
Abstract
Targeted temperature management (TTM), or therapeutic hypothermia, is one of the most potent neuroprotective approaches after ischemic and traumatic brain injuries. TTM has been applied clinically with various methods, but effective achievement and maintenance of the target temperature remain challenging. Furthermore, timing of cooling and target body and brain temperature to optimize effectiveness for neuroprotection and to minimize side effects are yet to be standardized. Focal brain cooling is a potential strategy to minimize adverse effects of systemic TTM. In this study, we report on a focal brain cooling device for animals and its effectiveness of focal cooling in several animal models of ischemic cerebral stroke. A focal brain cooling device was constructed using a Peltier's element, a thermoelectric heat pump. The device was validated for its cooling ability, and optimal settings to induce an effective intracranial temperature were determined using male Sprague-Dawley rats. Transient and permanent middle cerebral artery occlusions were experimentally induced, and focal brain cooling was applied using the device varying the timing and duration of cooling. The stroke-induced infarct and edema volumes were evaluated from Nissl-stained cryosections. The focal brain cooling device was able to decrease and subsequently maintained cerebral hypothermia in free-moving rats without altering the core temperature. The device with validated intracranial temperatures produced neuroprotective effects in the acute phase of ischemic neural death, reperfusion injury, progressing damage to the penumbra, and edema formation. In conclusion, our validated focal cooling device enabled rapid and accurate cerebral TTM in rats. Using this device, we were able to test the neuroprotective effect of focal TTM in several pathological stages of cerebral ischemia, which warrants further studies to develop clinically feasible TTM procedures for patients with cerebral stroke.
Introduction
Targeted temperature management (TTM), or therapeutic hypothermia, after ischemic or traumatic brain injuries is one of the most potent neuroprotective approaches known to date, since it influences multiple metabolic and molecular events following ischemia (Yenari and Han, 2012; Perman et al., 2014). The conventionally used methods induce general hypothermia in stroke patients by using external cooling, such as cooling blankets and cold water immersion, and internal cooling, for example, through venous catheters (Andresen et al., 2015). Disadvantages of external cooling methods are slow cooling to achieve the desired temperature and difficulty to accurately maintain the target temperature. Internal cooling achieves target temperature faster (Steinberg et al., 2004), whereas both external and internal methods can cause shivering or other adverse effects due to the body's responses to heat loss. Accordingly, focal brain cooling may be an optimal approach to achieve TTM promptly and to avoid adverse effects.
Although considered to be effective, the mechanisms of hypothermia-induced neuroprotection in patients remain to be fully clarified, improvement of functional outcome is to be confirmed, and clinical procedures are to be standardized (Harris et al., 2012). Therefore, preclinical animal experiments are indispensable to investigate the effect of timing of cooling, target body and brain temperature, and adverse effects and effectiveness for neuroprotection. Systemic cooling demonstrated efficacy in an experimental ischemic stroke (Clark et al., 2008, 2009), but it is challenging to achieve a desired temperature stably counteracting the body's thermoregulatory system and the procedure is stressful to animals (Vieites-Prado et al., 2016). Accordingly, several focal cooling devices have been developed and yielded varied neuroprotective effects (Clark and Colbourne, 2007; Fingas et al., 2007; Clark et al., 2009; Fujioka et al., 2010a; Silasi and Colbourne, 2011; He et al., 2013; Lu et al., 2016).
In the present study, we constructed a focal brain cooling device, which can lead to rapid and controlled brain cooling in free-moving rats without altering the core body temperature. Using this device, the neuroprotective effect of hypothermia was investigated in rat models of transient and permanent middle cerebral artery occlusion (tMCAO and pMCAO), varying timing and duration of focal brain cooling, under anesthesia and free-moving conditions.
Materials and Methods
Animals
All experimental procedures were approved by the Institutional Animal Use Committee at Kurume University and were performed in accordance with institutional guidelines for animal use. Male Sprague-Dawley rats (280–350 g; n = 82 in total) were purchased and housed in groups of 4–6 animals per case before surgery or singly after surgery with ad libitum access to feed and water. All surgical procedures were done under anesthesia: sevoflurane was used for induction and maintenance (at 5% and 2.5%, respectively) in a carrier gas of 30% oxygen and 70% nitrogen.
Focal cooling
Focal brain cooling was applied by the device, constructed in our laboratory (Neuroanesthesia Research Laboratory, Kurume University) using a Peltier's element (Fig. 1A; FerroTec, Tokyo, Japan). The Peltier's element consists of N-type and P-type semiconductors connected in series (Fig. 1A); when a voltage is applied, heat is transported from one side to another, in an electric current direction-dependent manner (Fig. 1B). The cooling device was constructed with a thermometer, Peltier's element, and tubes for water circulation along with a water pump combined with a water cooling device to prevent extreme temperature increases on the heat-releasing side of the Peltier's element while it provides constant cooling (Fig. 1C inset). The temperature of the Peltier probe was precisely controlled using a commercially available proportional integral differential controller. Under anesthesia, animals were fixed at the stereotaxic apparatus and the skull was exposed. The skull was thinned using an electric drill (4 mm in diameter, −3 mm AP, and 3 mm ML from the bregma) unless this had already been done earlier for pMCAO surgery (Fig. 1D). The Peltier device was placed on the thinned skull surface. For the free-moving experiment, the probe was fixed with three screws and dental cement. All cooling was done by setting the Peltier probe at 15°C to achieve a neuroprotective brain temperature of 33°C, unless otherwise stated. Apparent behavioral signs for cooling-induced adverse effects, including shivering and activity changes, were monitored throughout the experiment. Rewarming was achieved spontaneously by removing the device, without regulating the rewarming rate.
