
Abstract
Outcomes of cardiac arrest (CA) because of drowning in children are generally poor, but some reports show that cases with post-CA hypothermia because of drowning exhibit good recovery when treated with targeted temperature management (TTM). However, because electroencephalogram (EEG) findings are not reported in those cases, a complete examination of brain damage has not been performed during TTM. Here we report a case of a 15-month-old boy with post-CA hypothermia recovery after treating with TTM, along with EEG findings. The initial clinical and laboratory data and resuscitation history in the current case strongly indicated an unfavorable outcome. However, the return of normal EEG findings after 36 hours postadmission may indicate favorable neurological outcomes. Although reliable evidence has not been established, we recommend maintained mild therapeutic hypothermia using TTM, followed by slow rewarming in patients with post-CA hypothermia because of drowning, based on the observations in the current case and in other studies.
Introduction
T
The outcomes in children with cardiac arrest (CA) because of drowning are generally poor (Kieboom et al., 2015), but cases with hypothermia after CA because of drowning show good recovery when treated with targeted temperature management (TTM) (Hein et al., 2004; Guenther et al., 2009; Kawati et al., 2009; Romlin et al., 2015). However, in these cases, the findings of electroencephalogram (EEG), which indicate neurological outcomes (Kessler et al., 2011; Topjian et al., 2016), have not been reported (Hein et al., 2004; Guenther et al., 2009; Kawati et al., 2009; Romlin et al., 2015), and EEG is recommended for neurological monitoring by the International Liaison Committee on Resuscitation for post-CA children (Maconochie et al., 2015). Therefore, the degree of brain damage after CA has only been evaluated using initial laboratory data and the details of patient's resuscitative history; thus, complete examination of brain damage has not yet been performed.
Here we report a significant case of a 15-month-old boy with post-CA hypothermia because of drowning, who recovered after treatment with TTM. We also discuss the findings of EEG obtained during TTM.
Case Presentation
A 15-month-old boy was admitted to our emergency department after CA because of drowning. He had no developmental problems and had been in a good state of health until the drowning accident. He was playing inside the house but had gone to the bathroom alone and accidentally fell into a bathtub of cool water. When his parents found him lying in the water, he was comatose and pulseless. The estimated duration of submersion was around 5 minutes. Cardiopulmonary resuscitation was performed by emergency medical services. Return of spontaneous circulation (ROSC) had not been obtained during prehospital resuscitation, and on admission, electrocardiogram showed pulseless electrical activity. By performing pediatric advance life support with endotracheal intubation and epinephrine (total of six doses) administration, ROSC was obtained 18 minutes after arrival (∼68 minutes after CA). His Glasgow Coma Scale score was 3 and pupil dilation was 6 mm and nonreactive. Arterial blood gas analysis showed pH 6.44; PaCO2, 154 mmHg; PaO2, 47.2 mmHg; HCO3, 9.7 mEq/L; and lactate level, 12.2 mmol/L. Brain computed tomography (CT) revealed severe brain edema and obscure gray–white matter differentiation (Fig. 1). Bladder temperature was 30.4°C. TTM was initiated using a surface device (water circulating gel-coated pads) and was scheduled to maintain his core temperature of 34.0°C for 48 hours to avoid worsening of brain edema, with slow rewarming at the rate of 0.05°C/h (Fig. 2). Approximately 2 hours after hospital arrival, two-channel simplified continuous EEG monitoring was initiated. The target temperature of 34°C was achieved 154 minutes after ROSC, after which two-channel simplified continuous EEG revealed burst suppression (Fig. 3). This burst suppression persisted for several hours, but disappeared at 36 hours after ROSC. His pupils were reactive at the same time. A repeated CT obtained on the third day revealed a reduction in the brain edema. On the fifth day, the international 10–20 system electroencephalography showed no abnormality. The patient was extubated on day 15 after admission and transferred to a pediatric general ward. After performing a neurological evaluation and receiving rehabilitation, he was discharged home on day 70 after admission. The patient made a recovery with a Pediatric Cerebral Performance Category of 1 at 1 year and 2 months after the accident.

