
Abstract
Therapeutic hypothermia is recommended by international guidelines after cardio-circulatory arrest. However, the effects of different temperatures during the first 24 hours after deep hypothermic circulatory arrest (DHCA) for aortic arch surgery on survival and neurologic outcome are undefined. We hypothesize that temperature variation after aortic arch surgery is associated with survival and neurologic outcome. In the period 2010–2014, a total of 210 consecutive patients undergoing aortic arch surgery with DHCA were included. They were retrospectively divided into three groups by median nasopharyngeal temperature within 24 hours after rewarming: hypothermia (<36°C; n = 65), normothermia (36–37°C; n = 110), and hyperthermia (>37°C; n = 35). Multivariate stepwise logistic and linear regressions were performed to determine whether different temperature independently predicted 30-day mortality, stroke incidence, and neurologic outcome assessed by cerebral performance category (CPC) at hospital discharge. Compared with normothermia, hyperthermia was independently associated with a higher risk of 30-day mortality (28.6% vs. 10.9%; odds ratio [OR] 2.8; 95% confidence interval [CI], 1.1–8.6; p = 0.005), stroke incidence (64.3% vs. 9.1%; OR 9.1; 95% CI, 2.7–23.0; p = 0.001), and poor neurologic outcome (CPC 3–5) (68.8% vs. 39.6%; OR 4.8; 95% CI, 1.4–8.7; p = 0.01). No significant differences were demonstrated between hypothermia and normothermia. Postoperative hypothermia is not associated with a better outcome after aortic arch surgery with DHCA. However, postoperative hyperthermia (>37°C) is associated with high stroke incidence, poor neurologic outcome, and increased 30-day mortality. Target temperature management in the first 24 hours after surgery should be evaluated in prospective randomized trials.
Introduction
D
Target temperature management has recently been demonstrated to be neuroprotective in cardiac arrest survivors (Dragancea et al., 2015; Leary et al., 2015). Therapeutic hypothermia and target temperature management are now recommended during the first 24 hours in postresuscitation care after cardiac arrest (Nunnally et al., 2011; Nolan et al., 2015).
However, a possible role for target temperature management during the first 24 hours after rewarming from DHCA has never been investigated.
On the other hand, although there is a general consensus that hyperthermia should be avoided during rewarming, the consequences of postrewarming hyperthermia remain unknown (Shum-Tim et al., 1998). The development of hyperthermia in this setting is most frequently an adaptive response to cell damage, activation of inflammatory cascades, infections, or thermoregulatory dysregulation (Bar-Yosef et al., 2004).
Although some clinical studies in comatose cardiac arrest survivors found a significant association between postresuscitation hyperthermia and worse outcome, the relationship between temperature after rewarming from DHCA and clinical outcomes remains largely unclear (Bro-Jeppesen et al., 2013; Lee et al., 2015).
We sought to evaluate the influence of hyperthermia and hypothermia during the first 24 hours after rewarming from DHCA and the association of temperature variation with survival and neurologic outcome.
Materials and Methods
Study design
This was a retrospective observational cohort study of consecutive adult patients undergone aortic arch surgery with DHCA at the Division of Cardiac Surgery University Hospital of Verona in the period January 1, 2010 to December 31, 2014. Exclusion criteria were documented of suspected preoperative infections and signs of systemic inflammatory response syndrome.
Patients were divided into three groups by the median nasopharyngeal temperature within 24 hours after rewarming from DHCA: hypothermia (<36°C), normothermia (36–37°C), and hyperthermia (>37°C). The nasopharyngeal temperature was recorded hourly. There were no existing protocols on temperature management in the intensive care unit. Patients undergoing active rewarming in the intensive care unit were excluded.
