
Abstract
The effect of temperature on cerebral injury during hypothermic circulatory arrest (HCA) has never been specifically studied. This study aimed to compare the effects of two different temperatures used for HCA on the degree of brain injury in pig models. Thirteen pigs were randomly assigned to a deep hypothermic circulatory arrest (DHCA) group (n = 5), moderate hypothermic circulatory arrest (MHCA) group (n = 5), or control group (n = 3). No significant differences in immunohistochemical assay results, including Bax, Bcl-2, and Caspase 3 staining, and a TUNEL assay, were observed between the DHCA and MHCA groups. Furthermore, no significant difference was found for biomarkers of brain injury (Soluble protein-100B) between the two experimental groups. Similarly, no significant difference was observed in the trend of changes in inflammatory factors, including tumor necrosis factor-α, interleukin (IL)-2, and IL-6, between the two groups (p > 0.05). However, coagulation factors, including FXI and FVII, were different between the DHCA and MHCA groups (p < 0.05). Therefore, it can be concluded that MHCA does not increase the risk of cerebral injury. Considering the adverse effects of DHCA on the coagulation system, MHCA is more suitable for current clinical practice.
Introduction
Currently, cardiopulmonary bypass (CPB) in conjunction with hypothermic circulatory arrest (HCA) is used for aortic arch and other complex congenital heart defect repairs (Lai et al., 2002; Ehrlich et al., 2003; Khaladj et al., 2008). However, the optimal temperature for HCA remains controversial, and no specific data are available from animal studies directly investigating the different degrees of brain injury induced while performing this procedure at different temperatures. HCA is the most common application used in clinical practice, with a goal of achieving maximal suppression of the cerebral metabolic rate of oxygen consumption (Michenfelder and Milde, 1992; Mezrow et al., 1994), but the 30-day mortality and mortality-corrected permanent neurological dysfunction rates in HCA surgery are still ∼19.4% and 11.5%, respectively (Krüger et al., 2011). HCA has been shown to have deleterious effects on the central nervous system by inducing endothelial dysfunction, apoptosis, and necrosis (Cooper et al., 2000; Ananiadou et al., 2005).
Obtaining a sufficient cerebral sample from humans is presently difficult. Therefore, animal experiments are necessary to perform a systematic analysis of the neuroprotective effects of different HCA strategies. The purpose of this study was to compare the impact of the degree of hypothermia on neurological outcomes using biomarkers of brain injury and determine their capacity in alleviating brain injury in a pig CPB model without selective cerebral perfusion.
Materials and Methods
All procedures were carried out according to a protocol approved by the Beijing Anzhen Hospital Ethics Committee. Animals were obtained from the Beijing Animal Experiment Center of Fuwai Hospital and received care in compliance with the Guide for the Care and Use of Laboratory Animals prepared by the National Academy of Sciences and published by the National Institutes of Health.
Experimental design
Thirteen pigs (Animal Experiment Center of Fuwai Hospital, Beijing) were anesthetized, intubated, placed on mechanical ventilation, and randomized to 30 minutes of circulatory arrest without cerebral perfusion at a nasopharyngeal temperature of 15°C [deep hypothermic circulatory arrest (DHCA) group, n = 5] or 25°C [moderate hypothermic circulatory arrest (MHCA) group, n = 5]. The other three pigs were used as a control group that was sacrificed directly without surgery. There were no differences in the preoperative age or weight of the pigs across the groups (4–5 months old and weighing 100.2 ± 5.1 kg). HCA was performed for 30 minutes. Blood samples were obtained at each time point, as shown in Figure 1. The whole blood was directly placed on the heparin sodium tube and vibrated uniformly. The plasma was obtained by centrifugation at 3000 rpm for 5 minutes at 4°C. The sample was stored at −80°C. The sample was taken out and naturally thawed at 4°C before the test. The supernatant was taken for testing at 3000 rpm for 1 minute before the test. The time points included the following: T1 = start of anesthesia; T2 = cooling to 32°C; T3 = cooling to the target temperature; T4 = after 30 minutes of HCA; T5 = rewarming to 32°C; T6 = rewarming to 36°C; T7 = 2 hours after rewarming to 36°C; T8 = 4 hours after rewarming to 36°C; T9 = 6 hours after rewarming to 36°C; T10 = 24 hours after rewarming to 36°C. The brain was immediately removed by craniotomy and divided by a midsagittal cut. The frontal cortex was subjected to immunohistochemical analysis to examine the neurologic outcomes.
