
Abstract
Therapeutic hypothermia (TH) is a potent neuroprotectant for experimental ischemic stroke, but studies of TH for intracerebral hemorrhage (ICH) are emerging. We systematically reviewed the experimental literature to assess TH efficacy for ICH. We found 18 suitable papers; quality scores were moderately good. Compared with normothermia, TH reduced measures of edema (mean effect size (95% CI) −1.6873 (−2.3640, −1.0106), p < 0.0001) or blood–brain barrier leakage (p < 0.0001) and improved behavioral outcomes (p < 0.0001). There was no evidence of publication bias. In this meta-analysis of available preclinical studies of ICH, TH is potently effective for reducing perihematomal edema and for improving behavioral outcomes.
Introduction
N
In both human and animal models of ICH, neuropathology studies demonstrate hematoma toxicity, oxidative stress, and inflammation around the hemorrhage (Aronowski and Zhao, 2011). Therapeutic hypothermia (TH) is an established neuroprotectant, which has demonstrated the capacity to prevent neuronal loss and improve functional outcome in animal models of cerebral ischemia (Dumitrascu et al., 2016; van der Worp et al., 2010) and in clinical treatment of cerebral edema after acute brain injury (Polderman, 2008; Kollmar and Schwab, 2009).
Fever occurs in more than 90% of patients with ICH (Schwarz et al., 2000) and is independently associated with hematoma growth after ICH (Rincon et al., 2013), possibly by increasing metabolism of the brain and exacerbating neuronal injury. Results have been positive for both temperature modulation for fever after ICH (Rincon et al., 2013; Lord et al., 2014) and TH in the setting of ICH (Kollmar et al., 2010; Staykov et al., 2013), although data regarding outcomes remain somewhat limited. Human clinical trials for TH for ICH are underway to address to establish whether TH has a benefit on clinical outcome (Kollmar et al., 2012; Rincon et al., 2014). We aimed at identifying whether existing preclinical data support a hypothesis of an overall benefit of TH over normothermia (NT).
Materials and Methods
We conducted a systematic search guided by prior protocols (Macleod et al., 2009; Dumitrascu et al., 2016) of the medical literature by using Web of Science, Pubmed and Ovid using search terms (((* intracerebral hemorrhage[MESH] OR ICH [MESH] OR intracranial hemorrhage [MESH] OR hemorrhagic stroke[MESH] OR brain hemorrhage [MESH])) AND (hypothermia OR temperature)) AND animal. All abstracts that reported various modalities of TH in different animal models of ICH were identified. The papers were included in the systematic analysis if they reported the treatment effect of induced hypothermia versus NT in animal ICH models. Each paper was rated for scientific rigor and quality by using published criteria (Macleod et al., 2009).
The following data were collected and analyzed: gender, animal species, model of ICH induction, modality of induced hypothermia, hypothermia duration, timing between ICH induction and hypothermia initiation, the target temperature, temperature measurement model, hematoma volumes, neurobehavioral scores, cerebral edema volume by both brain water content and blood–brain barrier breakdown, gene expression, and numbers of cells labeled with various markers of apoptosis or necrosis.
The computed normalized effect sizes and standard errors were summarized in a meta-analysis, assuming a random-effects model weighting each mean effect size by standard error (Vesterinen et al., 2014). Heterogeneity was tested with the Q statistic. We assessed for publication and other bias by using funnel plot asymmetry, trim-and-fill analysis, and Eggers regression (Sena et al., 2010). Funnel plots measure the treatment effect against study size to detect bias with greater asymmetry, indicating bias and trim-and-fill analysis, and then impute theoretical missing studies (Vesterinen et al., 2014). Meta-regression was performed by using a mixed-effects model with treatment onset delay and duration entered as fixed factors. All analyses were completed by using R version 3.2.2 and the metafor package (ver 1.9-8) (Viechtbauer, 2010).