Surgical and anesthetic technique
All patients underwent aortic arch replacement to treat aortic arch aneurysm or dissection. General anesthesia was performed in a standardized fashion with propofol, sufentanil, vecuronium, and isoflurane. The near-infrared spectroscopy was monitored throughout surgery. After systemic heparinization (300 IU/kg), cardiopulmonary bypass (CPB) and systemic cooling were initiated to the target temperature of 16–20°C. Acid-base management was based on pH-stat principles. Repeated administration of cold cardioplegia solution and topical cooling were used for myocardial protection. The arterial cannulation site was primarily the femoral artery, and venous cannulation was the right atrium.
On reaching the target temperature, 500 mg of thiopental was administered, the patient's head was packed in ice, and DHCA was initiated. An SCP was performed according to the surgeon's judgment (target flow, 10–20 mL/[kg·min] via bilateral carotid artery infusion).
After aortic arch repair, the aortic graft was cannulated for antegrade arterial perfusion; on commencement of CPB, the patient was warmed to 36.5°C (avoiding blood-bath gradients of >10°C) and weaned from CPB. Active rewarming was complete on reaching a nasopharyngeal temperature of 36.5°C. Perioperative blood products were transfused according to the attending physician's judgment, taking into account the patient's clinical status and available laboratory values.
Study outcome
Patient demographics and perioperative risk factors were abstracted by using medical records and recorded in an electronic database (Microsoft Access; Microsoft, Seattle, WA). The following end points were recorded for each patient: 30-day mortality, perioperative stroke incidence, and neurologic outcome assessed by the cerebral performance category (CPC) score. The CPC score reflects both mortality and morbidity (Jacobs and Nadkarni, 2009); these score values were assessed at follow-up, which was performed at least 6 months after surgery. A favorable outcome was defined as a CPC score of 1 or 2, that is, alive with good cerebral performance or sufficient cerebral function for independent activities of daily life, with or without mild neurological or psychological deficits; ability to work in a sheltered environment was considered to indicate a CPC score of 2. The CPC scores 3 to 5 were recorded as unfavorable outcomes.
To assess the effect of different postoperative temperature on transfusion requirements, bleeding determining reoperation and blood components transfused within 48 hours of surgery were recorded.
Statistical analysis
All statistical analyses were performed by using PASW/SPSS statistical software version 18 (IBM, Inc., Chicago, IL). Continuous variables were expressed as the mean ± standard deviation, and categorical (frequency) variables were expressed as percentages. Univariate logistic regression analyses were initially conducted to test for between-groups differences in patient preoperative demographics, risk factors, and preoperative medications (Table 1). Categorical variables were analyzed with the χ2 or Fisher exact tests. Continuous variables were first examined for normality of distribution: The t-test was used for those variables with normal distributions, and the nonparametric Wilcoxon rank-sum test was applied for the variables with skewed distributions. In all tests, two-tailed p-values were calculated.
CPB, cardiopulmonary bypass; DHCA, deep hypothermic circulatory arrest; PCT, procalcitonin; SCP, selective cerebral perfusion; WBC, white blood cells.
To control for demographic factors, medications, and perioperative and operative risk factors, multivariate stepwise logistic regression was performed on all patient data to determine whether hypothermia and hyperthermia were independently associated with study outcomes than with normothermia. Multivariable Cox proportional hazards models were applied after checking for underlying assumptions of linearity, proportionality, and lack of interactions and odds ratio (OR) and 95% confidence interval (CI) are reported.
Results
A total of 210 consecutive patients underwent aortic arch surgery with DHCA and were considered for the present study. Normothermia characterized the first 24 hours in the ICU in 110 patients; an additional, 65 patients were hypothermic and 35 more patients experienced hyperthermia.
Patient demographics and perioperative risk factors are presented in Table 1. Patients in the hyperthermia group had a marginally higher occurrence of SCP (p = 0.06), whereas CPB duration tended to be higher in the hypothermia group (p = 0.09). Of note, the groups did not significantly differ with respect to age, gender distribution, diabetes, history of smoking, and renal insufficiency.
