
Abstract
Targeted temperature management (TTM) is an important treatment modality in pediatric neurocritical care. There are different types of devices available to deliver this therapy, but limited pediatric data exist. This quality improvement study evaluates the use of a surface cooling device that uses gel-adhesive pads for TTM in critically ill pediatric patients. An institutional TTM protocol to use the gel-adhesive pad system was developed with three different temperature goals: normothermia (goal temperature 37°C), mild hypothermia (goal temperature 35°C with rewarming duration of 12 hours to normothermia), and moderate hypothermia (goal temperature 33°C with rewarming duration of 24 hours to normothermia). Protocol and device implementation required several different educational sessions for all members of the critical care team. An exploratory analysis was performed for 19 patients with complete clinical and device temperature data. The most common protocol used was normothermia (73.6%). By protocol, time to goal temperature was 58 minutes (22.0–112.8) for normothermia, 46.5 minutes (44.3–48.8) for mild hypothermia, and 93 minutes (46.5–406.5) for moderate hypothermia. Patients remained within ±0.5°C temperature goal 99% (96.0–99.3) of the time in the normothermia protocol, 99.5% (99–100) in mild hypothermia, and 93% (80–100) for the moderate hypothermia protocol. Shivering was the most common adverse event (35%). Our results show that use of the gel-adhesive pad system for pediatric TTM is feasible, efficacious with regard to achieving both a short time to target temperature and maintaining temperature goal, and, in this limited sample, was free from major adverse events. We also defined several technical aspects of device use in pediatric patients that should be considered in future trial design and/or clinical use. Further studies are needed to determine if this device is superior to other cooling devices for temperature management in the pediatric population.
Introduction
Fever (≥38°
Conventional methods for temperature control used commonly in the pediatric intensive care unit (PICU), such as the use of cold packs, surface cooling blankets, and intravenous cold fluids, are effective in temporary temperature reduction but often fail to maintain desired TTM goals with sufficient precision (Larsson et al., 2010; Fink et al., 2012). Commercially available devices that provide surface or intravascular cooling may facilitate faster time to achieve goal temperatures and more accurate maintenance of target temperatures (Pichon et al., 2007; Topjian et al., 2011). Studies in adult patients that compared the efficacy of these different devices for TTM suggest that endovascular cooling and surface cooling with a gel-adhesive pad system are superior to traditional surface cooling blankets that rely on water circulation for both induction time to goal temperature as well as time within target temperature (Sonder et al., 2018). Data in pediatrics are limited. In pediatric critical care, the use of endovascular catheters is limited by the diameter of the catheter relative to the vessel and the length of the catheters relative to children's inferior vena cava length (Topjian et al., 2019). To date, there are no studies evaluating the efficacy of surface cooling devices using gel-adhesive pad systems within pediatrics.
The aim of this study was to evaluate the feasibility and efficacy in inducing and maintaining target temperature using a gel-adhesive pad system in critically ill pediatric patents. We also assessed whether or not this approach was associated with adverse events. This study reports on the implementation and quality improvement (QI) metrics at a single-center PICU, including time to target temperature, time within goal temperature range, feasibility of implementation, and adverse events related to use of therapy.
Materials and Methods
This was a QI project to develop, implement, and evaluate a TTM protocol for a gel-adhesive pad system specific to critically ill infants and children at the University of Pittsburgh Medical Center (UPMC) Children's Hospital of Pittsburgh (CHP). UPMC CHP is a quaternary Level I children's hospital with a 36-bed PICU. The CHP PICU is staffed by 18 critical care attendings, 14 critical care fellows, 2 advance practice providers, 5–6 pediatric residents during each clinical rotation, 174 critical care nurses, 1 clinical nurse educator, and 1 programmatic nurse specialist in the educational support role. Education and protocol development began in December 2016 with device implementation in March 2017. Patient data were collected for this QI project from May 2017 to April 2019. This project and publication was approved by the UPMC CHP Quality Review Committee.
The Arctic Sun® 5000 Temperature Management System (Becton Dickinson & Co., Medivance, Louisville, CO) incorporates use of hydrogel surface pads through which water circulates. Pads are placed on the body to cover 40% of the body surface area (BSA). For older children and adolescents, pads are placed on the skin of the back, chest, abdomen, and both thighs. For infants and smaller children, pads are placed on the back, chest, and abdomen with thigh optional. Recommendations for pad sizing and placement are based on patient's weight in kilograms and provided by the company. The pads are connected to the control unit that adjusts the water temperature as needed to maintain temperature goals. Water temperature ranges between 4°C and 42°C and will adjust every 2 minutes based on the patient's temperature to reach the set temperature goal. For additional patient safety, we limited the water temperature parameters to 10–40°C on the device used for this implementation.