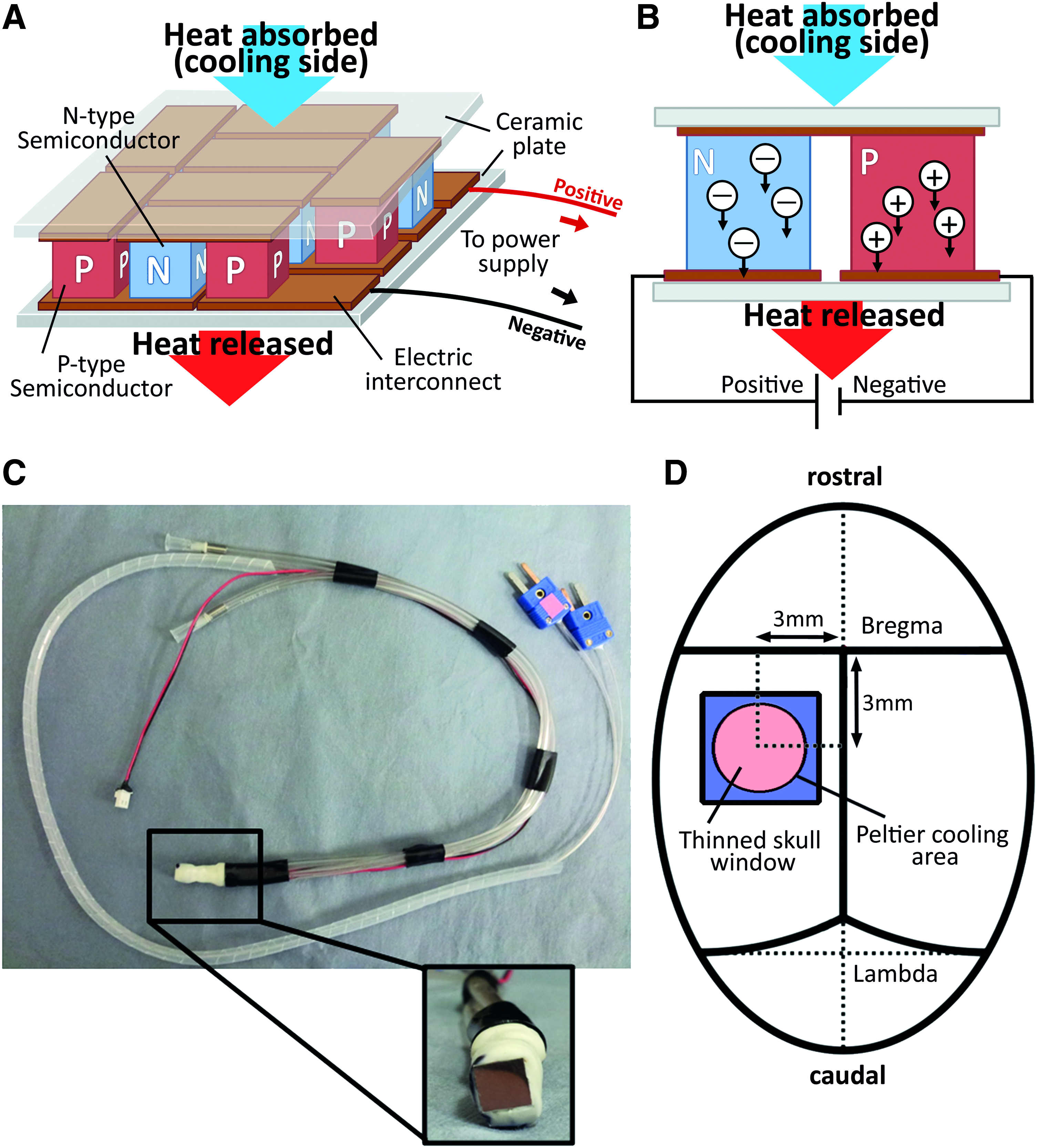
Peltier cooling device.
Determination of optimal temperature setting and monitoring of temperature maintenance
To validate focal cooling, animals were anesthetized, a small cranial window through the skull was created on the ipsilateral side, and a thermometer probe was inserted to measure striatum temperature (ML4 mm, AP0 mm, DV5 mm) (n = 3). The temperature was continuously recorded using LabChart software (ADInstruments, Nagoya, Japan) for each rat. The temperature setting of the Peltier device ranged from −5°C to 23°C and brain and rectal temperatures were recorded to find the optimal setting of Peltier device to produce a brain temperature of 33°C. After determining the optimal temperature setting, we observed the time course of the cooling in anesthetized rats (n = 3). An additional burr hole was made into the skull and a probe was inserted to measure cortex temperature (ML4 mm, AP-6 mm, DV2 mm). Animals were kept up to 60 minutes to assure temperature stabilization, and the Peltier device was then activated for 120 minutes.