Postoperative outcomes are summarized in Table 2. In-hospital mortality was 8% (9/110) in the normothermia group, 9% (6/65) in the hypothermia group, and 26% (9/35) in the hyperthermia group. Multiorgan system failure was the most common cause of death. There were five additional 30-day all-cause of death (three in normothermia, two in hypothermia, and one in hyperthermia). To determine whether hypothermia and hyperthermia were independently associated with a significantly higher risk of in-hospital death and 30-day all-cause mortality, multivariate stepwise logistic analysis was performed, controlling for patients' demographics, preoperative risk factors, and intraoperative variables (Figs. 1 and 2). Hyperthermia was independently associated with a higher risk of in-hospital death (p = 0.001) and 30-day all-cause mortality (p = 0.005) than normothermia. Hypothermia was not different from normothermia for in-hospital mortality (p = 0.2) and 30-day all-cause mortality (p = 0.1).
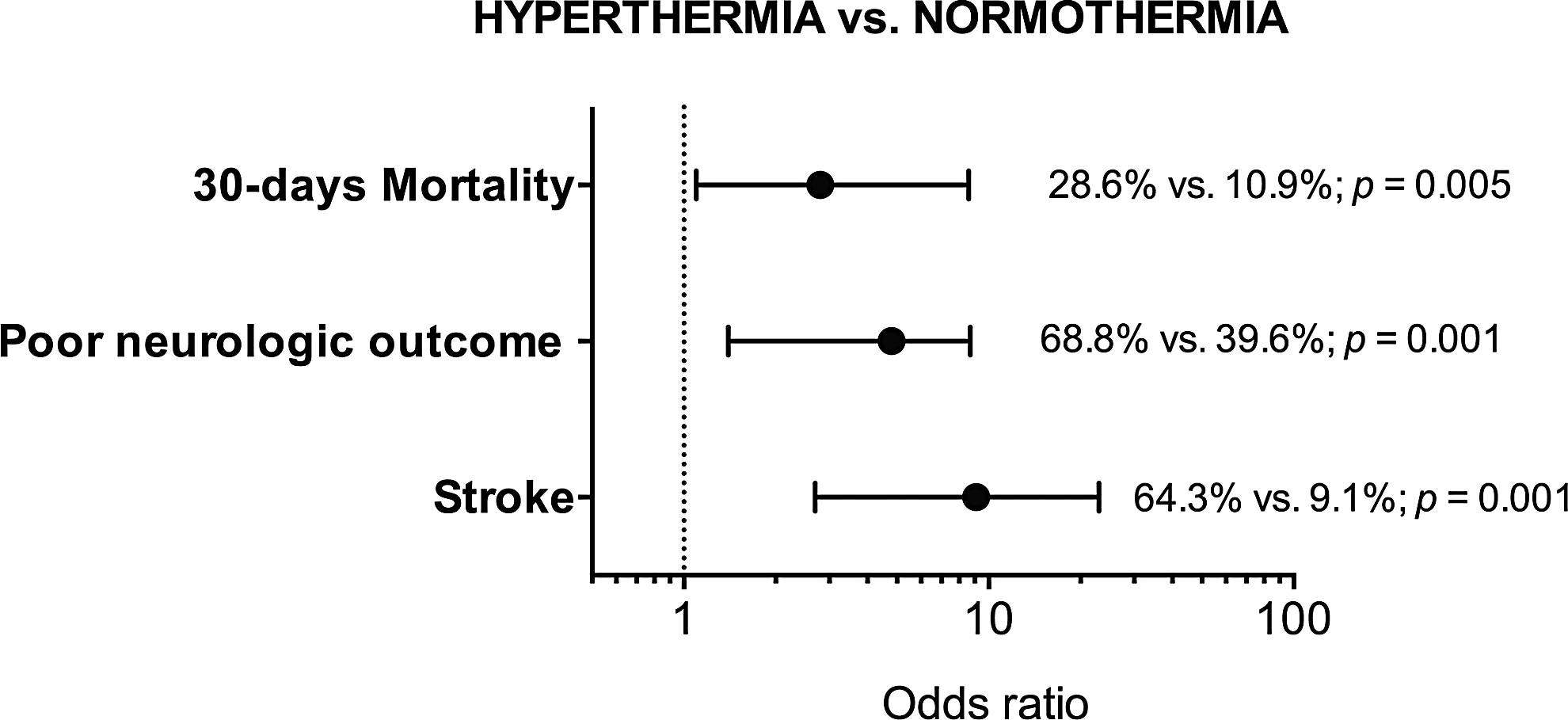
Hyperthermia group compared with normothermia group. Odds ratio and rates of the primary end points.