Our institutional TTM protocol was developed by a multidisciplinary team that included critical care physicians as well as nursing educators and leadership (Supplementary Data). This protocol included (1) guidelines to attain and maintain target temperature and rewarming (when applicable), (2) patient eligibility criteria for device use, (3) recommendations for temperature probe positioning, pad sizing based on patient weight, and pad positioning, (4) specific instructions based on protocol selected with screenshot instructions to walk end user through device setup, (5) recommended medical adjuvants for temperature control (e.g., acetaminophen administration, cold saline infusion, and ice packs) as well as sedative and neuromuscular blockade (NMB) requirements, and (6) monitoring for adverse events associated with TTM (including clinical nursing assessments and laboratory and vital sign monitoring).
Three specific TTM protocols were developed based on published evidence and division consensus: (1) normothermia (goal temperature 37°C), (2) mild hypothermia (goal temperature 35°C with recommended rewarming duration of 12 hours to goal of 37°C), and (3) moderate hypothermia (goal temperature 33°C with recommended rewarming duration of 24 hours to goal of 37°C). Recommended hypothermia duration was 24 hours, but may be modified by the team up to 72 hours. Total duration of therapy was determined by clinical team, but limited to a total length of 5 days. Device use on a given patient was restricted to a maximum of 5 days (unless extenuating circumstances were determined that necessitated longer periods of therapy) as the unit was limited to only one device and surface pads were recommended to be changed at that frequency by the company. Alterations to protocol targets were permitted if determined clinically appropriate per the treating critical care physician. To ensure accurate temperature measurements, our protocol preferentiated the use of esophageal temperature probes. Finally, both sedation and NMB were recommended in the protocol to assist with patient comfort, to minimize shivering, and reduce cerebral metabolic demands. However, use of these medications were at the discretion of the treating critical care physician.
Education regarding the device and the institutional protocol were disseminated to the PICU physicians and nursing staff using multiple methods. In-service educational sessions for TTM protocol, device use and device setup were provided to physicians and nursing by our PICU educational team consisting of clinical nurse educator, physician lead, and designated “super-users” in collaboration with representatives from Becton Dickinson & Co. These sessions occurred before device introduction at PICU staff meetings (nurse and physician) and for several nursing shift huddles within the immediate implementation period. In addition, educational refreshers continued during semiannual unit education fairs, PICU new hire nurse orientation, an annual hospital-wide trauma fair, and “just-in-time” with therapy initiation. Sessions involved hands-on simulation with a trainer device provided by Becton Dickinson & Co. that could operate in hypothermia and normothermia training modes. In addition, a select group of physician and nursing “super-users” were identified. This group received advanced educational training that included more detailed knowledge about the device, common pitfalls, and troubleshooting recommendations.
Electronic educational materials were disseminated to all providers to review the protocol and device both before the device launch and also as reminders throughout the initial rollout period. “Real-time” education was provided by nursing educators during therapy initiation and throughout the treatment course. If any issues were identified with device use, immediate review was performed with all care providers and appropriate recommendations for improvement were provided. Finally, interim reports regarding device use as well as educational updates were provided at divisional QI and safety meetings. Representatives from Becton Dickinson & Co. assisted in our educational rollout for all providers in the PICU through various timepoints during this QI project but were not involved in consultation for clinical management nor provided any equipment for use by CHP gratis.
To assess device accuracy, clinical data and device temperature data were obtained for patients placed on the gel-adhesive pad system device for the 2-year assessment period. Data obtained from the device permitted calculation of case duration in hours, protocol in which the device operated, time to target temperature in minutes, and a percentage of time spent within one degree of target temperature (±0.5°C). Clinical data included patient demographics, indication for TTM use, adjuvants used for temperature control, use of sedation and NMB, and adverse events related to device use. These data were collected by the bedside nurse and then verified by retrospective chart review. Any cases with incomplete data due to missing clinical or device data were excluded from analysis.
Descriptive statistics were compiled for demographic data, type of TTM, reason for TTM, starting temperature, length of TTM therapy and duration of rewarming, TTM adjuvants used, use of sedation and NMB, adverse events, and length of stay. Categorical variables were described using frequencies and percentages. Continuous variables were described using median and interquartile ranges. Statistical analysis was performed using RStudio (Boston, MA). Representative temperature curves were created using Graphpad Prism version 7 (San Diego, CA).
Results
There were a total of 46 cases using the gel-adhesive pad system between May 2017 to April 2019. The most common TTM protocol initiated was normothermia (n = 35, 76.1%), with the remainder being mild or moderate hypothermia cases. Just under half of the cases (41.3%) had complete data sets (both clinical and device data) obtained for analysis (Fig. 1). Of the 27 excluded cases, just more than half of them were excluded because of missing clinical documentation (n = 14). The majority of the excluded cases were in the normothermia protocol (59.3%, n = 16).