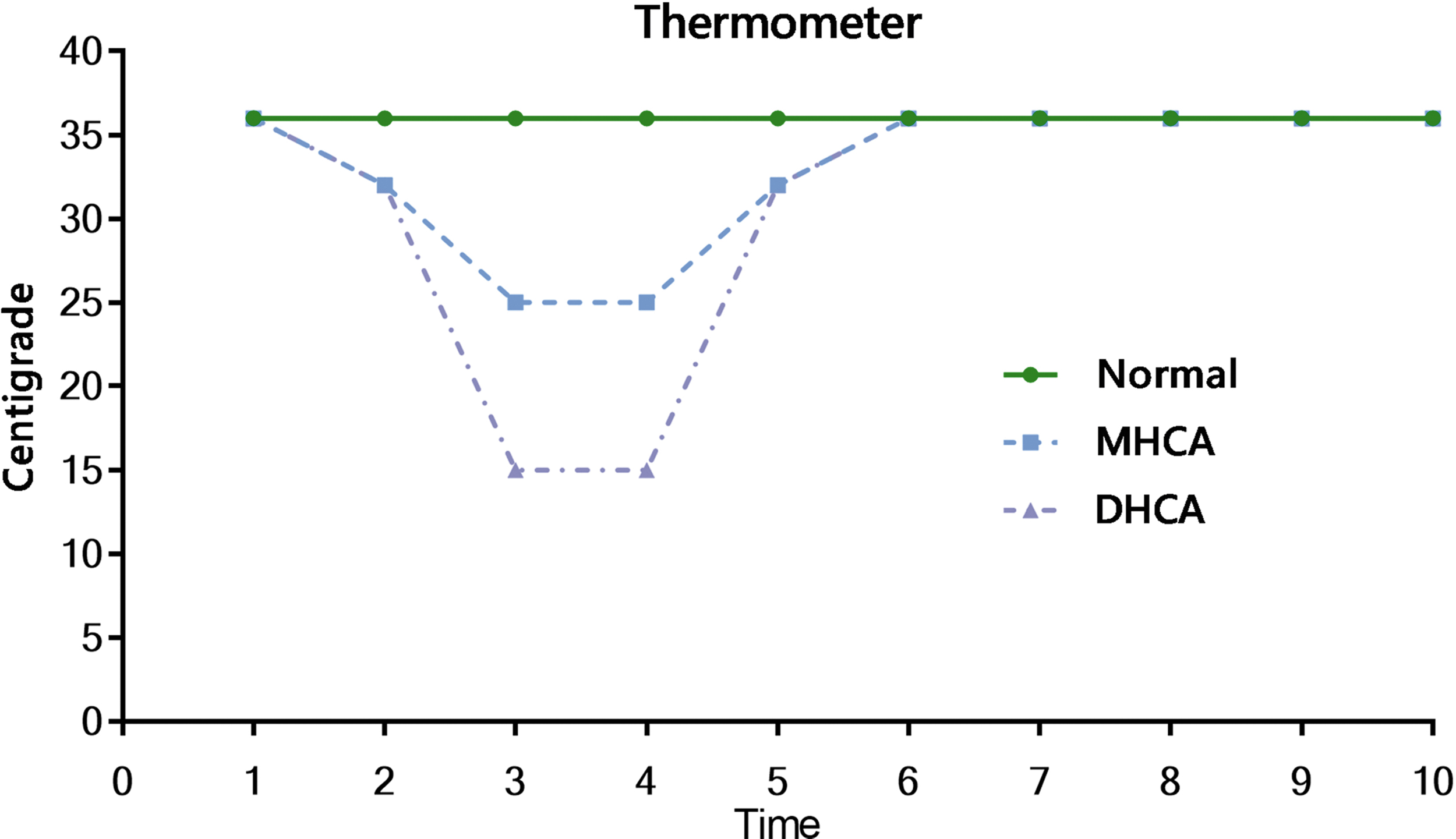
Temperature of the normal control group was controlled at 36°C. Temperature of the DHCA group can reach 15°C, and that of the MHCA group can reach 25°C. The HCA lasted for 30 minutes, and blood samples were collected at 10 time points. DHCA, deep hypothermic circulatory arrest; HCA, hypothermic circulatory arrest; MHCA, moderate hypothermic circulatory arrest.
Vital sign monitoring
Following initial central-line placement and before median sternotomy, an arterial pressure catheter was inserted via the femoral artery for pressure monitoring and blood gas analysis, and a venous catheter was inserted via the right femoral vein for fluid administration and blood sampling. Blood samples (20 mL) were obtained from the right femoral artery. The nasopharyngeal temperature was monitored with an imbedded temperature probe. The hemodynamic variables monitored in this analysis included blood pressure, heart rate, oxygen partial pressure, and electrocardiogram (ECG) traces via the ECG monitor.
