
Abstract
Therapeutic hypothermia is an established treatment in patients resuscitated from cardiac arrest. It is usually well-tolerated circulatory, but hypothermia negatively effects myocardial contraction and relaxation velocities and increases diastolic filling restrictions. A significant proportion of resuscitated patients are treated with long-acting beta-receptor blocking agents' prearrest, but the combined effects of hypothermia and beta-blockade on left ventricle (LV) function are not previously investigated. We hypothesized that beta1-adrenergic receptor blockade (esmolol infusion) exacerbates the negative effects of hypothermia on active myocardial motions, affecting both systolic and diastolic LV function. A pig (n = 10) study was performed to evaluate the myocardial effects of esmolol during hypothermia (33°C) and during normothermia, at spontaneous and pacing-increased heart rates (HRs). LV function was assessed by a LV pressure transducer, an epicardial ultrasonic transducer (wall thickness, wall thickening/thinning velocity) and an aortic ultrasonic flow-probe (stroke volume, cardiac output). The data were compared using a paired two-tailed Students t-test, and also analyzed using a linear mixed model to handle dependencies introduced by repeated measurements within each subject. The significance level was p ≤ 0.05. The effects of hypothermia and beta blockade were distinct and additive. Hypothermia reduced myocardial motion velocities and increased diastolic filling restrictions, but end-systolic wall thickness increased, and stroke volume and dP/dtmax (pumping function) were maintained. In contrast, esmolol predominantly affected systolic pumping function, by a negative inotropic effect. In combination, hypothermia and esmolol reduced myocardial velocities in systole and diastole by ∼40%, compared with normothermia without esmolol, inducing in combination both systolic and diastolic LV function impairment. The cardiac dysfunction deteriorated at increased HRs during hypothermia. Beta1-adrenergic receptor blockade (esmolol) exacerbates the negative effects of hypothermia on active myocardial contraction and relaxation. The combination of hypothermia with beta-blockade induces both systolic and diastolic LV function impairment.
Introduction
T
Moderate hypothermia is usually well-tolerated circulatory in cardiac arrest patients (Hovdenes et al., 2007), and cardiac pump function during moderate hypothermia is found to be preserved at spontaneous heart rate (HR) in experimental studies (Espinoza et al., 2013; Kerans et al., 2015). However, the motions of the myocardium change during hypothermia, that is, contraction and relaxation velocities, are reduced (Espinoza et al., 2013; Kerans et al., 2015). Due to increased diastolic filling restrictions, tolerance of pacing-induced increases in HR is also impaired during hypothermia (Espinoza et al., 2013; Kerans et al., 2015).
The significance of hypothermia-induced myocardial motion changes may be of most importance in conjunction with cardiac acting medications. In addition, postarrest tachyarrhythmia during hypothermia may be unfavorable to cardiac performance.
The combination of hypothermia with medications that block the myocardial beta1-adrenergic receptor (beta-blockers) is of particular interest. A significant percentage of resuscitated patients (28% in our University Hospital), not stated in any study to date, are treated with long-acting beta-blockers. The combined effects on left ventricle (LV) function are not, however, previously investigated.
The present experimental study aimed to investigate the effects of beta1-adrenergic receptor blockade (esmolol-infusion) on LV function during hypothermia, at spontaneous and pacing-increased HRs. We hypothesized that esmolol exacerbates the negative effects of hypothermia on active myocardial motions, affecting both systolic and diastolic LV function. In addition, we tested whether the response to increases in HR, observed during hypothermia, was further influenced by esmolol.
Methods
Overall design
A prospective controlled pig study was performed to evaluate the myocardial effects of esmolol (Brevibloc; Baxter, Deerfield, IL) during hypothermia (pulmonary artery temperature [Tpa] 33°C) and during normothermia (Tpa = 38°C, normothermia in the pig), at spontaneous and pacing-increased HRs.
