
Abstract
Fifty-four year-old man with recent history of myocardial infarction and a percutaneous coronary intervention who suffered a ventricular fibrillation arrest at home. He was resuscitated in the field. His heart rhythm was in atrial fibrillation. The cardiac catheterization showed a patent stent from his previous myocardial infarction and no new occlusions. He subsequently underwent hypothermia protocol using the Alsius CoolGard 3000 Temperature Control System and Icy Catheter. Heparin drip was started for atrial fibrillation 36 hours after catheter insertion and became therapeutic 2 hours before the end of cooling maintenance phase. Heparin drip was stopped 4 hours into the rewarming phase because of spontaneous conversion to sinus rhythm. Subcutaneous heparin was resumed for deep venous thrombosis prophylaxis. He was extubated to room air after hypothermia protocol. The cooling catheter was removed 88 hours after insertion. Within 1 minute of catheter removal, his oxygen saturation dropped to 80%. Transthoracic echocardiogram showed a mobile thrombus in the right atrium prolapsing into the right ventricle. Computer tomography angiography of the chest confirmed a large saddle embolus. Ninety minutes later, patient went into cardiac arrest with pulseless electrical activity while he was being considered for surgical embolectomy, but he could not be resuscitated. The temporal relationship of the catheter removal and his acute clinical decompensation led to believe that this was an intravascular cooling catheter (ICC)-related event. Providers should be cognizant of the complications of central venous catheters such as thrombosis formation, as it could lead to fatal pulmonary embolism. Physicians should promote frequent assessment of the access site(s) during routine physical examinations and potentially use point of care vascular ultrasound in high-risk cases to rule out a catheter-associated thrombus before catheter removal.
Introduction
I
Despite adequate VTE prophylaxis, catheter-related thrombus formation has been reported. In these cases, the etiology of the thrombus has been presumed to be related to vessel injury from the catheter tip (Righini et al., 2015). Many of those catheter-related thromboses have been subclinical (Seigel et al., 1993). On rare occasions, those thromboses may prove to be fatal.
Case
Our patient is a 54-year-old man with recent history of coronary artery disease and a percutaneous coronary intervention in the setting of previous myocardial infarction who suffered a ventricular fibrillation arrest at home. He was resuscitated in the field. He recovered spontaneous circulation with a cardiac rhythm of atrial fibrillation (new for the patient). He underwent a cardiac catheterization, which showed a patent stent from a previous coronary intervention and no new flow-limiting lesions. The patient spontaneously converted into sinus rhythm, but continued to have intermittent periods of atrial fibrillation on admission. The initiation of anticoagulation with intravenous unfractionated heparin infusion was delayed until a computed tomography scan of the head ruled out intracranial bleeding. The patient was not on any anticoagulation before this event. His initial echocardiogram did not suggest any intracardiac thrombus. He subsequently underwent therapeutic hypothermia using CoolGard 3000 Temperature Control System and Icy Catheter (Zoll Medical, Chelmsford, MA). The therapeutic anticoagulation (partial thromboplastin time 45–80) with heparin was achieved 2 hours before the end of cooling maintenance phase. He was also maintained on dual antiplatelet therapy for his recent coronary stent placement. The patient spontaneously converted to sinus rhythm within 48 hours of his hospital arrival and had no further evidence of atrial fibrillation. The heparin drip was stopped 2 hours into the rewarming phase. Subcutaneous unfractionated heparin (5000 U every 12 hours based on renal function) was resumed for deep venous thrombosis (DVT) prophylaxis at that time. He was extubated to room air after the hypothermia protocol was completed. The cooling catheter was removed 88 hours after its insertion. Within 1 minute of catheter removal, his oxygen saturation dropped to 80%. A transthoracic echocardiogram showed a dilated and hypokinetic right ventricle with preserved contractility of the apex, and a large, mobile thrombus in-transit in the right atrium prolapsing into the right ventricle (Fig. 1). Computer tomography angiography of the chest confirmed a large saddle pulmonary embolism (PE) (Fig. 2). Anticoagulation with intravenous unfractionated heparin was immediately initiated. One hour later, the patient went into cardiac arrest with pulseless electrical activity while he was being considered for surgical embolectomy. The patient succumbed after an unsuccessful resuscitation attempt. The temporal relationship of the catheter removal and his acute clinical decompensation led us to believe that this was an IVTM catheter-related event.