Surgical and CPB protocol
The extracorporeal circuit was primed with an injection of gelofusine and sodium lactate ringer's solution. After anesthesia, the ascending aorta was fully freed and the heart was exposed. After heparinization, CPB conduits were inserted into the ascending aorta and right atrium. This process was monitored by the CPB nursing system (MDD, 93/42/EEC, UK). The temperature of HCA was accurately regulated by a variable-temperature water tank (MAQUET, HCU30, Germany). The hematocrit value was 20–24% after induction of CPB. During CPB, the flow was maintained at 90–100 mL/(kg·min), and the average arterial pressure was maintained at 60–90 mmHg. The ascending aorta was blocked, and cardioplegia solution was perfused at the root of the ascending aorta when the nasopharyngeal temperature decreased to 32°C. After achieving the targeted nasopharyngeal temperature, CPB was stopped. In the DHCA group, pigs were cooled for ∼60 minutes. When the nasopharyngeal temperature reached 15°C, the heat exchanger continued to maintain the nasopharyngeal temperature at 15°C, and CPB was stopped. After 30 minutes of HCA, CPB was continued and the pigs were rewarmed to a nasopharyngeal temperature of 37°C. When the hemodynamics stabilized, the pigs were weaned from CPB and allowed to survive for 24 hours. The establishment of CPB and the operation procedure in the MHCA group were the same as those in the DHCA group, except for the target temperature (25°C). No procedures were performed in the control group.
Detection of apoptosis
Cerebral specimens were embedded in paraffin and sliced into 6-mm-thick coronal sections. These specimens were stained for Bax, Bcl-2, and Caspase3 to accurately detect the degree of brain injury. To detect apoptotic cells, sections were stained by deoxynucleotidyl transferase-mediated dUTP-biotin nick end labeling (TUNEL Assay Kit; Sigma, No. 11684795910, USA), according to the manufacturer's instructions. Detailed steps are described in Supplementary Data. An experienced pathologist, blinded to group assignment, counted TUNEL-positive cells under a light microscope. The apoptotic index was calculated as the ratio of apoptotic cell number to the total cell number for four randomly selected high-power fields (200 × magnification). Soluble protein-100B (S-100B) is a protein specifically expressed in the central nervous system, and some studies have shown that S-100B represents neuronal function injury. Therefore, brain injury induced by HCA was also assessed by detecting the S-100B level.
Statistical analysis
The Kolmogorov–Smirnov method was used to detect the normality of data distribution. Measurement data are reported as means and standard deviations, and one-way analysis of variance or the Wilcoxon rank-sum test was used to compare continuous variables. Categorical data are reported as percentages or counts, and a chi-square test or Fisher's test was used for comparisons. A t-test with a Bonferroni correction analysis for repeated measurements was used for comparisons among the 10 time points. SPSS 18.0 (SPSS, Inc., Chicago, IL) was used for all analyses, and a probability value <0.05 was considered statistically significant.
Results
Tissue sample analysis
As illustrated in Figure 2, immunohistochemical staining (Bax, Bcl-2, and Caspase 3) significantly increased in the experimental groups compared with the control group (p < 0.05). Figure 2 shows that no significant changes in Bax, Bcl-2, or Caspase-3 levels were observed between the DHCA and MHCA groups (p > 0.05). Similarly, according to a histogram of fluorescence produced by TUNEL staining, obvious differences were present between the control group and the experimental groups (p < 0.05), but no significant difference was found between the two experimental groups (p > 0.05) in Figure 3.

Expressions of Bax, Bcl-2, and Caspase-3 in the tissue sections of three groups, respectively. The positive factors in the blue box were counted and the corresponding histogram was drawn. The histogram shows that there is a significant difference between the normal group and the experimental group (p < 0.05), but not between the two experimental groups (p > 0.05) *p < 0.05, relevance degree. DHCA, deep hypothermic circulatory arrest; MHCA, moderate hypothermic circulatory arrest.
