
Abstract
Therapeutic hypothermia during cardiac surgery has been widely used for neuroprotection and to attenuate the systemic inflammatory response due to cardiopulmonary bypass (CPB). Experimental data suggest that cold-shock protein RNA-binding motif 3 (RBM3), which is induced in response to hypothermia, plays a key role in hypothermia-induced organ protection. To date, investigation on RBM3 has been performed exclusively in vitro or in animal models, and the detection and regulation of RBM3 in human blood has not been investigated until now. The aim of this study was to investigate the level of RBM3 protein and cytokine expression profile involved in the inflammatory response in patients with congenital heart disease undergoing cardiac surgery involving CPB and therapeutic hypothermia. A single-center prospective trial with 23 patients undergoing cardiac surgery with CPB was performed. RBM3 protein was quantified in blood serum samples collected from patients and healthy individuals employing a new developed enzyme-linked immunosorbent assay. Cytokine levels were analyzed from dry blood spot samples using a Quanterix Simoa Immunoassay. For the first time, RBM3 protein was detected in blood samples of patients with congenital heart disease undergoing cardiac surgery. Hereby, RBM3 protein concentrations were significantly elevated in patients after cardiac surgery with CPB and mild hypothermia as compared with pre-surgery levels. Moreover, a complex immune reaction with significant induction of pro-inflammatory cytokines (interleukin [IL]-1 beta, IL-6, IL-8, IL-16, IL-18, monocyte chemotactic protein 1, CC-chemokine ligand [CCL]3, CCL4, intercellular adhesion molecule-1) in response to CPB was detected. Significantly elevated vascular endothelial growth factor and matrix metallopeptidase 3 concentrations reflecting ischemia/reperfusion-induced injury were observed 24 hours after weaning from CPB. The use of CPB is still associated with a complex inflammatory response. RBM3 protein is measurable in blood samples of patients with significantly higher concentrations after cardiac surgery with CPB and mild-to-moderate hypothermia. RBM3 is a new candidate as a biomarker for therapeutic hypothermia and a possible new therapeutic target for organ protection.
Introduction
Targeted temperature management
Therapeutic hypothermia has been confirmed to improve survival rates and neurological functional outcome in patients with hypoxic-ischemic brain injury (Polderman and Herold, 2009). Systemic mild hypothermia is recommended as the therapy of choice according to international guidelines in neonates suffering from hypoxic-ischemic brain injury after perinatal asphyxia as a significant reduction in mortality or major neurodevelopmental disability has been reported in several randomized controlled trials (Jacobs et al., 2013).
Targeted temperature management (TTM) is recommended for patients who survived an out-of-hospital cardiac arrest with successful return of spontaneous circulation (Bernard et al., 2002; The Hypothermia after Cardiac Arrest Study Group, 2002). A target temperature between 33°C and 36°C is recommended, as the TTM trial demonstrated that 33°C for 24 hours was not superior to 36°C on the primary outcome of death or poor neurological function at 180 days (Nielsen et al., 2013).
However, a just recently published large retrospective cohort study from Australia reported an increased in-hospital mortality and a higher incidence of fever in post-cardiac arrest patients since the publication of the TTM trial (Salter et al., 2018). To date, a benefit of hypothermia in children surviving an out-of- or in-hospital cardiac arrest remains controversial, as the trials that were published until now were underpowered for statistical significance on the primary end points but revealed a consistent beneficial effect of 33.0°C versus 36.0°C with respect to all functional outcomes and survival (Moler et al., 2016, 2017).
Systemic hypothermia during cardiac surgery has been widely used for neuroprotection and to attenuate the systemic inflammatory response during cardiopulmonary bypass (CPB). Target temperatures have shifted from deep hypothermia (21–27°C) to mild-to-moderate hypothermia (>28°C) as circulatory arrest is not mandatory for the majority of surgical procedures today. Several trials have observed similar or even better neurological outcomes with mild-to-moderate hypothermia, possibly due to less adverse side-effects and rewarming-induced cell damage (Bhalala et al., 2016). A meta-analysis including 142,541 adult patients receiving on-pump coronary artery bypass grafting showed no additional benefit provided by moderate compared with mild hypothermia (Greason et al., 2014). Consistently, no difference was observed in a pediatric population comparing the impact of moderate (24°C) to mild (34°C) hypothermia during CPB on systemic inflammatory response and organ injury (Stocker et al., 2011).
Inflammatory response to CPB
Despite the tremendous technological advances in cardiac surgery, CPB surgery continues to be associated with a significant inflammatory reaction (Durandy, 2014; Boehne et al., 2017). The inflammatory response to the extracorporeal circulation during CPB has many similarities with the systemic inflammatory response syndrome (SIRS) (Davies and Hagen, 1997). Exposure of the patient's blood to the non-endothelialized synthetic surface of the extracorporeal circuit leads to abnormal shear stress and activation of the innate immune system with endothelial dysfunction and disrupted microcirculation and, ultimately, end-organ injury may occur (Adib-Conquy and Cavaillon, 2009; Warren et al., 2009).
The early phase of the inflammatory response is caused by the contact of the patient's blood with a non-endothelial surface activating the complement system, whereas the late phase is a secondary response to reperfusion injury, coagulation disorders, and heparin/protamine reactions (Day and Taylor, 2005; Warren et al., 2009). Different immune cells such as monocytes, neutrophils, and lymphocytes are attracted and activated by C3 complement and other chemoattractants, releasing proinflammatory cytokines (Day and Taylor, 2005; Madhok et al., 2006).
In the late phase, ischemia/reperfusion (I/R) injury leads to splanchnic vasoconstriction and changes in the intestinal permeability, resulting in the release of endotoxins such as lipopolysaccharide (LPS) from the intestinal microflora (Aydin et al., 2003; Warren et al., 2009). In addition, the release of proinflammatory cytokines by ischemic cells and the production of reactive oxygen species cause cell membrane damage and impair microcirculation. Activation of the contact system and platelets, as well as the fibrinolytic system contribute to coagulation disorders with reduced microcirculation and increased risk for hemorrhages (Warren et al., 2009). Heparin/protamine reactions activate the classic pathway of the complement system to further stimulate inflammation and significant hemodilution with intercompartmental fluid shifts and tissue edema, aggravating endothelial dysfunction (Bruins et al., 2000; Hirleman and Larson, 2008).
