
Abstract
Hypothermia is associated with high mortality in sepsis, but it is now recognized that this association may simply reflect its higher prevalence in sicker patients. Furthermore, there is evidence to suggest that hypothermia may not represent a dysfunction in sepsis. In this study, we conducted a survey to assess how this scientific evidence relates to the perceptions of health care professionals regarding septic hypothermia, and how such perceptions drive clinical conduct concerning the use of active rewarming in this population. A survey with questions on opinions and management of spontaneous hypothermia in sepsis was developed and posted online at the European Society of Intensive Care Medicine (ESICM) website from March 24th, 2017 to the June 26th, 2017 and distributed by electronic email. Respondents were asked to fill in the survey from the perspective of their usual or average practice in their intensive care unit. In total, there were 440 survey respondents. Respondents were predominantly from Europe (66%) The majority of respondents were intensivists (78%) and worked in an academic hospital (66%). One percent of respondents were nurses. Most respondents (96%) reported that there was no protocol for the management of hypothermic sepsis. Of the respondents, 62% actively rewarmed patients with hypothermic sepsis. Hypothermia was defined as a temperature below 36°C (44%) and below 35°C (15%). Rewarming practices showed large variation in terms of the temperature, at which respondents initiate rewarming as well as the target temperature to which patients are rewarmed. The most predominant first-line rewarming method was forced-warm air followed by warm IV fluids. Rewarming decisions were mostly physician driven (58%). Most respondents thought rewarming was beneficial (43%), a small proportion thought rewarming to be harmful (9%). In conclusion, policies, procedures, and beliefs about spontaneous hypothermia and active rewarming in patients with sepsis are variable. This must be taken into consideration in designing future trials. We propose a working group to define hypothermic sepsis to improve comparability of research.
Introduction
An altered core body temperature is a hallmark of sepsis. Although fever is most commonly associated with sepsis, hypothermia occurs spontaneously in 10–35% of septic patients at the time of admission (Wiewel et al., 2016) and in an additional 30% of the patients during the intensive care unit (ICU) stay (Fonseca et al., 2016). Development of hypothermia is associated with a twofold increase in mortality compared to patients presenting with fever (Wiewel et al., 2016). This association has led to the hypothesis that hypothermia is a dysregulated, detrimental phenomenon in sepsis.
More recently, however, it has been increasingly recognized that the prognostic value of hypothermia does not imply that it is the hypothermia itself that worsens outcome, the main reason being that those septic patients who develop hypothermia are usually sicker than those who do not (Jiang et al., 2015). The notion that septic hypothermia reflects dysfunction has also been challenged by the finding that hypothermia in septic patients not subjected to active rewarming is a transient, self-limiting response that becomes rare when organ dysfunction is at a maximum in the hours preceding death (Fonseca et al., 2016). The same finding also raises the question as to whether it is necessary to actively rewarm those septic patients who develop hypothermia.
It is currently unknown how these scientific lines of evidence relate to the perceptions of health care professionals regarding septic hypothermia, as is unknown how such perceptions drive clinical conduct concerning the use of active rewarming in these cases. We conducted an online survey on septic hypothermia to address these questions. Using this survey, we aimed to characterize differences in definition and rewarming practices of spontaneous hypothermia during sepsis and determine to what extent these practices are protocolized.
Second, we aimed to assess current opinion on the effect of spontaneous hypothermia and rewarming patients with spontaneous hypothermia during sepsis. We hypothesized that rewarming practices and opinions regarding spontaneous hypothermia would be highly variable.
Methods
Survey
A survey containing questions about opinions and management of hypothermic sepsis was developed for this study (Supplementary Data S1). The survey was tested several times for unambiguous interpretation of questions by distributing the survey among intensivists in the ICU of the Academic Medical Center in Amsterdam and was revised according to specific comments of respondents.
It was then posted on the website European Society of Intensive Care Medicine (ESICM) and electronically mailed to members of the following ESICM sections: Systemic Inflammation and Sepsis (3268 members); Trauma and Emergency Medicine (7186 members); and Cardiovascular Dynamics (11,685 members). The survey was online from March 24th, 2017 to June 26th, 2017. Respondents were asked to fill in the survey from the perspective of the usual or average practice on their ICU. IP addresses were used to provide an indication of the amount of potential duplicate responses.
Statistical analysis
All analyses were performed in R (version 3.1.1) and SPSS version 24. Normally distributed data are presented as mean ± (standard deviation). Nonparametric data are presented as median (25–75th percentile).
Results
In total, there were 440 respondents to the survey. Of these, 288 (66%) of respondents were working in Europe, 67 in Asia (15%), and 39 (9%) in Latin America. 341 (78%) of respondents were intensivists. The main specialty area of respondents was intensive care (288 [59%]) followed by anesthesiology (114 [26%]) and internal medicine (40 [9%]). Respondents mainly worked in an academic hospital (290 [66%]) versus nonacademic hospital (150 [34%]). Reported years of ICU experience were evenly distributed; the largest portion of respondents (28%) reported 0–5 years of ICU experience. Only three (1%) nurses filled in the survey. Table 1 shows the characteristics of respondents in the survey.