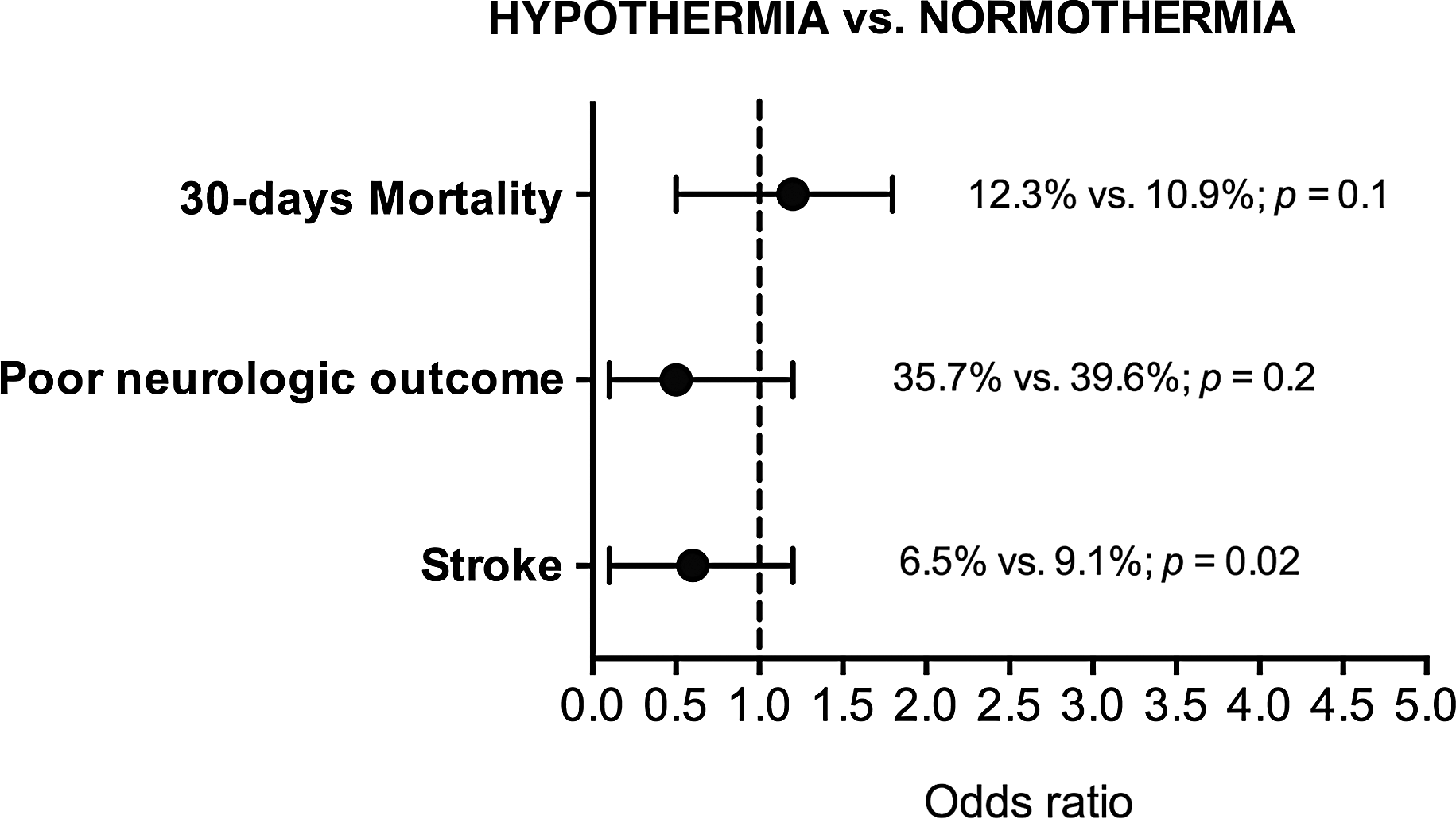
Hypothermia group compared with normothermia group. Odds ratio and rates of the primary end points.