Results
Our initial literature search identified 332 citations, from which we excluded 314 papers based on title or abstract review for no use of hypothermia (215), using an ischemic stroke model (67), traumatic model (25), subarachnoid/subdural/epidural hemorrhage model (35), traumatic mode, use of hypothermia in indications other than ICH (31), absent comparison against NT (18), not English (3), or human subjects (2). The final study group included 18 papers (Supplementary Appendix SA1; Supplementary Data are available online at www.liebertpub.com/ther).
Quality scores (8 points maximum) ranged from 1 to 6 (median[IQR] 4 [2, 4.25]). There was no relationship between quality score and effect size. All studies reported the species used, and none included a sample size or power estimation.
Study species included Sprague–Dawley rats in 12 studies, Wistar rats in 4 studies and one study each used a C57/BL6 mouse or a porcine model. The anesthetic used during the operation was reported in all but one study and included sodium pentobarbital (4 studies), isoflurane (11 studies), and chloralhdyrate (2 studies). Target cooling temperatures ranged from 32°C to 35°C. The delay to treatment start ranged from 1 to 24 hours, and the duration of TH ranged from 0 to 144 hours. Methods of cooling included whole body cooling (mechanical) (eight studies), whole body cooling (pharmacological) (two studies), and selective cooling with an implanted intracranial device (eight studies).
Intracerebral hematomas were induced by a stereotactic injection of collagenase (nine studies), autologous blood (eight studies), or thrombin (two studies). We computed the normalized mean difference in hematoma volumes comparing NT treatment with all modalities of TH after focal ICH. Across all target temperatures and cooling modalities, there was no statistically significant treatment effect (Fig. 1) with considerable heterogeneity (Q22 = 1415.67, p < 0.0001) (Supplementary Fig. S1).
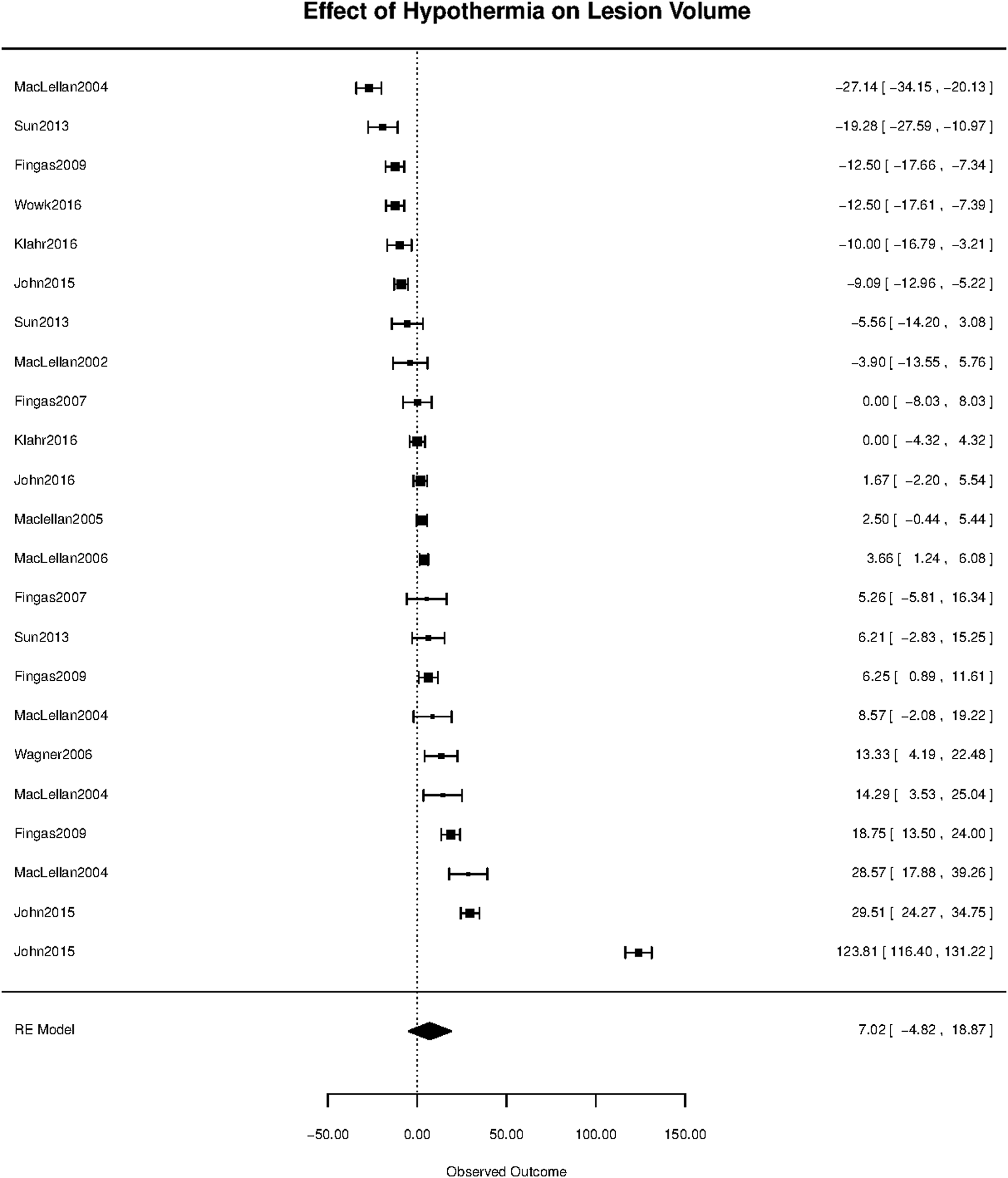