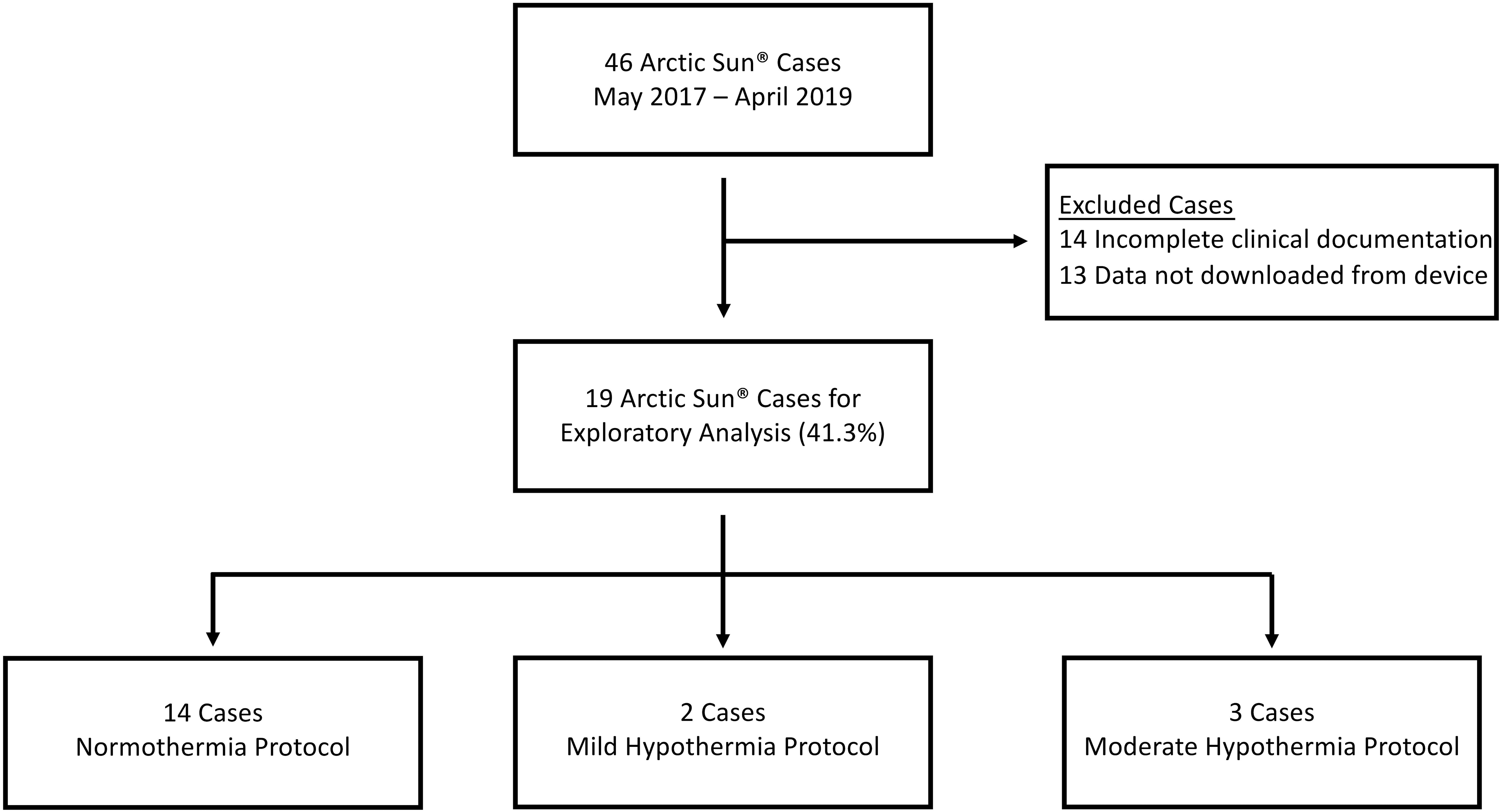
Consort flow diagram.
Demographic information for the 19 cases with complete data is shown in Table 1. The primary clinical indication for TTM management in the normothermia protocol was traumatic brain injury (n = 7, 50.0%). Cardiac or respiratory arrest was the most common clinical indication for both hypothermia protocols. One case of refractory status epilepticus was placed on the moderate hypothermia pathway. The patients in the mild hypothermia group were younger (1.38 years [0.83–1.92]) compared with those in the normothermia protocol (7 years [1.74–13.5]) and moderate hypothermia (5 years [0.17–14]). Patients placed on the normothermia protocol had a higher starting temperature than those placed on the hypothermia pathways (38.2°C [37.6–38.9] vs. 28.0°C [28.0–29.0] for mild hypothermia and 35.2°C [30.1–35.2] for moderate hypothermia).