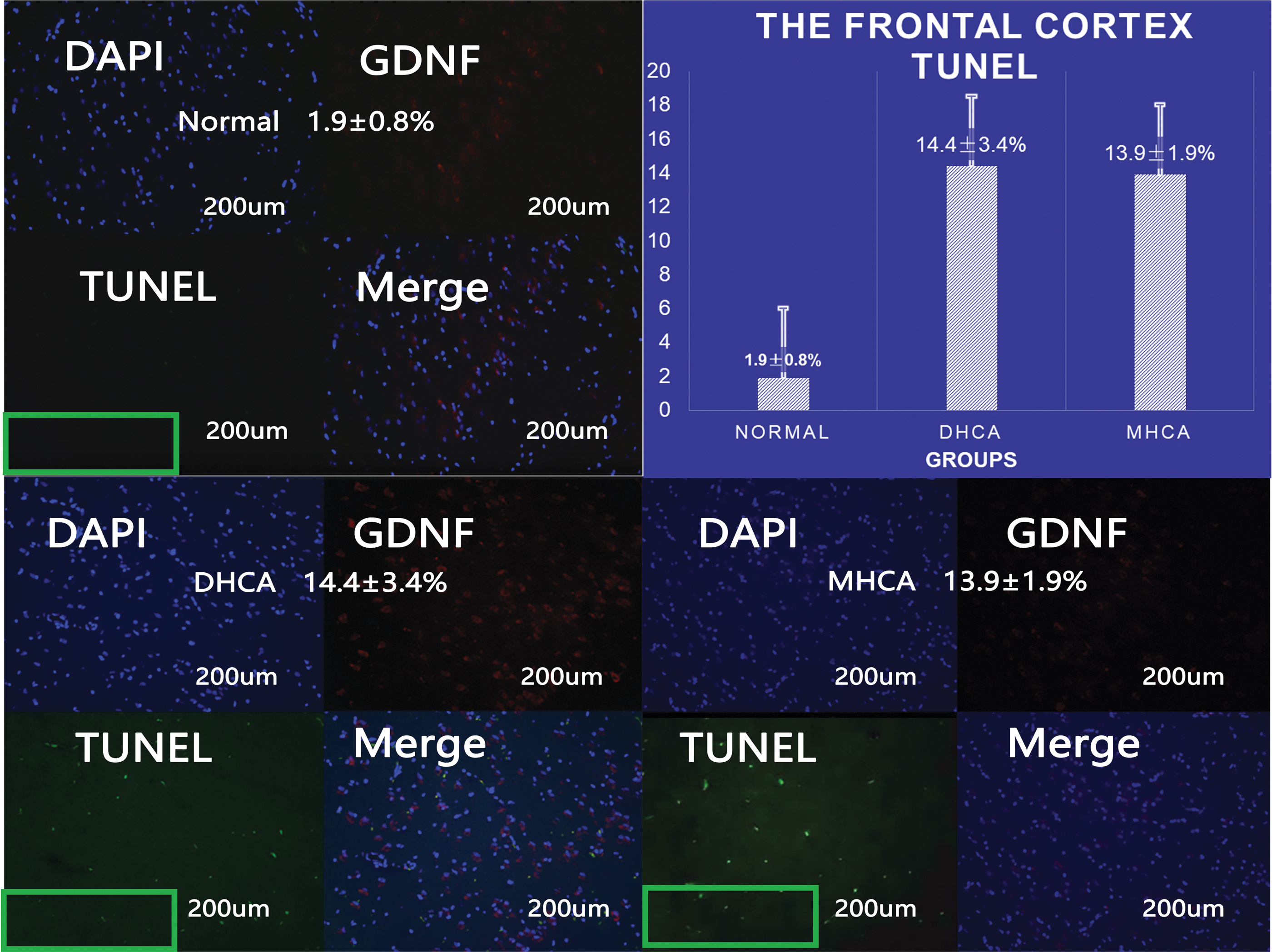
DAPI, GDNF, and TUNEL were used to evaluate the degree of brain neuron injury. To visualize neuron injury, we selected the most significant TUNEL staining. By counting the fluorescence rate of TUNEL staining in the green box and drawing the histogram, we observed obvious differences between the normal group and the experimental group (p < 0.05), but not between the two experimental groups (p > 0.05). DHCA, deep hypothermic circulatory arrest; MHCA, moderate hypothermic circulatory arrest.
Blood sample analysis
S-100B levels are shown in Table 1 and Figure 4. No differences were observed between the two experimental groups at time points T1–T4 (p > 0.05). Although a temporary increase in the S-100B level was observed in the MHCA group after HCA at time points T5–T6 (p = 0.02 and 0.02, respectively), the S-100B level quickly decreased to a level similar to that of the DHCA group after HCA at time points T7–T10 (p > 0.05). No significant differences were observed between DHCA and MHCA in blood gas analysis. Detailed data can be obtained from Supplementary Table S1.