Animal welfare
The experimental protocol (trial registration number: FOTS 3866) was approved by the Norwegian National Animal Research Authority and the animal experiments were performed in accordance with the European Convention for the Protection of Vertebrate Animals used for Experimental and Other Scientific Purposes (European Council, ETS No. 170). Personnel who handled the animals were certified with Federation of Laboratory Animal Science Associations category C. Detailed information according to the Animals in Research: Reporting In Vivo Experiments (ARRIVE) guidelines is presented in Supplement 1 (Kilkenny et al., 2010; Supplementary Data are available online at www.liebertpub.com/ther).
Animal preparation
Ten crossbred pigs, weight (median [range]) 49.8 (47.0–63.0) kg, were anesthetized and surgically prepared, as previously described (Kerans et al., 2015). In brief, intramuscular premedication with azaperone 3 mg/kg and ketamine 30 mg/kg with the addition of atropine 20 μg/kg was administrated in the pig enclosure, and anesthesia was maintained by intravenous morphine (1–2 mg/kg/h) and isoflurane inhalation (end-tidal concentration 1.0%–1.5%) in the operating theater without the use of muscle relaxants. Mechanical ventilation (Siemens KION 6.0; Solna, Sweden) was in volume control mode (tidal volume = 10 mL/kg, FiO2 = 40%, positive end-expiratory pressure (PEEP) = 5 cm H2O, respiratory rate = 18/min; adjusted to keep PaO2 within 20 ± 5 kPa and PaCO2 within 5.0 ± 0.5 kPa), and Ringer's acetate solution was infused at 20 mL/kg/h. A micromanometer pressure transducer (MPR-500; Millar Instruments, Houston, TX) was positioned in the LV. An epicardial ultrasonic transducer (Imasonic SA, Besançon, France) was sutured to the anterior LV wall to continuously measure wall thickness and wall-thickening/thinning velocity through the cardiac cycle (Espinoza et al., 2013; Kerans et al., 2015). The left femoral vein was cannulated by a water-circulated catheter (Cool Line; Zoll, Chelmsford, MA) positioned to the vena cava inferior and connected to a designated thermal regulation system (Coolgard 3000; Zoll) and adjusted in accordance with Tpa (Swan-Ganz CCO; Edwards Lifesciences, Irvine, CA). A 16 mm ultrasonic flow-probe (Transit Time Flow Measurement Probe; Medistim, Oslo, Norway) was placed on the ascending aorta to measure cardiac output (CO). Two pacemaker leads were attached to the right atrial appendage. The preparation took (mean ± standard deviation) 162 ± 24 min, and the experiments lasted 705 ± 58 min.
Interventions
All animals served as their own controls. The surgical preparation was followed by a 30-minute stabilization period (supine position, open chest, and pericardium) before measurements commenced. Measurements were made during normothermia and hypothermia, at spontaneous and atrial-paced HRs. Pacing was performed at 100 (HR100) and 120 (HR120) beats/min. After baseline measurements were obtained at all HRs, the measurements were repeated during infusion of 0.5 and 0.2 mg/kg/min esmolol at normothermia and hypothermia, respectively. Esmolol was the preferred beta blocker because of its short half-life. The selected dosages at normothermia and hypothermia were based on pilot experiments where esmolol was titrated to achieve an ∼15% reduction of systolic aortic blood pressure at spontaneous HR both during normothermia and hypothermia. Measurements during esmolol infusion commenced after 20 minutes infusion time.
In five animals, hypothermia was induced during the surgical preparation, and measurements were obtained at hypothermia first, followed by rewarming and corresponding measurements at normothermia.