Brain CT obtained on admission. CT, computed tomography.
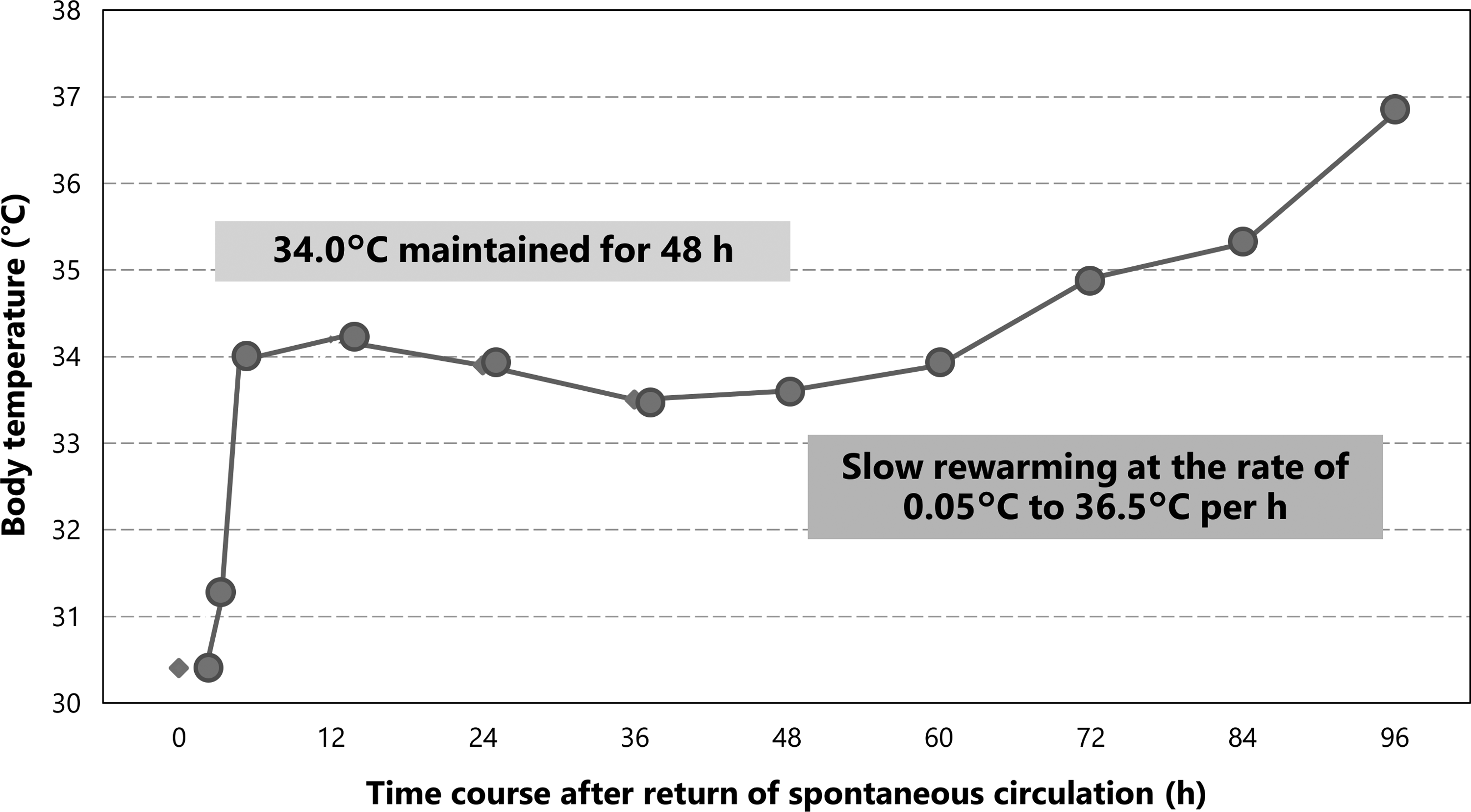
Details of TTM. TTM, targeted temperature management.