S-100B was detected at each time point in the two groups. There was no difference in S-100B between the two groups except for T5 and T6 time points. MHCA versus DHCA (T5 = rewarming to 32°C; T6 = rewarming to 36°C; p < 0.05). S-100B, soluble protein-100B; DHCA, deep hypothermic circulatory arrest; MHCA, moderate hypothermic circulatory arrest.
Soluble Protein-100B Level Analysis
Note: T1 = anesthesia starting; T2 = cooling to 32°C; T3 = cooling to target temperature; T4 = 30 minutes after HCA; T5 = rewarming to 32°C; T6 = rewarming to 36°C; T7 = rewarming to 36°C for 2 hours; T8 = rewarming to 36°C for 4 hours; T9 = rewarming to 36°C for 6 hours; T10 = rewarming to 36°C for 24 hours.
p < 0.05 DHCA versus MHCA at T5, T6 phases.
DHCA, deep hypothermic circulatory arrest; HCA, hypothermic circulatory arrest; MHCA, moderate hypothermic circulatory arrest.
The levels of inflammatory factors are shown in Figure 5. The trends in inflammatory factors, including tumor necrosis factor-α (TNF-α), interleukin (IL)-2, and IL-6, were similar between the two experimental groups, resulting in no significant differences. Table 2 shows that no difference was observed in the perioperative trends of inflammatory factors between the two groups.
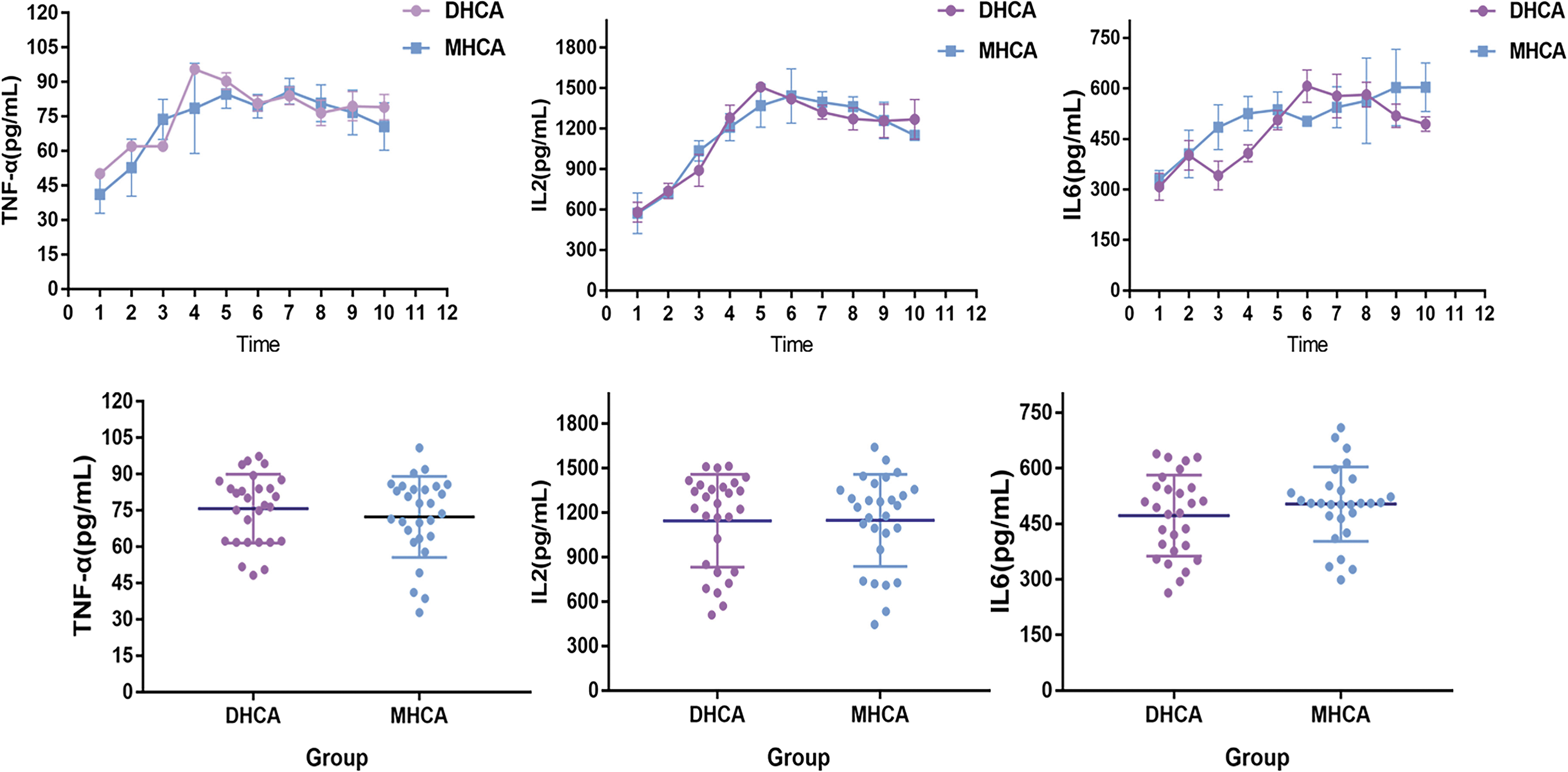
The trend of changes in inflammatory factors such as TNF-α, IL-2, IL-6 between the two experimental groups was similar. There was no statistical difference in matching t-test between the two groups (p > 0.05). DHCA, deep hypothermic circulatory arrest; IL, interleukin; MHCA, moderate hypothermic circulatory arrest; TNF-α, tumor necrosis factor-α.