Measurements
Systolic LV function was assessed by peak systolic LV pressure, peak systolic LV wall-thickening velocity (S′), peak LV pressure first time derivate (dP/dtmax), end-systolic LV wall thickness, and LV end-systolic pressure and stroke volume (SV = CO/HR) (Espinoza et al., 2010, 2013; Kerans et al., 2015). In diastole, the isovolumetric relaxation constant (τ) was used in accordance with Weiss as the measure of active myocardial relaxation (Weiss et al., 1976). In addition, the peak negative LV pressure derivate (dP/dtmin), LV end-diastolic wall thickness, and LV end-diastolic pressure were measured. At spontaneous HR, the early diastolic LV wall-thinning velocity peak (e′) was also measured. Systolic duration was measured from steep upstroke of dP/dt to dP/dtmin (end-systole) and diastolic duration from dP/dtmin to onset of systole. LV afterload was estimated from arterial elastance (Ea = end-systolic pressure/SV). Time for complete relaxation was defined as 3.5 times τ from end-systole and was calculated as a fraction of diastolic duration (3.5 · τ/diastolic duration) (Weisfeldt et al., 1978). In each pig, every variable was calculated as a mean from measurements in three consecutive cardiac cycles.
Statistical analyses
Data are reported as mean ± standard deviation if not otherwise stated. The data from normothermia and hypothermia (with and without esmolol, at spontaneous and paced HRs) were compared using a paired two-tailed Students t-test.
To study the effects of all interventions, the data were analyzed using a linear mixed model to handle dependencies introduced by repeated measurements within each subject. The data were analyzed using temperature level (Tpa), beta-blocker (BB) administration, and HR as determinants (factors) in a model, in which variable = β + β1 (Tpa) + β2 (BB) + β3a (HR100) + β3b (HR120) + β4 (Tpa × BB) + β5a (Tpa × HR100) + β5b (Tpa × HR120), with time of recording included as a covariate to account for the order of measurements and effects of time. Nonsignificant interaction factors and covariates were subtracted in screened models to allow the final selected model's covariance structure to present the lowest Akaike information criteria. Predicted values and residuals were inspected for goodness of model fit. Differences were considered significant if p ≤ 0.05. Statistical analyses were made using SPSS v.22 software (SPSS, Inc., Chicago, IL) and GraphPad prism 6.04 (GraphPad Software, La Jolla, CA).