Meta-analysis of the effect of therapeutic hypothermia (TH) on intracerebral lesion volume. Among the 18 papers included, there were 23 separate assessments of lesion volume that were converted to normalized treatment effects. There was no statistically significant effect of TH. Meta-regression for a moderating effect of delay to treatment, duration of TH, and mode of cooling showed no significant effects.
The effects on cerebral edema were measured by either brain water content or blood–brain barrier leakage as measured by Evans Blue extravasation. TH improved edema by both measures (Fig. 2). TH improved brain water content reduction (Fig. 2A) with a mean treatment effect size [95% CI] of −1.69 [−2.36, −1.01], p < 0.0001 in 20 comparisons with significant heterogeneity Q20 = 195.4724, p < 0.0001. There was no evidence of publication bias, funnel asymmetry, z = 1.2, p = 0.2218, and number of missing studies estimated at 0 (SE = 2.7826) (Supplementary Fig. S2). TH improved blood–brain barrier breakdown (Fig. 2B) in nine comparisons with a mean treatment effect size [95% CI] of −88.47 [−115.55, −61.39], p < 0.0001, with significant heterogeneity Q9 = 2910.2672, p < 0.0001. Again, there was no evidence of publication bias (Supplementary Fig. S3). The data, therefore, suggest a powerful treatment benefit from TH despite inter-laboratory variation, notably cooling modality, species, stroke model, and target temperature.

Meta-analysis of the effect of TH on cerebral edema. There were 21 assessments of brain water content
Reduction of perihematomal edema might be expected to influence behavioral outcome after ICH (Fig. 3), and indeed, there was a significant effect on behavior as measured in 20 experiments. The effects on neurobehavioral scores had an estimated mean effect size [95% CI] of 16.0310 [7.0539, 25.0082] p < 0.001 in a total of 21 comparisons. The estimate showed considerable heterogeneity (Q20) = 297.6192 (p < 0.0001), with no evidence of publication bias (Supplementary Fig. S4).