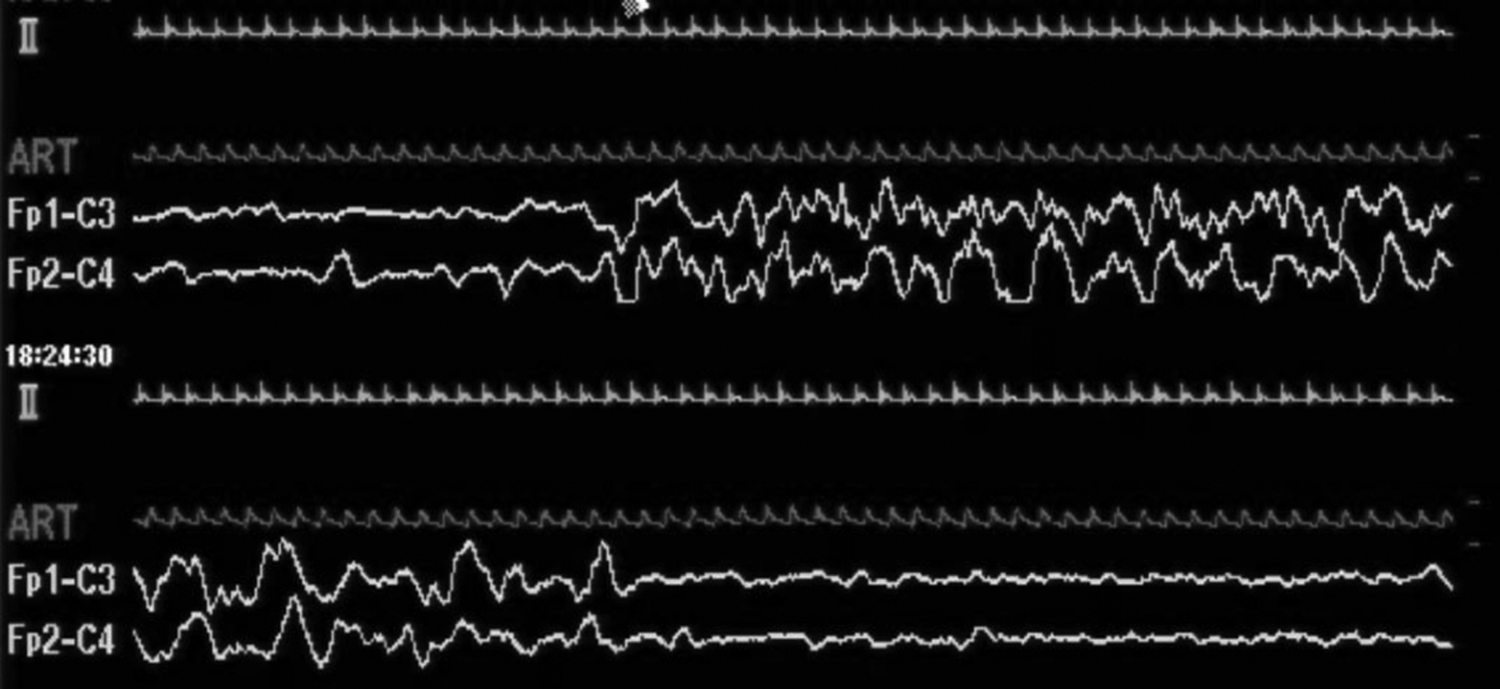
Two-channel simplified continuous EEG obtained during TTM. Two-channel simplified continuous EEG showing burst suppression when the patient's temperature reached 34°C. EEG, electroencephalogram.
Discussion
Several studies on early outcome predictors of pediatric out-of-hospital cardiac arrest (OHCA) have been published. Initial clinical data, such as pH (Moler et al., 2011) and lactate levels (Topjian et al., 2013), and resuscitative history (absence of prehospital ROSC; Goto et al., 2014), unwitnessed OHCA (Goto et al., 2014), frequent epinephrine administration (Moler et al., 2011), or CA caused by drowning or asphyxia (Moler et al., 2011) are associated with poor neurological outcomes. Based on these studies, clinical and laboratory findings obtained before initiating TTM therapy in our current case strongly suggested an unfavorable outcome.