Clinical and Device Data for Targeted Temperature Management Cases by Protocol
There was one patient where the BSA was not recorded.
Initial admission temperature was 28°C, the patient was rewarmed in manual mode to 33°C and then placed in the mild hypothermia pathway. The patient was placed in rewarm phase to reach 35°C and then maintained at this temperature for the remainder of the case without ever being placed into the normothermia mode on the device.
There were manual manipulations of the temperature goals throughout the duration of this case. The patient was transitioned into rewarm phase before the targeted hypothermia phase was completed.
BSA, body surface area; LOS, length of stay; NMB, neuromuscular blockade; PICU, pediatric intensive care unit; TBI, traumatic brain injury.
Median length of therapy for patients in the normothermia protocol was 101.3 hours (69.6–163.3), 106.6 hours (103.1–109.9) in mild hypothermia, and 82.6 hours (80.2–102.5) for moderate hypothermia. Time to target temperature was <60 minutes for both the normothermia and mild hypothermia cases (58 minutes [22.0–112.8] and 46.5 minutes [44.3–48.8], respectively). However, for moderate hypothermia the median time to reach target temperature was 93 minutes (46.5–406.5) (Fig. 2A). The percentage of time that patients remained within ±0.5°C of goal temperature was >99% for both the normothermia and mild hypothermia protocols (99% [96–99.3] and 99.5% [99–100], respectively), and >93% for the moderate hypothermia protocol (93% [80–100]) (Fig. 2B). There were three deaths at hospital discharge in the group managed by normothermia (21.4%), one death in the mild hypothermia group (50%), and one death in the moderate hypothermia group (33.3%). Further survival analysis cannot be completed due to the small sample size.
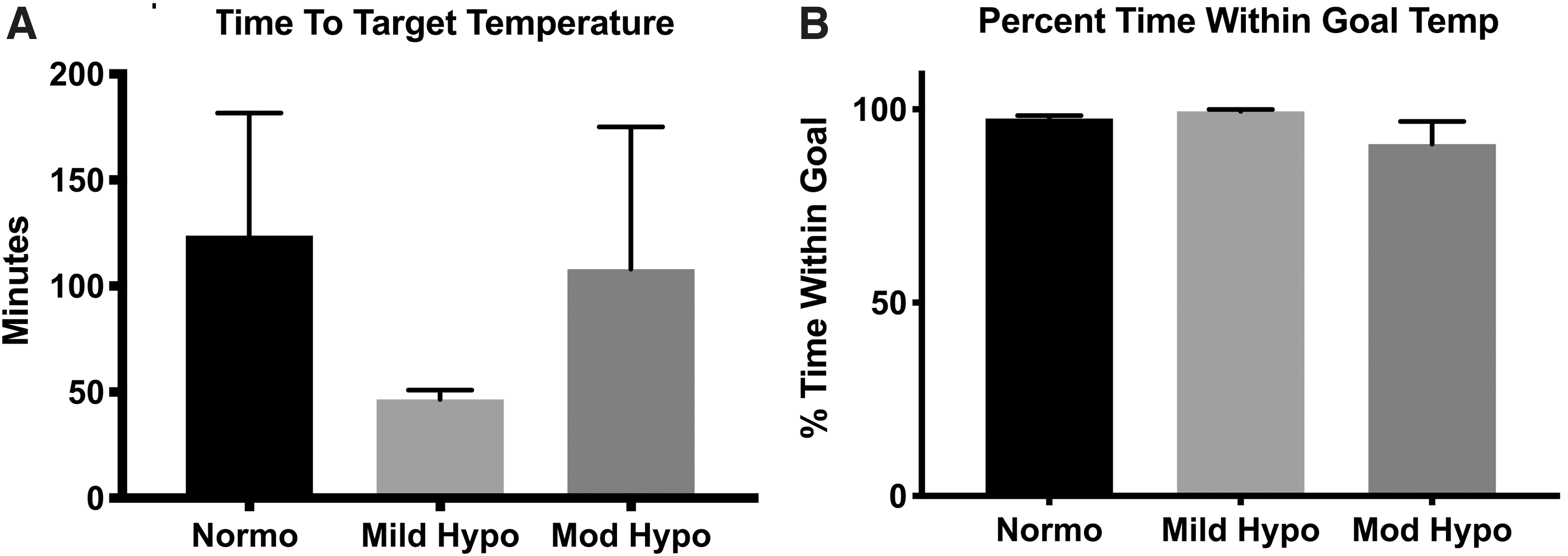
Time to reach target temperature
Figure 3 shows representative temperature curves for patients while on the TTM protocols and for a subsequent 12 hours after therapy discontinuation. Figure 3A illustrates a patient on the normothermia protocol with target temperature of 37°C. The patient's starting temperature was 39.2°C and total duration of therapy was 51 hours. This case showed rapid time to target temperature, minimal amount of time outside of target, and maintenance of temperature once device was discontinued. Figure 3B represents a patient on the mild hypothermia protocol with a goal temperature of 35°C. This patient's starting temperature was 33°C and after 60 hours period of targeted hypothermia, rewarming was performed to 36.5°C for a 24 hours period. Of note, manual manipulations were made to the target temperature on the device by the bedside team to achieve this rewarming rate, which was a point addressed in education to all providers. The patient had several measured temperatures above target range when therapy was discontinued. Total duration of therapy was 127 hours.