Experiment 1: Intra- and postocclusion cooling in the tMCAO model
Animals (n = 39) were randomly allocated into three groups (No cooling, Intra-MCAO cooling, and Post-MCAO cooling; Fig. 2A). Animals were anesthetized and body temperature was maintained at 37.0°C using a rectal probe and a heat pad (Unique Medical, Tokyo, Japan). A rectangular probe for the laser Doppler flowmetry (Unique Medical) was inserted under the temporal muscle over the temporal cortex to monitor the cerebral blood flow (CBF) (Harada et al., 2005). Rats were then subjected to tMCAO using a standard intraluminal filament model (Koizumi et al., 1986). A silicone-coated 30 mm 4–0 nylon monofilament (Doccol Corp., Sharon, MA) was inserted into the right internal carotid artery through a small incision at the common carotid artery. Only animals showing >70% reduction in CBF versus baseline were included in the analyses. Following tMCAO for 90 minutes, the filament was removed to allow reperfusion. For the Intra-MCAO cooling group, focal cooling was applied throughout the 90 minutes of tMCAO under anesthesia. For the Post-MCAO cooling group, focal cooling was applied immediately to 8 hours after filament removal under free-moving conditions. All animals were sacrificed 24 hours post-pMCAO and brains were collected for evaluation.
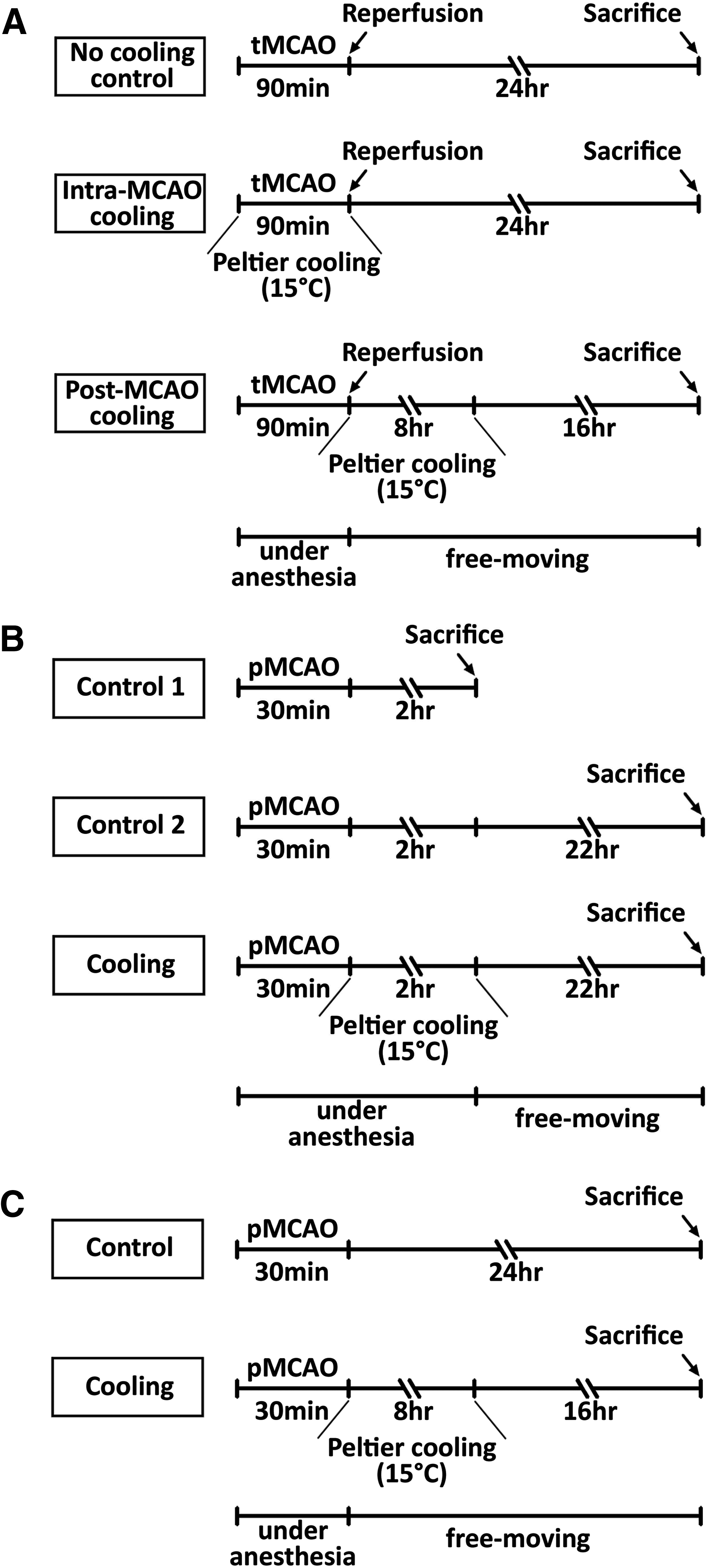
Timeline of the experiment 1
Experiment 2: Short-term postocclusion cooling in the pMCAO model
Animals (n = 22) were randomly allocated into three groups (Control 1, Control 2, and Cooling; Fig. 2B) Animals were anesthetized as described for Experiment 1 above and were subjected to pMCAO using a photothrombosis method (Fujioka et al., 2010b; Schmidt et al., 2012). A catheter was placed in the left femoral vein and the animal was fixed in the stereotaxic apparatus. The skull was exposed and thinned as described in the section on focal cooling. The thinned skull was illuminated with a green cold light source for 30 minutes to induce thrombosis at a small, defined area within the MCA territory. At the beginning of the illumination, rose Bengal dye was injected from the femoral catheter (1.3 mg/100 g body weight in 0.9% sterile saline). For Control 1 group, animals were left under anesthesia for another 2 hours after the completion of the illumination and were then sacrificed for brain collection. For Control 2 group, animals were allowed to recover for a further 22 hours and were then sacrificed to determine the size of the lesion being developed in the recovery time, by comparing with the Control 1 group. For Cooling group, focal cooling was applied for 2 hours after pMCAO under anesthesia. After the cooling device was removed, animals had a recovery period for 22 hours before being sacrificed 24 hours post-pMCAO for brain collection.