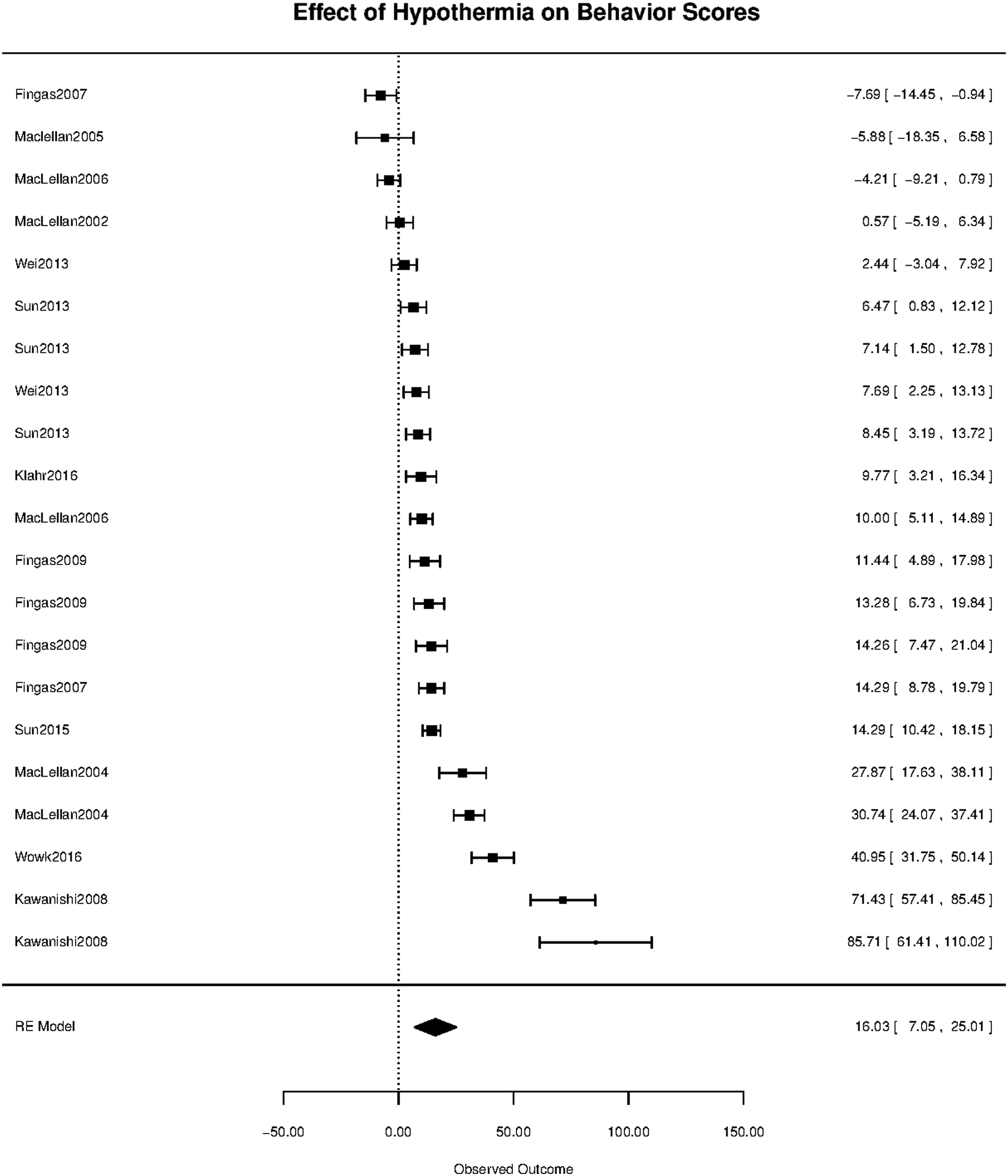
Meta-analysis of the effect of TH on behavioral score. There were 21 assessments in the available studies, using a variety of behavioral tasks. The raw data was used for tasks in which better performance yielded larger numerical measurement. For scales in which smaller numbers represented superior performance, the raw value was subtracted from the maximum possible scale score. Reported standard errors were converted to standard deviations. The results showed a significant benefit of TH. The normalized treatment effect was estimated as mean [95% CI] of 16.0310 [7.0539, 25.008], p < 0.001. The analysis shows considerable heterogeneity: Q 20 = 297.6192, p < 0.0001. There was no publication bias detected, with the test for funnel plot asymmetry z = 5.0575, p < 0.0001 but the estimated number of missing studies on the left side: 0 (SE = 2.0057).