Representative temperature curves on gel-adhesive pad system for patients on each of the three protocols: normothermia
Figure 3C demonstrates the temperature curve for a patient in moderate hypothermia protocol, goal temperature 33°C. The patient's starting temperature was 30.1°C. After the targeted hypothermia period of 24 hours, the patient was rewarmed for a 20 hours period to a goal of 36°C. During the normothermia phase, the patient experienced several hour-long periods where the device was disconnected and the pads were removed to facilitate imaging or interventional procedures. During this time, the patient had a noted decrease in temperature to 33.6°C. The patient's temperature was maintained at goal after discontinuation of therapy. Total case duration was 188 hours. Figure 3D represents temperature data for patient in the moderate hypothermia protocol that had a starting temperature of 35.2°C at the time of device application and required active cooling by the device to reach goal temperature. Of note, the patient's temperature at admission was 38°C, but the patient was cooled with passive measures to the starting temperature of 35.2°C with therapy initiation. The patient reached goal temperature of 33°C within 4 hours (0.5°C/h). There were several issues with this case, including inconsistencies between rectal and esophageal probe measurements with the rectal probe reading a higher temperature at the start of therapy. In addition, there were manual manipulations for the target temperature in addition to the device being placed in the wrong phase of therapy, thus explaining the documented time in the rewarm phase for the majority of the case duration. Given this issue, the figure illustrates the periods for therapeutic cooling, rewarming, and maintenance based on the clinical course. During the rewarming phase, the patient had an appreciable sharp change in temperature, which correlates to the environmental exposure during bath. The patient was rewarmed to a goal of 36°C. It should be noted that the patient had been transitioned from the device to the traditional cooling blanket because of shivering when off of NMB after this rewarming; however, the shivering continued, which required reinitiation of NMB. Total case duration on the device was ∼77 hours.
Temperature trends for the first 48 hours for the normothermia cases are shown in Figure 4. Initially, appreciable variation in temperatures are shown given the known differences in patient starting temperatures. However, this graph shows that once goal temperature is reached, temperatures appear to be maintained within goal with minimal deviation from the mean. For all three protocols, we also evaluated the device logs for extreme outliers of temperatures as a surrogate measure for evaluating device inaccuracy as well as safety of temperature control. In the normothermia cases, two patients had a temperature recorded >38°C. None of the patients in the normothermia protocol had temperatures recorded <32°C. In the hypothermia cases, none of the patients had temperatures recorded >38%. There was one patient in the moderate hypothermia protocol that a temperature recorded <32°C.