Cold-shock protein RNA-binding motif 3
Global protein synthesis is known to be repressed when the body temperature is reduced, whereas a small group of RNA-binding proteins, including RNA-binding motif 3 (RBM3), is induced in response to mild-to-moderate hypothermia (Danno et al., 1997; Tong et al., 2013). RBM3 is a small protein consisting of 157 amino acids with a molecular weight of 17 kDa (Derry et al., 1995). It has an arginine-glycine-rich domain that is referred to as RNA recognition motif that enables RBM3 to bind RNA (Derry et al., 1995).
Data suggest that RBM3 is expressed ubiquitously in the body, as it has been detected in various cell types (Zhu et al., 2016). The susceptibility of RBM3 to temperature seems to be very high, as decreasing the temperature to 36°C has been proven to be sufficient to significantly induce RBM3 expression (Jackson et al., 2015). On the contrary, hyperthermia (39–40°C) leads to decreased RBM3 expression (Danno et al., 2000; Wong et al., 2016).
Further, a variety of endogenous and environmental stressors have an impact on RBM3 regulation (Derry et al., 1995). In vitro experiments demonstrated that mild (8%) and severe (1%) hypoxia induced RBM3 in several non-neuronal cells without involvement of hypoxia-induced factor whereas no oxygen-associated regulation was observed in neuronal cells (Wellmann et al., 2004; Rosenthal et al., 2017). Exposure of late gestational mice to severe systemic hypoxia even led to the downregulation of RBM3 expression in the placenta and fetal brain tissue (Trollmann et al., 2010). Radiation was also observed to be able to induce RBM3 expression (Baba et al., 2008; Lebsack et al., 2010). Moreover, toxic agents or stimulation with LPS resulted in RBM3 upregulation (Cok et al., 2004; Ryan et al., 2005).
There is some knowledge about the cellular and molecular functions of RBM3, which seem to be multifarious. Data suggest that RBM3 plays a key role in post-transcriptional mRNA regulation to maintain protein synthesis under stressful cellular conditions (Dresios et al., 2005). RBM3 is involved in cell cycle regulation and cell proliferation. Overexpression of RBM3 reduces apoptosis, whereas RBM3 siRNA-knockout decreases cell viability and inhibits cell proliferation (Wellmann et al., 2010; Chip et al., 2011). RBM3 is found in various malignant proliferating cells and interestingly correlates with a good prognosis possibly through a higher susceptibility to chemotherapy in RBM3-expressing tumor cells (Jogi et al., 2009; Ehlen et al., 2010). In addition, a study by Peretti et al. (2015) showed that RBM3 is involved in synapse regeneration in a mouse model of neurodegenerative disease.
As the clinical application of TTM is still associated with severe adverse effects, the cold-shock protein RBM3 is a promising candidate as a biomarker during TTM and a possible new therapeutic target. To date, all data regarding RBM3 were achieved in cell culture or animal models. RBM3 was found to be detectable and regulated in human neurons in vitro, whereas detection and regulation of RBM3 in patients' blood in vivo has not been investigated (Rosenthal et al., 2017). In the current prospective clinical trial, the goal was to translate preclinical results of RBM3 expression to clinical practice.
Objective
To investigate the level of RBM3 protein and cytokine expression profile involved in the inflammatory response in patients with congenital heart disease undergoing cardiac surgery involving CPB and therapeutic hypothermia.
Methods
Study design
The single-center prospective trial was performed in the Department of Congenital Heart Disease/Pediatric Cardiology at the German Heart Institute Berlin, Germany. The study was approved by our institutional ethics committee (decision EA2/066/13), and informed consent was obtained. Patients were included in the study between November 2015 and March 2016. Preoperative, surgical, and postoperative treatment was carried out according to our clinical standard as previously described (Schmitt et al., 2016).
All patients received a central venous line, an arterial line, and a urinary catheter before surgery. Standardized CPB using polyvinyl tubing, roller pumping (mast-mounted pump; Stöckert Instruments, München, Germany), a hollow fiber membrane oxygenator (Capiox RX05; Terumo Cooperations, Tokyo, Japan), and antegrade intermittent cold crystalloid cardioplegia was performed. After the cardiac surgery, all patients were transferred to our intensive care unit. Blood samples were collected from the central venous line during the induction of the anesthesia (T1), after weaning from CPB (T2), and 24 h after the weaning from CPB (T3) as illustrated in Figure 1.
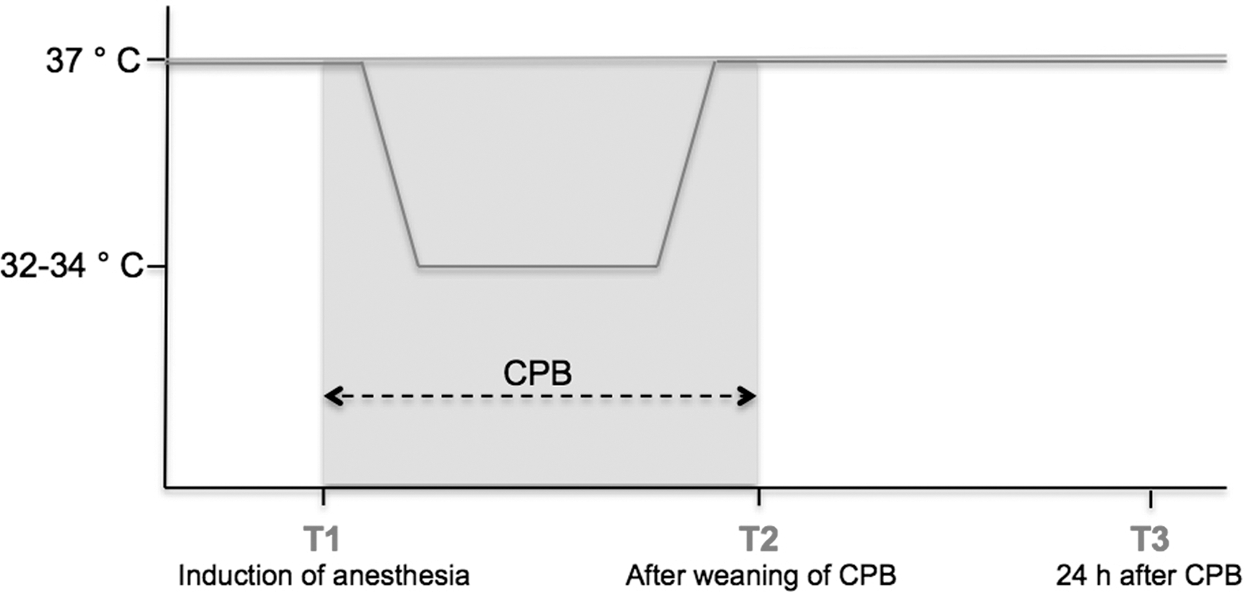
Study design. Blood samples were collected from the central venous line during the induction of the anesthesia (T1), after weaning from CPB (T2), and 24 hours after the weaning from CPB (T3). CPB, cardiopulmonary bypass.