Characteristics of Respondents
Rewarming: definitions and practice
Among the 440 respondents, 96% indicated that there was no written protocol for the management of hypothermic septic patients at their institution. Sixty-two percent of respondents reported that they actively rewarmed patients with spontaneous hypothermia during sepsis, compared to 38% who did not rewarm patients. Respondents were asked to specify per 0.1°C what their definition of hypothermia was. There was a wide range of definitions of hypothermia ranging from 34.0°C to 37.5°C. The most frequent answer was 36.0°C (44%) followed by 35.0°C (15%) (Fig. 1A shows answers grouped per 0.5°C).
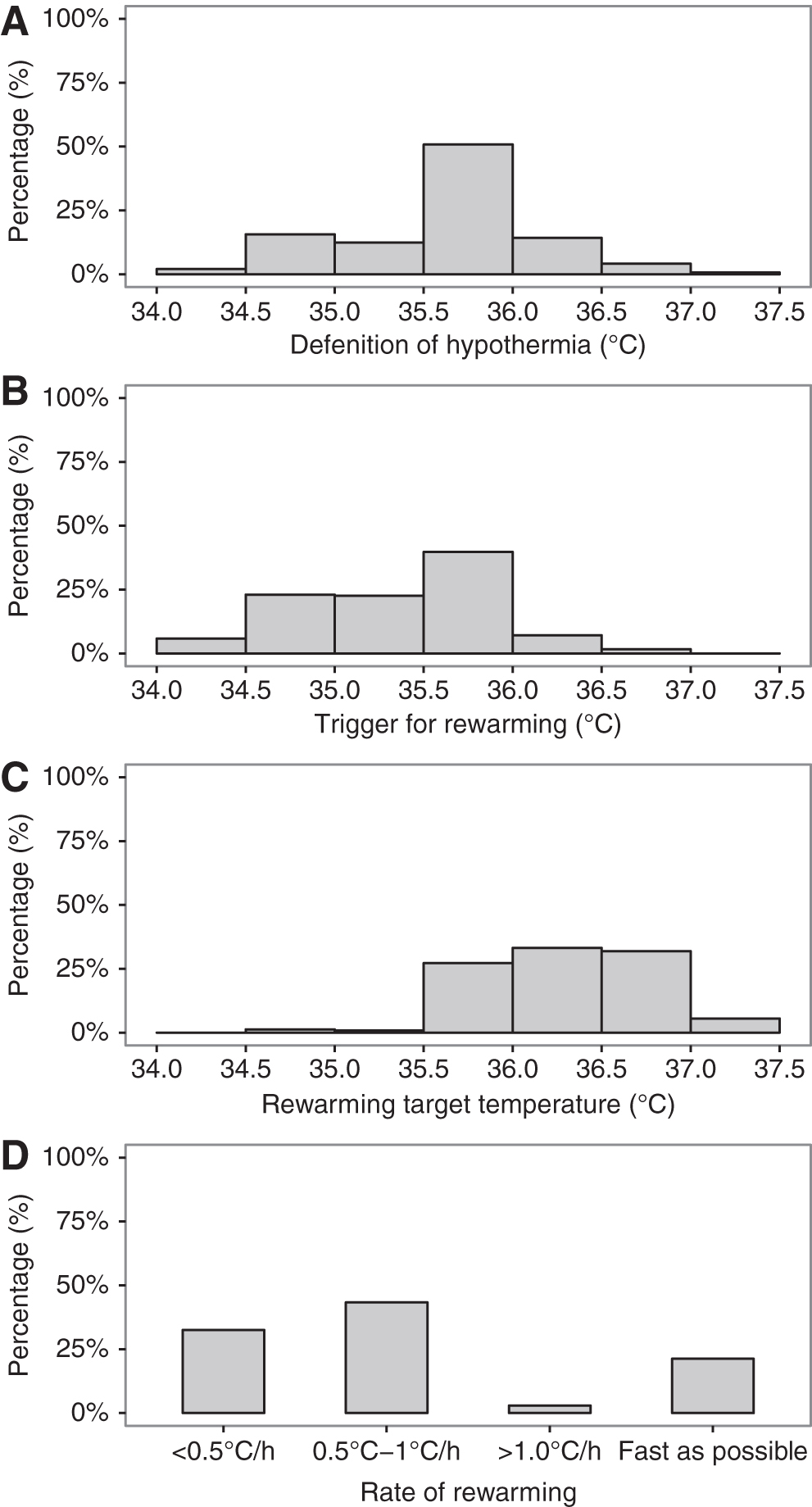
Respondents who actively rewarmed patients were asked about their rewarming practices. On average, most respondents considered rewarming patients from a temperature of 36.0°C (31%) (Fig. 1B). Forty-eight percent of respondents delayed rewarming of patients starting at a lower temperature than their hypothermia definition.