Results
Recordings of good quality were obtained from all 12 interventions in every experiment, except for one animal that was euthanized and excluded from analysis during hypothermia with esmolol administration at HR120, due to acute cardiac failure.
Spontaneous HR
Effects of hypothermia
Hypothermia reduced active myocardial contraction (S′) and relaxation (τ and e′) velocities (Figs. 1 and 2), reduced peak LV pressure, reduced HR (Table 1), prolonged systolic duration (Fig. 3), and reduced afterload, but maintained SV and dP/dtmax with an increased end-systolic wall thickness. Due to the reduced HR, diastolic duration was maintained, but diastolic filling was restricted as end-diastolic wall thickness increased.
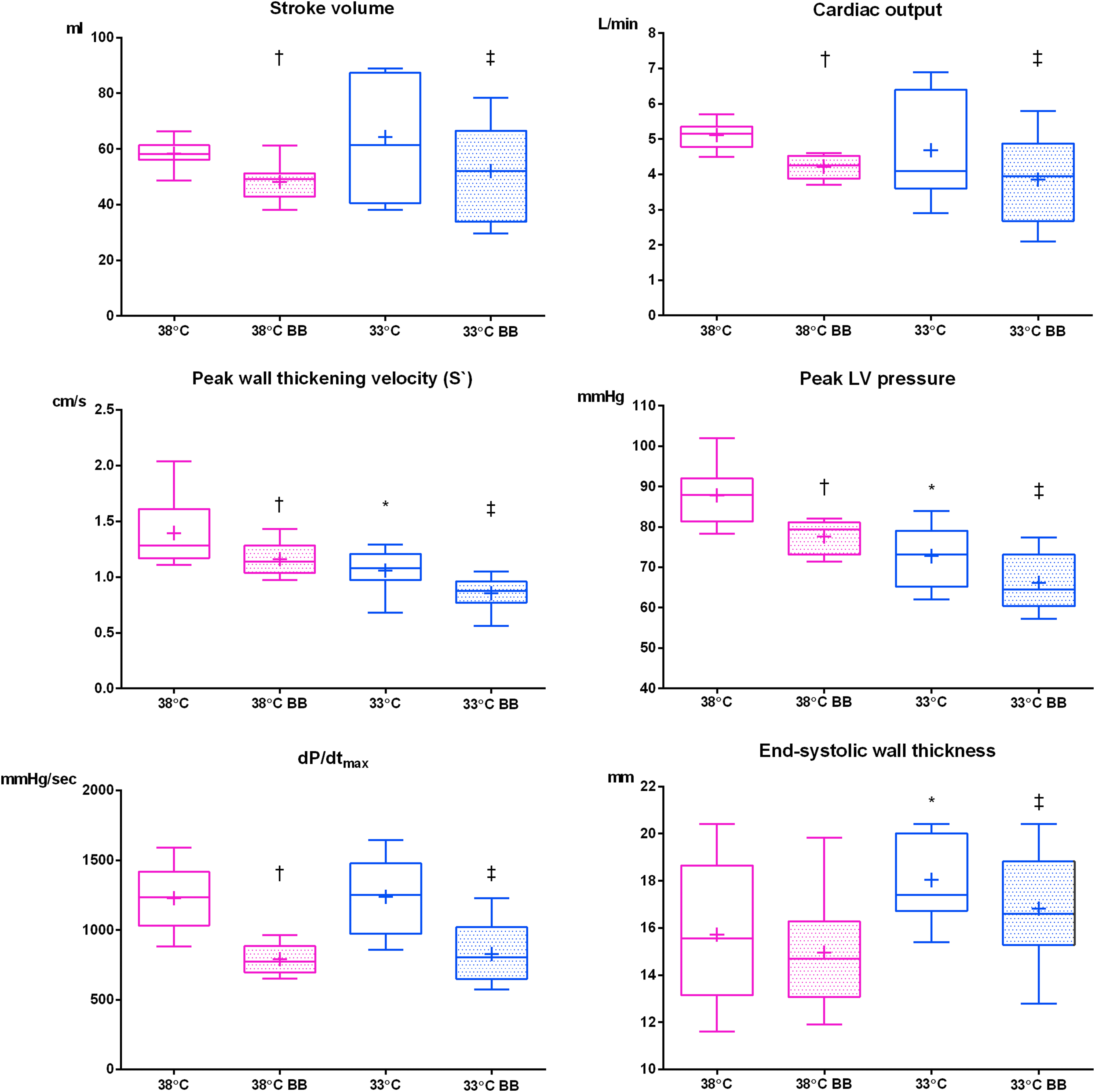
Systolic LV variables at spontaneous HR. Stroke volume, cardiac output, peak wall-thickening velocity (S′), peak LV pressure, peak LV pressure first time derivate (dP/dtmax), and end-systolic wall thickness during normothermia (38°C) and normothermia with 0.5 mg/kg/min esmolol (38°C BB), and during hypothermia (33°C) and hypothermia with 0.2 mg/kg/min esmolol (33°C BB) at spontaneous HR. The boxes extend from the 25th to 75th percentiles; line in box is plotted at the median and + at the mean; whiskers extend to the minimum and maximum values. The data were compared using a paired two-tailed Students t-test; 38°C versus 33°C (*p < 0.05), 38°C versus 38°C BB (†p < 0.05) and 33°C versus 33°C BB (‡p < 0.05). LV, left ventricle; BB, beta-blocker; HR, heart rate.

Diastolic LV variables at spontaneous HR. Isovolumetric relaxation constant (τ), peak negative LV pressure first time derivate (dP/dtmin), peak wall thinning velocity (e′), and end-diastolic wall thickness, during normothermia (38°C) and normothermia with 0.5 mg/kg/min esmolol (38°C BB), and during hypothermia (33°C) and hypothermia with 0.2 mg/kg/min esmolol (33°C BB) at spontaneous HR. The boxes extend from the 25th to 75th percentiles; line in box is plotted at the median and + at the mean; whiskers extend to the minimum and maximum values. The data were compared using a paired two-tailed Students t-test; 38°C versus 33°C (*p < 0.05), 38°C versus 38°C BB (†p < 0.05), and 33°C versus 33°C BB (‡p < 0.05).