Patients' demographic and perioperative characteristics
In our prospective trial, 23 patients were included; characteristics are summarized in Tables 1 and 2. Children as well as adults, representing the spectrum of patients with congenital heart disease, were recruited. The median age was 19.2 years (1–57). Patients suffered from a variety of congenital heart defects (Table 1). The majority of the patients (48%) underwent complex cardiac surgery, followed by valve reconstruction or replacement (26%) and modified Fontan-operation (13%). Sixteen patients (70%) had one or more prior surgical interventions. On-pump beating heart surgery to prevent reperfusion injury was performed in 6 patients (26%), whereas cross-clamping of the aorta was required in 17 patients (74%).
Demographic Data and Procedures
VSD, ventricular septal defect.
Cardiopulmonary Bypass and Perioperative Characteristics
ECMO, extracorporeal membrane oxygenation; VF, ventricular fibrillation.
Systemic mild-to-moderate hypothermia during CPB was applied in 16 patients (70%), whereas 6 patients were kept at normothermic temperatures during cardiac surgery. The most frequent severe complications after cardiac surgery were arrhythmias occurring in three patients (13%) followed by cerebral insult (4%). One patient suffered from low cardiac output requiring extracorporeal membrane oxygenation (4%) and eventually died (4%).
Bead-based multiplexed immunoassay for analyzation of dried blood spots
Samples of 13 patients were collected as dried blood spots (DBS). DBS samples were analyzed with an ultrasensitive Quanterix Simoa Immunoassay (“single molecule arrays”) by BioMedTech Tübingen, Germany in cooperation with the company HOT Screen, Reutlingen, Germany. Standard curve, control, and sample quality control were performed to ensure proper assay performance.
Enzyme-linked immunosorbent assay for RBM3 protein analysis
RBM3 protein levels were analyzed from 16 patients undergoing cardiac surgery at the German Heart Institute Berlin, Germany and 14 healthy individuals. For quantification of RBM3 in serum samples, the Human RBM3 ELISA Kit was developed by BioTeZ (Berlin, Germany), which is an immunological quantitative detection method based on a sandwich enzyme-linked immunosorbent assay. Two monocloncal antibodies (AH9 and HB9) were used as detection and capture antibody (Fig. 6).
Samples were prepared and analyzed according to the manufacturer's instructions. Briefly, serum samples were diluted 1:10 with RBM3 sample buffer. Then, 50 μl of the diluted samples or controls was simultaneously incubated in a 96-well plate pre-coated with 50 μL of a specific capture antibody against human RBM3 and a secondary horseradish peroxidase-conjugated antibody against the anti-RBM3 antibody at room temperature for 2 hours. After three washing steps, the color substrate tetramethylbenzidine was added to the wells and incubated with gentle shaking protected from light for 30 minutes. The reaction was stopped with the addition of a stop reagent, and extinctions were measured at 450 nm in a microplate reader (Multiascan Ascent; Thermo Fisher Scientific). The concentration of RBM3 was determined by interpolation from a standard curve.
Statistic analysis
Data were graphed and analyzed with Prism GraphPad 7 (GraphPad Software, Inc., Lajolla, CA). Variability between groups was compared with a Wilcoxon matched-pairs signed-ranks test. For all analyses, p < 0.05 was considered statistically significant.
Results
Myocardial cell damage after cardiac surgery with CPB
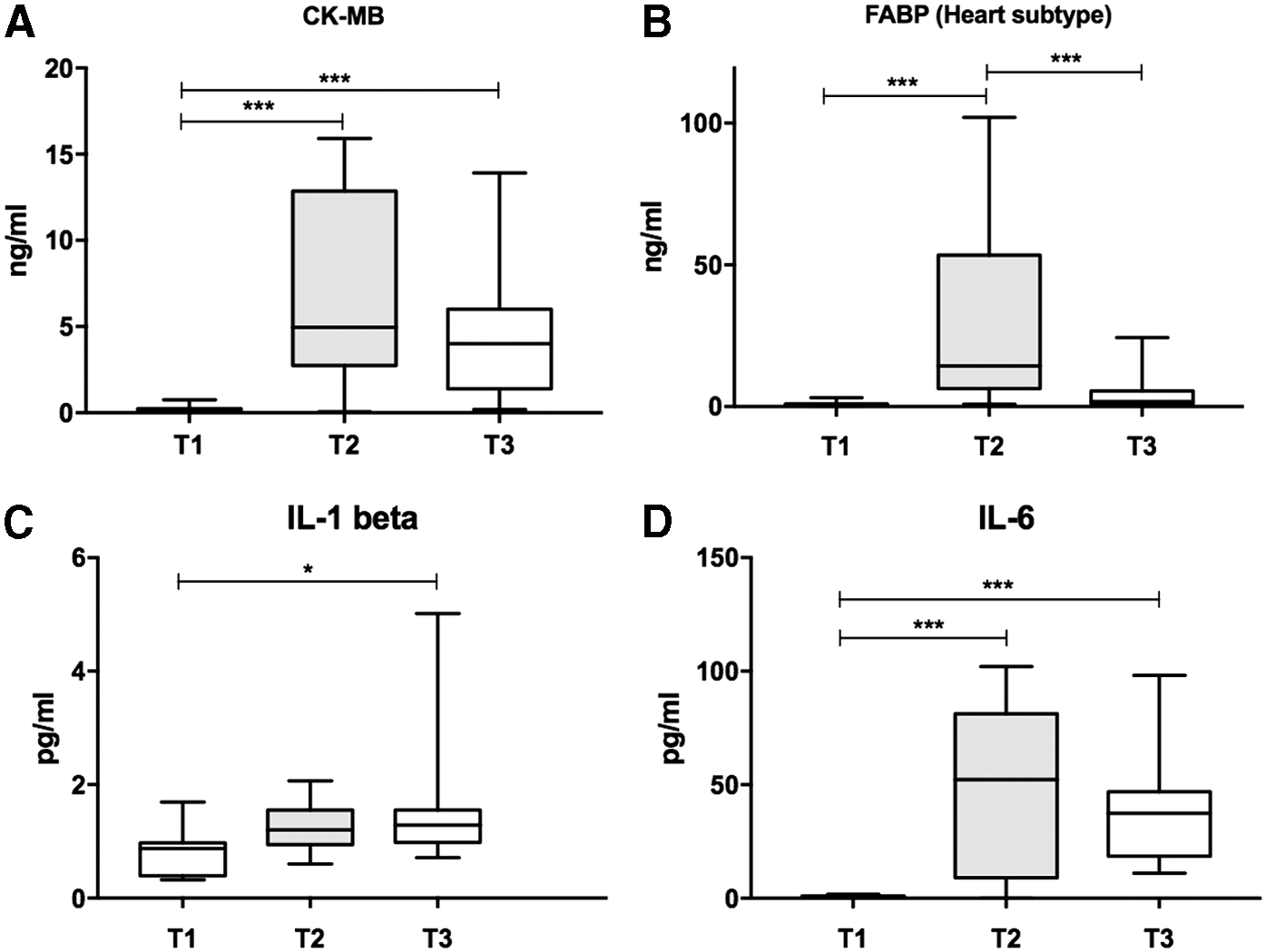
Cardiac surgery with the application of cardioplegia and CPB led to myocardial cell damage and the release of the intracellular protein creatine phosphokinase heart subtype (CK-MB) and heart-type fatty acid-binding protein (H-FABP). Levels of CK-MB and H-FABP were measured in patients' blood samples during the induction of anesthesia (T1), after weaning from CPB (T2), and 24 hours postoperative (T3) according to our protocol (Fig. 1). CK-MB-levels were significantly increased after weaning from CPB and 24 hours after CPB compared to pre-surgery values (Fig. 2). Consistently, FABP heart subtype was significantly elevated after weaning from CPB, but decreased rapidly to almost pre-surgery levels 24 hours after CPB (Fig. 2).