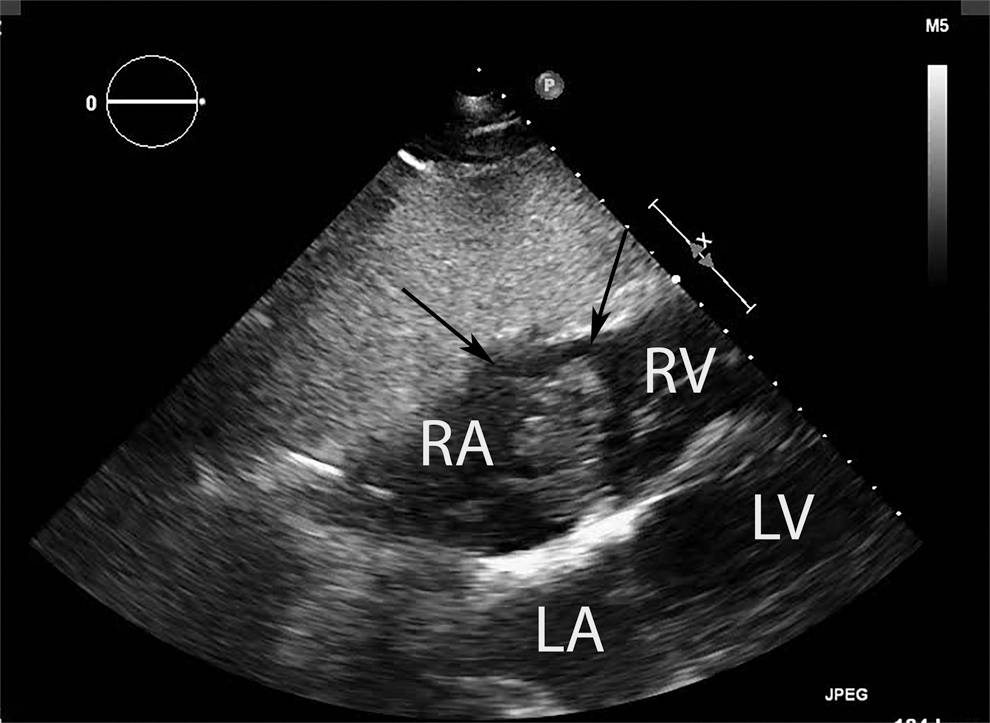
Subcostal four-chamber view during transthoracic echocardiogram: a large, mobile thrombus (arrows) in-transit is seen in the right atrium prolapsing into the right ventricle.
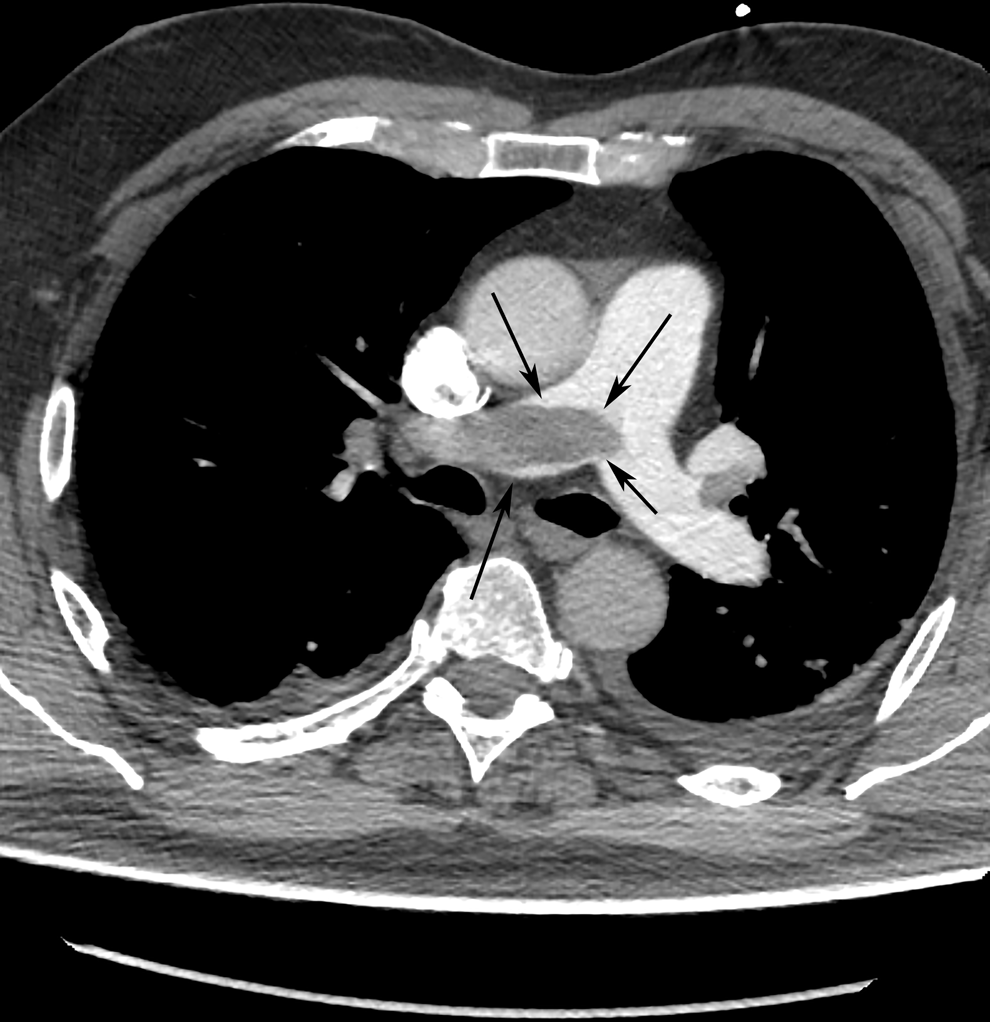
Computed tomography angiography of the chest showed extensive pulmonary embolism with saddle embolus (arrows) extending into the right main pulmonary artery.
Discussion
The American Heart Association has endorsed the use of therapeutic hypothermia as part of the postresuscitation therapy after almost all cardiac arrests. Therefore, the use of IVTM is expected to continue to increase as a cooling method. In this study, we present a case of a patient who underwent IVTM for hypothermia therapy using an Icy catheter who subsequently developed a fatal massive PE.
Critical care patients often require central venous catheters (CVC) to be placed for intravenous resuscitation, electrolyte repletion, and vasoactive drug or inotropic drug administration. However, studies have suggested that subclinical thrombosis of the catheter occurs in 20–30% of patients with indwelling catheters (Seigel et al., 1993). The most common insertion sites for CVC are the subclavian, internal jugular, and femoral veins. In a study of 76 trauma patients with unilateral femoral vein cannulation, iliofemoral DVT was identified in 14% of the cases (Mian et al., 1997). Although acquired and inherited risk factors predispose patients to developing DVT, the catheter instrumentation also plays a role in the development of CVC-related thrombosis. CVC made of silicon and polyurethane are less likely to cause DVT than the catheters made of polyethylene (Bozzetti et al., 1983; Pottecher et al., 1984; Borow and Crowley, 1985). In addition, the risk of thrombosis tends to increase with the increasing number of CVC lumena (Haire et al., 1991; Eastridge and Lefor, 1995). The intravascular cooling catheter is a triple lumen catheter composed of biocompatible polyurethane and polyethylene terephthalate, which theoretically could increase the risk of catheter-related thrombosis. To reduce the risk of thrombosis, the catheter surface is composed of a hydrophilic coating with heparin (Eastridge and Lefor, 1995).