Systolic and diastolic durations. Systolic and diastolic durations during normothermia (38°C) and normothermia with 0.5 mg/kg/min esmolol (38°C BB), and during hypothermia (33°C) and hypothermia with 0.2 mg/kg/min esmolol (33°C BB) at spontaneous HR (HRsp) and atrial-paced HRs 100 beats/min (HR100) and 120 beats/min (HR120); mean values with standard deviations. The effects of temperature (Tpa), esmolol administration (BB) and HR were analyzed in a linear mixed model, in which variable = β + β1 (Tpa) + β2 (BB) + β3a (HR100) + β3b (HR120) + β4 (Tpa × BB) + β5a (Tpa × HR100) + β5b (Tpa × HR120). β-coefficients and p-values are given for each variable.
Measurements during normothermia (38°C) and hypothermia (33°C), with esmolol infusion (38°C BB, 33°C BB) at spontaneous heart rate (HRsp) and atrial-paced heart rates 100 beats/min (HR100) and 120 beats/min (HR120). Values expressed as mean ± standard deviation. Data from 33°C versus 33°C BB compared using a paired two-tailed Students t-test, p-values are given for each variable.
BB, beta-blocker; τ, isovolumetric relaxation constant.
Effects of esmolol
Principally, the effects of esmolol were similar during normo- and hypothermia. Esmolol reduced pump function by an exclusively negative inotropic effect, as demonstrated by the reduced SV, dP/dtmax, and end-systolic wall thickness, without changes in preload (end-diastolic wall thickness) or afterload (Figs. 1 and 2). The systolic and diastolic velocities were reduced, but systolic and diastolic durations did not change (Fig. 3).
The effects of hypothermia and beta blockade were additive, with a resulting reduction of ∼40% in both systolic and diastolic velocities, compared with normothermia without esmolol. The combination of hypothermia and esmolol thus reduced both systolic and diastolic myocardial function.
Pacing-increased HRs
During normothermia, CO successively increased at HR100 and HR120 (Fig. 4).

Systolic LV variables at pacing-increased HRs. Stroke volume, cardiac output, peak wall-thickening velocity (S′), peak LV pressure, peak LV pressure first time derivate (dP/dtmax), and end-systolic wall thickness during normothermia (38°C) and normothermia with 0.5 mg/kg/min esmolol (38°C BB), and during hypothermia (33°C) and hypothermia with 0.2 mg/kg/min esmolol (33°C BB) at spontaneous HR (HRsp) and atrial-paced HRs 100 beats/min (HR100) and 120 beats/min (HR120); mean values with standard deviations. The effects of temperature (Tpa), esmolol administration (BB), and HR were analyzed in a linear mixed model, in which variable = β + β1 (Tpa) + β2 (BB) + β3a (HR100) + β3b (HR120) + β4 (Tpa × BB) + β5a (Tpa × HR100) + β5b (Tpa × HR120). β-coefficients and p-values are given for each variable.
Effects of hypothermia
Hypothermia impaired the CO response to increases in HR (Fig. 4) as the consequential SV reductions exceeded the significance of HR increments, consistent with a diastolic duration too short for complete relaxation (Fig. 5; Table 1).