Blood Sample Detection
Note: No significant differences were observed between DHCA and MHCA in inflammatory factors. Significant differences were observed between DHCA and MHCA in coagulation factors.
p < 0.01, significant relevance degree.
DHCA, deep hypothermic circulatory arrest; IL, interleukin; MHCA, moderate hypothermic circulatory arrest; TNF, tumor necrosis factor.
Changes in coagulation factors are shown in Figure 6. Significant differences were observed in critical coagulation factors, including FXI and FVII, between the two experimental groups (p < 0.05). Additionally, a paired samples t-test showed that the degree of changes in FVII and FXI was similar between the two experimental groups.
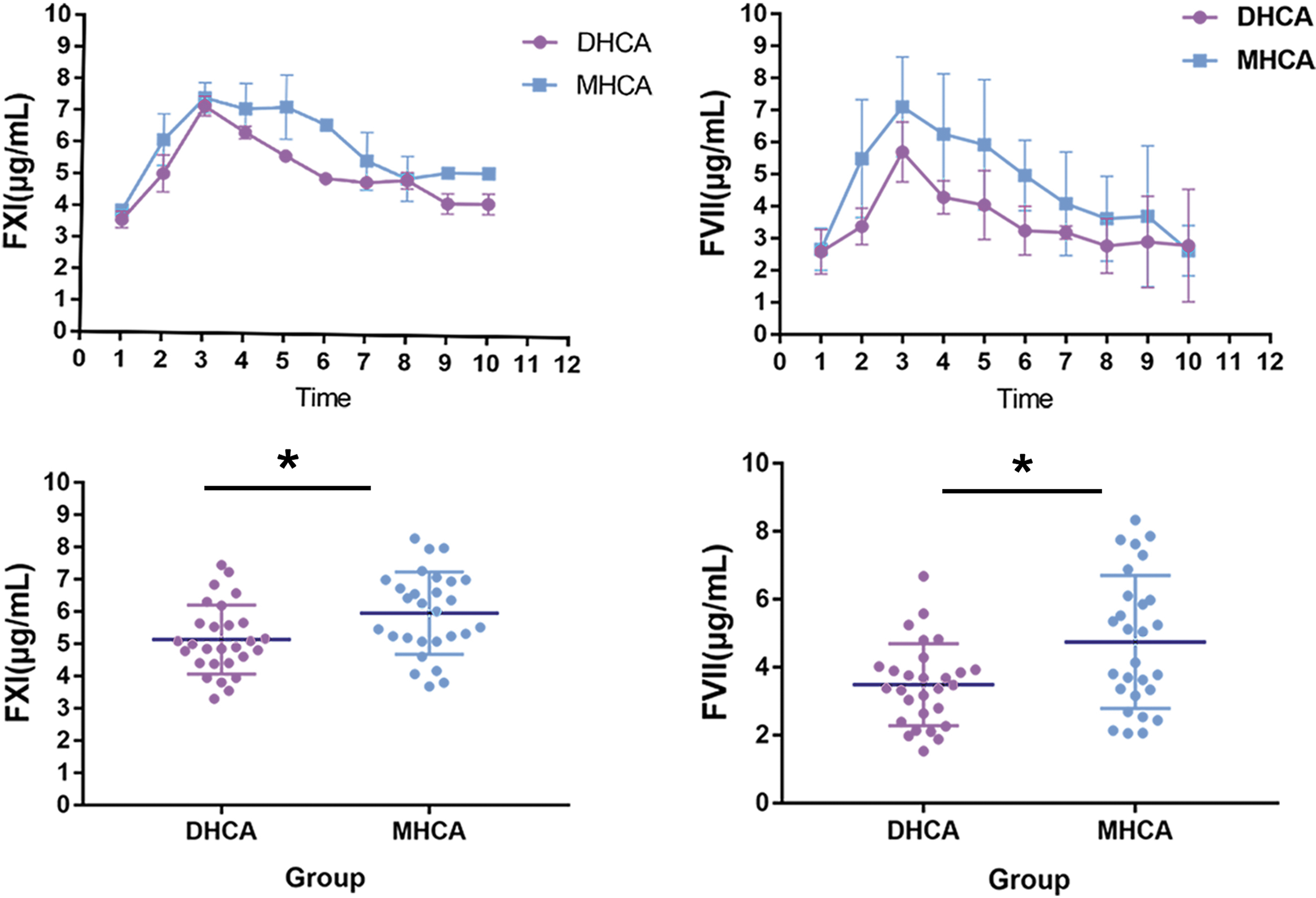
The trend of changes in coagulation factors such as FXI and FVII between the two experimental groups was similar. We observed statistical differences in these critical coagulation factors between the two groups (p < 0.05). *p < 0.05, relevance degree. DHCA, deep hypothermic circulatory arrest; MHCA, moderate hypothermic circulatory arrest.
Discussion
HCA has been used for ∼40 years as a means of interrupting the normal perfusion of the brain and preventing subsequent cerebral ischemic injury during various cardiovascular surgical procedures (Griepp et al., 1975). Aortic arch exploration and repair during the period of HCA is the current consensus management approach among the majority of surgical experts (Lai et al., 2002; Ehrlich et al., 2003; Khaladj et al., 2008). Since the introduction of aortic arch replacement in the 1950s by De Bakey et al. (1957), different degrees of hypothermia have been used during this procedure. HCA is divided into four types: mild hypothermia at 28.1–34°C, moderate hypothermia at 20.1–28°C, deep hypothermia at 14.1–20°C, and profound hypothermia at ≤14°C (Sutton et al., 1991).