Levels of pro- and anti-inflammatory cytokines and chemokines increased in response to CPB
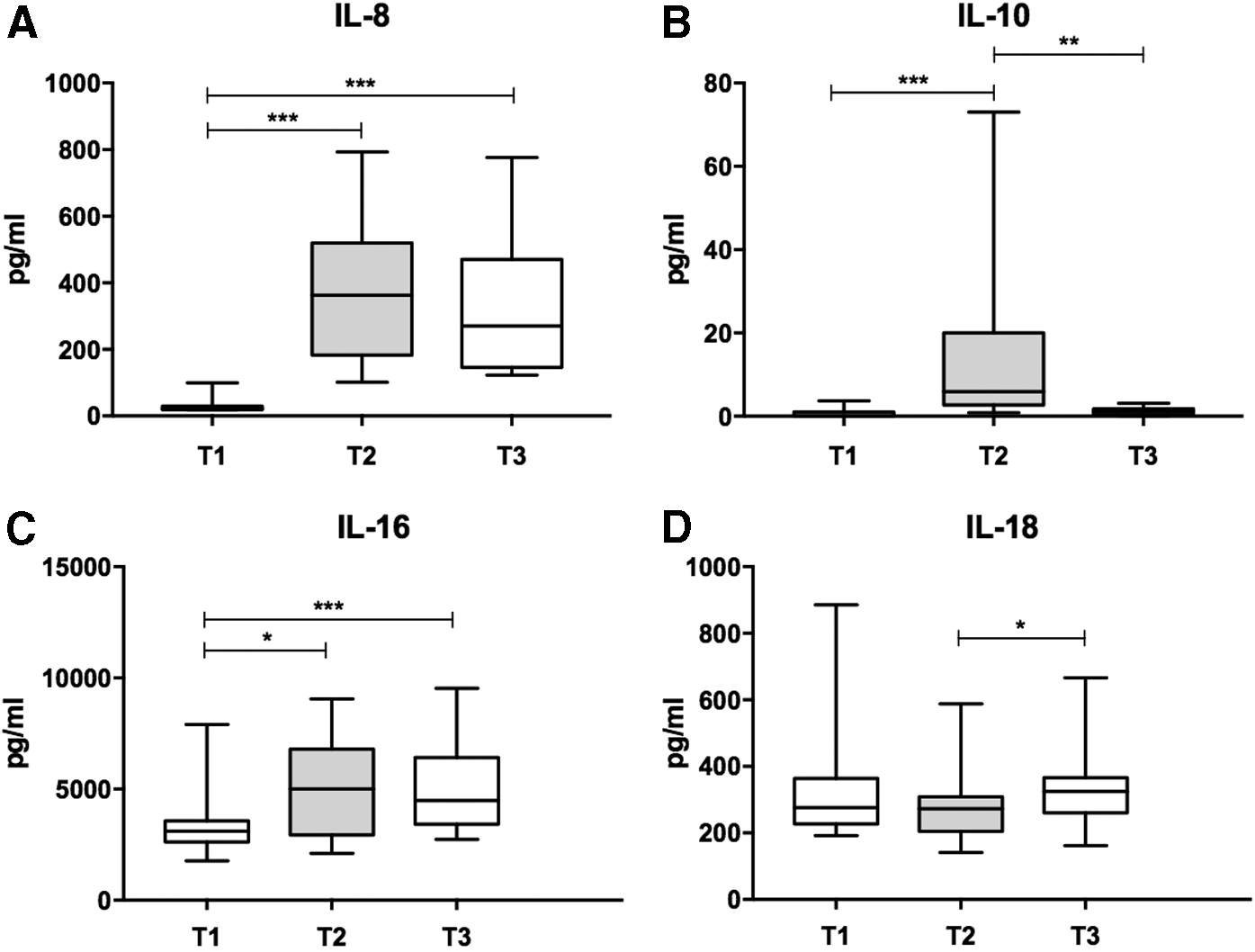
A complex modulation of pro- and antiinflammatory cytokines and chemokines in response to CPB could be observed in our study cohort. Cytokine levels were measured in patients' blood samples during the induction of anesthesia (T1), after weaning from CPB (T2) and 24 hours postoperative (T3) according to our protocol (Fig. 1). After weaning from CPB (T2), a significant increase in proinflammatory cytokines interleukin (IL)-6, IL-8, and IL-16 could be observed (Figs. 3 and 4), with levels remaining significantly increased 24 hours after CPB (Fig. 3). IL-1 beta and IL-18 were significantly increased 24 hours after CPB (Fig. 4).