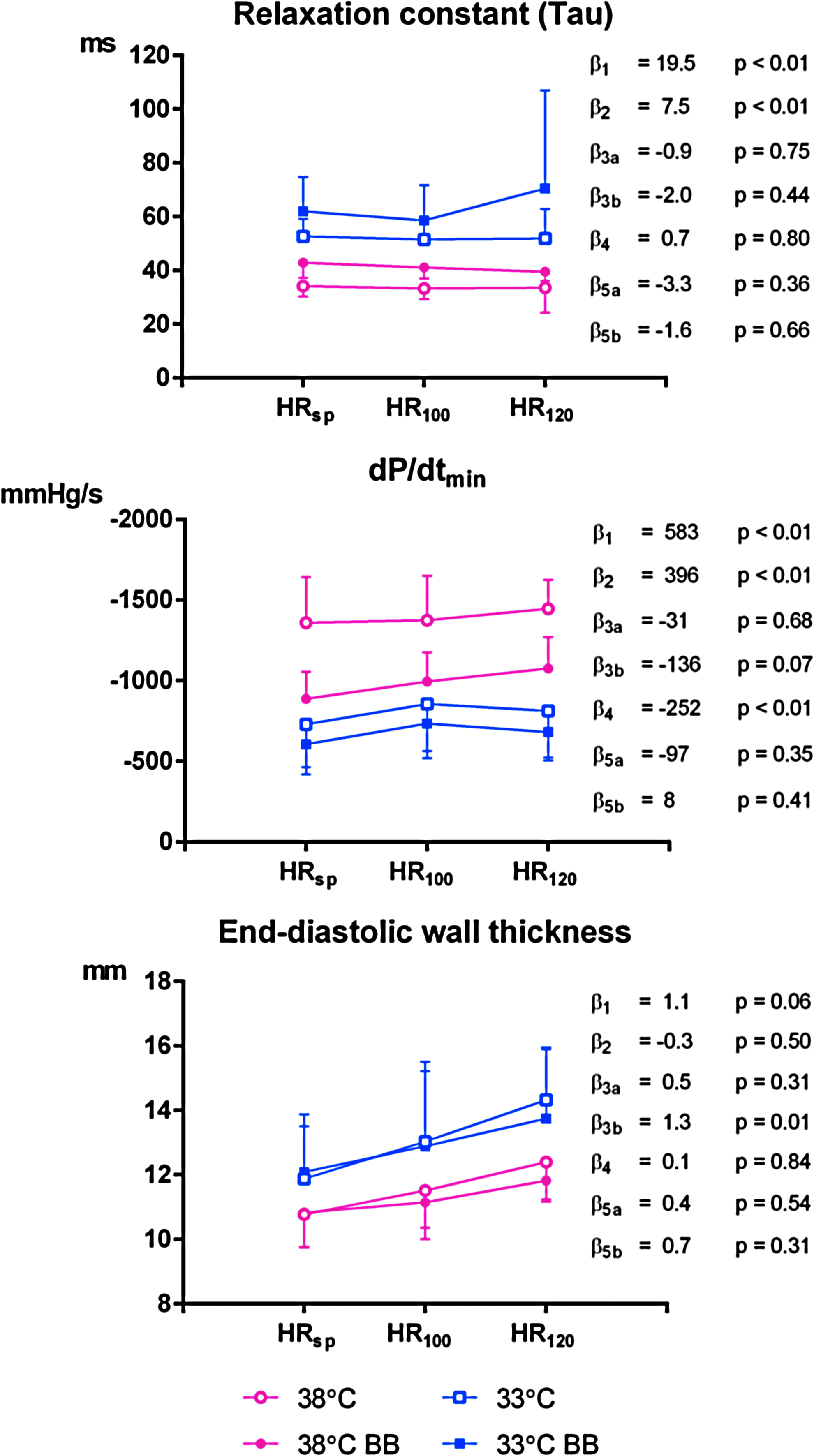
Diastolic LV variables at pacing-increased HRs. Isovolumetric relaxation constant (τ), peak negative LV pressure first time derivate (dP/dtmin), and end-diastolic wall thickness, during normothermia (38°C) and normothermia with 0.5 mg/kg/min esmolol (38°C BB), and during hypothermia (33°C) and hypothermia with 0.2 mg/kg/min esmolol (33°C BB) at spontaneous HR (HRsp) and atrial-paced HRs 100 beats/min (HR100) and 120 beats/min (HR120); mean values with standard deviations. The effects of temperature (Tpa), esmolol administration (BB), and HR were analyzed in a linear mixed model, in which variable = β + β1 (Tpa) + β2 (BB) + β3a (HR100) + β3b (HR120) + β4 (Tpa × BB) + β5a (Tpa × HR100) + β5b (Tpa × HR120). β-coefficients and p-values are given for each variable.