Experiment 3: Long-term postocclusion cooling in the pMCAO model
Animals (n = 15) were randomly allocated into two groups (Control and Cooling; Fig. 2C). Both groups were subjected to pMCAO for 30 minutes followed by 24 hours of recovery. Animals in the Cooling group received focal cooling for 8 hours. Because the cooling time is rather long, it was carried out under free-moving conditions. All animals were sacrificed 24 hours post-pMCAO and brains were collected.
Lesion evaluation
Infarct induced by tMCAO or pMCAO was morphometrically quantified. After experimental stroke induction and predefined survival time (Fig. 2), animals were sacrificed by decapitation and brains were promptly collected. The collected brains were fixed in 4% paraformaldehyde overnight. Serial coronal brain cryosections (20 μm in thickness) were prepared at intervals of 100 μm (Experiment 2), 200 μm (Experiment 3), or 500 μm (Experiment 1), and stained with cresyl violet (Nissl staining). The sections were photographed under a microscope and the areas of lesion and ipsilateral and contralateral hemispheres were determined using ImageJ 1.45 software (NIH, Maryland). Mean areas were calculated for adjacent slices, multiplied by the interval distance, and summed to determine the total infarct volume. In Experiment 1, edema volume was estimated as the volume increase in the affected hemisphere, expressed as percentage of whole-brain volume, which was estimated from the unaffected hemisphere. Assuming that both hemispheres are equal in volume and the volume increase occurs only in the affected area due to edema, lesion volume was corrected by subtracting edema volume. The results were statistically analyzed using one-way ANOVA followed by Tukey's post hoc test for Experiments 1 and 2, and t-test for Experiment 3.
Results
The focal cooling device effectively decreased brain temperature without changing core temperature
Using healthy animals, the capability of the Peltier device to reduce brain temperature was investigated. The striatal temperature (Fig. 3A blue) dropped along with the decreased temperature of Peltier device. The core temperature was successfully maintained unchanged (Fig. 3A red). When the Peltier probe was set at 15°C, brain temperature was at the most effective temperature for neuroprotection (33.20°C ± 0.90°C; mean ± SEM). Thus, the Peltier probe was set with a constant temperature of 15°C and we examined the temperature change of the body, striatum, and cortex by a 2-hour cooling. The cooling of the brain was rapidly achieved after cooling began (Fig. 3B) and the temperature was stable around 33°C for 2 hours (striatum 33.90 ± 0.05 and cortex 33.66 ± 0.05; mean ± SEM) without changing body temperature (37.15 ± 0.00). Striatum and cortex temperatures did not differ significantly. Throughout the experiments, no signs for cooling-induced behavior were observed.