Cytokine levels of proinflammatory IL-8 (
Chemokine levels of MCP-1 (
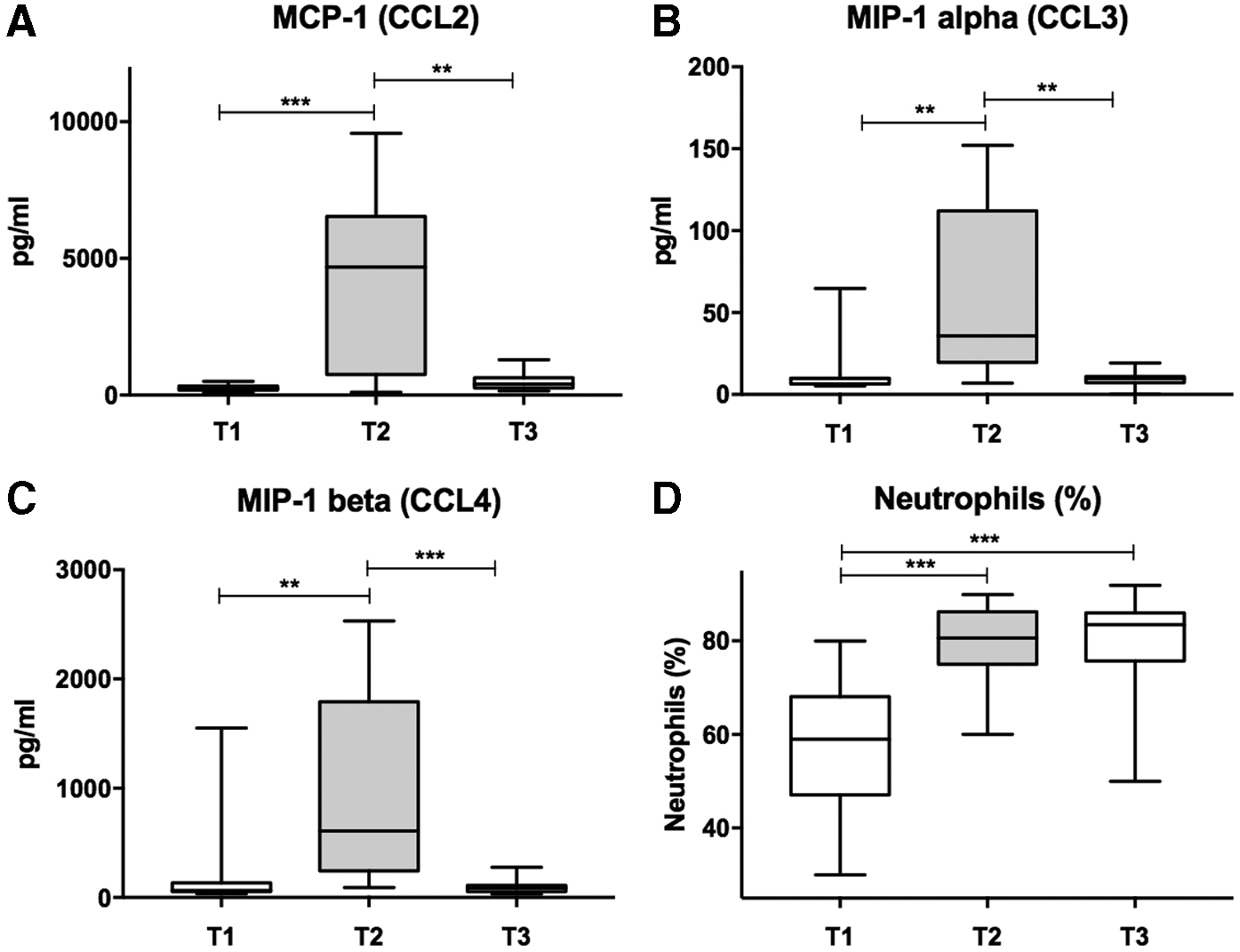
Moreover, chemokine levels of CC-chemokine ligand (CCL)2 (also known as monocyte chemoattractant 1 [MCP-1]), CCL3, and CCL4 were significantly increased after CPB and rapidly decreased to pre-surgery levels after 24 hours (Fig. 5). Consistently, the percentage of neutrophils in the patients' blood significantly increased after CPB and remained elevated 24 hours after cardiac surgery. Levels of proinflammatory tumor necrosis factor β (TNF-β) significantly increased after CPB and remained elevated 24 hours postoperative. Intercellular adhesion molecule 1 (ICAM-1) was significantly elevated 24 hours after CPB (Fig. 4). Anti-inflammatory cytokine IL-10 significantly increased in response to CPB at T2 but decreased rapidly to pre-surgery levels at T3 (Fig. 6).
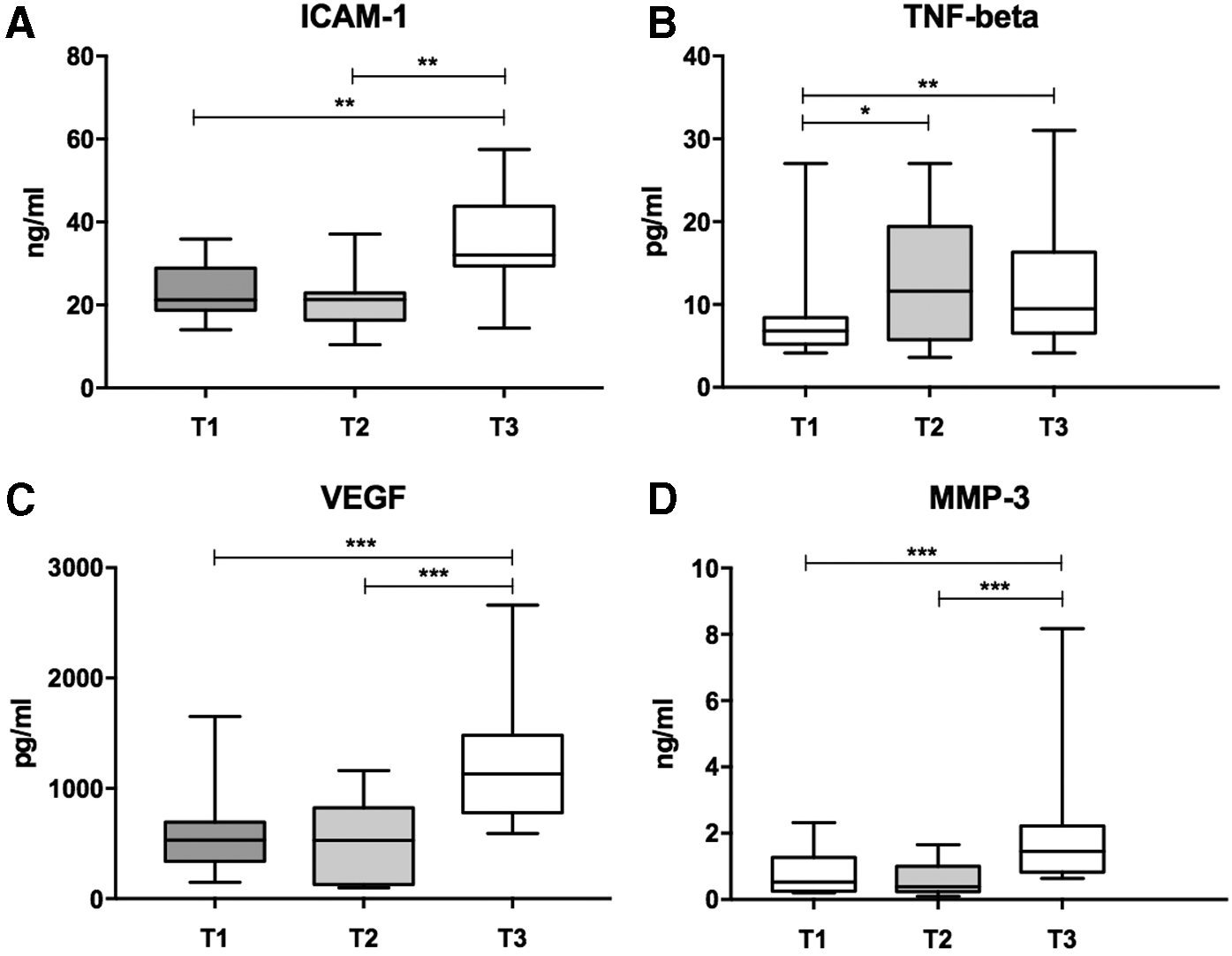
ICAM-1 was significantly elevated 24 hours after CPB