In the past, DHCA was favored in clinical practice because it deeply reduced the cerebral metabolic rate, excitatory transmitter release, ion influx, and vascular permeability (Todd and Warner, 1992). However, evidence from clinical studies suggested that the cooling and rewarming phases of DHCA were time-consuming, and the complications due to prolonged CPB remained a serious problem (Greeley et al., 1989; Croughwell et al., 1992; Kirsch et al., 2011). Therefore, MHCA is the most commonly used method of alleviating brain injury during aortic arch surgery in clinical practice (Tarola et al., 2018). However, the HCA temperature that is less harmful to the brain has not been determined. In clinical practice, it is difficult to obtain specimens directly after surgery. In addition, the degree of brain injury can only be indirectly assessed through clinical symptoms. In our study, pigs, which have similar genetic characteristics to humans, were used to establish HCA models. The specimens were collected after surgery, and pathological analysis of the specimens was performed. Along with a comparison of the biological parameters of the brain among the three groups, differences in brain injury without cerebral perfusion were systematically and integrally studied, thereby providing a theoretical basis for the selection of a hypothermic strategy in the treatment of type A aortic dissection.
Studies of the nervous system after HCA have become a topic of interest. However, few studies have examined neuronal injury alone without the application of cerebral perfusion. The use of cerebral perfusion during HCA has become a strategy to minimize neurological injury (Fraser et al., 2008). Most scholars believe that MHCA with cerebral perfusion has similar protective features to those of DHCA. Keeling et al. (2018) reviewed 3265 patients undergoing total aortic arch replacement using antegrade cerebral perfusion and found no difference in neurologic outcomes or in-hospital mortality between the MHCA and DHCA groups. Gong et al. (2016) also reached a similar conclusion. Moreover, Arnaoutakis et al. (2016) found that MHCA with antegrade cerebral perfusion did not appear to be associated with worse postoperative renal outcomes compared with DHCA with retrograde cerebral perfusion. In this study, we did not use cerebral perfusion and determined whether similar conclusions could be drawn.