Although the mechanism of benefit for TH is uncertain, many papers assayed a variety of genes that are known to be important in outcome after cerebral injury, including IL-1b (Wagner et al., 2006), claudin (Sun et al., 2013), occluding (Sun et al., 2013), bax (Sun et al., 2015), and caspase 3 (Sun et al., 2015). In six comparisons, all levels of TH showed a significant reduction in the amount of gene expression, with a mean effect size [95% CI] of −132.52 [−228.30, −36.74], p < 0.01 (Supplementary Figs. S5 and S6).
For all analyses, meta-regression failed to identify a significant influence of delay to treatment or duration of TH with one exception. The meta-analysis of gene suppression revealed a significant influence of TH duration (p < 0.01) such that longer treatment time was associated with greater gene suppression.
Discussion
Our data strongly support further the development of TH as a treatment for ICH. Although hematoma volume size was not affected by TH (Fig. 1), there was a powerful and significant effect in reducing edema formation (Fig. 2) and in improving behavioral outcome (Fig. 3). We used state-of-the-art meta-analysis techniques, as proposed, for rigorous evaluation of pre-clinical data (Vesterinen et al., 2014). The experimental quality of the trials we analyzed was reasonably good (median four out of possible eight points). Thus, the analysis supports TH as a promising putative treatment for ICH that requires further development in clinical application.
The mechanism of effect during TH is uncertain, although a number of salutary changes occur during TH: suppression of metabolic demand for scarce substrate; reduction of free radicals and excitotoxin release; reduction of endothelial cell swelling and damage; and limited entry of inflammatory cells into the damaged brain (Wu and Grotta, 2013). Our data to not address the putative mechanism of TH, but clearly the most important effect was on protecting BBB function and reducing perihematomal edema. Further mechanistic studies will be needed to explore this effect further.
We found considerable heterogeneity in these meta-analyses, but using funnel plots and trim-and-fill analysis (Supplementary Material), we found no evidence that negative trials are systematically missing from the literature. The most likely source of heterogeneity is the inclusion of studies spanning a wide range of species, methods, and techniques. Differences in design and methodological quality between the animal studies constitute a limitation of this systematic analysis. The underlying quality of the analyzed studies was good overall, but there was a considerable variation in rigor, which has been shown to influence treatment effect size, in general, but not in this analysis specifically.
Other limitations should be borne in mind. Despite the lack of evidence for publication bias, there remains considerable uncertainty in the literature as to whether all negative results are being published (Macleod et al., 2009). Stroke models typically utilize young healthy subjects free of the co-morbidities that are typically found in human stroke victims. The methods used to induce ICH in animals, while useful, do not faithfully reproduce the pathogenesis that is usually associated with human ICH.
In conclusion, using rigorous meta-analysis techniques, we showed that recent preclinical data suggest that TH was associated with a considerable reduction in perihematomal edema and significant improvement in behavioral outcome. The data support using TH for treatment of secondary injury in larger clinical trials of acute ICH.
Footnotes
Acknowledgments
This study was partially supported by NINDS R01 NS075930 and the Carmen and Louis Warschaw Family Foundation.
Author Contributions' Statement
K.M. contributed to the study conception and design, acquisition and interpretation of data, and drafting the article and approved the final version for publication. P.L. contributed to the study conception and design, data analysis and interpretation, and critical review of the article for intellectual content and approved the final version for publication.
Author Disclosure Statement
Dr. Lyden discloses that he is principal investigator of the ICTuS 2/3 trial of TH for acute ischemic stroke and a member of the DSMB for the FROST and COOL ARREST trials. Dr. Kara Melmed has nothing to disclose.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.