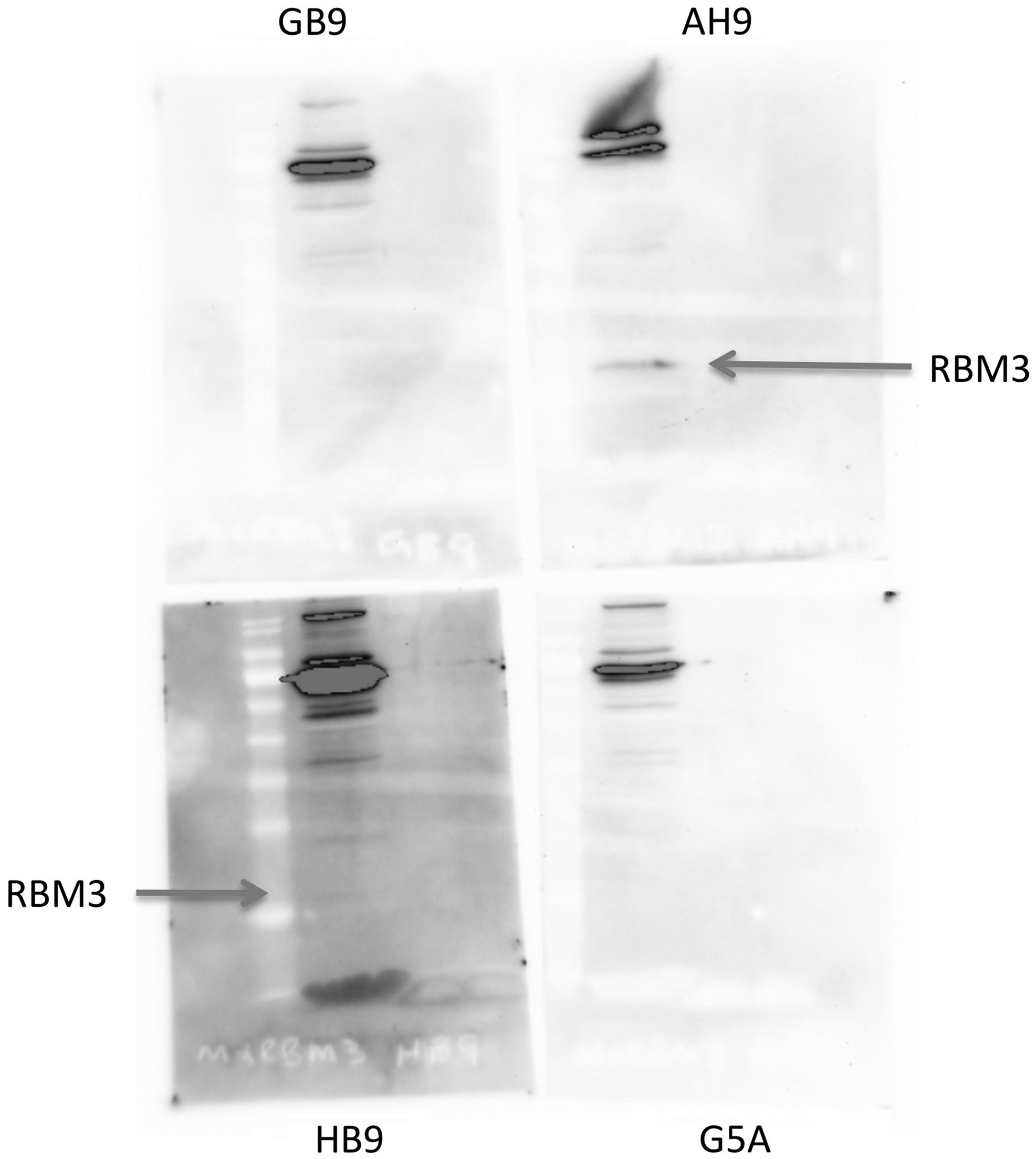
Western blot of RBM3 monoclonal antibodies. The clones AH9 and HB9 were used as detection and capture antibody for enzyme-linked immunosorbent assay analysis. RBM3, RNA-binding motif 3; CHD, congenital heart disease.
Reperfusion injury and tissue remodeling
I/R injury is known to be crucial during CPB, contributing to loss of cardiomyocytes and induction of secondary inflammation. This was reflected by a significant upregulation of vascular endothelial growth factor (VEGF) 24 hours after weaning from CPB (Fig. 3). Further, a significant upregulation of matrix metallopeptidase 3 (MMP-3), which is involved in the breakdown of extracellular matrix during tissue remodeling and angiogenesis, was observed 24 hours after CPB (Fig. 3). Inflammation caused by I/R injury in the late phase was reflected in significantly increased levels of proinflammatory cytokines IL-1 beta, IL-6, IL-8, and IL-16 in comparison to pre-surgery levels (Figs. 3 and 4).