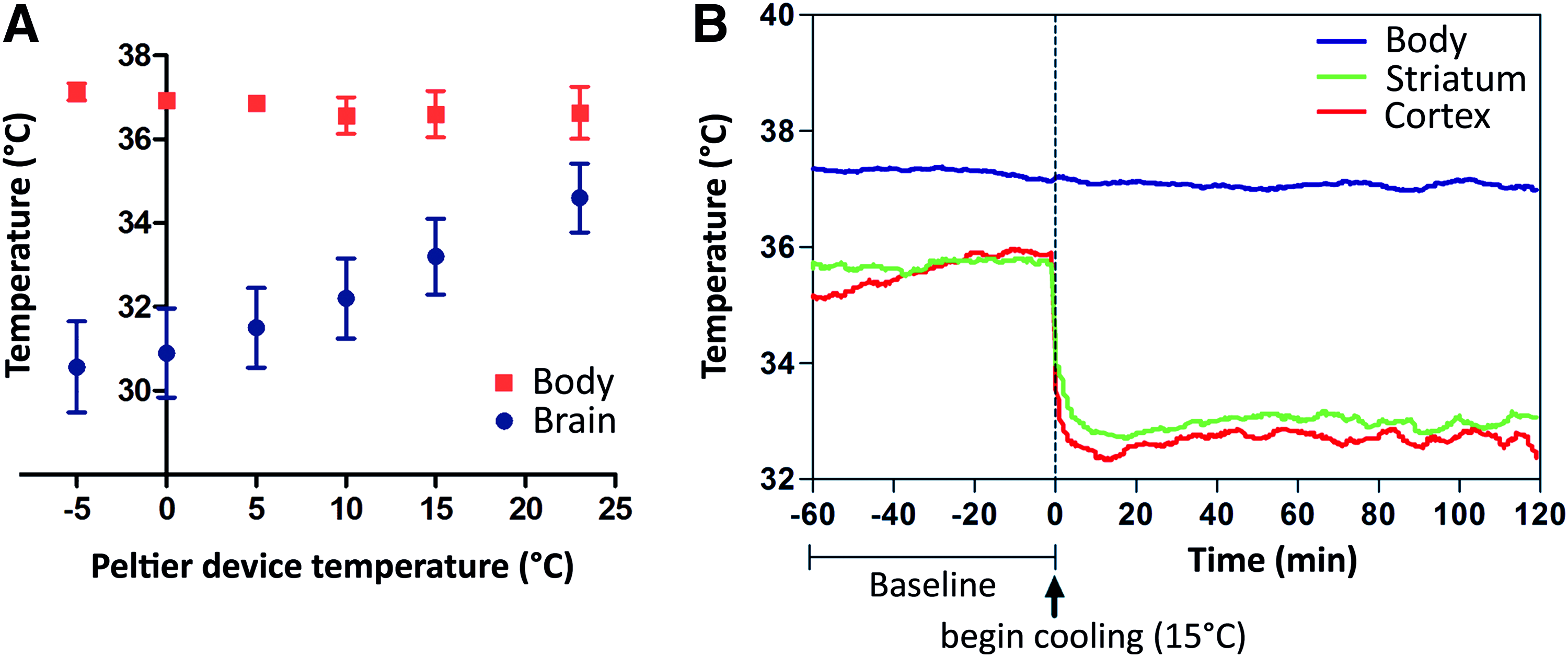
Validation of the Peltier cooling device.
Intra- and post-MCAO cooling decreased lesion volume in tMCAO (Experiment 1)
Effects of intra- and postocclusion focal cooling in tMCAO were investigated using the filament-induced tMCAO model (Fig. 2A). A total of 39 animals underwent surgery and MCAO was successfully induced in 34 animals. Before the intended evaluation time point, 11 of these animals died, and the percentage of deaths in each treatment group was not significantly different (p = 0.96; chi-square test). The number of animals analyzed were n = 7 for Intra-MCAO cooling, n = 8 for Post-MCAO cooling, and n = 8 for No cooling control groups. MCAO reduced CBF to 22.29% ± 1.82% (mean ± SEM) of the baseline, and returned to 75.75% ± 4.91% with reperfusion. At both intra- and post-MCAO, CBF was not influenced by cooling (p = 0.45 and 0.12, respectively, one-way ANOVA). Intra-MCAO cooling significantly decreased the lesion volume compared with No cooling control (p < 0.05) (Figs. 4A, B). The Post-MCAO group showed tendency to decrease lesion volume: neither the difference with No cooling control group nor the difference with Intra-MCAO cooling group was statistically significant (p > 0.05; Fig. 3C). Our results indicate that focal cooling is neuroprotective against damage caused by occlusion (Intra-MCAO group), and probably also against reperfusion damage (Post-MCAO group). Edema volume was significantly reduced in both Intra- and Post-MCAO groups compared with the No cooling control group (p < 0.01 for both) (Fig. 4C).

Experiment 1: Neuroprotective effect of focal cooling in tMCAO model.
Short-term cooling after pMCAO did not show beneficial effect on lesion size (Experiment 2)
Next, we used the pMCAO model induced by photothrombosis to investigate the effect of cooling exclusively on the occlusion damage observed in Experiment 1 (Fig. 2B; n = 22 in total; n = 7 in each group analyzed; one animal in Control 1 group died during the surgical procedure). In this pMCAO model, lesions were significantly smaller at the 2-hour time point than after 24 hours post-pMCAO induction (Fig. 5A, B; Control 1 vs. Control 2; p < 0.001). The chronological difference in lesion volume was interpreted as representing penumbra. Peltier cooling was applied for 2 hours following pMCAO induction to investigate its protective effect in tissues in penumbra, but lesion volume was not affected (Fig. 2; Control 2 vs. Cooling; p > 0.05).