In our study, we counted apoptotic cells and analyzed the apoptosis index in brain specimens subjected to TUNEL staining. Bax is a water-soluble protein that is homologous to Bcl-2. The Bax gene promotes apoptosis and belongs to the Bcl-2 gene family. Bax overexpression can antagonize the protective effect of Bcl-2 and cause cellular death, and Bcl-2 can inhibit cellular death caused by many cytotoxic factors (Hector and Prehn, 2009; Mohan et al., 2012). In addition, the Bax to Bcl-2 ratio has been found to be a critical factor for the inhibition of apoptosis. Thus, we measured the apoptosis level in cerebral cells using immunohistochemical techniques to determine the number of cells positive for apoptosis-related proteins, such as Bax, Bcl-2, and Caspase-3. Traditional theory suggested that if there is no cerebral perfusion, DHCA will perform better than MHCA (Strauch et al., 2005). However, our results showed no significant differences in cerebral apoptosis tests (Bax, Bcl-2, and Caspase-3). Importantly, S-100B levels quickly recovered in the MHCA group, indicating that the brain injury was similar between the two experimental groups without cerebral perfusion.
TNF-α participates in inflammation through the release of a series of inflammatory mediators. It can increase vascular permeability and cause inflammatory cell infiltration, resulting in tissue damage. Therefore, TNF-α is considered to play an important role in ischemia–reperfusion injury (Yuan et al., 2014; Gullo et al., 2017). In addition, IL-2 is the most important regulator of human cellular immunity. The main immunomodulatory effects of IL-2 include: inducing the proliferation of natural killer cells, increasing and enhancing their natural killing effects, and activating the macrophages and lymphocytes (Steinherz et al., 1996; Morimoto et al., 2005). The plasma concentration of IL-6 is related to severe brain injury. The IL-6 level is a predictor of short-term prognosis of patients with brain injury (Woiciechowsky et al., 2002). Our subsequent studies showed no significant changes in inflammatory factors, including TNF-α, IL-2, and IL-6, between the two experimental groups. Therefore, the degree of inflammation was similar between the two experimental groups. DHCA does not alleviate inflammation as previously thought, which provides theoretical support for our findings in tissue samples.
FXI is activated as a serine protease that promotes coagulation by activating the endogenous coagulation pathway (Schmaier, 2016). Human FVII is the initial enzyme of the exogenous coagulation pathway. It has been widely used to treat patients with bleeding, or patients without hemophilia (Schmaier, 2016). Our study showed that, unlike the inflammatory system, the coagulation system underwent drastic changes when the temperature changed. Changes in FXI and FVII are particularly evident during and after HCA, which is consistent with the notion that lower temperature could inhibit the function of the coagulation system. Among these two coagulation systems, exogenous coagulation system is the most seriously affected by hypothermia.
In fact, our study showed that DHCA did not alleviate more brain injury. DHCA is sometimes associated with complications such as severe bleeding and an increased requirement for blood products (Okita et al., 1997). Our experiment also suggested that an appropriate increase in temperature did not increase the inflammatory reaction even without cerebral perfusion. In conclusion, MHCA requires a shorter cooling and rewarming time compared with DHCA, potentially reducing the brain injury caused by long-term CPB. Compared with DHCA, MHCA has less influence on the blood coagulation system compared with DHCA. Additionally, MHCA did not also aggravate the inflammatory reaction. In the future, MHCA should be used in more surgeries to avoid the adverse effects of DHCA.
Study limitations
This study is subject to some limitations. In this experiment, we used heparin tubes to collect blood samples. This may have had some influence on the experimental results. Due to the cost of large animal experiments, we only tested cerebral tissue samples exposed to temperatures of 15°C and 25°C; we did not conduct further research on other organs, nor at different temperature settings. Further studies on the effects of hypothermia on the blood coagulation and inflammatory systems in piglets are needed.
Conclusions
MHCA is a method that has similar advantages as DHCA, as shown by the similar levels of injury biomarkers and degrees of brain apoptosis. Both were associated with equivalent low risks of cerebrovascular neurological events. But MHCA had less influence on the blood coagulation system and required a shorter cooling and rewarming time compared with DHCA. This study provided evidence for the clinical safety and efficacy of MHCA in emergency aortic arch repair, suggesting that MHCA is more suitable than DHCA in clinical practice.
Footnotes
Acknowledgments
We acknowledge Jiachen Li, Zining Wu, and Yuqiang Pei (Beijing Institute of Heart Lung and Blood Vessel Diseases and Beijing Anzhen Hospital, Capital Medical University, China) for reviewing the article during its development. This study was financially supported by grants from the National Science Foundation of China (81600362), Beijing Municipal Administration of Hospitals' Youth Programme (QML20170602), and The Capital Health Research and Development of Special (2018-2-2-66).
Author Disclosure Statement
The authors have nothing to disclose with regard to commercial support.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.