RBM3 protein levels increase after CPB
RBM3 levels were measured in 16 patients and 14 healthy individuals (Fig. 7). RBM3 was distributed in a non-Gaussian manner. RBM3 levels varied from 370 to 16,214 pg/mL, and median level was 2622 pg/mL. There were no significant differences in RBM3 protein levels between healthy individuals and patients with congenital heart disease (CHD) at T1 (Fig. 7).

RBM3 protein levels in blood of 30 people, of whom 14 were healthy individuals and 16 were patients with CHD
According to our protocol, RBM3 protein was measured in patients' blood samples during the induction of anesthesia (T1), after weaning from CPB (T2) and 24 hours after the surgery (T3) (Fig. 1). RBM3 protein levels were significantly increased after weaning from CPB compared with pre-surgery levels and remained elevated until 24 hours after CPB, though not to significance (Fig. 7). In 13 out of 16 patients, the body temperature during CPB was reduced to 32–34°C. Only three patients underwent cardiac surgery under normothermia. RBM3 was significantly increased after CPB in patients treated with mild-to-moderate hypothermia during CPB and remained elevated 24 hours after CPB, even though not statistically significant (Fig. 8). In the three patients in whom normothermia was maintained during CPB, no significant change in RBM3 levels could be detected (Fig. 8). We did not find a correlation between age and baseline RBM3 (T1) or an increase in RBM3 after CPB (T2) in our study cohort (Fig. 8).
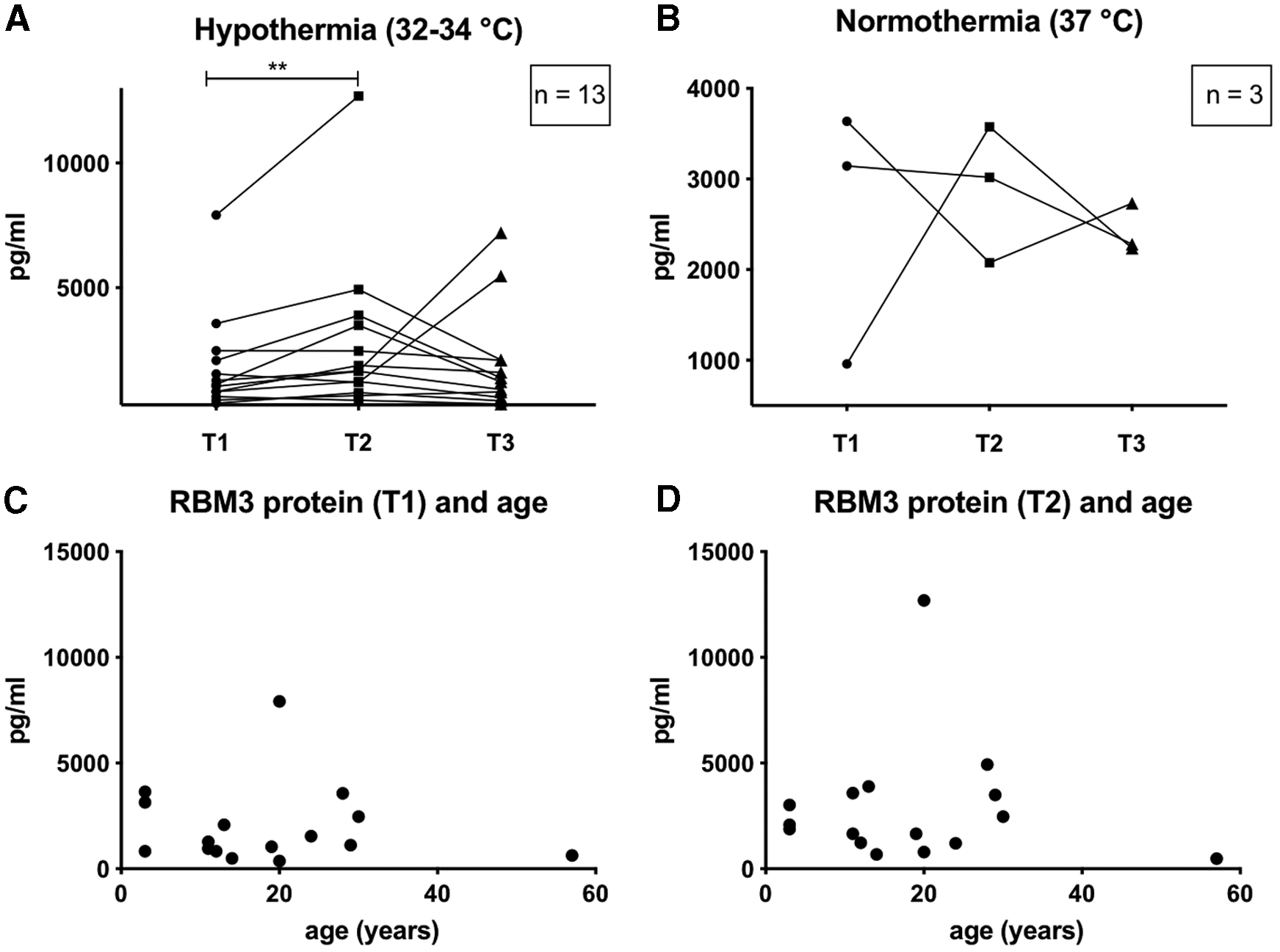
RBM3-protein levels in patients who received cardiac surgery in mild-to-moderate hypothermia were increased after weaning of CPB
Discussion
Inflammatory response to CPB
In this study, we investigated the regulation of RBM3 protein and cytokines in blood samples of patients with congenital heart disease undergoing cardiac surgery with CPB and therapeutic hypothermia.
First, we measured significantly increased levels of proinflammatory cytokines IL-1 beta, IL-6, IL-8, IL-16, and IL-18 after weaning from CPB in our cohort. Prior studies have observed similar increases in levels of IL-6 and IL-8 in pediatric and adult patients after CPB, correlating with intensive care unit length of stay, duration of mechanical ventilation, administration of blood products, and lower central venous saturation, suggesting compromised hemodynamics (Madhok et al., 2006; Allan et al., 2010; de Fontnouvelle et al., 2017).
An increase in IL-1 beta levels after CPB as observed was reported by some authors, whereas others did not (Madhok et al., 2006; Gu et al., 2008). IL-16 functions as a chemoattractant for CD4-positive cells and primes them for their responsiveness to other cytokines (Murphey and Weaver, 2016). IL-18 (or interferon-gamma inducing factor) stimulates natural killer and T cells to release interferon γ, which specifically activates macrophages (Murphey and Weaver, 2016). To the best of our knowledge, we are the first to observe a modulation of IL-16 and IL-18 levels after CPB in either pediatric or adult patients, indicating their contribution to SIRS in response to CPB.