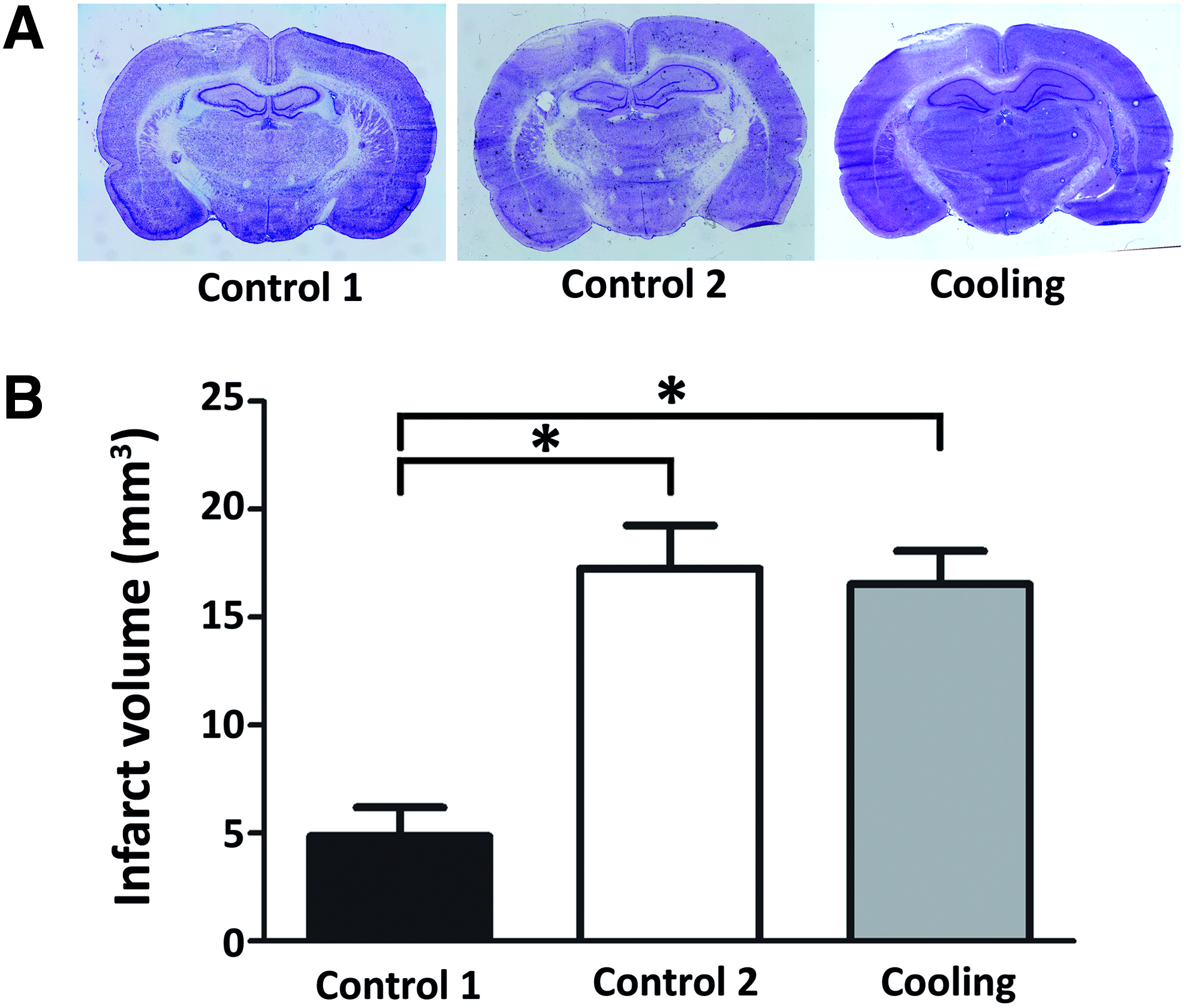
Experiment 2: Neuroprotective effect of short-term focal cooling in pMCAO model.
Long-term cooling after pMCAO decreased lesion size (Experiment 3)
In Experiment 3, 15 animals were subjected to pMCAO and either long-term focal cooling (8 hours; n = 8) or no cooling procedures (n = 7) under free-moving conditions immediately after pMCAO induction (Fig. 2C). One animal in the focal Cooling group died before the evaluation point. The 8-hour cooling showed significantly smaller lesion volume than the Control group (p < 0.0001) (Fig. 6A, B). Unlike Experiment 2, anesthesia was terminated immediately after pMCAO induction in Experiment 3. The lesion volume was significantly greater in Control group of Experiment 3 than Control 2 of Experiment 2 (24.34 ± 1.21 and 17.26 ± 2.00, respectively; p = 0.0103, t-test). Cooling group in Experiment 2, which was not different in lesion volume compared with Control 2 in Experiment 2, had a significantly smaller lesion volume than the Control group in Experiment 3 (16.54 ± 1.52 and 24.34 ± 1.21, respectively; p < 0.0017, t-test), implying a neuroprotective effect of 2-hour post-MCAO anesthesia in Experiment 2.