CI, confidence interval; CPC, cerebral performance category; OR, odds ratio.
The incidence of stroke in the hyperthermia group was ninefold higher than in the normothermia group (64.3% vs. 9.1%; p = 0.001; OR, 9.1; 95% CI, 2.7–23.0). Hypothermia had a lower incidence of stroke compared with normothermia, but the difference was not significant (6.5% vs. 9.1%; p = 0.02).
Poor neurologic outcome defined as a CPC score between 3 and 5 was higher in the hyperthermia group than in the normothermia group (68.8% vs. 39.6%; p = 0.001; OR 4.8; 95% CI, 1.4–8.7.). Indeed, hypothermia was demonstrated to be neither detrimental nor preventive on poor neurological outcome compared with normothermia (35.7% vs. 39.6%; p = 0.2; OR 0.5; 95% CI, 0.1–1.3).
No significant difference was observed between groups in the amount of transfused packed red blood cells, fresh-frozen plasma, and pooled platelets (Table 3).
Discussion
Cerebral ischemia is the major pathogenic factor leading to neuronal dysfunction and death after aortic arch surgery (Shimizu et al., 2013). Since the introduction of aortic arch replacement in the 1950s by DeBakey and Cooley, the two main methods of brain protection during this procedure have been different degrees of hypothermia and adjuncts for cerebral perfusion (Tsai et al., 2013). The ideal temperature during hypothermic circulatory arrest remains unclear, and the introduction of SCP has generated a debate on whether deep hypothermia or moderate hypothermia is preferable (Linardi et al., 2016).
Most of the efforts to improve neuroprotection and general outcome in aortic arch surgery are limited to the ischemic phase. However, it is reasonable to identify at least two additional critical phases for neuroprotection. The first is reperfusion with consequent rewarming. Any neuroprotection afforded by hypothermia is counterbalanced by damage occurring during the rewarming process (Grigore et al., 2002). Indeed, brain temperature, as measured in the jugular bulb, frequently exceeds 38°C during rewarming (Cook et al., 1994). In addition, rewarming is associated with jugular bulb desaturation, which, in turn, has been associated with neurocognitive dysfunction (Croughwell et al., 1994; Kadoi et al., 2001).
The second additional critical phase of neuroprotection is the early postoperative period. The concept of target temperature management, which is nowadays recommended during the first 24 hours after cardiac arrest, has not been considered after circulatory arrest induced for aortic arch surgery.
Numerous studies, both in experimental models of cerebral ischemia and in stroke in humans, have repeatedly demonstrated the deleterious effects of hyperthermia and the protective effects of hypothermia (Chen et al., 1991; Kim et al., 1996; Rungatscher et al., 2012, 2013). The pathophysiological explanation for this deleterious effect relates to the existence of zones of ischemic but potentially viable tissue known as the penumbra. This area is vulnerable to secondary insults, and its fate greatly influences the ultimate neurological outcome (Bar-Yosef et al., 2004). Increased temperature is associated with an increased metabolic rate, potentially worsening the delicate balance between oxygen supply and demand existing in the ischemic penumbra (Wang et al., 2009). Hyperthermia is also linked with other potentially harmful effects, including accentuated release of toxic excitatory neurotransmitters, increased oxygen free-radical formation, blood-brain barrier disruption, cytoskeleton destruction, increased number of ischemic depolarizations, and increased neural intracellular lactic acidosis (Karaszewski et al., 2009; Wang et al., 2009). Even mild degrees of hyperthermia might be harmful; animal models of cerebral ischemia found that a temperature increase of as small as 1–2°C was enough to increase damage (Saini et al., 2009).