Effects of esmolol
The effects of esmolol were similar at spontaneous and pacing-increased HRs, with a resulting CO reduction of ∼0.8 L/min during hypothermia and 1 L/min during normothermia at all HRs (Fig. 4).
At increased HRs, the combination of hypothermia and esmolol severely impaired both systolic and diastolic LV function. Although both hypothermia and esmolol reduced relaxation velocity, and relaxation was incomplete, end-diastolic pressure did not rise (Table 1) and esmolol administration during hypothermia did not further restrict diastolic filling at increased HRs (Fig. 5).
Discussion
In the present animal study, an impairment of LV function during hypothermia with beta1-adrenergic receptor blockade is demonstrated for the first time. Both hypothermia and beta blockade reduced the velocities of myocardial contraction and relaxation, and the effects were additive.
During hypothermia, the slower contraction velocity was compensated for by a prolonged systolic duration allowing adequate time to preserve pump function (maintained SV, dP/dtmax, and increased end-systolic wall thickness) and balance the effect of increased diastolic filling restrictions. Particularly, at higher HRs, diastolic function was also affected, as diastolic duration became too short for complete relaxation.
In contrast, beta1-adrenergic receptor blockade predominantly affected systolic pumping function, and as hypothesized, exacerbated the negative effects of hypothermia. In combination, hypothermia and beta1-adrenergic receptor blockade induced both systolic and diastolic myocardial dysfunction.
During hypothermia, pacing-induced HR increments resulted in SV reductions due to filling restrictions. Esmolol did not further aggravate the response to increased HR, as esmolol mainly affected systolic function.
Postarrest cardiac dysfunction is a major cause of death in the cardiac arrest population (Laurent et al., 2002; Laver et al., 2004) and seems mainly related to impaired systolic function, although diastolic function can also be adversely affected (Cerchiari et al., 1993; Gazmuri et al., 1996; Kern et al., 1996, 1997; Bergan et al., 2015). The LV dysfunction responds to treatment with beta1-receptor agonists, such as dobutamine (Kern et al., 1997). Administration of a beta1-receptor blocking agent seems counterintuitive and could probably worsen postarrest systolic dysfunction. A reduced cardiac work load postarrest, as induced by hypothermia (Espinoza et al., 2013; Kerans et al., 2015), is reasonably beneficial to the injured or failing heart. A further reduction in work load and systolic performance, however, as induced by beta blockade, could possibly be excessive and accompanied by major side effects, such as a hypotensive low CO state with adverse organ hypoperfusion.
Cardiac function may be very vulnerable after a cardiac arrest. As many patients are treated with long acting beta-blockers prearrest, the combination of hypothermia and beta1-adrenergic receptor blockade is a relevant clinical issue. Such treatment prearrest may interact with hypothermia, requiring extra caution by the clinicians.
According to a targeted temperature management (TTM) trial, the outcome after postarrest hypothermia treatment targeting 36°C is similar to a target of 33°C (Nielsen et al., 2013), which also is found to apply to patients admitted in cardiac shock (Zobel et al., 2012; Schmidt-Schweda et al., 2013; Annborn et al., 2014). Hence, in patients treated with beta-blockers prearrest, a temperature target of 36°C postarrest may be considered a safe and cautious approach. Furthermore, one might consider postponing any initiation of beta-blocker medication postarrest, until the period of hypothermia treatment is completed.