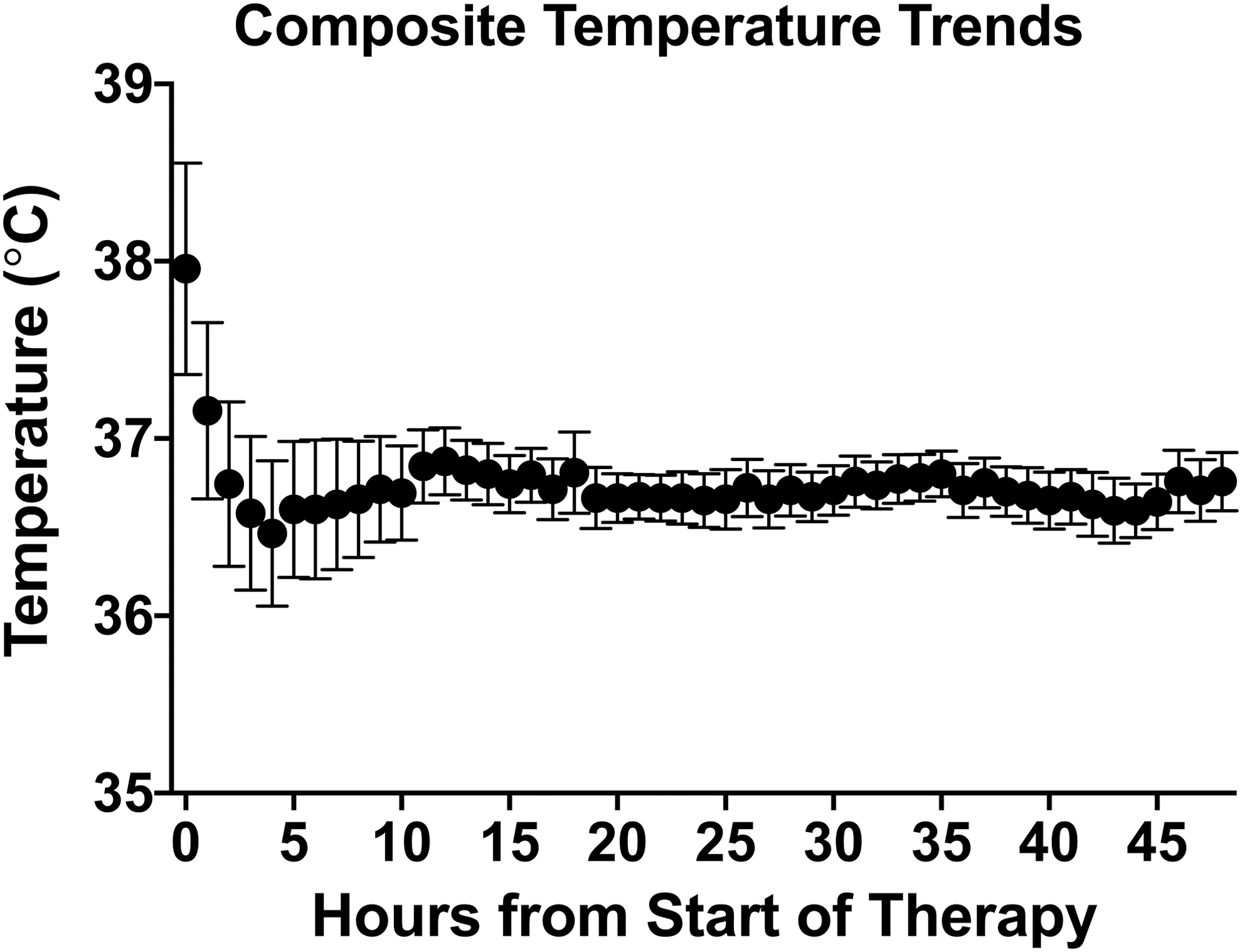
Comparative temperature trends for the normothermia cases for the first 48 hours of therapy. Temperatures are displayed as mean ± SEM. SEM, standard error of the mean.
Acetaminophen administration was a commonly used adjuvant for temperature management in normothermia cases before the initiation of therapy, but was not used in any of the hypothermia cases given that patient's starting temperatures were hypothermic (Table 1). Supplemental measures such as use of ice packs and reduction in ventilator humidification temperature were encouraged in the protocol; however, use was not documented and, therefore, could not be evaluated. Sedatives or analgesic medications were used at the initiation of therapy in the majority cases (89.5%; n = 17 cases). Sedative medications were mostly administered continuously. If sedative infusions were held, or only intermittent dosing used, the clinical reasoning was to facilitate neurological examinations. The most commonly used medication for sedation or analgesia was fentanyl. Similarly, NMB was used during therapy in the majority of cases, most commonly continuous cisatracurium (68.4%, n = 13 cases). Less than half of the patients were on NMB during the initiation of therapy. Reason for NMB to be held at TTM initiation was also to facilitate neurological examination. For both sedative/analgesic and NMB medications initiated after the start of therapy, the primary indication was shivering.
The most common adverse event related to TTM management was shivering (36.8% of cases). Several episodes were documented at times when sedation and NMB were held to facilitate clinical examinations. All patients received additional intermittent sedative or analgesic medications with or without NMB for treatment. The second most common adverse event was device alarms due to inadequate body surface coverage because of pad size. This issue was remedied after we broadened our pad size selection in 2018 as a QI intervention. Initially, we stocked only four pad sizes (small universal, x-small, small, and large); however, we expanded our pad size range to include all the pad size options available (neonatal, small universal, xx-small, x-small, small, medium, large, and universal). There was one episode of brief vasoactive medication initiation due to hypotension that correlated with patient receiving a bath while on normothermia therapy. As the patient's body temperature dropped during the bath, the device appropriately increased its water temperature resulting in vasodilation and corresponding hypotension. One case of premature therapy discontinuation was the result of persistent hypertension despite additional sedation. Additional safety monitoring focused on provider use of the device and required continual just-in-time training to remind bedside practitioners to not manually adjust the temperature on the device.