Second, we investigated the modulation of various chemokines and observed significantly elevated levels of CCL2 (MCP-1), CCL3, and CCL4 after CPB, which have been described (Ghorbel et al., 2010; Onorati et al., 2011; Beer et al., 2014). Correspondingly, the percentage of neutrophils, known to be the main targets of the analyzed chemokines, was increased in our patient cohort (Huber et al., 2017). CCL2 has been reported to correlate with longer operation time, a need for inotropic support, and reoperation in pediatric patients (Lotan et al., 2001; Gessler et al., 2005).
Third, we observed significantly increased levels of TNF-β and ICAM-1 after CPB, whereas levels of TNF-α did not change in our study cohort (data not shown). TNF-β is a multifunctional cytokine with potent cytotoxic activity and is an activator of the nuclear factor-kappa B signaling pathway (Murphey and Weaver, 2016). We are the first to describe elevated serum TNF-β-levels after cardiac surgery with CPB. The role of TNF-α, on the other hand, remains controversial, as some investigators have observed increased levels after CPB, whereas others could not detect any modulation (Ishida et al., 2006; Allan et al., 2010; Amanullah et al., 2016; de Fontnouvelle et al., 2017; De Iuliis et al., 2017). Modulation of ICAM-1 levels, which is expressed by endothelial cells to bind activated leukocytes and facilitate their transmigration to tissue, was previously described after CPB (Liu et al., 2014; Murphey and Weaver, 2016).
Last, we measured significantly increased levels of the anti-inflammatory cytokines IL-10 after CPB, as reported by prior investigators (Madhok et al., 2006; Allan et al., 2010; De Iuliis et al., 2017). IL-10 has a strong immunmodulatory function, as it is capable of downregulating the antigen-presenting capacity of innate immune cells through a reduction in human leukocyte antigen expression (Adib-Conquy and Cavaillon, 2009; Murphey and Weaver, 2016).
The clinical relevance of the inflammatory response to cardiac surgery and CPB remains controversial. A correlation between increased proinflammatory cytokine levels and various clinical parameters has been previously described. On the contrary, the systemic application of steroids, such as methylprednisolone or dexamethasone, known to ubiquitously modulate the immune response at the cellular and humoral level did not have a persuading clinical benefit for children or adults undergoing cardiac surgery with CPB in clinical trials (Whitlock et al., 2015; Elhoff et al., 2016).
I/R injury
I/R injury is known to significantly contribute to inflammation during CPB and is reflected by the significant elevation of circulatory proinflammatory cytokines IL-1 beta, IL-6, IL-8, and IL-16 in the late phase (24 hours after CPB) in our patient cohort. We further observed a significant increase in VEGF, a known target of hypoxia-induced factor-1α (HIF-1α) and a marker for endothelial damage. HIF-1α is upregulated under hypoxic conditions; therefore, the increase in VEGF in the patients' samples is presumably a consequence of I/R injury. Last, we observed increased levels of the proteolytic enzyme MMP-3, which is involved in the breakdown of extracellular matrix during tissue remodeling and angiogenesis that occurs during I/R.
RBM3 protein regulation
Experimental data suggest that RBM3 plays a key role in hypothermia-induced neuroprotection (Chip et al., 2011; Peretti et al., 2015). To our knowledge, we are the first to demonstrate that RBM3 protein can be detected in human blood serum samples.
First, RBM3 was measured in 14 healthy individuals and 16 patients with CHD. Different concentrations with a wide concentration range were seen with a non-Gaussian distribution. No significant differences in RBM3 concentration between healthy probands and patients with CHD were observed. Interestingly, RBM3 concentration was slightly increased in the healthy group, possibly due to hemodilution as a result of perioperative volume management in the CHD group that received cardiac surgery.
Second, RBM3 levels were significantly increased after cardiac surgery, utilizing CPB and mild-to-moderate hypothermia. This increase could be hypothermia-mediated, as this mechanism has been well described in several experimental studies (Danno et al., 1997; Tong et al., 2013; Rosenthal et al., 2017). Unfortunately, we could only include a small number of patients who received normothermic CPB (n = 3), so no final conclusion can be drawn due to the small sample size and high standard deviation.
Experimental data indicate that RBM3 is highly expressed in young animals during early brain development and is mostly absent in adult animals (Pilotte et al., 2009; Jackson et al., 2018). In our rather small patient cohort, we could not observe a correlation between baseline RBM3 protein levels or increase of RBM3 protein after CPB and hypothermia and the age of the patients (Fig. 8). As the youngest patient in whom RBM3 protein was analyzed was three years old and no neonates or younger infants were included, no final conclusions about the impact of age on RBM3 protein expression in humans can be drawn. Nevertheless, it seems promising that RBM3 protein was also measurable and regulated in older patients.
Limitations
Our study is limited by a small number of patients and a heterogenous cohort. A far-reaching conclusion about the effects of hypothermia cannot be drawn because of the lack of a control group of patients who were operated under normothermic conditions. Additional research is needed to determine the impact of age on RBM3 protein expression. The increase in RBM3 protein concentration could also be a response to cellular stress caused by the extracorporeal circulation, systemic inflammation reaction, and I/R injury occurring during CPB, which has been characterized by cytokine regulation profiles. Ultimately, RBM3 protein concentration in patients' serum samples could also be increased as a result of cell lysis during extracorporeal circulation. Further research is needed to conclusively answer these questions and elucidate the underlying molecular pathway.
Conclusion
RBM3 protein is measurable in patients' blood samples with significantly higher concentrations after cardiac surgery with CPB and mild-to-moderate hypothermia. RBM3 is a new candidate as a biomarker for therapeutic hypothermia and a possible new therapeutic target for organ protection. Despite the recent technological progress, the use of CPB is still associated with a complex inflammatory response and therapeutically diminishing it could have a beneficial impact on the clinical outcome of pediatric and adult patients.
Footnotes
Acknowledgments
Dr. L.-M.R. and Dr. C.P. are participants in the Berlin Institute of Health Charité (Junior) Clinician Scientist Program funded by the Charité–Universitätsmedizin Berlin and the Berlin Institute of Health. The authors thank Thomas Joos from BioMedTech, Tübingen, Germany for the help in analyzing the DBS samples and Nora Ebermann, medical technician, for her support on this research.
Author Disclosure Statement
No competing financial interests exist.