In the present study, cardiac dysfunction deteriorated at increased HRs during hypothermia. Accordingly, the frequently occurring tachyarrhythmia in patients postarrest may be unfavorable to their cardiac performance, requiring prompt treatment such as electroconversion. In need of medications, a cautious administration of an antiarrhythmic drug that does not further negatively affect myocardial function may be preferred.
Finally, esmolol is proposed as a cardioprotective drug related to cardiac arrest (Cammarata et al., 2004; Killingsworth et al., 2004; Zhang and Li, 2013), and also during cardiac surgery (Laub et al., 1996; Geissler et al., 2001; Dahle et al., 2015) and in conjunction with coronary reperfusion treatment of myocardial infarction (Geissler et al., 2000; Booth et al., 2002). With hypothermia involved in such treatments, attention to the negative effects of hypothermia combined with beta1-adrenergic receptor blockade on myocardial function is advised.
Limitations
The myocardial effects of moderate hypothermia are assumed to be reversible (Espinoza et al., 2013; Kerans et al., 2015), and although the effects of esmolol are rapidly offset when administration is discontinued (Angaran et al., 1986), the mixed model analysis revealed a minor intervention order dependency regarding absolute values of certain LV function variables. The effects of esmolol, however, did not relate to time or temperature level order.
Due to the long rewarming period (∼2–3 hours), a persistent beta blockade as a result of the reduced esmolol metabolism during hypothermia (Melendez et al., 1990) seems unlikely, but cannot be excluded.
At the given esmolol dosage, pig heart-rate was not reduced. In a previous study, a single injection of 100 mg (i.e., 2 mg/kg) esmolol only slightly reduced HR (Espinoza et al., 2010). Although esmolol affects blood pressure more than HR even in humans, the response to esmolol seems to vary among different species. A reduced HR could influence the diastolic filling restrictions. On the contrary, esmolol made it possible to compare myocardial effects at unchanged spontaneous HR. Other beta-receptor blocking agents, possibly affecting HR differently, were considered less suitable due to the longer half-life.
In the present study, the anesthesia—despite being easily adjustable and intended to reduce the sympathetic response to hypothermia—could possibly affect the cardiovascular system differently during hypothermia and normothermia. Postarrest hypothermia with deep anesthesia, including opiates, is, however, in routine clinical use.
Conclusions
In the present animal study, beta1-adrenergic receptor blockade (esmolol) exacerbated the negative effects of hypothermia on active myocardial contraction and relaxation. The effects of hypothermia and beta blockade were distinct and additive inducing in combination both systolic and diastolic LV function impairment.
Ethics Approval
The experimental protocol (trial registration number: FOTS 3866; registered November 7, 2011) was approved by the Norwegian National Animal Research Authority and the animal experiments were performed in accordance with the European Convention for the Protection of Vertebrate Animals used for Experimental and Other Scientific Purposes (European Council, ETS No. 170).
Availability of Data and Materials
Data supporting the findings are presented in the article.
Footnotes
Acknowledgments
The authors thank the staff at the Intervention Center for assistance during the experiments as well as the animal research veterinary and the staff at the Department of Comparative Medicine for care of the animals. This work was performed at the Intervention Center at Rikshospitalet, Oslo University Hospital. The costs of the experiments were supported by departmental funds from the Intervention Center and the Department of Research and Development, Oslo University Hospital, and an additional grant was received from John and Inger Astrup Fredriksen's health fund.
Authors' Contributions
H.A.B.: study design, data collection, data analyses, and article preparation; P.S.H.: study design, data collection, data analyses, and revision of article; A.E.: study design, data collection, data analyses, and revision of article; V.K.: study design, data collection, and revision of article; H.S.: study design, data collection, revision of article; E.F.: study design and revision of article; J.F.B.: study design, data collection, data analyses, and article revision. All authors: read and approved the final article.
Author Disclosure Statement
All authors are employed by Oslo University Hospital. The authors declare that no competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.