The target temperature to which patients are rewarmed also varied; most patients were rewarmed to a target temperature of 37°C (28%) (Fig. 1C). There was a large variation in rewarming practice, which ranged from 0.5°C per hour to as fast as possible (Fig. 1D). Among respondents, 58% said that the decision to rewarm patients was predominantly physician driven compared with 42% who said that it was nurse driven.
Respondents were asked which factors influenced their decision to rewarm patients on a scale of 0 (not influential at all) to 5 (extremely influential). Shivering was the most influential (3 [2–4]), followed by the presence of shock (3 [2–3]). The predominant first-line method of rewarming was forced warm air (90%), followed by warmed IV fluids (36%).
Respondents opinion
Respondents were also asked their opinion on the effect of hypothermia on the outcome of patients. Most respondents expressed a belief that hypothermia is associated with increased mortality (66%), followed by do not know (24%), does not affect mortality (8%), and decreases mortality (2%). The majority of respondents believe that patients should be rewarmed (55%), compared with 18% who believe that patients should not be rewarmed. Among respondents who believe that patients should be rewarmed, the majority (52%) believe that rewarming negates the negative effects of hypothermia. Among respondents who believe that patients should not be rewarmed, 41% believe that rewarming negated the positive effects of spontaneous hypothermia.
Discussion
In this study, we describe the results of a survey on the management of patients with spontaneous hypothermia. The main findings of this study are as follows: (1) both the definition of spontaneous hypothermia and the practice of active rewarming in these patients are extremely variable; (2) a considerable proportion of respondents do not rewarm patients with spontaneous hypothermia during sepsis; and (3) there is no consensus on the etiology of spontaneous hypothermia.
This study is the first to provide detailed insight into temperature management of patients with spontaneous hypothermia in sepsis. The practice of rewarming remains controversial. Considering that hypothermia is associated with an increased mortality, rewarming is understandable, likely in an attempt to negate any adverse effects of hypothermia. The practice of rewarming may be further motivated by physicians' drive to reach physiological values. A majority of respondents in our survey (62%) indicated that they rewarmed patients with hypothermic sepsis. In a recent survey among UK physicians, a majority of physicians (84%) also rewarmed patients, whereas 16% indicated that they would not rewarm septic patients below a temperature of 34°C (Beverly et al., 2016). Only 60% of respondents in this study were concerned with a body temperature of 35–36°C in this patient population (Beverly et al., 2016).
Taken together, the differences in temperature management practice is indicative of a lack of clarity on this issue. The results from this survey make it clear that a robust definition of hypothermia is warranted. This would enable comparisons of incidences and outcome of rewarming practices.
Clinical observational studies overwhelmingly point to hypothermia adversely effecting outcome (Wiewel et al., 2016). In light of these studies, it is noteworthy that none of the respondents reported to have a protocol in place for the management of hypothermic sepsis, most probably due to lack of strong clinical evidence. The aforementioned clinical studies are observational in nature and therefore cannot infer causation between hypothermia and outcome. Moreover, there are no randomized trials studying the impact of rewarming in hypothermic septic patients. If rewarming benefits patients, it is unclear at which temperature they should be rewarmed as well as to which target temperature and how fast patients should be rewarmed. It would be interesting to see the effect that rewarming to target temperatures is in respect to outcome and specifically immune response. In vitro experiments have shown that rewarming can improve immune responses (Billeter et al., 2015).
On the contrary, experimental evidence points to hypothermia being an adaptive response (Steiner et al., 2017). In hypothermic rodents with endotoxemia, thermogenic capacity is intact, arguing against hypothermia being a defect in thermogenic capacity (Romanovsky et al., 1996). Also, hypothermic rodents actively seek colder environments (Almeida et al., 2006) and spontaneous hypothermia also improved survival in mice infected with E. coli (Liu et al., 2012). Moreover, rewarming can potentially have adverse effects such as ischemia reperfusion injury and increased metabolism (Bisschops et al., 2012). A randomized clinical trial would clarify the discrepancy between experimental studies and clinical observations.
There are several limitations that apply to this study. An inherent limitation of this online survey is that we do not know the percentage of respondents or duplicates. To provide an indication of the rate of response to this survey, we have added the number of members of each contacted ESICM section, which provided most of the responses. We used IP address to address potential duplicate responses to the survey. In total, there were 15 duplicate addresses. The majority of these duplicates had different respondent characteristics. In three cases, there were similar respondent characteristics. We did not remove these. Also, the respondents in this survey were predominantly from European countries, limiting the translatability to other countries. Finally, a large proportion of respondents said that rewarming decisions were nurse driven and only three nurses filled in the survey. We do not know how well the physicians' answers reflect rewarming practices by nurses.
Conclusions
In conclusion, policies, procedures, and beliefs about spontaneous hypothermia and active rewarming in patients with sepsis are variable.
The variation in practice must be taken into consideration in designing trials on temperature management in hypothermic sepsis patients. As a starting point, we propose a working group to define hypothermic sepsis to improve comparability of research on this subject.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.