
Abstract
Effects of brain temperature modulation on cerebral hemodynamics are unclear. We aimed at investigating changes of dynamic cerebral autoregulation (AR) indices during induction of deep hypothermia (HT) in a porcine model mimicking the clinical scenario of accidental HT. Thirteen pigs were surface-cooled to a core temperature of 28°C. High-frequency monitoring included brain temperature, mean arterial blood pressure (MAP), intracranial pressure (ICP), brain tissue oxygen tension (PbtO2), and regional oxygen saturation (rSO2) assessed by near-infrared spectroscopy to calculate AR-indices (pressure reactivity index [PRx], oxygen reactivity index [ORx], and cerebral oximetry index [COx]). Brain temperature decreased from 39.3°C ± 0.8°C to 28.8°C ± 1.0°C within a median 160 minutes (interquartile range 146–191 minutes), reflecting a rapid induction of deep HT (−4°C/h). MAP and cerebral perfusion pressure (CPP) remained stable until a brain temperature of 35°C (69 ± 8 mmHg, 53 ± 7 mmHg) and decreased to 58 ± 17 mmHg and 40 ± 17 mmHg at 28°C (p = 0.031 and p = 0.015). Despite the decrease in MAP and CPP, brain oxygenation increased (PbtO2: +5 mmHg, p = 0.037; rSO2: +7.3%, p = 0.029). There was no change in ICP during HT induction. Baseline AR-indices reflected normal cerebral AR and did not change until a brain temperature of 34°C (ORx), 33°C (PRx), and 30°C (COx). At lower temperature, AR-indices increased (PRx: p < 0.001, ORx: p = 0.02, COx: p = 0.03), reflecting impaired cerebral AR. Cerebrovascular reactivity is impaired at lower brain temperature levels. Although these temperatures are usually not targeted in clinical routine, this should be kept in mind when treating patients with accidental deep HT.
Introduction
Deep hypothermia (HT) (<28°C)
Monitoring cerebral AR is an integral part in the critical care management of hospitalized brain injured patients (Johnson et al., 2016; Rivera-Lara et al., 2017; Gaasch et al., 2018), and a loss of cerebral AR has been linked to secondary brain injury and poor outcome (Donnelly et al., 2016; Gaasch et al., 2018). Most cerebral AR indices are still assessed invasively, including the pressure reactivity index (PRx; moving correlation coefficient of MAP and intracranial pressure [ICP]), the oxygen reactivity index (ORx; moving correlation coefficient between cerebral perfusion pressure [CPP] and brain tissue oxygen tension [PbtO2]), and the cerebral oximetry index (COx; regional oxygen saturation [rSO2] and MAP) (Czosnyka et al., 1997; Jaeger et al., 2006; Rivera-Lara et al., 2017). Based on the lack of feasibility to assess cerebral AR invasively in hypothermic patients in the prehospital setting or perioperatively, we studied the complex interaction of pressure-dependent energy delivery to the brain in the setting of induced deep
Materials and Methods
Detailed information on animal preparation and the protocol of the main experiment are reported elsewhere (Putzer et al., 2016). A summary of important information is given here. This study was approved by the Institutional Animal Care and Use Committee of the University of Innsbruck and the Austrian Ministry of Science, Research and Economy (Protocol number: BMWF-66.011/0027-II/3b/2013). It was conducted at our experimental research unit in compliance with EU regulations for animal experimentation (Directive 2010/63/EU of the European Parliament and the European Council) and reporting is in accordance with current ARRIVE guidelines.
Animal preparation and anesthesia
This study was performed in 13 domestic pigs weighing between 35 and 50 kg. The pigs were fasted overnight with free access to water. Premedication was done with azaperone (4 mg/kg IM; Jansen, Vienna, Austria) and atropine (0.01 mg/kg IM). Anesthesia was induced with ketamine (25 mg/kg IM) and propofol (1 mg/kg IV). After endotracheal intubation during spontaneous ventilation, the pigs were ventilated volume-controlled (Evita 2; Draeger, Lübeck, Germany) with 21% inspiratory oxygen and a tidal volume of 6–8 mL/kg body weight to maintain normocapnia (35–45 mmHg). During
Neuromonitoring
A near-infrared spectroscopy (NIRS) optode (INVOS™ System; Somanetics, Inc., Troy, MI) was placed on the right forehead for rSO2 measurements. A brain tissue oxygen catheter (LICOX; Integra NeuroSciences, Ratingen, Germany) and a combined ICP/Temperature probe (Neurovent-P Raumedic, Münchberg, Germany) were placed in the white matter of the corresponding region of the left hemisphere. Arterial catheters were attached to pressure transducers (1290A; Hewlett Packard, Böblingen, Germany) and calibrated at the level of the meatus acusticus for CPP calculations. Hemodynamic and respiratory variables were measured and analyzed by using an AS/3 Monitor (Datex-Ohmeda AS/3; GE Health-care, Buckinghamshire, UK).