Discussion
This QI analysis highlights that TTM is feasible in critically ill pediatric patients using a gel-adhesive pad surface device, such as the Arctic Sun. Our study highlights three pertinent findings related to the use of this device for TTM: (1) The gel-adhesive pad system can reach goal temperature quickly and maintain TTM goals with a high level of accuracy; (2) attention to unique considerations for pediatric patients is required for protocol development, device application, and safety; and (3) commitment to educational efforts and the implementation of “super-users” may have played a valuable role in achieving the success that was observed. Given the known challenges that are linked to achieving rapid induction of TTM and rigorous maintenance of target temperature as observed in this preliminary study, our findings support the need for larger clinical studies directly comparing this new device with current surface cooling methods.
To our knowledge, this is the first study to evaluate the feasibility and efficacy of a gel-adhesive pad system in achieving and maintaining TTM in pediatric patients. Specific devices for TTM control targeting the pediatric population are lacking. Invasive catheter-based systems in children would pose feasibility and safety challenges, particularly in infants and young children. Thus, this gel pad approach for pediatric use is a welcomed potential development. For safe and effective TTM, a device should allow the patient to reach target temperature efficiently, maintain target temperature accurately, and in hypothermia protocols, allow for controlled rewarming.
For all three TTM protocols, time to target temperature was ∼90 minutes, with normothermia and mild hypothermia protocols reaching target temperatures in <60 minutes. This time to target temperature is less than what has been reported in adult studies that evaluated a gel-adhesive pad system device either independently or in comparison with other cooling devices (Carhuapoma et al., 2003; Mayer et al., 2004; Heard et al., 2010). Among adult studies, there was consistency in the time to reach goal temperature with the gel-adhesive pad system compared with a wide range of time to goal temperature for the traditional devices. Specifically, in these studies goal temperature was reached in 2.5–3 hours for the gel-adhesive pad system compared with 4–16 hours for traditional cooling devices (Mayer et al., 2004; Heard et al., 2010; Aujla et al., 2017). The shorter duration needed to reach target temperature in children versus adults using a gel pad system might be anticipated given the larger surface area to volume ratio in children.
We showed that target temperatures were maintained with notable accuracy, with recorded temperatures within goal >99% of the time with normothermia and mild hypothermia cases. Similarly, studies within adult critical care patients have shown superiority of the gel-adhesive pad system versus traditional cooling blanket use in maintaining temperatures with higher accuracy (Aujla et al., 2017). Further randomized pediatric studies are necessary to assess if there are differences in efficacy between the different TTM modalities and to identify if there is a form of TTM that is superior in specific clinical scenarios. For example, a gel-adhesive pad system may not be the best option for patients with impaired skin integrity due to burns, patients with hemodynamic instability, or patients expected to spend significant amounts of time in procedures such as imaging or operative/interventional, if the pads need to be removed for periods of time.
We recognize that in these 19 cases, time to target temperature represented a variety of scenarios, including both the traditional induction of hypothermia in a normothermic patient and normalization of temperature in a febrile patient, but also other scenarios that are encountered in the use of TTM, particularly after cardiac arrest in infants and children, such as increasing temperature from a level of spontaneous hypothermia below target. All of these scenarios represent clinically relevant examples of TTM—and thus, our data suggest that each can be managed in a facile manner using this gel-adhesive pad approach given the diverse starting temperatures in the different protocols. Thus, beyond the high level of rigorous temperature control once at target, this device appeared to demonstrate efficacy in induction across the clinical spectrum.
The gel-adhesive pads need to cover approximately 40% of the total BSA to accurately measure and manage the temperature. There are a wide variety of pad sizes that are commercially available for use. As the pediatric population has significant heterogeneity with regard to patients' weight, height, and age, it is likely imperative to find the appropriate pad size to obtain optimal coverage. For this study period, our institution initially carried only a select number of the different pad sizes to keep costs down while gauging the range of pad sizes needed based on our patient population. However, throughout this process, we found it necessary to have a variety of different pad sizes in stock despite the additional cost for this inventory. We found that at times pad sizing needed to be adjusted appropriately for patient's given body shape and size variability in our population—especially patients with weights or heights on the extremes of the expected range for a particular pad size. Appropriate pad fit and size allowed not only for optimal device functioning but also eliminated any device alarms related to water flow. Thus, pad fit, sizing, and application were areas that were highlighted by providers specifically during protocol development, educational efforts, and focus areas for improvement strategies. One way in which the unit optimized pad size selection was to keep “sample pads” of each size in the equipment room for reference before opening new pad packages for patients. Diverse pad inventory and potential sizing issues are unique pediatric considerations for use of the gel-adhesive pad system that necessitate specific attention during protocol development and when deciding if device implementation is appropriate within a pediatric unit. However, a study specifically evaluating the impact of pad size selection on device efficacy or safety in pediatric patients has not been carried out.