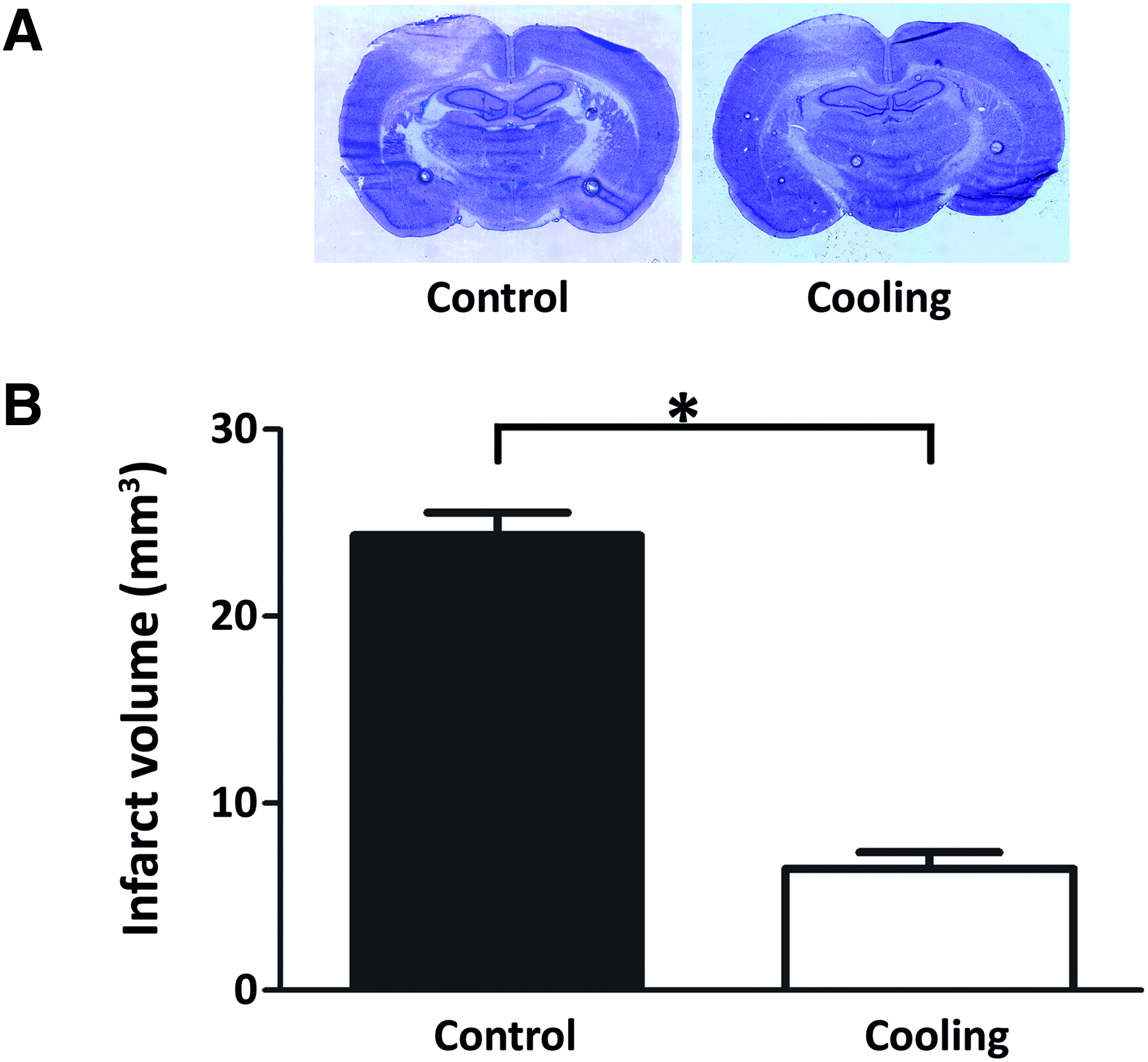
Experiment 3: Neuroprotective effect of long-term focal cooling in pMCAO model.
Discussion
In this study, we demonstrated that the Peltier cooling device induced focal brain cooling with accurate temperature control in rats. We found that the Peltier device-induced focal brain cooling had neuroprotective effects in the acute phase of ischemic neural death, and against reperfusion injury, progressing damage to the penumbra, and edema formation.
The device rapidly reduced the brain temperature to the target level and enabled long-term focal cooling under free-moving conditions. Our study confirmed that a brain temperature of 33–34°C, which is most neuroprotective in experimental cerebral ischemia (Kollmar et al., 2007), was neuroprotective. In addition, no apparent behavioral signs for cooling-induced adverse effects were observed. In a previous study, Peltier device-induced hypothermia with the same principle showed positive effects on experimentally induced seizure or nociceptive pain (Fujioka et al., 2010a). The neuroprotective effect is possibly due to suppressed electrical activity in neurons, demonstrated in a seizure model as suppressed epileptic discharges in electrocorticography (Fujii et al., 2012).
Ischemia causes acute irreversible neuronal damage in the ischemic core. In strategies to preserve brain functions after ischemic stroke, interest has turned toward protecting penumbra, defined as the brain area surrounding ischemic core, where tissue is affected by ischemia but still viable if promptly treated (Astrup et al., 1981). In cerebral ischemia, rescuing the penumbra tissue is as important as minimizing the acute damage.
In the tMCAO model, intra-MCAO cooling produced more effective neuroprotection than post-MCAO cooling (Fig. 3C). This finding is consistent with the view that cooling at the acute phase of ischemia suppresses propagation of neuroelectrical instability (Ding et al., 2009), resulting in suppression of acute damage in the ischemic core, and TTM at this time point is critical for neuroprotection. Nonetheless, the Post-MCAO cooling group in Experiment 1 showed a tendency toward reduced lesion volume, although not to the same extent as intra-MCAO. We consider that protective effects of postischemic TTM during and after reperfusion against reperfusion injury and progressive damage in the ischemic penumbra are plausible. Notably, edema volume was significantly reduced in both Intra- and Post-tMCAO cooling groups. It is possible that the mild neuroprotection is due to cooling-induced edema suppression.
The photochemically induced pMCAO model produces the ischemic insult but no reperfusion insult. Our investigations in pMCAO model allowed a focus on the cooling effect against ischemic insult alone. It has been argued if there is a penumbra in the pMCAO model, because no reperfusion occurs (Labat-gest and Tomasi, 2013). Grome et al. argue that the growth of the ischemic lesion completes within 4 hours and apparent enlargement of the lesion thereafter is merely due to increased water content, not progressive neuronal death in penumbra (Grome et al., 1988). We observed a greater lesion volume in rats with 24-hour survival than in those with only 2-hour survival time in Experiment 2 (Control 1 vs. Control 2; Fig. 5B). We consider this difference in lesion volume to represent ischemic penumbra, in line with other studies demonstrating lesion enlargement up to 24 hours (Kuroiwa et al., 2009; Fujioka et al., 2010b). Therefore, we conclude that the reduced lesion volume observed in Experiment 3 was due to cooling-induced neuroprotection.