Study protocol and cooling procedure
The study protocol mimicked the scenario of a severely hypothermic patient. After calibrating the LICOX probe according to the manufacturers' specifications, the experimental protocol was commenced with baseline measurements of hemodynamic, respiratory and cerebral oxygenation parameters and blood gases. The pigs were then surface-cooled with crushed ice until a core temperature of 28°C was reached. At this point, recordings for this analysis were stopped and the protocol continued as previously described (Putzer et al., 2016). After completion of the experimental protocol, the animals were euthanized.
Measurements
High-frequency measurements included MAP, ICP, end-tidal CO2 (etCO2), oxygen saturation (SpO2) and regional tissue (rSO2), and PbtO2. CPP was calculated as the difference between MAP and ICP.
AR indices (PRx, ORx, and COx) were calculated as originally described (Czosnyka et al., 1997; Jaeger et al., 2006; Rivera-Lara et al., 2017): A moving Pearson correlation of 30 ten-second intervals between ICP and MAP for PRx and between rSO2 and MAP for COx was calculated. For ORx, 120 one-minute intervals were used, to correlate PbtO2 und CPP. For every moving window, a minimum of 50% of data points had to be available to calculate a value. Blood gases were taken at baseline and stepwise during the cooling period at every 2°C temperature drop (Table 1). Overall, brain temperature was used for analysis, if not mentioned otherwise.
Arterial Blood Gases at Different Temperature Levels
Note that brain temperature highly correlated with core temperature. (r = 0.995, p < 0.001).
Significant compared
Statistical analysis
We used SPSS (v24; IBM) for statistical analysis. To correct for piglet weight and different duration of cooling time, we calculated the percentage of cooling time (down to 28°C) and used this variable as longitudinal reference. Statistical analysis for repeated measurements was done, using univariate and/or multivariate generalized estimating equation (GEE) models, with the correlation matrix best fitting the data and fitting selection criteria as described elsewhere (Gaasch et al., 2018). Linear mixed-effects analysis was performed in R (R Core Team, 2012) and lme4 (Bates et al., 2012), with predicted values obtained by using the ggpredict() function (Lüdecke, 2018). Important co-variates are specified in the Results section. For group differences, Student's t-test or Mann–Whitney U tests were used as appropriate. Multiple comparisons in GEE models were corrected by using the Least Significant Difference method; otherwise, no correction for multiple comparisons was used. A p-value <0.05 was considered statistically significant.
Results
Data from 13 pigs were obtained and included in the analysis. The pigs had a median weight of 38 kg (interquartile range [IQR]: 36–43) and were 110.5 cm long (IQR: 108.5–115.0). All pigs were male except for one.
Temperature
Mean baseline core temperature was 39.3°C ± 0.8°C and significantly decreased by 10.5°C (95% confidence interval [CI]: 9.7–11.5, p > 0.001) to 28.8°C ± 1.0°C after 160 minutes (IQR: 146–191 minutes). Brain and core temperature were highly correlated (r = 0.995, p < 0.001).
Neuromonitoring
ICP did not change over time (16 ± 0.9 mmHg at baseline and 17 ± 1.7 mmHg at 28°C). Baseline MAP and CPP were 69 ± 8 mmHg and 53 ± 7 mmHg, respectively, and remained constant until a temperature of 35°C was reached. Thereafter, MAP and CPP significantly decreased to 58 ± 17 mmHg (p = 0.031) and 40 ± 17 mmHg (p = 0.015) at 28°C brain temperature (Fig. 1).

Time course of CPP during the induction of hypothermia (mean ±95% CI). CPP, cerebral perfusion pressure; MAP, mean arterial blood pressure; PbtO2, brain tissue oxygen tension.
PbtO2 significantly increased from 9 ± 3 mmHg to 14 ± 5 mmHg during the cooling period (p = 0.037). This change remained significant even after correcting for end-tidal CO2 (p = 0.012).
Baseline rSO2 increased during the cooling period from 54% ± 3% to 62% ± 11% at 29°C (+7.3; 95% CI: 0.5–9.2; p = 0.029).