Although the thrombogenicity of IVTM catheters have not been compared directly with other femoral catheters, it is possible that they have a similar thrombotic risk. Consequently, IVTM catheters should be promptly removed upon completion of hypothermia protocol to avoid fatal complication such as in our case. There were several possible explanations for this event. The intravascular cooling catheter is a triple lumen catheter made out of biocompatible polyurethane and polyethylene terephthalate and therefore could potentially be associated with higher risk of thrombosis (Bozzetti et al., 1983; Pottecher et al., 1984; Borow and Crowley, 1985; Haire et al., 1991; Eastridge and Lefor, 1995). In addition, the FDA approval for intravascular cooling catheter is 72 hours. The catheter indwelling time for our patient was 88 hours, 16 hours longer than its FDA recommended time, which could have contributed to thrombus formation. It is also possible that our patient had an underlying acquired or inherited hypercoagulable disorder that was not previously diagnosed. The temporal relationship between the time of the catheter removal and the onset of acute respiratory failure (1 minute after the removal of the catheter) suggested that the event was catheter related. Nonetheless, we cannot exclude the possibility of a preexisting PE on admission, since neither Doppler of the legs nor chest computed tomography angiography was done to rule out a thromboembolism.
The literature regarding the thrombogenicity of endovascular cooling catheters is mixed. Temperature regulation catheter was first introduced in 1969. We performed a literature search of articles published in PubMed from 1960 to 2016 using the search terms “intravascular cooling catheter” in combination with “venous thrombosis,” “deep vein thrombosis,” or “pulmonary embolism.” There were five publications reporting the development of thrombosis related to the use of IVTM catheter (Table 1). Among these, two cases occurred in postcardiac arrest patients after therapeutic hypothermia (Lau et al. 2010; Retamal et al., 2011). We found a case series by Prunet et al. (2009) describing two patients who developed DVTs from IVTM catheters that were used for severe head trauma and severe burns. In addition, a retrospective study in 2007 comprised 11 patients who underwent IVTM after severe head injuries showed that 33% of the patients developed DVTs related to the catheter if the catheter was removed within 4 days. The number rose to 75% if the catheter remained longer than 4 days (Simosa et al., 2007). Furthermore Gierman et al. published a case series in 2013 investigating the incidence of thrombosis related to IVTM catheters in postcardiac arrest and traumatic brain injured patients. They found that 10 of 47 patients treated with IVTM were diagnosed with venous thrombosis. Four of those had DVT, one had PE, and five patients had caval thrombus (Gierman et al., 2013).
Author did not specify which type of Alsius catheter.
DVT, deep venous thrombosis; PE, pulmonary embolism.
Other studies of the effectiveness of therapeutic hypothermia did not reveal an increase in the incidence of DVT. In fact, it was shown that in noncardiac arrest Neuro-ICU patients, only 5% of patients developed DVTs and only 1% developed nonfatal PE. The rate of DVT and nonfatal PE were even lower in cardiac arrest patients, 0.94% and 0.13%, respectively (Zoll Temperature Management White Paper, 2016). In addition, two multicenter randomized controlled trials comparing surface cooling to IVTM showed that IVTM catheters were not associated with increased incidence of DVT compared with standard CVC (Diringer, 2004; Deye et al., 2015).
The literature regarding to the thrombogenicity of IVTM catheters versus standard CVC is mixed, but it is reasonable to assume that IVTM catheters have similar incidence of thrombosis as standard CVC. However, direct comparison between the two types of catheters has not been studied. Such a study would be limited by the fact that patients who require IVTM tend to be sicker, which put them at higher risk for disseminated intravascular coagulopathy. Furthermore, hypothermic body temperature may also alter patients' coagulation pathway causing abnormal coagulopathy or bleeding. Critical care providers should be aware of the complications of CVC (including cooling catheters), promote frequent assessment of the access site(s) during routine physical examinations, and potentially use point of care vascular ultrasound in high-risk cases or prolonged indwelling times to rule out a catheter-associated thrombus before catheter removal. Although current guideline does not support anticoagulation for thrombosis prevention during IVTM, it is an area of possible future investigation to mitigate thrombosis formation.
Footnotes
Author Disclosure Statement
No competing financial interests exist.