Short-term cooling apparently did not promote neuroprotection in pMCAO rats (Experiment 2; Fig. 5B). However, the detection of a cooling effect may have been complicated by the use of sevoflurane, a volatile anesthetic with a known neuroprotective effect (Kitano et al., 2007; Adamczyk et al., 2010; Ren et al., 2014). The Control 2 group in Experiment 2 showed significantly smaller infarct volume compared with the Control group in Experiment 3. The only difference between the two control groups was the 2-hour postoperative anesthesia in Control 2 in Experiment 2 (Fig. 2B, C). Accordingly, the neuroprotective effect of cooling may have been undetectable due to the neuroprotection by anesthesia in Experiment 2. In the absence of sevoflurane, long-term cooling in Experiment 3 had a marked neuroprotective effect (Fig. 6B), which suggests that postischemic TTM requires long-term cooling, as suggested in previous reports (Clark et al., 2008, 2009).
In the present study, we analyzed the influence of focal cooling on neuronal death with 8 hours as the longest cooling duration. However, changes in excitability in surviving neurons surrounding the ischemic lesion continue developing long after lesion induction, and such changes may underlie the functional deficits observed after stroke (Schiene et al., 1996; Fujioka et al., 2010b). Therefore, focal cooling in excess of 8 hours may be needed for optimal neuroprotection. Furthermore, it has been reported that a postischemic cooling-induced neuroprotective effect that was evident 3 days postischemia disappeared within 2 months (Dietrich et al., 1993). We evaluated lesion volume at time points up to 24 hours post-MCAO, and we can thus draw no conclusion on the long-term neuroprotective ability of focal cooling. Further investigation is required as to whether longer cooling therapy has more positive impact on these neurons, as demonstrated in a previous study that 48-hour TTM was more neuroprotective than shorter TTM durations in rats after pMCAO (Clark et al., 2008). In addition, two other important issues were not addressed in our study: neuromotor function and rewarming rate. In particular, rewarming rates can influence outcomes of hypothermia-induced neuroprotection (Matsushita et al., 2001; Suehiro et al., 2003; John and Colbourne, 2016) and had the potential to interfere with the results in this study. Further studies are required to elucidate the durability of hypothermia-induced neuroprotection and whether functional recovery accompanies, as well as an optimal rewarming rate to maximize cooling benefit.
Peltier cooling device possesses a number of advantages over other cooling methods for research in experimental animals: prompt achievement of target temperature, focal cooling with a relatively small temperature gradient, and the feasibility for long-time use under free-moving conditions with normal body temperature. Peltier cooling device also overcomes potential interference in the lesion evaluation from neuroprotective volatile anesthesia and adverse effects associated with whole-body hypothermia. In addition, research with the Peltier cooling device may provide new insights into the focal brain hypothermia-induced neuroprotection, especially in the field of ischemic stroke, where translation of knowledge obtained from animal research to clinical practice is currently unsatisfactory.
The Peltier's element-based thermoelectric cooling has been demonstrated to produce a relatively small temperature gradient and not to affect contralateral functionality (Fujioka et al., 2010a; Fujii et al., 2012). However, the selectivity of the device and optimal target region temperature require further research, and direct temperature measurement of other brain regions will be crucial in such research. Due to the small temperature gradient, the Peltier probe has to be as close as possible to the target area, and therefore, any such device must be implantable to achieve long-term cooling in conscious humans. However, the most critical disadvantage of Peltier's element-based device is that the heat-releasing side of the device needs to be continuously cooled, thereby preventing immediate clinical application of the device. Thus, the use of Peltier device may be more feasible in anesthetized patients during the acute phase of cerebral ischemia in anesthetized patients. The Peltier cooling system has been extensively studied for the treatment of epilepsy and has demonstrated clinical efficacy with an intraoperative application in epilepsy patients (Nomura et al., 2014). Efforts to develop clinically feasible implantable device are continuing (Dinis et al., 2017; Hata et al., 2017), and Peltier's element-based cooling has been successfully tested in nonhuman primate (Inoue et al., 2017), as a potential clinically therapeutic strategy.
Conclusion
In this study, we validated a focal cooling device and tested its neuroprotective effect in several models of experimental ischemic stroke in rats. The device achieved accurate and stable focal brain TTM. Our results demonstrated that TTM at 33°C is protective against acute ischemic injury, progressive damage of the penumbra, and reperfusion injury. Long-term focal brain cooling under free-moving conditions was effective, but the most appropriate cooling period is to be determined in further experiments.
Footnotes
Acknowledgments
We thank Ms. Regina Altendorf (Department of Medicine 2, Universitätsklinikum Erlangen) for her technical expertise and Mr. Henry Smith for editing services. This study was financially supported by ELAN foundation of University Hospital Erlangen and a Grant-in-Aid for Challenging Exploratory Research (23659751), Japan Society for the Promotion of Science.
Author Disclosure Statement
No competing financial interests exist.