Cerebral AR indices
The time course of all measured cerebral AR indices is shown in Figure 2. Baseline AR-indices reflected normal cerebral AR in all pigs and did not change significantly until a temperature of 34°C (ORx), 33°C (PRx), and 30°C (COx) was reached. At lower temperatures, AR-indices significantly worsened: from −0.10 ± 0.25 to +0.34 ± 0.35 at 28°C (p < 0.001) for PRx, from 0.12 (±0.18) to 0.16 at 28°C (+0.28, p = 0.018) for ORx, and COx increased by 0.15 to a maximum of 0.17 ± 0.14 (p = 0.03), reflecting impaired cerebral AR. PRx and ORx correlated comparably well (r = 0.15 p < 0.01). There was no correlation between COx and PRx or ORx (p = 0.23, p = 0.28).
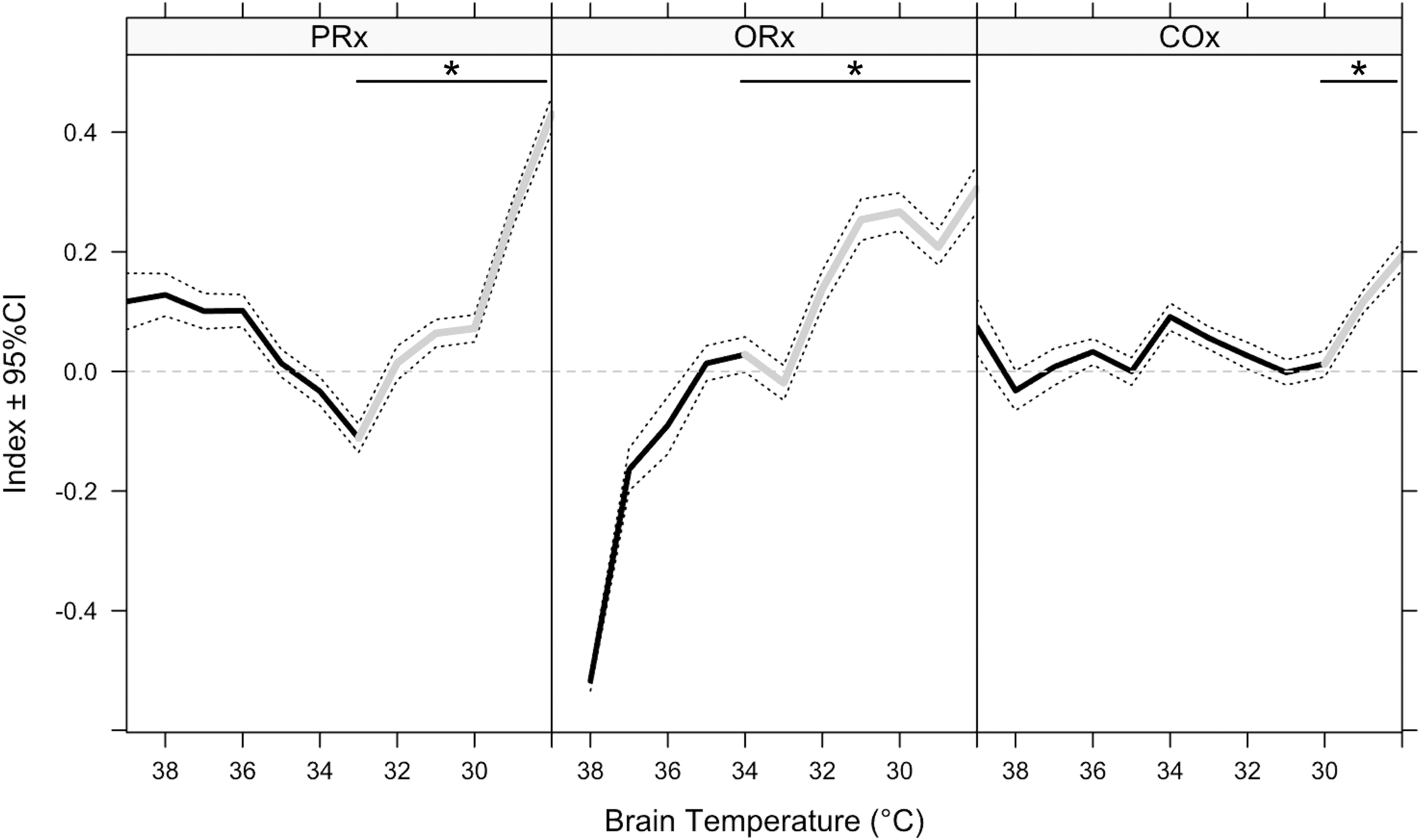
Time course of cerebral autoregulation indices over the cooling period (mean ±95% CI). *Difference significant p < 0.05. CI, confidence interval; COx, cerebral oximetry index; ORx, oxygen reactivity index; PRx, pressure reactivity index.
