient was neurologically intact (cerebral performance category 1) at 6 months of follow-up. This case demonstrates the potential benefit and applicability of postarrest TTM in patients after repair of blunt myocardial rupture.
Introduction
T
Case Presentation
A 48-year-old male driver was trapped in his car between two trucks during a major traffic accident. He was brought to our emergency center 30 minutes after the accident by the local rescue and emergency service. At the emergency center, he was confused and complained of having a tight chest. We immediately initiated resuscitation and primary survey with fluid administration. Primary survey revealed no airway compromise, with equal bilateral air entry. The patient's pupils were of equal size with prompt reaction, and there were no gross neurological deficits. His blood pressure was 100/60 mmHg, pulse rate 103/min, respiratory rate 23/min, and his Glasgow Coma Scale (GCS) score was 9.
Focused sonographic assessment for trauma showed no free intraperitoneal fluid, but a small liver laceration and large amounts of pericardial fluid without cardiac tamponade. Chest, pelvic, and lateral cervical-spine X-rays revealed unremarkable findings. However, immediately before examining the computed tomography (CT) scan, his blood pressure was 68/40 mmHg. We performed endotracheal intubation and administered a total of 1000 mL of normal saline in preparation for a blood transfusion. His systolic blood pressure recovered to >90 mmHg after resuscitation. We suspected multiple injuries and a bleeding focus. Examination of a brain CT showed no evidence of intracranial injury, but chest CT showed a large hematoma in the anterior mediastinum, associated with hemopericardium (Fig. 1).
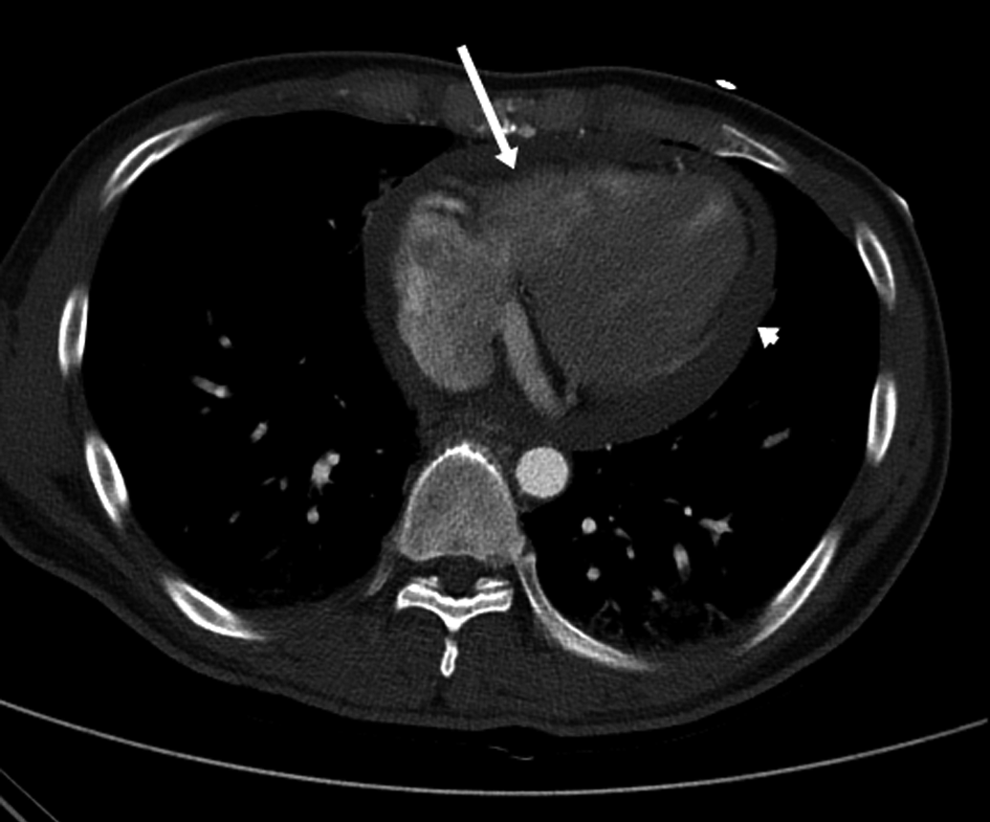
Chest CT showed a large hematoma in the anterior mediastinum (white arrow) associated with hemopericardium (arrowhead). CT, computed tomography.
The patient developed cardiac arrest during the operative preparations. Bedside-focused echocardiography was repeated during cardiopulmonary resuscitation, which revealed a large pericardial effusion and signs of cardiac tamponade (Fig. 2). We performed ultrasound-guided pericardiocentesis through the subxiphoid route. Spontaneous circulation was restored after drainage of 200 mL of fresh blood, and return of spontaneous circulation (ROSC) was achieved 20 minutes after the collapse. His GCS score was 3 (E1V1M1). We, therefore, decided to perform TTM immediately after repair of myocardial rupture.

Focused assessment with sonography for trauma showed a large pericardial effusion with diastolic collapse of the right ventricular free wall (arrows).