We further compared our current case with previously reported cases of patients with post-CA hypothermia after drowning who were treated with TTM (Table 1). Obvious prehospital ROSC was obtained only in the case reported by Guenther et al. (2009) and ROSC was obtained after arrival at hospital in three cases, including our present case (Hein et al., 2004; Romlin et al., 2015). All five cases had no witnesses during the arrest. Epinephrine doses were described in the cases reported by Guenther et al. (2009), Romlin et al. (2015), and our present case at zero, four, and six doses of epinephrine, respectively. The lowest blood pH among the four cases with available pH data was found in our case (Hein et al., 2004; Guenther et al., 2009; Romlin et al., 2015). However, the highest lactate level (22 mmol/L) was found in the case reported by Romlin et al. (2015), followed by our case and that of Guenther et al. (2009); this value was obtained from a venous blood sample in the case reported by Romlin et al. The first lactate level examined using arterial blood was 12.2 mmol/L in the case reported by Romlin et al., a value same as that found in our case. Considering the mentioned comparisons, we concluded that the current case is the most severe case of OHCA.
CA, cardiac arrest; N/A, not applicable; PEA, pulseless electrical activity; ROSC, return of spontaneous circulation.
EEG findings were not reported for other cases (Hein et al., 2004; Guenther et al., 2009; Kawati et al., 2009; Romlin et al., 2015), but are reported for our current case. Several studies showed that isoelectric or burst suppression is associated with mortality or unfavorable neurological outcomes in pediatric CA (Kessler et al., 2011; Topjian et al., 2016). However, detailed examination revealed that patients with an initial isoelectric or burst suppression background still had a favorable outcome in a relatively small number of patients (5/42 and 7/24, respectively) in a study by Topjian et al. (2016). They found an association between change in EEG and poor neurological outcomes in pediatric patients with CA (Topjian et al., 2016), but the type and timing of change in EEG associated with favorable neurological outcomes have not been determined in children. However, in adult patients with CA, Oh et al. reported a poor neurological outcome rate of 98.2% in patients with burst suppression. Furthermore, the presence of burst suppression in itself and a lack of normal trace development within 36 hours were associated with poor outcomes (Oh et al., 2015). Although the discrepancy between pediatric and adult patients after CA remains unexplored, it may possibly be derived from differences in the extents of functional recovery and in the interpretations of EEGs. Thus, whether the presence of burst suppression in pediatric patients with CA is associated with poor outcomes remains unknown. Therefore, the EEG transition at 36 hours postadmission in the current case may be a crucial factor associated with favorable neurological outcomes in patients with post-CA hypothermia because of drowning who are treated with TTM.
Compared with therapeutic normothermia, therapeutic hypothermia does not show any significant benefits in neurological outcomes in comatose children after OHCA (Moler et al., 2015). However, patients who drowned in ice water with core body temperature ≤32°C were excluded from this trial. The post hoc analysis of drowning cases from this study revealed that there were no significant differences in neurological outcomes in children after drowning in a subgroup analysis, but association between initial temperature and outcome was undocumented (Moler et al., 2016). Thus, the effect of TTM in children with hypothermia on admission remains unknown.
Conclusion
The initial clinical and laboratory data and resuscitation history in the current case strongly indicated an unfavorable outcome. However, the return of normal EEG findings after 36 hours postadmission may indicate favorable neurological outcomes. Although reliable evidence has not been established, we recommend maintained mild therapeutic hypothermia using TTM, followed by slow rewarming in patients with post-CA hypothermia because of drowning, based on the observations in the current case and in other studies.
Consent
Informed consent was obtained from the patient's family for publication of this case report and any accompanying images.
Footnotes
Author Disclosure Statement
No competing financial interests exist.