We recognize that this study was insufficient in sample to address the issue of safety. However, we found several safety aspects about use of the gel-adhesive pad device that need to be highlighted and considered in designing protocols for future larger studies and/or clinical use. First, as this device continuously adjusts to the patient's temperature to achieve the goals, it is important to consider the location and accuracy of temperature probe placement. We found that a rectal probe can become displaced during patient positioning or after a bowel movement that affects temperature accuracy and potentially exposes the patient to wide fluctuations in water temperature. Given these concerns, our protocol recommended use of an esophageal temperature probe to be connected to the device. In addition, we found that exposure during patient bathing may result in small fluctuations in patient temperature that may trigger the device to increase circulating water temperature leading to vasodilation. This may be a significant change especially in a hemodynamically unstable or fragile patient.
The majority of the literature for gel-adhesive pad system reports minor skin injuries with use of the system; however, there are some reports of more significant skin injuries (Varon et al., 2008; Jarrah et al., 2011; Wang et al., 2013). Given these potential concerns for skin injuries, our protocol necessitated frequent nursing assessments to monitor for signs of injury and implementation of skin protective interventions to minimize pressure injuries located at potential trouble spots (axillae, groin, and breast tissue). As noted earlier, our institution also set additional limitations on the range of water temperatures to prevent thermal exposure injuries.
Continued educational efforts (large group session and just-in-time training) of both our nursing and physician staff were felt to be necessary throughout the entirety of this process. Such efforts allowed for addressing common pitfalls with device setup or use, ensure understanding of protocol recommendations, and optimization of patient selection for device utilization. Identification and training of nursing and physician “super-users” created a select group of providers with more granular knowledge of the device setup, functionality, and potential user errors. This intervention allowed for improved safety and limited delays with therapy initiation at any time. Such “super-users” were also helpful in management scenarios where clinical management goals were changed (e.g., adjusting target temperature goals during therapy or deviation of set goal temperatures from the recommended protocol temperatures), this intervention ensured such changes were made on the device in a safe manner that allowed for continued controlled temperature management. Even with the intense focus on education during this quality initiative, there were still several instances of manipulation the temperature goals on the device or use of the protocol phases incorrectly. Highlighting the importance of continued educational efforts and the extensive time required to focus on education for a large critical care unit with many different bedside providers and physicians.
This case series may be helpful to other centers considering how best to provide TTM to their pediatric patients specifically if the gel pad system is selected. There are several limitations to this study that need to be considered. We were limited in analyzing data for cases that had complete clinical and device information and there was a substantial number of gel-adhesive pad system cases with missing clinical data. However, the 19 cases presented in this exploratory analysis were not selected based on any specific outcome and we believe that they are representative of the necessary feasibility and efficacy elements for this preliminary evaluation. We recognize that there were several deviations from our recommended protocol in the 19 cases illustrated. As this was a QI intervention, there was no requirement for clinicians to follow the recommended temperatures in the protocol as the device does allow for deviations upon setup and during therapy. The QI interventions focused on device setup, use, and efficacy based on the set goals provided by the clinical team. A larger pediatric study with protocolized temperature control without these deviations will provide further guidance to the understanding of the efficacy based on each protocol.
Given the small number of patient cases using traditional cooling blanket devices as well as the lack of randomization in our study, we cannot make adequate comparisons to draw conclusions about the superiority of either cooling mechanism for pediatric patients. We also cannot make claims on safety. We also noted a trend that our providers transitioned to using the gel-adhesive pad system device over the traditional cooling blanket for most TTM needs, so we had fewer overall cases that used the traditional cooling blanket than anticipated during the evaluation period. These factors thus precluded a meaningful comparison in the absence of a controlled trial in our population. Finally, the cost of both the device as well as the adhesive pads needs to be considered. The device costs between $40,000 and $60,000 USD depending on if new or refurbished and a complete set of pads for one treatment (maximum of 5 days of use) is approximately $900 USD. However, if efficacious in providing rigorous TTM, improved outcomes related to the optimal delivery of hypothermia and/or the well-known deleterious effects of fever after acute brain injury could outweigh additional costs.
Conclusion
Our pediatric experience with delivery of TTM using the gel-adhesive pad system demonstrated that it was feasible, and appeared to perform efficaciously with regard to both time to target temperature and with precision of temperature control during TTM—whether normothermia or hypothermic targets were utilized. We also defined several technical aspects of device use in pediatric patients that should be considered in future trial design and/or clinical use.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.