The patient was then transported promptly to the operating room and underwent a median sternotomy followed by an inverted-T pericardiotomy and hematoma evacuation. A 1.5-cm rupture between the superior vena cava and the right atrium (Fig. 3) and a 0.5-cm rupture at the left atrial appendage were oversewn without cardiopulmonary bypass. The patient's mean arterial pressure had decreased to 56 mmHg before successful repair, despite administration of inotropes and vasopressors, and his oxygen saturation had been <80% on FiO2 of 1.0 over 1 hour. His core body temperature was 36.0°C.

Intraoperative view. Hemorrhage was controlled with a clamp. Rupture of the superior vena cava at right atrial junction (white arrow).
Immediately after returning from the operating room, we performed TTM using a surface-cooling device (Arctic sun®; Bard Medical, Louisville, CO) with cold saline infusion (4°C) 4 h 20 min post-ROSC. The target body temperature of 34.5°C was reached 3 h after implementation.
The results of initial laboratory tests on admission to intensive care unit showed respiratory acidosis of pH 7.3 mmHg and PaCO2 56 mmHg with elevated lactate 6.1 mmol/L, as well as elevated levels of cardiac markers, creatinine kinase (CK) was 771 IU/L (reference value 0–190), CK-MB 68.9 IU/L (reference value 0–3.6) and Troponin-T 1.47 ng/mL (reference value 0.0–0.1). Coagulation tests such as platelet count, international normalized ratio (INR), and aPTT were all within normal limits. Electrocardiographic findings did not reveal anything specific of arrhythmia, heart blocks, or ST-segment changes.
On the second day, the patient underwent sensory evoked potential (SEP) to assess prognosis 44 hours post-ROSC. SEP showed bilateral prolonged absolute latencies of cortical N20 waves (left 22.8 milliseconds, right 22.4 milliseconds). On the third day, the patient was monitored using electroencephalogram (EEG). EEG showed no epileptiform discharge and a diffuse alpha frequency activity. In addition, diffusion-weighted MRI on the fourth day revealed T2 high signal intensity lesions in the left frontal subcortical white matter without abnormal diffusion restriction.
Coagulation parameters and hemoglobin were closely monitored during and after the course of hypothermia. Platelet nadir (72 × 109/L) at 7 hours after induction of TTM subsequently improved. The INR and aPTT counts changed minimally.
TTM was maintained for 24 hours, and controlled gradual rewarming was then initiated. The target rewarming rate was 0.5°C of temperature elevation every 12 hours. Follow-up coagulation testing after rewarming (36.0°C) revealed a slightly decreased platelet count (85 × 109/L), and normal INR (1.05) and aPTT (31.4 seconds) (Fig. 4). After rewarming, the patient experienced confusion and nocturnal agitation, but achieved a GCS score of 15 at 26 hours postrewarming. He subsequently recovered with no further cardiac events and was discharged 3 weeks after admission, with no other serious complications. The patient was neurologically intact (cerebral performance category 1) at 6 months of follow-up.
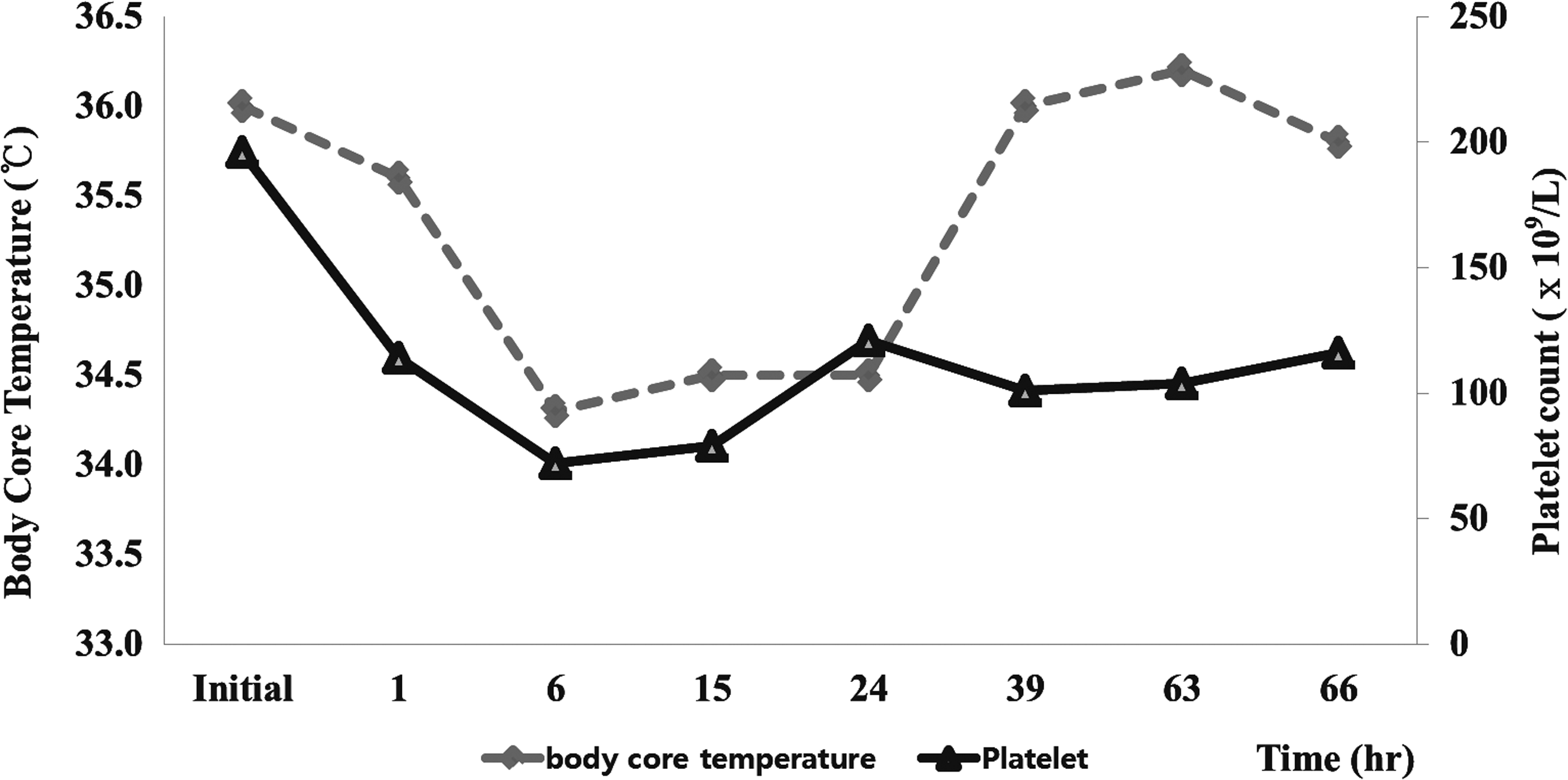
Core body temperature and platelet count during therapeutic hypothermia.
Discussion