In a mixed-effects model, brain temperature remained significant (χ2 = 319.9, p ≤ 0.001) and PRx was further associated with heart rate (HR) (χ2 = 7.1329, p < 0.01), MAP (χ2 = 17.937, p < 0.001), and EtCO2 (χ2 = 4.44, p = 0.03). ORx was associated with brain temperature (χ2 = 66.39, p < 0.001) and was also influenced by MAP (χ2 = 57.125, p < 0.001) and EtCO2 (χ2 = 655.86, p < 0.001). No significant association was seen for ORx and HR (p = 0.053). In this mixed model, COx showed an insignificant association to brain temperature (p = 0.12). It was, however, associated with MAP (χ2 = 114.87, p < 0.001), HR (χ2 = 12.28, p < 0.001), and EtCO2 (χ2 = 7.38, p < 0.01).
End-tidal CO2 significantly decreased from 38.25 mmHg (±1.95) at 39°C to 22.5 mmHg (±5.17) at 28°C (p < 0.01).
Fraction of inspired oxygen (FiO2) was kept constant during the whole cooling period at 21% ± 0.9%. Hematocrit and hemoglobin levels were comparable in all piglets with a median of 24% (IQR: 23–25%) and 8.2 mg/dL (IQR: 8.2–8.2 mg/dL), respectively.
Discussion
The main finding of this study is that mild
Cerebrovascular AR refers to the ability of the brain vessels to regulate cerebral blood flow (CBF) over a wide range of CPP levels (Donnelly et al., 2016). When CPP decreases below the lower or above the upper inflection point of the cerebral AR curve, oxygen and glucose delivery solely depend on the perfusion pressure. This evidentially results in cerebral hypoperfusion and ischemic brain injury when CPP is too low, or cerebral edema and raised ICP when CPP is raised above the upper inflection point of the cerebral AR curve (Skinhoj and Strandgaard, 1973). Besides other factors (Donnelly et al., 2016),
Controlled
Cerebral AR indices, which were introduced in the management of the critically ill neurological patient in the 1990s (Czosnyka et al., 1997), may allow for monitoring of AR integrity and facilitate individual adjustments of MAP to improve cerebral perfusion in hypothermic patients. Today, many indices of cerebrovascular AR have been described. The PRx relates to the correlation between MAP and ICP (Czosnyka et al., 1997). It shows negative values while AR is preserved, whereas with impaired AR an increase in MAP will cause passive dilation of cerebral vessels and, consequently, an increase in CBF and ICP, resulting in positive PRx values. Analogous, the ORx describes the relationship between CPP and PbtO2 (Jaeger et al., 2006), and the COx between COx between MAP and rSO2 (Rivera-Lara L et al., 2017). When cerebral vessels are pressure passive because of impaired AR, an increase in CPP will lead to an increase in CBF and oxygen delivery and therefore PbtO2 and rSO2. Thus, both indices will be positive. Cerebral oxygenation depends on many aspects alongside cerebral AR. The physiological cascade assessed by oxygen derived indices such as ORx and, to an even greater extend, COx, may be influenced by physiological and environmental circumstances which may further be determined by temperature. This limitation should be kept in mind when comparing ORx and COx to other indices such as the pressure derived PRx.
There is no consensus on which index is best used (Donnelly et al., 2016), as they represent very different physiological aspects (Zeiler et al., 2017). We, therefore, assessed all three AR indices and observed the same trend when analyzing relative changes over time. Cerebral AR was relatively stable during mild
Our data further demonstrate that
Despite impaired AR status and a decrease in perfusion pressure in our experiment, we observed an increase in brain oxygenation. In a state of impaired cerebral AR, the observed increase in PbtO2 may be due to hyperemia; however, given the low levels of MAP alongside the lack of ICP increase usually accompanying hyperemia (Kelly et al., 1996), the changes in PbtO2 may more likely be interpreted as a decrease in energy consumption caused by metabolic suppression during
The findings of this experimental study may not directly be transferable to humans. Piglets have higher body temperature at rest (Hannon et al., 1990), thus, the temperature levels at which impaired AR was documented may not be the same in humans. Also, ICP values observed in our study seem high in comparison to humans. However, our findings are compatible with previous studies reporting ICP values for sedated pigs in supine position (Yannopoulos et al., 2006; Heuer et al., 2012; Putzer et al., 2018). Further, accidental
During
Conclusion
In conclusion, we found evidence of impaired cerebral AR during induced deep
Footnotes
Acknowledgments
This work was funded by the Department of Anesthesiology and Critical Care Medicine, Medical University of Innsbruck, Innsbruck, Austria; and the Institute of Mountain Emergency Medicine at the European Academy, Bolzano, Italy.
Author Disclosure Statement
No competing financial interests exist.