Against this background, it is plausible that cerebral hyperthermia, often accompanying the rewarming stage or the first hours after intervention, may exacerbate neurological damage after DHCA.
Theoretically, two approaches can be pursued to try to prevent rewarming-induced cerebral hyperthermia. One approach is to slow the rate of rewarming by limiting the difference between blood temperature and the water temperature in the CPB heat-exchanger apparatus. This approach reduced the incidence of jugular bulb desaturation and postoperative neurocognitive dysfunction (Grigore et al., 2009; Gordan et al., 2010). A possible disadvantage of this approach is prolongation of the rewarming stage, which may increase overall CPB time.
The second approach to prevent cerebral hyperthermia is to limit the target rewarming temperature. Traditionally, separation from bypass is attempted after normothermia has been accomplished. Although this separation temperature varies among institutions, a nasopharyngeal temperature of 36–37°C would likely be a common temperature goal. However, brain temperature during the rewarming phase has been shown to be ∼1–3°C higher than the nasopharyngeal temperature and a significant discrepancy remains well into the postoperative period (Bar-Yosef et al., 2004). Limiting the rewarming nasopharyngeal temperature to 34–35°C should, therefore, prevent cerebral hyperthermia. In fact, this approach was used in a randomized, controlled trial with a demonstrable improvement in neurocognitive function after coronary artery bypass surgery (Nathan et al., 2001). The obvious drawback with this approach is the occurrence of mild hypothermia in the first several hours after separation from CPB, especially because separation from CPB is usually accompanied by a continued decrease in temperature (referred to as after-drop) of at least 0.5°C.
In addition, hypothermia is known to reduce the activity of enzymes that are involved in platelet activation pathways and clotting factors, both of which can increase transfusion requirements after surgical intervention (Insler et al., 2000). In the present study, transfusion requirement did not differ significantly between hypothermia and normothermia groups. Similarly, there was no observed difference in the incidence of surgical re-exploration.
It should be noted that to date no recommendation for a guideline is provided regarding optimal temperature for weaning from CPB due to insufficient evidence (Engelman et al., 2015).
Excessive rewarming after DHCA may induce cerebral hyperthermia, negating the beneficial effect of the previous hypothermic period. Limiting the rewarming temperature may, thus, allow the full realization of the theoretical benefits of DHCA. Although the present study fails to demonstrate a positive association with mild hypothermia during 24 hours after intervention, hyperthermia was demonstrated to be associated with higher mortality, higher stroke incidence, and poor neurologic outcome. Mild postoperative hypothermia was not associated with increased transfusion requirements; however, it may have at least a preventive role in the insidious onset of hyperthermia.
This study was limited in that it was a retrospective cohort study from a single institution. In addition, despite the use of logistic regression models to adjust for potential confounders that may have affected outcomes, other immeasurable factors, nonetheless, may have biased the results.
To define the temperature course and to compare groups, we considered median nasopharyngeal temperature within 24 hours after rewarming and not peak values. The threshold temperature between normothermia and hyperthermia was considered to be 37°C (Zeiner et al., 2001).
From the present study, it is not possible to determine whether hyperthermia is the consequence and not a possible cause of neurologic damage. However, the aim of our study was not to focus on causes of hyperthermia after circulatory arrest but to demonstrate the association with temperature variation and outcome.
Although the cause and effect of elevated temperature on survival and neurologic recovery were not proved, it seems prudent to rigorously control temperature in the first 24 hours after rewarming.
Conclusions
Postoperative hyperthermia is independently associated with higher mortality and neurologic morbidity after aortic arch surgery with DHCA. Postoperative hypothermia is not associated with better outcome compared with normothermia. Clinical trials evaluating the efficacy of target temperature management after rewarming are needed.
Footnotes
Acknowledgment
The authors especially thank Enrico Marcotto for the technical assistance rendered in performing this study.
Author Disclosure Statement
No competing financial interests exist.