This case report demonstrates the safety and benefit of TTM after cardiac arrest in patients with blunt traumatic cardiac rupture. TTM can improve the neurological outcome after cardiac arrest, compared with no temperature management (Arrich et al., 2016). Although one case series suggested that carefully selected trauma patients who remained comatose after resuscitation from cardiac arrest may benefit from induced hypothermia (Tuma et al., 2011), the use of hypothermia or TTM in cardiac-arrest patients after severe trauma remains poorly understood.
Trauma patients who suffer cardiac arrest have very poor survival. Timely resuscitation, including emergency thoracotomy, extracorporeal life support, and TH, has been suggested to improve survival in patients with such serious conditions (Tisherman, 2013). However, the probability of survival remains very low for patients sustaining severe chest trauma with acute cardiac arrest, and blunt traumatic rupture of the myocardium with tamponade is also associated with high mortality (Nan et al., 2009).
Resuscitative thoracotomy with pericardiotomy is the definitive management option for cardiac tamponade because of blunt chest trauma. If emergency thoracotomy is not immediately available, pericardiocentesis can provide an effective temporary measure until definitive treatment can be performed, as in our patient (American College of Surgeons, 2012). We repeated the focused assessment with sonography for trauma as a diagnostic and therapeutic tool for hemopericardium (Chelly et al., 2004).
One of the major concerns regarding the use of TTM in trauma victims is the potential impact on coagulopathy. Hypothermia can impair blood clotting; TH induces platelet dysfunction at temperatures ≤35°C and inhibits the coagulation cascade at temperatures ≤33°C. (Polderman, 2009). Bleeding diathesis and ongoing bleeding are, therefore, relative contraindications for the use of TH (Polderman, 2008). The use of TH after traumatic cardiac arrest is thus still under investigation. Many experimental studies have shown that induction of TTM can improve survival in a severe-hemorrhagic-shock model (Wu et al., 2005). Some experts advocate cooling at a slightly higher temperature of 34.5–35°C in patients with suspected or active bleeding (Rittenberger et al., 2015). However, TH should be used cautiously in patients with active bleeding or at high risk of bleeding, and the source of bleeding should be controlled before cooling the core body temperature (Polderman, 2009).
In the present case, we believed that the beneficial effect of TTM outweighed the risk of hypothermia-induced coagulopathy. We also implemented TTM (to a target body temperature of 34.5°C) after successful repair of myocardial rupture sites to minimize the risk of bleeding. There was no evidence of clinically significant bleeding during the TTM period in this case, and coagulation parameters and hemoglobin only changed minimally, within normal limits. Although the patient's platelet count fell below normal reference values, it recovered quickly without the need for platelet transfusion.
Conclusion
This case demonstrates that postarrest TTM can be safe and beneficial after repair of myocardial rupture from blunt chest trauma. TTM might also help to improve neurological outcomes after successful resuscitation in blunt cardiac trauma patients.
Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Footnotes
Author Disclosure Statement
No competing financial interests exist.